
Abstract
Introduction
Virtual consultations are increasingly being used in cancer rehabilitation, yet little is known about how the virtual consultation format shapes patients’ sense of embodied presence and relational care. This study explores how women diagnosed with breast cancer or ductal carcinoma in situ experience rehabilitative virtual consultations with nurses and focuses on how virtual consultations influence bodily presence, body modalities, and relational interaction.
Methods
An exploratory qualitative study was conducted using semi-structured telephone interviews with fourteen women who had participated in a nurse-led rehabilitative virtual consultation one year after treatment. Using Braun and Clarke's Reflexive Thematic Analysis, we analysed the data with particular attention to how digital mediation reconfigured embodied presence and relational care.
Results
Across the dataset, virtual consultations were experienced as altering body modalities and reducing embodied presence when bodily matters were addressed on-screen. Patients experienced vulnerability associated with the absence of physical co-presence and touch but also highlighted how the home environment created a sense of calm and safety. The analysis generated one overarching theme, The Body's Vulnerabilities in the Virtual Space, with four subthemes showing how virtual consultations continuously shifted between connection and disconnection, and how familiarity with the nurse supported relational grounding.
Discussion
The findings demonstrate that virtual consultations reconfigure embodied presence in cancer rehabilitation, which requires patients and nurses to negotiate new body modalities shaped by technology and by the environments from which they participate in the virtual consultation. These dynamics influence vulnerability, trust, and relational care, which underscores the need for digital health practices that recognize spatial embodiment and actively support embodied engagement at a distance.
Keywords
Introduction
Virtual consultations are synchronous clinical interactions between patients and healthcare professionals conducted through video-based communication technologies. They provide an alternative to face-to-face consultations between patients and healthcare professionals 1 and have rapidly become a patient-preferred and increasingly used consultation form within Western and high-income healthcare systems. 2 Patients highlight time savings, reduced travel, and improved opportunities to balance work and family commitments as key advantages. 3 A literature review reports that patients experience video consultations as making participation in follow-up care feasible in cases of long travel distances or mobility limitations. 4 In chronic care pathways, such as for diabetes, patients frequently report an increased sense of self-management and a perception of closer clinical contact when video consultations are combined with home monitoring.5,6 Similarly, studies from a gynaecological outpatient setting report that patients experience video consultations as “giving me less time as a patient and more time as myself,” a sentiment reflecting reduced logistical “medicalization” and improved integration into everyday life while simultaneously fostering a feeling of being seen and supported. 7 In cancer care, virtual consultations are emerging as a valuable complementary component within comprehensive cancer care delivery models.8–11 This is also evident in breast cancer care, where virtual consultations have been associated with improved quality of life, reduced psychological distress, high patient satisfaction, and increased convenience and accessibility in follow-up and survivorship care.12–14
Breast cancer is the most commonly diagnosed cancer in women, with approximately 2.3 million diagnoses worldwide in 2022. 15 In Western countries, women undergoing curative treatment for low-risk invasive breast cancer and ductal carcinoma in situ attend follow-ups with healthcare professionals at hospitals. 16 Follow-up is essential to monitor recurrence or progression and to support the patient's rehabilitation, physical and psychosocial adjustment, and health-related quality of life as they transition from active treatment to longer-term survivorship.16,17
Traditionally, follow-up consultations have been conducted in person at the hospital. The physical presence of the patient and the clinician in a shared clinical environment has underpinned assessments of surgical outcomes, including the clinician's expert visual and manual evaluation of whether postoperative healing and function are progressing as expected, as well as assessments of lymphoedema, functional impairments, body image concerns, and psychosocial rehabilitation. 16 However, there is growing recognition that not all post-treatment interactions require a physical examination and that consultations focused on education, counseling, self-management support, or symptom review could feasibly be conducted via virtual consultation with a specialist nurse. 12 Virtual consultation interventions among breast cancer survivors have shown improvements in quality of life, reductions in distress, and enhanced self-management. 13 However, although research on virtual consultations in oncology is expanding, evidence remains limited on how nurse-led rehabilitative consultations shape patients’ sense of connection and engagement with nursing professionals. One recent commentary highlights that despite promising feasibility and acceptability, empirical insight into how the virtual format influences the relational dynamics of care, perceptions of presence, and embodied aspects of virtual interactions is lacking. 18 Embodied care concerns how care is communicated and experienced through bodily presence, relational attunement, and sensory interaction between patients and healthcare professionals. 19 Bodily presence refers to the experience of being physically and relationally present and acknowledged within the clinical encounter. 20 This study aimed to investigate the experiences of women diagnosed with breast cancer or ductal carcinoma in situ who participated in rehabilitative virtual consultations with nurses, with a focus on how the virtual format shaped the women's sense of bodily presence and relational interaction.
Methodology
Design
This study adopted an exploratory qualitative approach using semi-structured interviews and reflexive thematic analysis as described by Braun and Clarke. 21 Reflexive thematic analysis is a theoretically flexible and interpretative approach that emphasizes researcher reflexivity and the active role of the researcher in knowledge production, allowing researchers to generate meaningful insights without being bound to a specific theoretical tradition.21,22 The study adhered to the Declaration of Helsinki, and all participants provided informed consent. This article has been prepared in accordance with the Reflexive Thematic Analysis Reporting Guidelines. 22
Participants and setting
A purposeful sampling strategy was used to recruit women whose diagnoses and clinical trajectories matched the study aims.23,24 Fourteen women were invited and agreed to participate. Eligible participants were women diagnosed with either low-risk cancer mamae or ductal carcinoma in situ who had completed the routine one-year post-treatment rehabilitative virtual consultation through the Epic electronic health record platform. 25 Following the virtual consultation, the consulting nurse asked whether the women would consent to being contacted by the clinical nurse specialist regarding participation in the interview study. Women with ductal carcinoma in situ were included as well as women with low-risk cancer mamae because these patients follow comparable treatment pathways and share similar needs in the post-treatment phase. 26
The rehabilitative consultation is conducted by one of the nurses, lasts approximately one hour, and is structured around a preparatory form, which is electronically provided to patients in advance (Figure 1). The form addresses perceived challenges with daily activities, sources of support, social difficulties, and physical and psychological burdens, and allows patients to raise any additional concerns they wish to discuss. At the hospital in this study, patients are routinely offered a rehabilitative virtual consultation one year after completion of treatment. Traditionally, these consultations were conducted in person, but since January 2023, they have been delivered virtually as part of a hospital-wide strategy to convert suitable consultations into virtual consultations. Patients unable to participate virtually are still offered in-person consultations in the outpatient clinic.
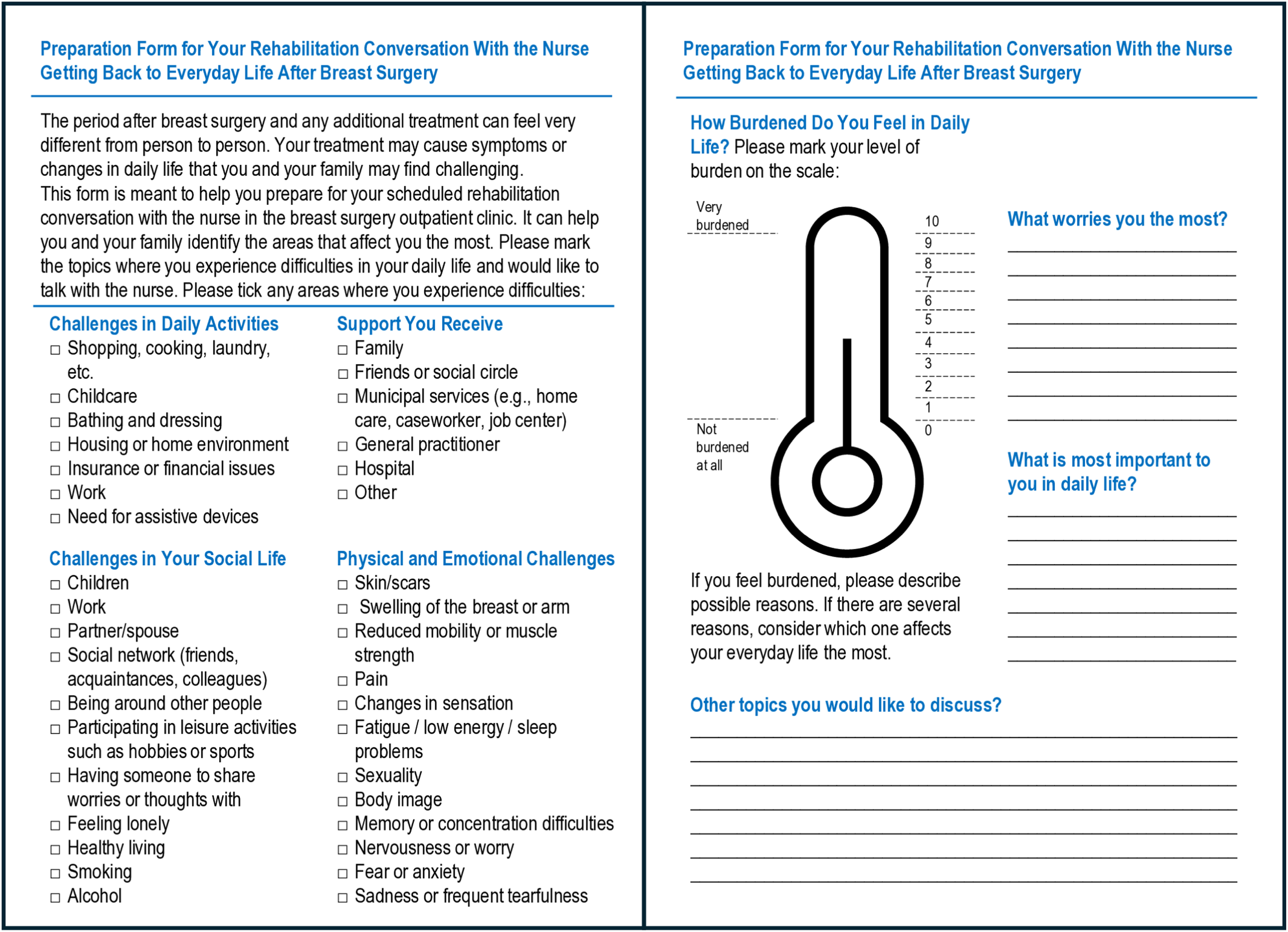
Preparation form distributed to patients along with the invitation to the rehabilitation consultation, supporting reflection on daily challenges and rehabilitation needs.
Immediately following the virtual consultation, the women were invited to participate in a qualitative interview by a clinical nurse specialist working at the outpatient clinic. This clinical nurse specialist was responsible for recruitment and interviewing but had not conducted the participants’ virtual consultations. Participants were recruited from the outpatient clinic at a department of plastic and breast surgery at a tertiary university hospital in Roskilde, Denmark. Recruitment continued until sufficient richness and depth of data had been obtained to address the research aim.
Data collection
Data were generated through semi-structured individual interviews 27 conducted between April 9 and September 18, 2025, by a female clinical nurse specialist. All interviews followed an interview guide developed by the entire author team to ensure coherence with the study aims and were designed in line with Braun and Clarke's emphasis on broad, open-ended, and flexible questioning to allow the patients’ perspectives to unfold. 23 Telephone interviews represented the most feasible approach for ensuring broad patient participation regardless of geographical distance from the hospital. Recent methodological literature demonstrates that telephone interviews are a fully valid mode of qualitative data collection, capable of generating rich and meaningful accounts comparable to in-person interviews.28,29 The interviews lasted between 18 and 25 min each. All interviews were audio recorded and transcribed verbatim prior to analysis.
Reflexive positioning
The study team represented different professional backgrounds within the research field. The first team member, head of research at the department and associate professor in nursing, had six years of experience within breast cancer care and clinical research in the field and led the analytical process. Another team member, a clinical nurse specialist and master's student, had 14 years of clinical experience in breast cancer care and rehabilitation within the study setting and conducted the interviews. A professor of nursing contributed broader qualitative expertise and theoretical perspectives that supported critical reflection and interpretation throughout the analysis. To support methodological congruence and integrity within the reflexive thematic analysis approach, the researchers acknowledged that their professional backgrounds, clinical experiences, theoretical interests, and subjectivities inevitably shaped both data generation and interpretation. Reflexive discussions within the author group were therefore used throughout the analytical process to promote reflexive openness and transparency and to critically consider how different perspectives and assumptions influenced the development and interpretation of the themes.
Data analysis
Braun and Clarke's Reflexive Thematic Analysis was applied to guide the analytical process.21,22 The analysis involved an iterative and interpretative process of thematic coding in which the researchers moved between the interview material, codes, and themes. The analysis focused primarily on semantic meanings within the participants’ accounts while also allowing interpretative engagement with relational and embodied experiences. Coding was understood as an active and reflexive process through which patterns of shared meaning were constructed. The interview material was coded multiple times to support engagement with the dataset. An initial round of coding was conducted by STH and MB and subsequently discussed within the author group to ensure a shared understanding, analytical coherence, and reflexive interpretation. This was followed by a secondary round of coding focused on refining and developing themes, conducted by STH and MB and then discussed with JW until a coherent interpretation. Through this iterative and reflexive approach, themes were generated that captured central aspects of the patients’ experiences with virtual consultations. Reflexivity was integral to the analysis and enabled the researchers to actively interpret and engage with the interview material while keeping in mind that the data cannot be treated as fully objective. This analytical strategy facilitated the systematic identification of patterns within the dataset, which yielded nuanced insights into patients’ perspectives on receiving rehabilitation via online video consultations with a nurse. NVivo 15 30 was used to organize and manage the dataset and to assist the coding process. In the subsequent interpretation, Bollnow's existential theory of space was applied in the discussion of the themes to illuminate how spatial conditions shape patients’ embodied experiences in virtual care settings. 31
Results
Participants
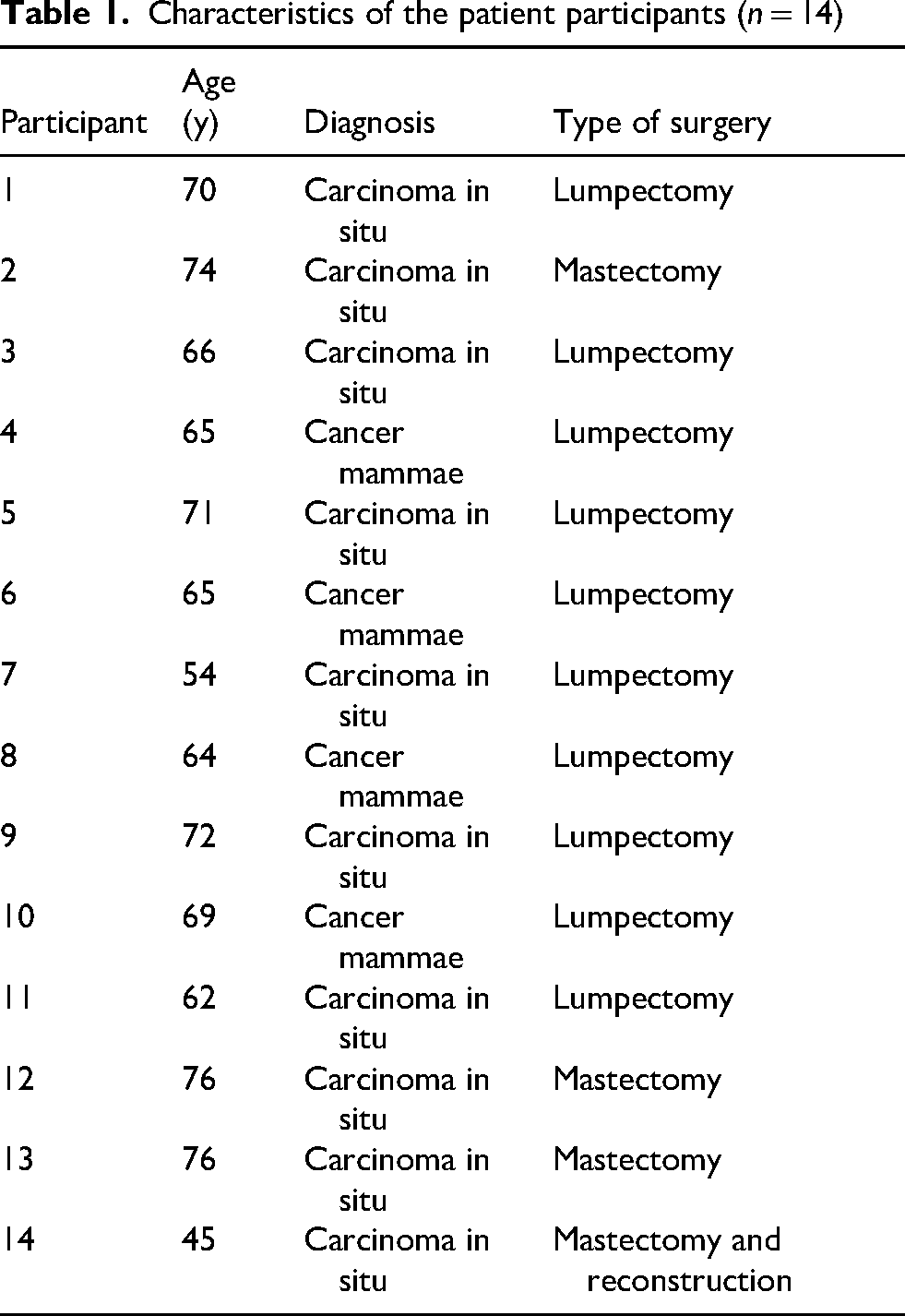
All participants were women, Danish-speaking, and self-identified as being of Danish ethnicity. Participants had undergone different types of breast surgery, including lumpectomy (n = 10), mastectomy (n = 3), or mastectomy followed by breast reconstruction (n = 1). Participants ranged in age from 45 to 76 years (mean age 66 years) and lived in both urban and rural municipalities surrounding the hospital catchment area (Table 1).
Characteristics of the patient participants (n = 14)
The analysis yielded one overarching theme, “The Body's Vulnerabilities in the Virtual Space,” which captured how patients experienced the interplay between bodily presence, virtual mediation, and relational care, including the inherent vulnerability of addressing bodily matters in an online format. Although patients continued to need embodied engagement to support rehabilitative conversations that fundamentally revolved around the body after cancer, the virtual setting tended to reduce their sense of embodied presence. This overarching theme was expressed through four interrelated subthemes: (1) When the Body Is Absent in the Virtual Room; (2) When Safety Moves Home; (3) The Thin Threshold of the Virtual Space; and (4) Relational Grounding Through the Familiar. In the following, each subtheme is introduced with a participant quotation, followed by an analytical elaboration of the theme.
When the body is absent in the virtual room
If you need to talk about something more difficult. If you’ve had a complicated course and need to discuss something hard, then it might feel better to sit face-to-face. Otherwise, the person on the screen really has to be skilled at staying with you in a difficult conversation despite the distance of the screen. You do get closer when you sit together in person and look each other in the eye. That's just how it is. (Participant 14)
When safety moves home
I think the conversation felt calmer because I was at home. I didn’t have to worry about anyone coming in and interrupting, for example. […] I can see this is the way forward in many cases. (Participant 4)
The thin threshold of the virtual space
It was completely fine talking to the nurse on screen. Once my husband had set everything up, I had no problems. But at first, I was a bit nervous about whether it would work, because I can’t handle it myself. And if you disappeared from the screen, how would I get you back? I have no idea. It's all just nonsense to me. (Participant 9)
Relational grounding through the familiar
It's easy to establish a relationship when you have the video on and in that way have each other right there, even if it's just on a screen. […] In that sense she can also read me, I think. If I had tried to hide something or just brush past it, I imagine she would have been able to pick up on it. (Participant 6)
Discussion
Our findings show how patients experienced a reduced sense of embodied presence when bodily matters were addressed through virtual consultations. Although the patients appreciated the flexibility and accessibility of the virtual format, they also described a specific form of vulnerability arising from the absence of physical co-presence and touch in conversations that fundamentally revolved around the body and previous physical illness. This resonates with other evidence showing that even small disruptions in communication or care continuity can act as critical thresholds where vulnerable patients risk being overlooked. 32 Reduced embodied presence was not experienced in the same way by all patients. Rather, the virtual format appeared to reshape how bodily presence and relational connection were experienced. While some women experienced distance and uncertainty due to reduced physical co-presence, others described the home environment and familiar surroundings as facilitating emotional safety, comfort, and relational grounding during the consultation.
The findings should be understood within the context of breast cancer rehabilitation, where breast cancer is linked to body image disruption and significant psychosocial consequences following treatment and surgery.33,34 Previous qualitative research has shown how women may experience altered bodily identity, femininity, and self-understanding while adapting to a “new normal” body after breast cancer treatment. 35 In this context, embodied and relational dimensions of care may hold particular significance in virtual consultations. However, the findings related to vulnerability, relational attunement, and bodily communication may also be relevant beyond breast cancer care and potentially transferable to cancer care more broadly when sensitive bodily experiences are addressed virtually.36,37
These findings of this study align with previous studies showing that virtual consultations can offer flexibility and a sense of autonomy while also challenging traditional forms of embodied and relational care. 38 Previous research in cancer and chronic care contexts also highlights patients’ appreciation of convenience and control at home but seldom addresses how bodily presence and emotional attunement may be altered when care is moved online.39,40 These findings mirror what the Lancet Oncology's Commission on the Human Crisis in Cancer identifies as a growing erosion of human presence in oncology, whereby technological efficiencies increasingly overshadow relational and embodied dimensions of care. 41 The Commission identifies a growing imbalance between technological innovation and the human dimensions of cancer care and neglect of the core practices that uphold dignity, alleviate suffering, and build trust among patients and healthcare professionals.
The findings indicate that healthcare professionals must attend carefully to how a sense of safety and relational attunement are established in virtual care. In physical hospital settings, clinicians routinely draw on well-known practices to protect patient privacy and create a secure relational environment, for example, by closing the curtain around the bed or arranging the room to signal confidentiality and care. A comparable form of intentional framing is needed in virtual consultations. Although the home setting may appear private, the experiences of the patients in our study showed that the virtual space does not automatically function as a safe or bounded clinical environment. Similarly, previous research has shown that the absence of tactile contact can be challenging for healthcare professionals, as nursing and clinical assessment are closely tied to the ability to physically examine and sense the patient. 42 Creating clarity about the structure of the encounter, attending to signals of comfort and readiness, and acknowledging the patient's domestic surroundings as part of the consultation can help cultivate a virtual space that supports dignity, emotional security, and embodied presence when sensitive bodily issues are discussed.43,44 An additional area for professional development is the cultivation of a clinical culture in which patients feel able to engage bodily in the virtual encounter, including showing a mastectomy scar when relevant, so that the consultation can fulfill its rehabilitative aims by addressing both psychosocial and physical needs. In line with Bollnow's view that “spaces receive their essence not from ‘space,’ but from places,” the findings illustrate that virtual consultations do not occur in neutral or empty environments. 31 Instead, both patients and professionals inhabit situated places such as living rooms, offices, kitchens, and bedrooms, each shaping how the body is sensed, displayed, and understood. As Bollnow points out, ‘man is never a subject deprived of space’; rather, humans are always embedded in lived spatial relationships that give meaning to their bodily experiences. 31 This study shows how these spatial relations shift when care is relocated to digital environments, producing new body modalities that are neither fully physical nor disembodied but are relationally shaped by the places from which the patients connect. See Figure 2 for an overview of the study findings and their implications for virtual cancer care.
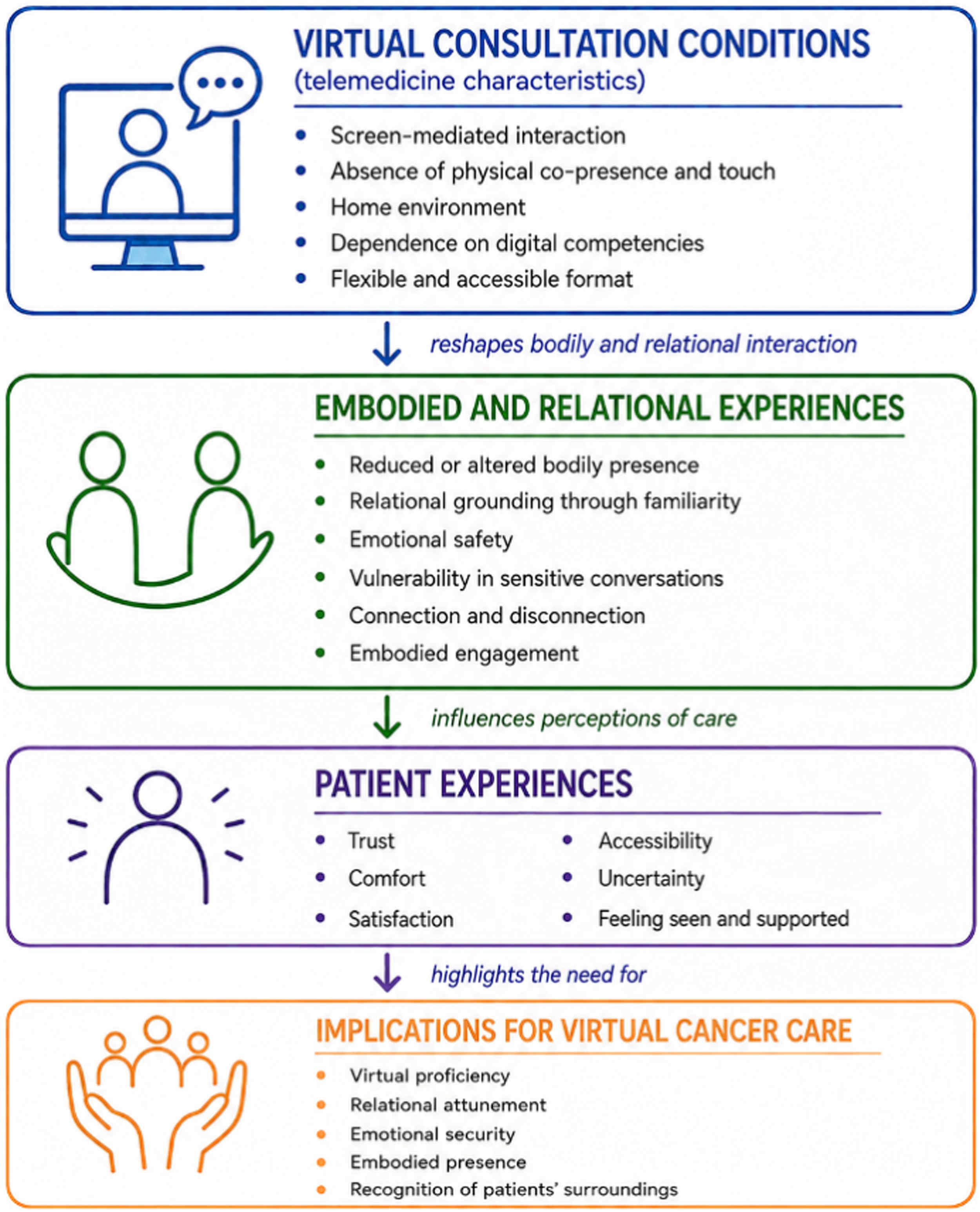
How virtual consultations reshape embodied and relational care in cancer rehabilitation. The model presents the study findings in an integrated and clinically applicable format by illustrating how specific aspects of telemedicine shape embodied and relational experiences, which in turn influence patient experiences of trust, comfort, safety, and uncertainty. The model further highlights observable mechanisms and practical implications for relational and embodied virtual cancer care.
A strength of this study is that the interviewer's clinical insight and familiarity with the rehabilitative context enabled a focused exploration of patients’ experiences. Reflexive engagement with the interviewer's professional affiliation and clinical experience was understood as inherent to the research process, where researcher subjectivity functioned as an analytic tool shaping both the interview interaction and subsequent analysis. A limitation is that the quality of the virtual consultations may have been influenced by the nurses’ digital and relational competencies, as healthcare professionals’ virtual proficiency has been identified as important for effective telehealth interactions.6,44
In conclusion, our study broadens understandings of embodied care and highlights the importance of digital health practices that recognize spatial embodiment and support relational grounding at a distance. The virtual setting reconfigures body modalities, requiring patients and professionals to negotiate an altered embodied presence shaped by technology and the environments from which they connect. These dynamics influence how vulnerability, trust, and professional attunement develop, underscoring the need to balance technological innovation with the human dimensions of core cancer care to uphold dignity, alleviate suffering, and build trust. Further research should examine how embodied interaction can be actively engaged in virtual consultations, for example, by discussing or showing patients’ surgical scars in the digital setting.
Supplemental Material
sj-pdf-1-jtt-10.1177_1357633X261461835 - Supplemental material for Embodied care at a distance: How virtual consultations reshape bodily presence and trust in cancer rehabilitation in women with breast cancer or ductal carcinoma in situ
Supplemental material, sj-pdf-1-jtt-10.1177_1357633X261461835 for Embodied care at a distance: How virtual consultations reshape bodily presence and trust in cancer rehabilitation in women with breast cancer or ductal carcinoma in situ by Stine Thestrup Hansen, Jeanette Weise1 and Malene Beck in Journal of Telemedicine and Telecare
Footnotes
Acknowledgments
We thank the patients who generously contributed their time and participated in this study.
Ethical considerations
The study was registered in the Research Registry of Region Zealand (REG-116-2023). In Denmark, approval from the Medical Research Ethics Committee is not required for studies based solely on qualitative interviews; therefore, no Committee approval was sought.
Consent to participate
All participants provided informed consent.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.