
Abstract
We examined the frequency of use by patients of a web-based reporting system to monitor and control cardiovascular disease (CVD) risk factors. A total of 192 patients with intermediate or high CVD risk were categorized into four quartiles based on their frequency of use of the telemedicine reporting system over one year. The lowest frequency users (Quartile I) averaged 17 reporting days in one year and the highest frequency users (Quartile IV) averaged 211 reporting days in one year. Factors associated with more frequent use were overall knowledge of CVD (P = 0.014), blood lipids (P = 0.017), smoking (P = 0.036), higher scores in medication self-efficacy (P = 0.016) and higher income (P = 0.002). All quartiles showed trends of decreasing systolic blood pressure from hypertensive (≥140 mm Hg) to pre-hypertensive (<140) ranges. Patients were able to lower CVD risk with as few as two transmissions per month using the telemedicine system. Telemedicine reporting coupled with self-assessment of health status can promote a strong patient-provider partnership for managing the chronic risk factors of CVD.
Introduction
Asymptomatic conditions including hyperlipidaemia, hypertension and diabetes increase the risk of cardiovascular disease (CVD) and contribute to CVD mortality. 1 Effective management of chronic risk in the presymptomatic phase of CVD is important in preventing CVD, and is rarely achieved in conventional practice. 2 Effective long-term reduction of CVD risk requires a patient-centred approach in which a strong patient-provider partnership is established and frequent patient-provider communication occurs.3,4
Active patient participation is a key part of managing chronic CVD risk.5,6 Patients with greater knowledge of their health conditions are more likely to adhere to treatment plans, communicate effectively with providers and modify lifestyle choices to improve health.7,8 Despite the importance of patient-provider communication in CVD risk management, patients often lack resources to maintain communication with their providers. 9 An Internet-based communication system can provide a convenient means of maintaining patient-provider interaction between office visits to manage chronic CVD risk factors.10,11
Patient knowledge plays an important role in patient participation in conventional treatment plans. 9 We hypothesized that the frequency of patient use of an Internet-based communication system linking patient and provider to manage CVD risk depends on patient health knowledge.
Methods
The present study examined the relation between patient health knowledge and behaviour, and use of a web-based telemedicine system, in a larger clinical trial. The aim of the clinical trial was to discover whether a web-based telemedicine system coupled with health status self-assessment could decrease CVD risk factors (hypertension, dyslipidaemia and smoking) in underserved inner city and rural populations. The trial was approved by the appropriate ethics committees. Primary outcome data for the trial has been published elsewhere. 12
The trial participants were of either sex, aged 18–85 years, with a 10% or greater 10-year risk of CVD.13,14 The study was conducted at the Temple University Medical Center (urban) and the Geisinger Medical Center (rural). The patients were followed for one year. The primary end-point was a reduction in their 10-year CVD risk determined by the Framingham Risk Score.
All patients were able to read and had access to a telephone. Exclusion criteria were: overt coronary artery disease, class 3 or 4 heart failure, angina, significant cognitive deficits, end stage renal disease on dialysis, patients living in nursing homes or boarding homes, and pregnancy. Patients who were unable to understand the study protocol or who were not competent to sign the informed consent were also excluded. All patients were instructed about the nature of the study, and signed an informed consent form. Patients were provided with a digital sphygmomanometer, pedometer and bodyweight scale if needed. All subjects received training in use of the Internet, and instructions on use of the telemedicine reporting system. 15 They were asked to record home blood pressure, daily steps, bodyweight and cigarette use, and report the data via the Internet communication system once a week.
The telemedicine system was web-based and allowed patients to log on from any computer with Internet access to enter information and correspond with health practitioners. Patients were not provided with computers but were trained to access the website from their own home computers.
Assessments
Patients were assessed at baseline, and at the conclusion of the study after one year. An initial physical examination, electrocardiogram, and blood and urine analyses were performed in an outpatient medical setting. A fasting blood sample was obtained from each subject to determine total cholesterol, LDL, HDL, triglycerides, C-reactive protein, glucose and HbA1c levels. The physical examination included measurement of height, bodyweight, waist circumference, blood pressure and 6-minute walk distance. 16 All patients underwent a formal assessment of CVD risk using the Framingham risk assessment model, which incorporates non-modifiable (age, sex) and modifiable (blood pressure, cholesterol, HDL, smoking status and diabetes) risk factors.13,14
Health knowledge and self-efficacy assessment
A health knowledge questionnaire (Cronbach's alpha = 0.72) was administered at baseline to assess patient knowledge of cholesterol, weight loss, diabetes, exercise, smoking, blood pressure and nutrition. 17 The knowledge questionnaire comprised 29 multiple-choice questions (at 5th grade reading level). In each content area, at least one question assessed patient knowledge of the following: targets or goals of each risk factor, associated risks of each risk factor, and desirable lifestyle or behavioural changes to reduce risk. The scores were added for each section, and a total knowledge score was calculated as the percentage of correct answers.
A 26-question self-efficacy survey (Cronbach's alpha = 0.70) was administered at baseline to assess patients’ confidence in their ability to persist with taking medications in a variety of situations. 18 A mean score was calculated for the items using a 3-point scale (from 1 = not sure at all to 3 = very sure).
Data analysis
We used multiple linear regression to evaluate the effect of health knowledge, behaviour, demographics and health measures on Internet use. The dependent variable was the number of days of Internet reporting. We compared first and fourth quartile measures using Student's t-test and compared data for four quartiles using univariate analysis of variance. A standard package was used for the analysis (SPSS version 19.0).
Results
A total of 192 subjects used the telemedicine system. The lowest frequency users (Quartile I) used the system for approximately 17 days in one year, while the highest frequency users (Quartile IV) used the system 13 times as frequently, see Table 1.
Characteristics of the subjects in the four quartiles of frequency of use of the telemedicine system over a one-year period. Values in parentheses represent SDs

Framingham 10 year CVD risk
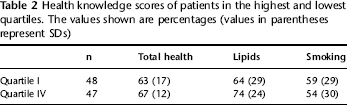
Multiple regression analysis of days of Internet use vs. baseline knowledge scores revealed that overall knowledge of CVD (P = 0.014), lipids (P = 0.017) and smoking (P = 0.036) were associated with more frequent use of the telemedicine system. More frequent users were also found to have a significantly higher score in medication self-efficacy than less frequent users (P = 0.016). Internet use was correlated with income level (P = 0.003), but not with medical insurance, urban or rural location or ethnicity. The health knowledge scores of the lowest (Quartile I) and highest (Quartile IV) groups of Internet use are shown in Table 2. When comparing the highest and lowest quartiles, only lipid knowledge showed a difference (P = 0.060).
Health knowledge scores of patients in the highest and lowest quartiles. The values shown are percentages (values in parentheses represent SDs)
Discussion
Because CVD has a long asymptomatic phase, managing CVD risk is often neglected until a cardiovascular event occurs. A strong patient-provider partnership for education and motivation is essential to manage chronic CVD risk in asymptomatic subjects. 6 An Internet-based telemedicine system provides a convenient method of communication between patient and provider, and can enable the personalization of treatment plans to follow and treat complex CVD risk patterns.3,4
In the present study, we found that the frequency of use of a web-based telemedicine system correlated with baseline patient knowledge of health, medication self-efficacy and income. Although the telemedicine system was widely accessible, its utilization was variable and depended on patient health knowledge related to CVD risk. Knowledgeable patients may have recognized the importance of risk modification and been more likely to utilise the telemedicine system. We also found that patients with higher medication self-efficacy scores were more likely to use the telemedicine reporting system. Self-efficacy refers to a person's confidence in his or her ability to perform an activity to accomplish a certain goal. 19 This reflection of patient attitude suggests that patients who feel more in control of their situations are more likely to take further steps to promote their own well being. Patients with higher income levels were found to use the system more frequently, and this may have been a consequence of greater Internet accessibility.
All patients showed a general trend of decreasing systolic blood pressure from hypertensive (≥140 mmHg) to pre-hypertensive ranges over the course of the study. This improvement was a trend among both high and low frequency users, suggesting that fewer than two transmissions per month were sufficient to motivate patients to improve systolic blood pressure. The most critical factor in promoting patient self-assessment is health knowledge. 20 Educating patients about health conditions motivates them to monitor their progress and communicate with their providers, ultimately improving their CVD risk.
Other studies have shown that patient knowledge of health conditions improves the outcome of patients undergoing conventional treatment of chronic conditions.7,8 Grover et al. 7 found that patients who were knowledgeable about their coronary risk were more likely to adhere to treatment plans and achieve a greater reduction in low-density lipoprotein levels. Deber et al. 21 suggested that patients have a relatively high desire for information regarding their health conditions. De Lusignan et al. 22 found high patient compliance rates in the use of telemonitoring devices by patients with chronic heart failure; however, they did not address factors that promoted patient usage of the system. Although studies examining factors contributing to patient usage of telemedicine reporting systems have not been reported, patient knowledge has been proven to have a profound impact on adherence to conventional treatment methods.
The present analysis was based on data acquired from a one-year study that was conducted in a medically underserved population. Thus, the results may not be generalizable.
Conclusion
To reduce the frequency of overt CVD events, early prevention is needed. Telemedicine reporting coupled with self-assessment of health status can promote a strong patient-provider partnership to manage the chronic risk factors of CVD. Patients can lower their CVD risk with as few as two transmissions per month using a telemedicine system. Although a web-based reporting system encourages frequent patient self-monitoring and communication with providers, it is the patient's choice to use the system to manage CVD risk factors. Patients with greater health knowledge are more likely to use it, and thus, improve CVD risk. 10 By taking steps to improve patient health knowledge, healthcare providers can enhance patient involvement in the treatment process and improve patient outcomes.
Footnotes
Acknowledgements
The study was supported by a grant from the Commonwealth of Pennsylvania (RFA-ME02-380). AB is a consultant for InSight Telehealth LLC and WS owns stocks in InSight Telehealth LLC.