Abstract

In honor of Jay D. Coffman (1928–2006), distinguished internist and research of vascular medicine and clinical cardiology, SVM sponsors an annual award in vascular medicine and biology research. The top finalists make oral presentations during the Jay D. Coffman Young Investigator Presentation that will be held on Thursday, June 16, at 2:30 p.m. The winners of the Jay D. Coffman Young Investigator Award will be announced prior to the close of the annual meeting.
Top-scoring original research abstracts were invited to participate in the Best of SVM Science session. Authors will give oral presentations during the Rapid Fire Session on Friday, June 17, at 11:15 a.m.
Authors will give poster presentations on Thursday, June 16, at 5 p.m. Poster professors will moderate discussion.
For more information about the meeting visit: www.vascularmed.org/AM16
Jay D. Coffman Young Investigator Award Presentations
YIA 1
Hypoxia and Ischemia-Induced Platelet Dysregulation
University of Rochester, New York, USA
Background: We recently reported that a novel platelet protein called ERK5 may contribute to dysregulated platelet activity in the ischemic microvascular environment. In this study we sought to determine whether hypoxia altered the platelet phenotype and activation state.
Methods: Human or mouse platelet activation and expression of proteins known to be platelet-activating were examined after platelet exposure in vivo or ex vivo to reduced oxygen (5-10% O2). Platelet activation was assessed by FACS (surface P-selectin expression), plasma platelet factor 4 (PF4) concentration, or by platelet spreading on a fibrinogen matrix (laser confocal microscopy). Mice subjected to unilateral pneumonectomy were employed as an additional surrogate for hypoxic disease.
Results: In platelets ex vivo at 10% O2, platelet ERK5 protein expression was increased by 2-fold, RAC1 by 2-fold, and P70S6K by 50-fold at 3 hrs. Mouse platelet activation was enhanced after 5% O2 exposure vs. 21% O2 ex vivo for 30 mins, while human platelet activation was more heterogeneous. Platelet activation and protein synthesis were suppressed during hypoxic conditions in platelet ERK5-deficient mice. The protein degradation inhibitor MG132 further increased protein expression of ERK5, RAC1, and P70S6K during hypoxia while a specific P70S6K blocker, PF4708671, abolished protein synthesis. Mice living at 10% O2 for 5 days vs. 21% O2 showed enhanced agonist-mediated platelet activation. In mice with unilateral pneumonectomy vs. sham surgery, hypoxia was accompanied by increased platelet ERK5 activation coincident with enhanced platelet activation (Fig. 1), with a marked increase in pulmonary staining for platelet precursor megakaryocytes.
Conclusions: The platelet phenotype in a hypoxic environment changes and is in part ERK5-dependent. Platelet ERK5 may be a viable target to prevent this maladaptive phenotypic switch which may account for thrombotic events and unexpected anti-platelet drug responses in ischemic diseases.

The platelet phenotype is altered by hypoxia. (A) Platelets from wild-type (WT) mice are activated following exposure to hypoxia (5% O2 ex vivo), with TRAP as a positive control for platelet activation. Platelet activation reported as surface p-selectin mean fluorescence intensity (MFI) ± SD, n=4, *p < 0.05 vs. 21 %O2. (B) Platelets from WT mice were exposed to hypoxia (5% O2 ex vivo), for the times noted. Marked increase in platelet protein expression was noted following hypoxia, shown by immunoblotting (I.B.). Molecular weight shown in kiloDaltons (kDa). (C) Platelets isolated from WT mice after 5 days of hypoxia (10% O2 in vivo) spread more readily on a fibrinogen matrix (mean surface area ± SEM (n=26-35, ** p= 0.002). (D) Platelets isolated from WT mice after 5 days of hypoxia (10% O2 in vivo) are more readily activated, reported as P-selectin mean fluorescence intensity (MFI) ± SD, n=5, *p < 0.05 vs. 0 agonist.
YIA 2
Use of Machine Learning to Accurately Predict Adverse Events in Patients with Peripheral Artery Disease Using Electronic Health Record Data
1Stanford Health Care, California, USA, 2Stanford University, California, USA
Introduction: Patients with peripheral artery disease (PAD) are at high risk of major adverse cardiac and cerebrovascular events (MACCE). However, no currently available risk scores accurately delineate which patients are most likely to sustain an event, creating a missed opportunity for more aggressive risk factor management. We set out to develop a novel predictive model – based on automated machine learning algorithms using electronic health record (EHR) data – with the aim of identifying which PAD patients are most likely to have an adverse outcome during follow-up.
Methods: Data were derived from patients with a diagnosis of PAD at our institution. Novel machine-learning algorithms including random forest and penalized regression predictive models were developed using structured and unstructured data that including lab values, diagnosis codes, medications, and clinical notes. Patients were matched for total follow-up time to remove length of patient records as a biasing factor in our predictive models.
Results: After matching for length of follow-up, 3807 patients were included in our models. A total of 1269 patients had a MACCE after PAD diagnosis. The median time to MACCE was 2.8 years after PAD diagnosis. Utilizing 1492 different variables extracted from the EHR, our best predictive model was able to very accurately predict which patients would go on to have a MACCE event after diagnosis of PAD with an AUC of 0.9, with a sensitivity, specificity and positive predictive value of 0.90, 0.96, and 0.93, respectively.
Conclusions: Hypothesis-free, machine-learning algorithms using freely available data in the EHR can accurately predict which PAD patients are most likely to go on to develop future MACCE. While these findings require validation in an independent data set, there is hope that these informatics approaches can be applied to the medical record in an automated fashion to risk stratify patients with vascular disease and identify those who might benefit from more aggressive disease management in real-time.
YIA 3
The Remarkable Heterogeneity of Ankle-Brachial Indices in Patients Undergoing Revascularization for Critical Limb Ischemia
University of Michigan Health System, Ann Arbor, Michigan, USA
Background: Critical limb ischemia (CLI) is diagnosed by the presence of rest pain, tissue ulceration, and/or gangrene due to chronic arterial insufficiency. Notably, these signs/symptoms may also be due to non-vascular etiologies (e.g. diabetic neuropathy). There has been a recent increase in revascularization treatment for CLI, though it remains unclear what fraction of patients (pts) have severe peripheral artery disease (PAD) on functional testing. We described the distribution of pre-intervention treated limb ankle-brachial indices (ABIs) among CLI pts undergoing percutaneous vascular intervention (PVI) or surgical revascularization (SR) across 47 hospitals in Michigan.
Methods: Among 10,704 pts with signs/symptoms of CLI (rest pain and/or tissue ulceration/gangrene), 9091 (85%) underwent PVI and 1613 (15%) underwent SR from 1/2012 – 6/2015. We excluded pts with acute limb ischemia, and used chi-square and t-tests to make comparisons.
Results: 918 (56%) pts had ABIs documented in the hospital record prior to SR, compared to 4385 (48%) prior to PVI. SR pts had evidence of more severe PAD, as demonstrated by lower ABIs [SR mean ± SD: 0.61 ± 0.29; PVI mean ± SD: 0.71 ± 0.28; P < 0.01]. There was substantial variation in ABIs within each group (Figure). Severe PAD (ABI ⩽0.4) was uncommon (16%), and was more prevalent in SR pts [245 (27%); PVI: 625 (14%); P < 0.01]. An ABI ⩽0.4 was also uncommon in pts with rest pain only (n = 438, 17%) as well as in pts with ulceration/gangrene (n = 432, 16%).
Conclusions: Only a small fraction of pts undergoing revascularization for CLI in contemporary practice had severe PAD by ABI testing raising the question of the utility of the ABI in determining disease severity in this population. The marked disconnect between ABI severity and clinical diagnosis suggests the need for standardization of functional PAD testing in pts with signs/symptoms concerning for CLI.

YIA 4
Prevalence of Intracranial Aneurysms in Women with Fibromuscular Dysplasia: A Report from the United States Registry for Fibromuscular Dysplasia
1University of Michigan Medical School, Ann Arbor, Michigan, USA, 2Cleveland Clinic Foundation, Ohio, USA, 3Icahn School of Medicine at Mount Sinai, New York, USA, 4University of Michigan Health System, Michigan, USA, 5University of Virginia Health System, Virginia, USA, 6Vascular Health Alliance, South Carolina, USA, 7Massachusetts General Hospital Fireman Vascular Center, Massachusetts, USA
Background: Fibromuscular dysplasia (FMD) is an uncommon, non-inflammatory, non-atherosclerotic disease of medium and large arteries. It is suspected that the prevalence of intracranial aneurysm (IA) in FMD is increased relative to that of the general U.S. population (estimated at 2-5%). Previous estimates of IA prevalence in patients with FMD come from neurosurgery case series, which suffer from biases in patient inclusion. We examined IA prevalence in FMD patients enrolled in a large clinical registry.
Methods: Patients enrolled in the US Registry for FMD with intracranial (IC) imaging at baseline were included. Patients who were male, under 18 years old at time of diagnosis, or had another disease with predisposition to aneurysm formation (e.g., Marfan’s Syndrome) were excluded. Imaging reports of all patients with reported internal carotid, vertebral, and suspected IC artery aneurysms were reviewed.
Results: 660 of 1063 (62%) female patients in the Registry had IC imaging prior to enrollment. Eighty-four of those (12.7%) had a saccular or broad-based IA of at least 2 mm in greatest dimension. The size of the largest IA in each patient is reported in the Figure; IA ⩾ 5 mm occurred in 42% of patients with aneurysms. Twenty-six of 84 patients (31%) had more than one IA; the mean number of IAs per patient was 1.5. Thirty-three of 84 patients (39%) had at least one IA repaired. IA was not significantly associated with the presence of extracranial carotid and vertebral FMD (P = 0.20) or renal FMD (P = 0.83).
Conclusions: The prevalence of IA in women with FMD was much higher than in the general population. Therefore, it is recommended that all FMD patients have intracranial imaging if not already performed.

YIA 5
A 5-Year Analysis of Outcomes for Pulmonary Embolism Based on Class of Anticoagulant at Discharge
1University of Toledo College of Medicine, Ohio, USA, 2ProMedica Physicians Jobst Vascular, Ohio, USA
Background: Direct acting oral anticoagulants (DOACs) targeting factor Xa are increasingly being prescribed as definitive treatment for VTE. There are little clinical data on the impact of this major shift regarding the management of VTE. The purpose of this study is to determine if there are differences in outcomes based on discharge anticoagulant class for patients newly diagnosed with PE from a metropolitan hospital.
Methods: A 5-year retrospective chart review was conducted beginning in 2010, at a major metropolitan hospital for PE outcomes focusing on readmission, VTE recurrence, hospital length of stay (LOS), and mortality at 6 and 12 months. Discharge medication was classified as warfarin, DOAC, or other (enoxaparin, heparin, or fondaparinux). A multivariate analysis was performed controlling for confounding factors. Bleeding was not independently analyzed.
Results: Three-hundred nineteen patients were identified. Significantly reduced LOS was observed in patients discharged on DOACs versus warfarin. Twelve-month mortality was shown to be significantly lower with lower PESI class and discharge on DOACs. Neither 30-day readmission nor 6-month VTE recurrence was different based either on discharge anticoagulant or PESI class, although, there was a trend towards increased recurrence with lower PESI class.
Conclusions: Decreased LOS was observed in patients discharged on DOACs. Twelve-month all-cause mortality was lower in patients discharged on DOACs, and tended to be lower in patients with lower PESI scores.

this group consisted of enoxaparin, unfractionated heparin and fondaparinux.
Best of SVM Science Rapid Fire Session
Rapid Fire 1
Walking Capacity is Positively Related with Heart Rate Variability in Symptomatic Peripheral Artery Disease
1Hospital Israelita Albert Einstein, São Paulo, São Paulo, Brazil, 2University of São Paulo, São Paulo, Brazil, 3University of Pernambuco, Pernambuco, Brazil, 4James Cook University, Queensland, Australia
Background: Symptomatic peripheral artery disease (PAD) patients have low heart rate variability (HRV), which is a predictor of cardiovascular disease incidence and mortality. However, whether walking capacity is associated with HRV in these patients remains unknown. Therefore, this study investigated whether walking capacity is associated with HRV in symptomatic PAD patients.
Methods: Ninety-five patients were recruited. Patients undertook a supine position for 20 minutes with the final 10 minutes examined for resting HRV. Time domain, frequency domain and non-linear indices were evaluated. A maximal treadmill test (Gardner protocol) was performed to assess total walking distance (TWD). Post-hoc Mann-Whitney U tests were used to identify differences between PAD patient groups. Spearman rank correlations were employed to examine the relationship between TWD and HRV parameters.
Results: Symptomatic PAD patients with high walking capacity exhibited significantly greater HRV in comparison with patients with low walking capacity. Furthermore, walking capacity was positively associated with time domain and non-linear indices of HRV (all p<0.05).
Conclusion: A greater walking capacity is associated with better HRV in symptomatic PAD patients.
Rapid Fire 2
Racial Differences in Mobility Loss in Peripheral Artery Disease
1Northwestern Feinberg School of Medicine, Chicago, USA, 2University of Maryland School of Medicine, Maryland, USA, 3National Institute on Aging, Maryland, USA, 4The University of Chicago MedicineChicago, USA, 5Stanford University, California, USA, 6University of California at San Diego, California, USA
Introduction: It is unclear whether African-Americans with peripheral artery disease (PAD) have faster functional decline than Caucasians with PAD.
Method: Participants with an ankle brachial index (ABI) < 0.90 were identified from Chicago medical centers. Mobility impairment and the six-minute walk were assessed at baseline and subsequently every 6 to 12 months. Mobility loss was defined as becoming unable to walk up and down a flight of stairs or walk ¼ mile without assistance.
Results: Of 1272 PAD participants, 360 (28%) were African-American. Mean follow-up is 44 months. Among participants without baseline mobility impairment, African-American race was associated with a higher rate of mobility loss, adjusting for age, sex, ABI, comorbidities, smoking, and other confounders (hazard ratio (HR)=1.41, 95% Confidence Interval (CI)=1.04 to 1.90, P=0.03). This association was attenuated and no longer significant after additional adjustment for socioeconomic status (HR=1.16, 95% CI=0.83 to 1.63, P=0.38) and physical activity (P=0.12), respectively. Among participants able to walk six minutes continuously at baseline, African-American race was associated with a higher rate of becoming unable to walk six minutes continuously, adjusting for age, sex, ABI, comorbidities, and other confounders (HR=1.47, 95% CI=1.08 to 2.00, P=0.015). This was attenuated after additional adjustment for socioeconomic status (HR=1.23, 95% CI=0.89 to 1.72, P=0.21) but not after adjustment for physical activity (P=0.02).
Conclusion: African-Americans with PAD have higher rates of mobility loss and becoming unable to walk six-minutes continuously compared to whites with PAD. These differences appeared related, in part, to racial disparities in socioeconomic status and physical activity.
Rapid Fire 3
Higher-Intensity Statin Use in Patients with Symptomatic Peripheral Artery Disease (PAD) is Associated with Longer Survival
1UC Davis Medical Center, Sacramento, California, USA, 2Denver VA, Colorado, USA, 3University of Colorado Medical Center, Colorado, USA
Background: The relative benefit of higher statin dosing in patients with PAD has not previously been reported. We compared the effectiveness of low-moderate intensity (LMI) vs. high-intensity (HI) statin dose on clinical outcomes in patients with PAD.
Methods: We reviewed 909 patients with symptomatic PAD (45% Claudication, 55% CLI) who underwent therapeutic endovascular intervention from 2006 – 2013. High-intensity statin was defined as atorvastatin 40-80mg or rosuvastatin 20-40mg. Baseline demographics, procedural data, and outcomes were retrospectively analyzed.
Results: Sixty-nine (n=629) percent of the total cohort were prescribed statins. The mean low density lipoprotein (LDL) level was similar in patients on LMI vs. HI (80 ± 30 vs. 87 ± 44 mg/dL, p = 0.14). Among patients prescribed statins, 20% (n=124) were prescribed HI statin therapy. Baseline demographics such as age (68 ± 12 vs. 67 ± 10 yrs, p = 0.25), BMI (28 ± 8 vs. 28 ± 5 kg/m2, p = 0.79), smoking history (76 vs. 80%, p=0.42), diabetes (55 vs. 50%, p=0.17), and hypertension (88 vs. 89%, p = 0.78) were similar between the two groups (LMI vs. HI). There was a higher prevalence of coronary artery disease (56 vs. 75%, p=0.0001), aspirin use (73 vs. 88%, p=0.002), and clopidogrel use (31 vs. 44%, p=0.006) use in patients on HI (vs. LMI). After propensity weighting, LMI statin therapy was associated with worse 5-year rates of overall survival (HR: 0.64, 95% CI: 0.42 – 0.97, p = 0.04). There was a trend toward worse freedom from MACE events (death, stroke, MI) in patients on LMI statin (64 vs. 50%, HR 0.68, 95% CI 0.5 - 1.0, p = 0.06).
Conclusion: In PAD patients treated with endovascular therapy, concomitant use of HI statin therapy was associated with improved survival. Further studies are needed to determine if the improved overall mortality with HI therapy is due to decreased adverse cardiovascular and/or due to decreased limb events.

Rapid Fire 4
A Vascular Health Maintenance Program for Patients with Peripheral Artery Disease Results in Lower Mortality, Morbidity, and Healthcare Resource Use
1University of Manitoba, Winnipeg, Canada, 2Grace General Hospital, Manitoba, Canada
Background: Despite well-established guidelines for risk factor modification in peripheral artery disease (PAD), treatment remains inadequate. Since 2004 the Manitoba Vascular Health Program (MVHP) has aggressively treated risk factors among patients referred for management of PAD. This retrospective cohort study compared outcomes of patients with PAD managed by the MVHP to those receiving usual care from 2004 to 2013. The objective was to determine whether participation in a vascular health maintenance program significantly impacted mortality, morbidity, or healthcare resource use.
Methods: Patients documented to have PAD from 2004 to 2013 were identified via electronic records of ABI measurements from provincial vascular laboratories. Comparison of de-identified data for various outcomes between MVHP participants (n=1193) and non-participants (n=4477) was facilitated by an extensive, validated health outcomes database at the Manitoba Centre for Health Policy. An intention-to-treat approach was used for analysis. Chi-square tests were used for categorical data, and t-tests for continuous data. Outcomes assessed were all-cause and cardiovascular mortality, lower limb amputation, healthcare resource utilization, and incidence of hypertension, diabetes or dialysis.
Results: MVHP participation was associated with a reduction in all-cause mortality (19.1% vs. 29.4%, p<0.01), cardiovascular mortality (6.7% vs.11.0%, p<0.01), lower limb amputation (4.5% vs. 7.2%, p<0.01), hospital admissions (339 vs. 545, p<0.01) hospital days (5.48 vs. 9.64, p<0.01) and reduced likelihood of diabetes (5.1% vs. 8.2%, p<0.01), hypertension (4.2% vs. 13.7%, p<0.01) and need for dialysis (0.7% vs. 1.6%, p<0.05).
Conclusion: This study is the first to demonstrate that a vascular health maintenance program results in lower mortality, morbidity. and healthcare resource use. Establishment of health maintenance programs for enrollment of all patients with PAD is recommended.
Rapid Fire 5
National Trends in Outcomes After Elective Pulmonary Endarterectomy
1University of Iowa, Iowa City, USA, 2Massachusetts General Hospital, Boston, USA
Background: Pulmonary endarterectomy (PEA) is a widely accepted treatment of advanced chronic thromboembolic pulmonary hypertension (CTEPH). Our objective was to define the national trends in outcomes after PEA using a large national database.
Methods: We used the Nationwide Inpatient Sample Database from 2009-2013 in this study. We identified all patients who underwent elective PEA during their hospitalization using International Classification of Diseases, 9th revision codes (N=308). In-hospital death was the primary outcome. Multivariable linear and logistic regression models were used to evaluate relationships between predictors (patient demographics, comorbidities and hospital factors) and outcomes. A P value of ⩽0.05 was considered significant for all comparisons.
Results: The incidence of in-hospital mortality was 5.8%; it was significantly lower in larger hospitals (>325-425 beds). The risk of in-hospital mortality increased from 2% in year 2009 to 9.8% in year 2013. The multivariable logistic regression analysis demonstrated a 3.14 times increase in the risk for in-hospital mortality following PEA performed at smaller hospitals (< 325-425 beds; P= 0.028). About 22% of the surgeries were performed in smaller hospitals.
Conclusions: The incidence of in-hospital mortality after PEA has a worsening trend over a 5-year period, and the risk for in-hospital death was significantly higher among patients who underwent PEA at smaller size hospitals.
Rapid Fire 6
An Automated Reminder System to Improve Inferior Vena Cava Filter Retrieval
Massachusetts General Hospital, Boston, USA
Background: Despite the technical advances of modern Inferior Vena Cava Filters (IVCF), retrieval rates are poor, and these devices are often left indwelling longer than needed. An automated system could improve IVCF retrieval practice patterns.
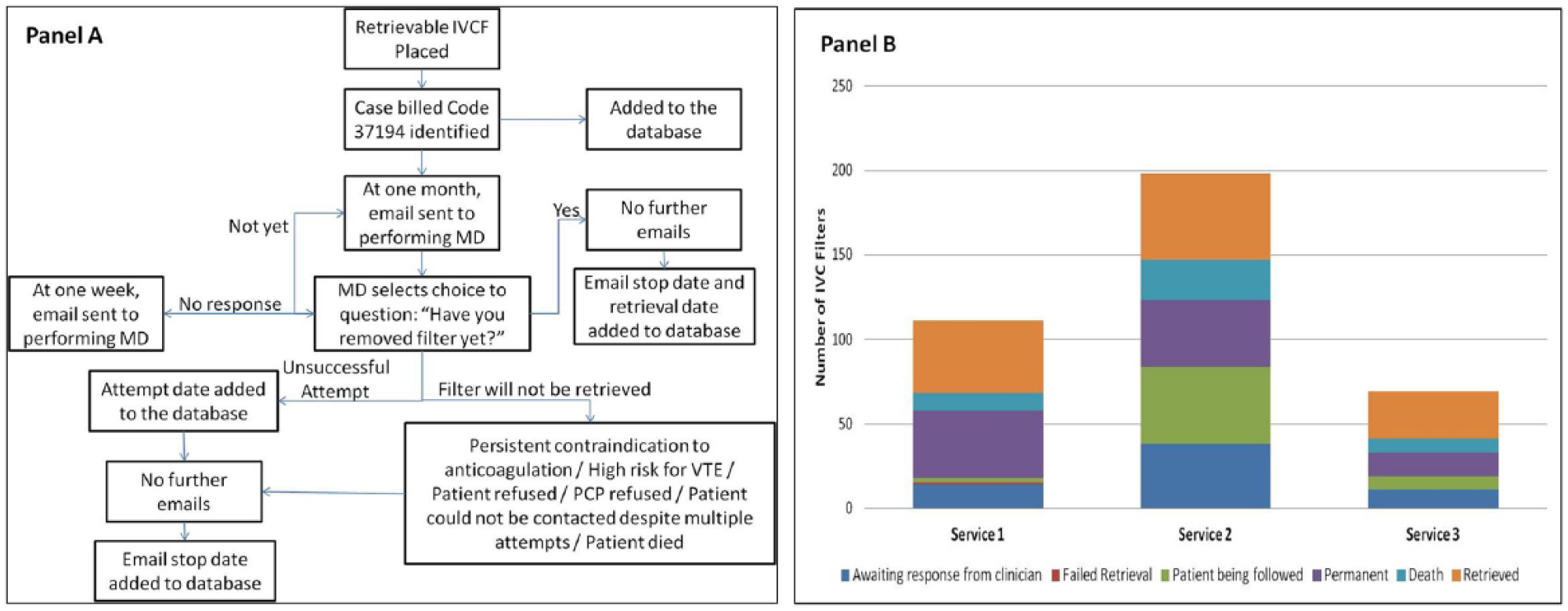
Methods: An automated IVCF retrieval reminder system was implemented at a tertiary medical center across all specialties that place IVCF (Figure, Panel A). Data were compared regarding IVCF-retrieval before (‘pre’ group, 1/1/2009-12/31/2011) and after implementation of this system (‘post’ group, 6/1/13 -6/1/15).
Results: Overall 1,066 IVCF insertions by 21 providers in 3 services were examined; 688 ‘pre’ and 378 ‘post’. Retrieval rate was 252/688 (36.6%) and 122/378 (32.3%) in the ‘pre’ and ‘post’ groups, respectively (P=0.15). Time to IVCF retrieval was shorter after system implementation (164.1±133.2 days vs. 111.0±78.1 days, P<0.0001). In the ‘post’ group IVCF were not retrieved due to patient death in 42/378 (11.1%) and decision to leave the IVCF in permanently in 93/378 (24.6%). Overall, IVCF outcomes were known in 83.3% of patients in the ‘post’ group (Figure, Panel B).
Conclusions: Not all IVCF can or should be retrieved. While an automated reminder system did not improve retrieval rate, it was associated with shorter IVCF dwell times, and offered rich information about the appropriateness and complexities of IVCF retrieval-related practice patterns and outcomes, which have resulted in improvements in our quality initiatives.
Arterial and Aortic Disease
Poster 1
Web-based Automated Carotid Artery Plaque Measurements Tool for Multicenter Clinical Trial: A Diabetic Cohort Study
1AtheroPoint, Roseville, California, USA, 2Azienda Ospedaliero Universitaria (A.O.U.) di Cagliari, Cagliari, Italy, 3NIT Raipur, Chhattisgarh, India, 4 Toho University, Tokyo, Japan, 5National Center for Global Health and Medicine, Tokyo, Japan, 6 Department of Electrical Engineering, NIT Raipur, Chhattisgarh, India, 7Vascular Screening and Diagnostic Centre London, Nicosia, Cyprus, 8UC Davis Vascular Center University of California, Davis, California, USA
Objectives: Multicenter clinical pharmaceutical trials require a platform where plaque measurements can demonstrate reproducibility and ensure observer variability. This study presents AtheroCloud™ - a novel cloud-based smart carotid intima-media thickness (cIMT) measurement in B-mode ultrasound - an anytime-anywhere screening tool for stroke risk assessment and its stratification.
Methods: The ultrasound arterial scans from multiple centers can be uploaded from the local server into the Cloud and multiple users around the globe can compute the cIMT measurements using AtheroCloud™ in a point-of-care setup. Vascular reports can be computed instantaneously. We benchmarked AtheroCloud against Sonographer and manual tracings.
Results: IRB approved, Toho University, Japan. One hundred patients (75 M/25 F, mean age: 68±11 years)consisted of L/R CCA artery (200 ultrasound images), (Toshiba, Japan) were collected using a 7.5-MHz transducer. The measured cIMTs (in mm) for left and right necks were: (i) AtheroCloud (0.87±0.20, 0.77±0.20); (ii) Sonographer (0.97±0.26, 0.89±0.29) and (iii) Manual (0.90±0.20, 0.79±0.20), respectively. The coefficient of correlation (CC) between Sonographer Vs. manual for L/R cIMT was 0.74 (P<0.0001) and 0.65 (P<0.0001), compared AtheroCloud Vs. manual for L/R was 0.96 (P<0.0001) and 0.97 (P<0.0001), respectively. We observed that 91.15% of the population in AtheroCloud had a mean cIMT error less than 0.11 mm as compared to Sonographer’s 68.31%. The AUC for the ROC was 0.99 for AtheroCloud compared to 0.81 for Sonographer. Our Framingham Risk Score stratified the population into three bins as follows: 39% in low-risk, 70.66% in medium-risk and 10.66% in high-risk bins. Statistical tests were performed to demonstrate consistency, reliability and accuracy of the results.
Conclusions: The proposed AtheroCloud system is a completely automated, fast, accurate, reproducible, reliable, anytime-anywhere smart tool for multi-center clinical trials and routine vascular screening.
Poster 2
Graduated Compression Stockings Do Not Improve Walking Capacity and Calf Muscle Oxygen Saturation Parameters During Six-Minute Walk Test in Intermittent Claudication Patients
1Hospital Israelita Albert Einstein, São Paulo, Brazil, 2University of Pernambuco, Brazil, 3University of São Paulo, Brazil, 4University of Maringá, Paraná, Brazil
Background: Graduated compression stockings (GCS) have been used to improve arterial and/or venous hemodynamic in patients with venous and lymphatic insufficiency. Moreover, GCS has been used in healthy individuals and athletes to improve sports performance. However, It has not been studied if GCS may lead beneficial effects in intermittent claudication (IC) patients, improving their walking capacity.
Methods: Eighteen patients with IC performed the six-minute walking test in two conditions in random order: GCS or placebo sock. Onset claudication distance and total walking distance were obtained. The calf muscle oxygen saturation (StO2) was continuously monitored before, during and after six-minute walk test. Comparisons of the walking capacity and StO2 parameters between GCS and placebo conditions were analyzed by Wilcoxon rank sum test.
Results: The onset claudication distance (GCS: 120 ± 99 meters vs. Placebo: 150 ± 126 meters; P=0,798) and total walking distance (GCS: 330 ± 108 meters vs. Placebo: 324 ± 60 meters; P=0,130) were similar between conditions. There were no differences in StO2 parameters between conditions (p>0.05).
Conclusion: GCS do not improve walking performance and oxygenation saturation during six-minute walk test in patients with IC.
Poster 3
A Lower Aorto-Iliac Bifurcation Position is Not Independently Associated with Incident Cardiovascular Disease Events: The Multi-Ethnic Study of Atherosclerosis (MESA)
University of California, San Diego, California, USA
Background: The aorto-iliac bifurcation distance (AIBD), the distance (mm) from the aorto-iliac bifurcation to the L5/S1 disc space, is used to determine the position of the bifurcation relative to the lumbar spine (larger AIBD = higher bifurcation position, smaller AIBD = lower bifurcation position). Atherosclerotic risk factors of age, gender, hypertension and smoking were associated with a lower bifurcation position, but risk factors commonly associated with arterial stiffness, diabetes and elevated triglycerides, were associated with a higher bifurcation position. We surmised that the bifurcation position may be an independent marker for vascular aging, and hypothesized that it may also be an independent marker for incident CVD events.
Methods: In a multi-ethnic cohort of community-dwelling individuals, free from clinically manifest CVD at recruitment, computer tomography (CT) was used to measure the AIBD, and this distance was used to determine the bifurcation position. Cox proportional hazard was used to determine associations of the bifurcation position with future coronary heart disease (CHD, defined as myocardial infarction, resuscitated cardiac arrest, sudden cardiac death), CVD (defined as CHD plus stroke and stroke death), and all-cause mortality (ACM).
Results: In 1711 participants (51% men), the mean AIBD was 26 ± 15mm. After a median follow-up of 10 years, 63 (3.7%) developed CHD, 100 (5.8%) developed CVD, and 129 (7.5%) were deceased. After adjustments for CVD risk factors, hazard ratios for CHD (HR = 0.8, 95% CI: 0.4 to 1.7), CVD (HR = 0.9, 95% CI: 0.5 to 1.7), and ACM (HR = 1.1, 95% CI: 0.6 to 1.8) were non-significant. (Table)
Conclusion: Despite being an independent marker for adverse vascular changes in the aorta, the aorto-iliac bifurcation position was not independently associated with future CVD events. Researchers should investigate the utility of other age-related anatomical changes in the vasculature in CVD risk prediction.
Unadjusted and adjusted Cox proportional hazard ratios of aorto-iliac bifuraction distance (AIBD) quartiles for cardiovascular disease events.
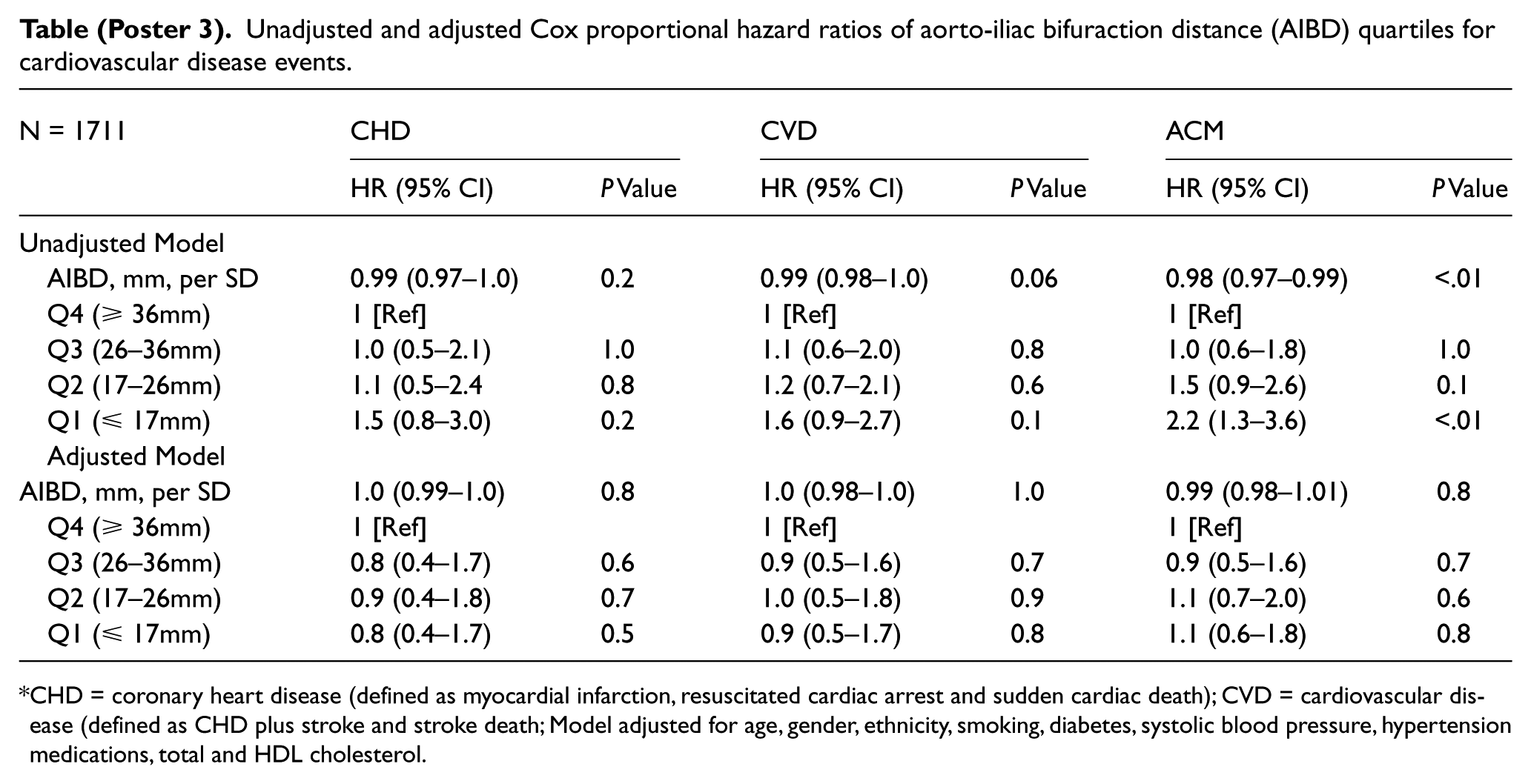
CHD = coronary heart disease (defined as myocardial infarction, resuscitated cardiac arrest and sudden cardiac death); CVD = cardiovascular disease (defined as CHD plus stroke and stroke death; Model adjusted for age, gender, ethnicity, smoking, diabetes, systolic blood pressure, hypertension medications, total and HDL cholesterol.
Poster 4
Long-Term Effects of Exercise Program in Major Adverse Events in Patients with Claudication
1University of Oklahoma Health Sciences Center, Oklahoma City, Oklahoma, USA, 2College of Public Health, University of Oklahoma Health Sciences Center, Oklahoma City, Oklahoma, USA
Background: The long-term effects of participating in a walking program on major adverse cardiac events (MACE) and major adverse limb events (MALE) in patients with intermittent claudication (IC) is not known.
Methods: Medical records of 180 patients randomized to either a supervised exercise program, a home-based exercise program, or a light resistance training, attention control group were reviewed for lower extremity revascularization, stroke, myocardial infarction and amputations. Social Security Death Index was reviewed for publicly available mortality data. The Kaplan-Meier method was used to estimate time-to-event distributions, which were compared between groups using a log-rank test.
Results: Medical record data was available on 94 out of 180 participants who were followed at the University of Oklahoma Medical Center or at the Oklahoma City VA Medical Center. The follow-up ranged from < 2 months to 10.7 years, with a median follow-up duration of 5.1 years. Subjects assigned to either exercise group were more likely to have had lower extremity revascularization (p = 0.049) and cerebrovascular accident (p = 0.028) at baseline than the control group. There was no significant difference among the randomized groups according to survival (p=0.48), and event-free survival to revascularization (p=0.17), myocardial infarction (p=0.23), stroke (p=0.33) and amputations (p=0.48). However, the event-free survival time to having at least one of the events was significantly longer (p=0.016) in the control group. When baseline group differences in prevalence of lower extremity revascularization and cerebrovascular disease were adjusted, event-free survival time to at least one event was no longer significant among groups (p=0.63).
Conclusions: We found no long-term MACE/MALE difference in outcomes among IC patients who participated in short-term, home-based, and on-site supervised walking programs. Further studies with larger samples and complete follow-up are needed.
Poster 5
Critical Examination of Toe-Brachial Index – Defining Normal
Mayo Clinic, Rochester, Minnesota, USA
Objectives: To define normal toe-brachial index (TBI).
Methods: Patients referred to the outpatient non-invasive vascular laboratory for peripheral disease were evaluated by Doppler waveforms, segmental pressures (resting and post-exercise), and transcutaneous oximetry (TcP02) as ordered. Total patients evaluated including toe pressures: N= 2679. Limbs were categorized by criteria per modality tested into two specific subgroups: “Normal” (N= 780: normal Doppler waveform, normal segmental pressures at rest and post-exercise) and “Abnormal” (N= 750: abnormal Doppler waveform, abnormal pressures at rest and post-exercise). The toe pressure and toe-brachial Index (TBI) values were obtained by digital cuff with photoplethysmography signal return without heating of the limb or probe. Values were compared within and between each group. Additionally, the relationship to TcP02 was evaluated.
Results: N= 1530, “Normal” group mean TBI 0.79, “Abnormal” group mean TBI 0.42, ROC- 0.61. There is statistical significance between both groups.
Conclusion: When no peripheral arterial disease is present as measured by non-invasive vascular laboratory criteria, a TBI value of 0.79 and above is considered “normal”. This is higher than values suggested in the literature, likely due the define normal to include the post-exercise ankle-brachial indices value. A TBI of 0.70 or 0.60 provides little discriminatory value. The utility of using TBI as screening tool for peripheral arterial disease requires further study.
Poster 6
Lower Extremity Fibromuscular Dysplasia: Clinical Manifestations, Diagnostic Testing, and Approach to Management
1Cleveland Clinic, Cleveland, Ohio, USA, 2Michigan State University, Michigan, USA, 3Cincinnati Children’s Hospital Medical Center, Ohio, USA
Background: Fibromuscular dysplasia (FMD), a disease well described in the renal and cerebrovascular arteries, also manifests in the lower extremity (LE) arteries.
Methods: This study reports on clinical presentation, vascular laboratory findings and treatment of patients with LE FMD at a single center.
Results: At our center, 100 of 449 FMD patients evaluated had imaging of the LE arteries, of which 62 were found to have LE FMD. The majority of patients were women (96.8%) and the average age at the time of diagnosis was 52 ± 11.3 years. All patients had FMD present in another vascular territory, most commonly in the renal (80.6%) and extracranial carotid arteries (79.0%). Most patients had multifocal FMD (95.2%) and bilateral LE disease (67.7%), with the external (87.1%), common (19.4%) and internal iliac arteries (11.3%) most commonly affected. Presenting symptoms of LE involvement included claudication (22.6%), atypical leg symptoms (14.5%), and dissection (6.5%), but most patients were asymptomatic (71.0%) and diagnosed after detection of a bruit on physical exam or incidentally by imaging. Beading, turbulent flow, velocity shifts and/or elevated velocities were noted in patients who underwent duplex ultrasound testing. Of those with treadmill testing, mean resting ABIs were 1.09 (right and left) and 7/27 patients (26.0%) had ABIs ⩽ 0.9 post-exercise. Nearly all patients were managed medically (98.4%) and only one patient required vascular procedures.
Conclusion: FMD less commonly affects the LE arteries and can present as claudication, atypical leg symptoms or dissection. Duplex ultrasound may be useful for diagnosis in patients with suspected disease. Most patients with LE FMD are asymptomatic and are managed medically.
Poster 7
Efficacy of Ankle-Foot Orthoses on Walking Ability in Peripheral Artery Disease: The AFO for PAD Trial I
1University of Montana; International Heart Institute; University of Colorado, Missoula, Montana, USA, 2International Heart Institute, Montana, USA, 3University of Montana, Montana, USA
Background: Intermittent claudication (IC) is a significant cause of walking limitation for patients with peripheral artery disease (PAD). Devices called ankle-foot orthoses (AFO) have been developed that store elastic energy in a footstep and release the stored energy during the propulsive phase of walking that assists calf muscle function. The aim of this study is to determine the efficacy of AFO on walking ability in PAD patients.
Methods: This is an ongoing open-label, non-randomized study recruiting fifteen PAD patients with calf IC. Patients complete two baseline exercise tests on a graded treadmill with and without the AFO. Patients then receive upfront advice to walk with the devices for 12 weeks. The primary outcome in the intent-to-treat analysis is change in peak walking time (PWT) at 12 weeks. Secondary outcomes include change in claudication onset time (COT), peak walking distance (PWD) from the 6-min walk test, and patient-reported outcomes via the Walking Impairment Questionnaire (WIQ) and Medical Outcomes Study Short Form 36-item (SF-36) questionnaire. Study staff are blinded to device usage or lack thereof during the exercise tests. Thus the interim analysis compares the average of baseline outcomes with and without the AFO to the average of post-12 week outcomes with and without the devices.
Results: The interim analysis (n=12) indicated patients had significantly greater PWT from baseline to 12 weeks (mean±SD: 8.3±5.5 to 10.3±5.4 min, p<0.05). There was an improvement (p<0.05) in COT (+2.6±2.5 min), PWD (+46.0±61.3 m), WIQ combined scores (+24.0±16.6%) and the SF-36 physical component score (+3.4±5.2%).
Conclusions: Preliminary results indicated PAD patients using AFO improved the primary outcome of PWT as well as other measures. AFO for PAD may have substantial clinical impact by attenuating IC in the calf muscles, thus allowing patients to increase total volume of physical activity in community settings.
Poster 8
Incidence and Outcomes of Patients with Depression Undergoing Endovascular Interventions for Peripheral Arterial Disease
1VA North Texas Health Care, Dallas, Texas, USA, 2VA NORTH TEXAS, Texas, USA, 3UTSW, Texas, USA
Background: Currently, there is limited evidence on the impact of treated depression on disease severity and clinical outcomes of patients with peripheral arterial disease (PAD).
Methods: We analyzed consecutive veteran patients enrolled in the XLPAD study (NCT01904851) undergoing endovascular revascularization of infra-inguinal peripheral arteries between July 2005 and October 2014. Depression and its treatment were established based on clinical information recorded in the electronic medical records.
Results: A total of 337 patients were analyzed; 88 (26.1%) had depression. Those with depression were younger (62.6±7.1 vs. 64.9±8.2 ;p=0.015) and white (75% vs. 61%; p=0.04) without significant gender differences.Smoking, diabetes mellitus and prior coronary artery disease were equally distributed between depressed and non-depressed patients. Depression was mostly treated with selective serotonin reuptake inhibitors (33%) and tricyclic antidepressants (14%). Patients with depression presented predominantly with claudication over critical limb ischemia (17% vs. 27%; both p=0.04), and predominantly underwent superficial femoral artery revascularization (94% vs. 79%; p=0.001). Lesion length was longer in patients with depression (136±84 vs. 123±67.1 mm; p=0.15) and also more heavily calcified (88% vs. 79%; p=0.05). Overall major adverse cardiovascular events and major adverse limb events at 12 months were similar in patients diagnosed with depression and non-depressed patients. (Figure 1).
Conclusions: Nearly a third of patients with PAD undergoing endovascular intervention are treated for depression. These patients are younger, predominantly white, present with longer and more heavily calcified lesions, and undergo superficial femoral artery revascularization. Their 12-month clinical outcomes are similar to that of non-depressed patients.

Poster 9
Comparison of the Clinical Outcomes of Medical Therapy, Thoracic Endovascular Aneurysmal Repair (TEVAR), and Surgical Management for Acute Complicated Type B Aortic Dissection (TBAD)
Philippine Heart Center, Quezon City, National Capital Region, Philippines
Introduction: Data on the best management option for type B aortic dissection are still insufficient. The general consensus is to treat stable, acute, uncomplicated TBAD medically followed by regular ambulatory visits and imaging, while interventional therapy is recommended for acute complicated TBAD. However, most Filipino patients are treated medically due to the high cost and risk of surgery. This study was conducted to evaluate the outcomes of acute complicated TBAD undergoing medical therapy alone; minimally invasive therapy (TEVAR) plus medical management; and surgical plus medical management.
Methods: This is a retrospective cohort study done at Philippine Heart Center involving 44 adult patients admitted from January 2010-June 2015 with a diagnosis of acute complicated TBAD. Of these patients, 32 were treated medically, 10 underwent surgery, and only 2 patients had TEVAR. Outcomes of interest include persistent pain, vascular complications, re-intervention from the initial management strategy, and death.
Results: Majority of the patients were male, hypertensive, and smokers. Only 34% had concomitant CAD; 20% of patients had aneurysm prior to the occurence of dissection. The overall mortality rate is 22.7%, higher for the interventional group in the first 30 days, but mortality is increased in the medical group in the long-term. The 5-year survival is estimated at 75% for conservative therapy, 90% for open surgical repair, and 50% for the endovascular approach. Major outcome occurred in 53% of patients in the medical and 33% of patients in the interventional group (p=0.06).
Conclusion: Open surgical repair is still the standard therapy in patients presenting with acute complicated TBAD. The suboptimal rates of morbidity and mortality of endovascular therapy cannot be concluded in the study because of the very small number of patients subjected to this treatment strategy. Prospective studies are therefore recommended to empower the small cohort studies to arrive at more reliable conclusions.
Poster 10
Short- and Long-Term Outcomes of Medical, Endovascular, and Surgical Treatment of Takayasus Arteritis
Philippine Heart Center, Quezon City, National Capital Region, Philippines
Introduction: Studies on the clinical profile and early and midterm outcomes of medical and/or surgical treatment of Filipinos with diagnosed Takayasus arteritis have been done by Abrena and Barcinas, et al. in the 1990s up to 2005; however, the long-term outcome, including that of recently developed endovascular treatment, has not been discussed. This study focuses on the late outcomes of treatment for Takayasus arteritis, and aims to improve the management of patients with such disease.
Methods: This is a retrospective cohort study done at Philippine Heart Center involving 39 adult patients admitted from January 2006-June 2015 with a diagnosis of Takayasus Arteritis. Of these patients, 26 were treated medically, 12 underwent surgery, and only 1 patients had endovascular therapy. Outcomes of interest include persistent symptoms, uncontrolled BP, vascular, neurologic, renal, cardiac complications, re-intervention from the initial management strategy and death.
Results:Majority of the patients were female, 31% were male, mean age of 38, with a diagnosis of Type V Takayasus arteritis. The mean duration of time from onset of symptoms to diagnosis is 2.8 years with mean duration of treatment of 7.8 years. Mostly were given steroids and anti-hypertensives. Most common risk factors are hypertension and dyslipidemia. 21% had pregnancy during the course of illness.Most common presentation is diminished pulse and aneurysm is the most common CT scan finding. The overall mortality rate is 18%, 10% in the short term and 8% in the long term, and mostly are patients on medical treatment.
Conclusion: Corticosteroids are still the cornerstone of medical therapy in the active phase of Takayasu arteritis. Late diagnosis and late initiation of treatment contributed to poor outcomes.
Poster 11
Outcomes in Patients with Critical Limb Ischemia (CLI) and Heart Failure (HF) with Preserved and Reduced Ejection Fraction (EF)
1UC Davis Medical Center, Sacramento, California, USA, 2UC Davis University, California, USA, 3University of Colorado Denver, Colorado, USA
Background: In patients with CLI, a history of HF predicts adverse 2-year outcomes. Longer-term outcomes stratified by EF are unknown.
Methods: We reviewed 381 patients with CLI undergoing lower extremity intervention from 2006-2013 in the UCD-PAD registry. HF was defined as documented presentation with signs and symptoms of heart failure. The baseline demographics, procedural data, and outcomes were retrospectively analyzed.
Results: One-hundred twenty (31%) patients had a prior diagnosis of HF, of which 55 had an EF of >40% (HFpEF), 46 had an EF of ⩽40% (HFrEF), and 19 had an unknown EF. Baseline demographics including, BMI (27±6 vs. 27±6 kg/m2, p=0.53), smoking status (67 vs. 68%, p=0.87), hypertension (85 vs. 85%, p=0.79), diabetes (60 vs. 70%, p=0.06), statin use (61 vs. 71%, p=0.06), aspirin use (61 vs. 69%, p=0.10), clopidogrel use (30 vs. 31%, p=0.79) and Rutherford class (p=0.27) were similar between the two groups (no-HF vs. HF). The HF group had a lower baseline EF (41±16 vs. 53±12%, p=0.001) and had higher rates of CAD (70 vs. 41%, p=0.001). The 5-year survival was higher in the no-HF group (43%) compared to both the HFpEF group (27%, HR 2.2 CI 1.4-3.5, p=0.0001) and the HFrEF group (24%, HR 2.8 CI 1.8-4.2, p=0.0001), with similar trends in the freedom from MACE rates. However, there was no difference in the 5-year survival between the two HF groups (HR 0.8 CI 0.5-1.3, p=0.32).
Conclusions: A history of HF, irrespective of the severity of left ventricular dysfunction, is a very poor prognostic indicator among patients with CLI undergoing endovascular intervention, with 5-year survival around 25%.

Kaplan Meier survival curve for CLI patients without HF vs. HF with EF>40% and HF with EF=40%
Poster 12
Discovering Peripheral Arterial Disease Cases from Clinical Notes Using Natural Language Processing
Mayo Clinic, Rochester, Minnesota, USA
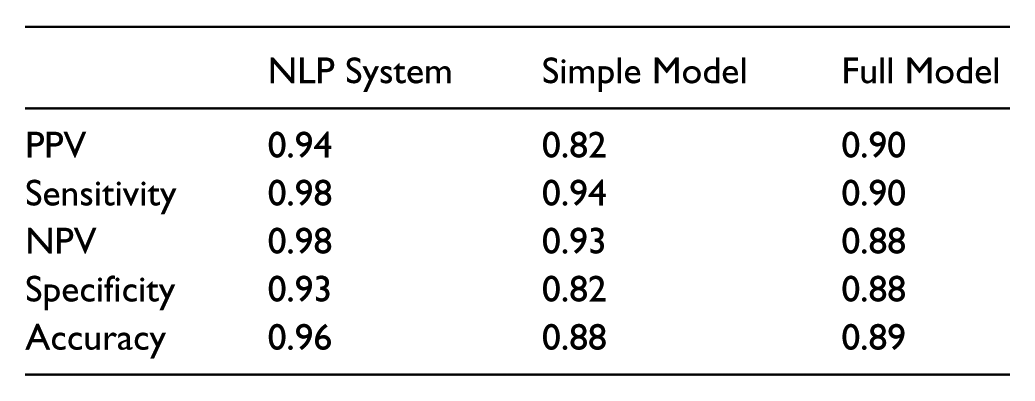
Electronic health records (EHR) are repository of patient information that can be mined to conduct clinical investigation from big data. Peripheral arterial disease (PAD) is a highly prevalent disease diagnosed by abnormal ankle-brachial index (ABI). However results of ABI reports may not be readily available, and clinicians may need to manually review EHR for identifying PAD patients. In addition, lack of automated processes for identifying PAD patients from EHR is an obstacle to conduct clinical studies using big data. We previously validated algorithms for PAD ascertainment using PAD-related ICD-9 diagnostic codes (simple model) and a combination of ICD-9 codes and procedural codes (full model). Natural language processing (NLP) has been successfully applied to many clinical applications such as genome-wide association studies and cohort identification. Previously we have applied NLP algorithms to ascertain PAD status from radiology reports. Our goal was to develop an NLP system for automated ascertainment of PAD cases from clinical notes. The system found concepts in text that match specified criteria and defined PAD status, based on available evidence from clinical notes. The system was validated by manual chart abstraction. The dataset processed by NLP system had 200 patients and 57,372 clinical notes in the Mayo EHR. There were 103 PAD cases (diagnosed by ABI) and 97 controls (with normal ABI). NLP system classified PAD cases from that data with high PPV, sensitivity, NPV, and specificity.
Conclusion: Our NLP system automatically ascertains PAD status from clinical notes in an accurate manner, and is independent of billing codes status. The NLP system will enhance capabilities for PAD research including big data, precision medicine, and epidemiologic studies, and facilitate clinical decision making at the point-of-care.
Poster 13
Preoperative Beta Blockers Reduce Perioperative Mortality in Open AAA Repair
Johns Hopkins Medical Institutions, Baltimore, Maryland, USA
Introduction: Current practice guidelines recommend use of certain preoperative medication in high risk for cardiac events patients undergoing open abdominal aortic aneurysm (AAA) repair. This aims to decrease perioperative cardiac morbidity and mortality in the at risk patient population. However, there is lack of evidence of the role preoperative medications and patient characteristics play in perioperative mortality of open AAA repair patients in large multispecialty national database outside clinical trials.
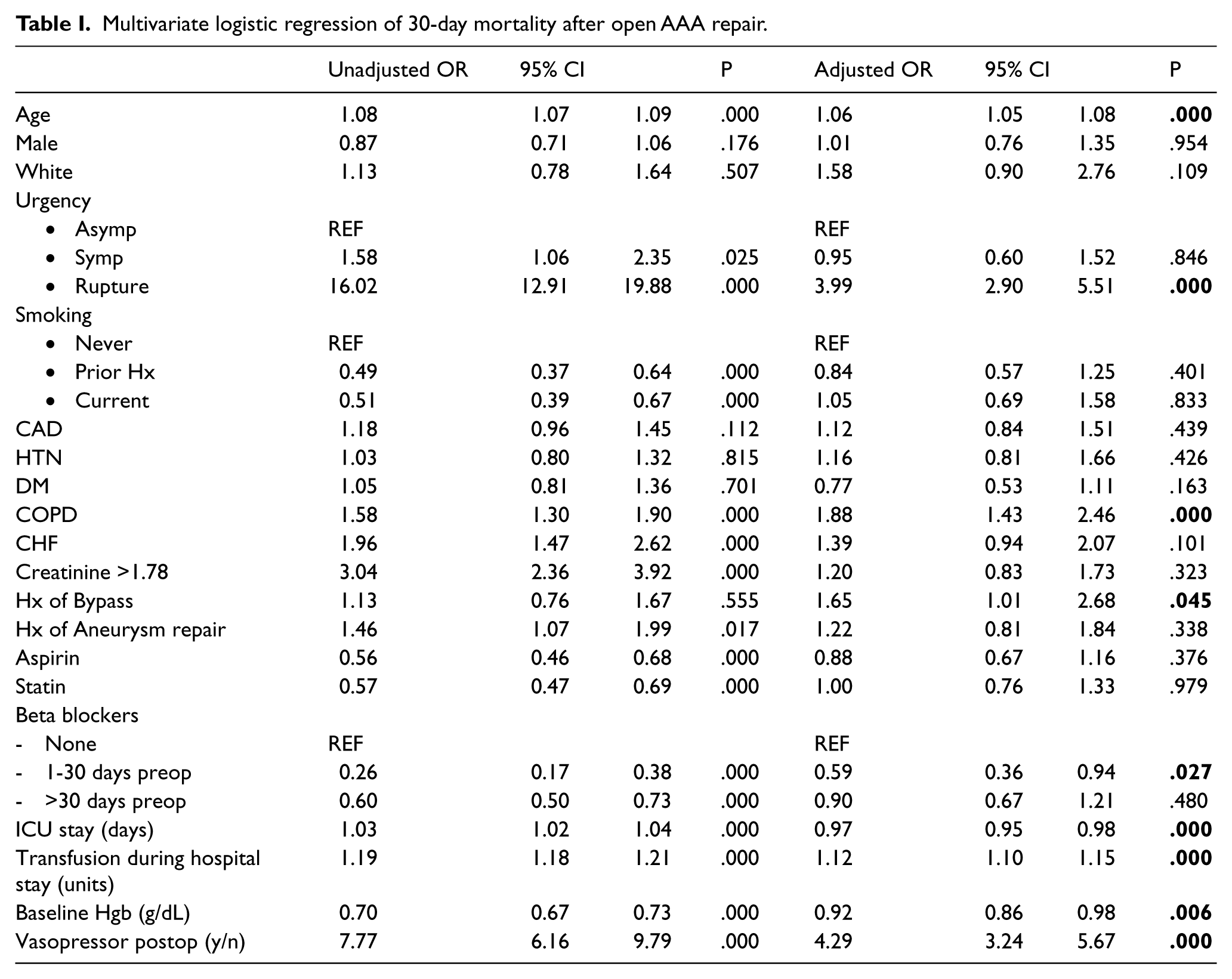
Methods: We analyzed all patients who underwent open AAA repair between 2003 and 2014 in the Vascular Quality Initiative. A multivariate logistic regression model was constructed to assess the effects of age, gender, diabetes, hypertension, coronary artery disease (prior myocardial infarction, stable angina, unstable angina), congestive heart failure (CHF), COPD, smoking, symptomatic status, renal and hemoglobin status, and pre-operative medications on 30-day mortality.
Results: A total of 5,765 patients underwent open AAA repair (mean age 70.0 years, and 74% male). Perioperative mortality for open repair was 8.9%. After adjusting for all Society for Vascular Surgery-recommended criteria of high cardiac risk (angina pectoris, prior myocardial infarction, prior CHF, renal insufficiency and diabetes mellitus), beta blockers use for 1-30 days preoperatively was associated with a 41% reduction in 30-day mortality (OR 0.59, 95%CI 0.36-0.94, P=0.027). A baseline hemoglobin status increase of one unit (g/dL) was associated with an 8% decrease in 30-day mortality (OR 0.92, 95%CI 0.86-0.98, P=0.006). Other significant predictors of 30-day mortality included COPD, history of arterial bypass, and postoperative vasopressor use (OR: 1.88; 1.65 and 4.29, respectively. All P<0.05).
Conclusion: Preoperative beta blockers use is associated with reduced 30-day mortality in all open AAA patients. Their role in the average cardiac risk patient population during open aneurysm repair should be studies prospectively.
Multivariate logistic regression of 30-day mortality after open AAA repair.
Poster 14
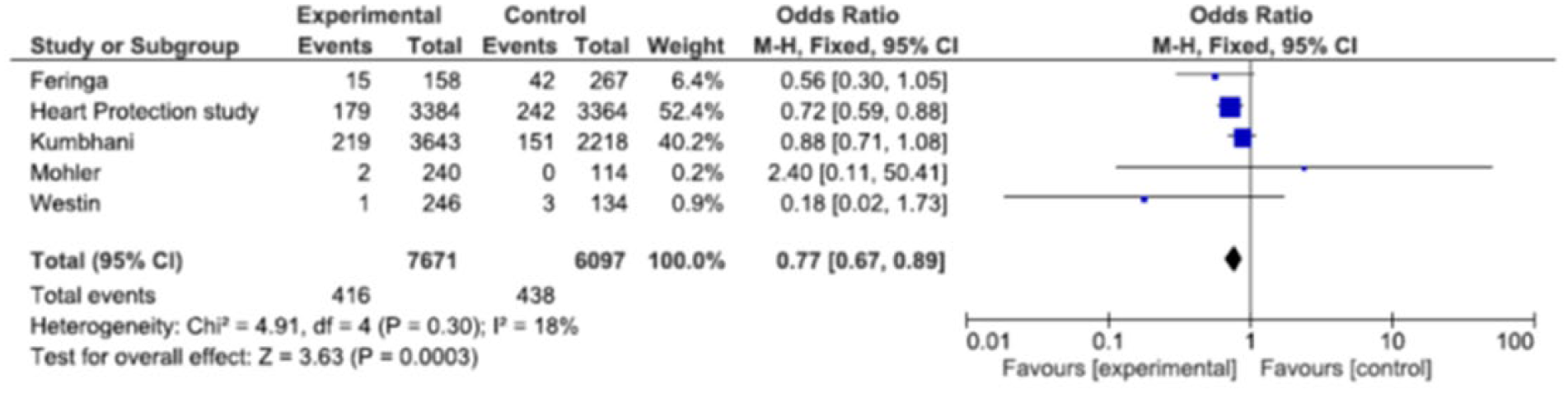
Statin Therapy Reduces the Incidence of Stroke, but Effect on Overall Cardiovascular Mortality Needs Further Evaluation in Patients with Peripheral Artery Disease
1Cleveland Clinic at Fairview Hospital, Ohio, USA, 2Cleveland Clinic Foundation, Ohio, USA, 3MetroHealth Medical Center, Ohio, USA
Background: Statin therapy has been shown to reduce stroke and cardiovascular mortality in patients with coronary artery disease (CAD); however, there is still a lack of conclusive data in patients with peripheral artery disease (PAD).
Methods: MEDLINE and EMBASE were searched from inception to December 2015 to look for the randomized controlled trials and retrospective and prospective studies that assessed the role of statin therapy in PAD population. Studies were only included if they reported incidence of cardiovascular mortality and/or stroke. Statistical analysis was performed using the comprehensive meta-analysis software RevMan version 5.3 to obtain the odds ratio (risk ratio) estimates and also the forest plot comparisons.
Conclusion: This meta-analysis shows that in patients with PAD, statin therapy significantly reduces the incidence of stroke, though its effect on overall cardiovascular mortality did not reach statistical significance. There is a need to design a large randomized controlled trial of statin therapy in PAD patients.

Imaging
Poster 15
Non-invasive Ultrasonic Differentiation of Carotid Plaque Tissue Based on Spectral Analysis of Radiofrequency Data
1Cleveland Clinic, Lerner Research Institute, Cleveland, Ohio, USA, 2Cleveland Clinic, Heart & Vascular Institute, Ohio, USA, 33Cleveland Clinic Lerner College of Medicine, Ohio, USA
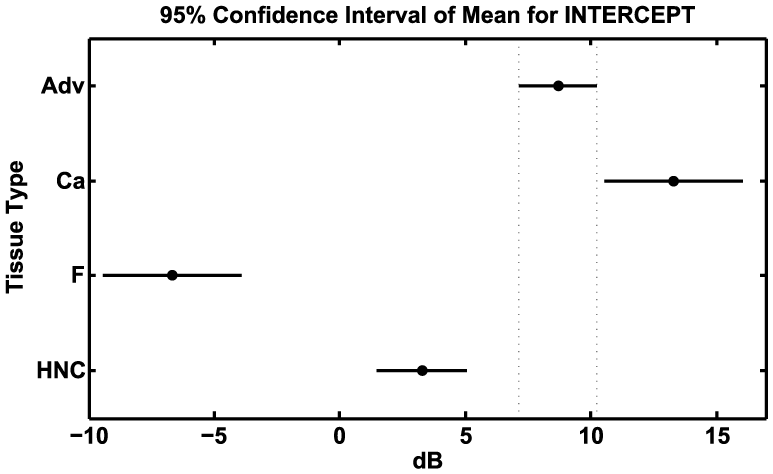
Introduction: Carotid artery atherosclerosis is the source of 15-20% of strokes, and many of these cases were asymptomatic. At this time, there is no point-of-care ultrasound-based screening tool capable of determining the risk of stroke for patients with asymptomatic carotid artery stenosis (CAS). Duplex ultrasound, MRA, and CTA reliably provide the location and severity of stenosis, but efforts to provide a measure of plaque composition have been limited. A reliable estimation of plaque composition may improve stroke risk assessment. Spectral analysis of ultrasonic radiofrequency (RF) signals was investigated as a tool for measuring carotid plaque tissue composition.
Methods: Through an IRB-approved clinical study, research ultrasound RF signals backscattered from carotid plaque were collected prior to a scheduled carotid endarterectomy (CEA). The RF signals were acquired using a Siemens S3000 system with Axius Direct software. Excised plaque was obtained for histological processing, and slides were matched to the in vivo RF data. These RF data were processed to compensate for attenuation, diffraction, and system effects. An estimate of the backscatter transfer function was obtained, and a linear fit was performed (3-7 MHz) to obtain spectral parameters: intercept, mid-band fit (MBF) and slope. Regions with homogenous tissue were defined for four categories (#): adventitia - Adv(114); calcium - Ca(32); hemorrhagic or necrotic core - HNC(74); and fibrous or fibro-fatty - F(32). ANOVA was performed with a Bonferroni correction and significance level of 0.05. Data were obtained from 19 CEA and 4 normal subjects. The means for all tissue types are significantly different for the intercept (Figure depicts the 95% confidence interval) while the means for the slope and MBF are distinct for a subset of types.
Results: Prior efforts to distinguish carotid plaque types have been limited to grayscale or intensity-dominated measures. The results indicate that including spectral parameters increases tissue differentiation as compared to intensity based measures alone.
Poster 16 - Withdrawn
Poster 17
Association of Carotid Arterial Strain Measured with Speckle Tracking and Echocardiography Derived Cardiac Parameters
1Baylor College of Medicine, Houston, Texas, USA, 2Michael E. DeBakey Veterans Affairs Medical Center, Texas, USA, 3Ben Taub General Hospital, Texas, USA
Introduction: Strain measures of carotid stiffness with echo-speckle-tracking (EST) has been shown to be associated with cardiovascular disease risk factors. The relationship between measures of carotid arterial strain (CAS) and echocardiographic parameters, however, has not been described.
Objective: The aim of our study was to examine the relationship between CAS measured with EST and echocardiographic parameters.
Methods: EST was used to measure peak CAS of both common carotid arteries in 51 diabetic and 49 hypertensive patients. Global circumferential CAS values were averaged over 2 cardiac cycles for each carotid artery. Bilateral CAS values were averaged for each patient. Data from clinical echocardiograms performed on the same day were collected, consisting of left ventricular (LV) ejection fraction, mitral E and A inflow velocities, mitral lateral and septal e’ tissue velocities, LV outflow tract (LVOT) diameter and LVOT velocity time integral (VTI). The diastolic parameters of averaged e’ tissue velocity, E/A ratio and respective E/e’ ratios were derived.
Results: Linear regression (Table) and Spearman’s rank correlation (p-values) performed on unadjusted data in diabetics both showed a significant relationship between CAS and mitral E (p=0.046), LVOT VTI (p=0.031) and E/e’ septal ratio (p=0.041). After adjusting for ultrasound probe type, age, race, gender, systolic and diastolic blood pressures, and heart rate, a significant relationship between LVOT VTI and CAS persisted (p=0.03). No relationships were seen between cardiac parameters and CAS in hypertensives.
Conclusions: Some echocardiographic parameters including mitral E, E/e’ septal ratio and LVOT VTI are associated with carotid arterial strain in diabetics. Carotid stiffness measures in diabetics may more closely reflect impairment in cardiac function than in non-diabetic hypertensives. These findings suggest a more systemic cardiovascular pathophysiology in this population.

Clinical Science/Epidemiology: Other
Poster 18
Vascular Surgery Subspecialty Referral Patterns in a Regional Military Healthcare System: An Attempt to Improve the Process
Walter-Reed National Military Medical Center, Bethesda, Maryland, USA
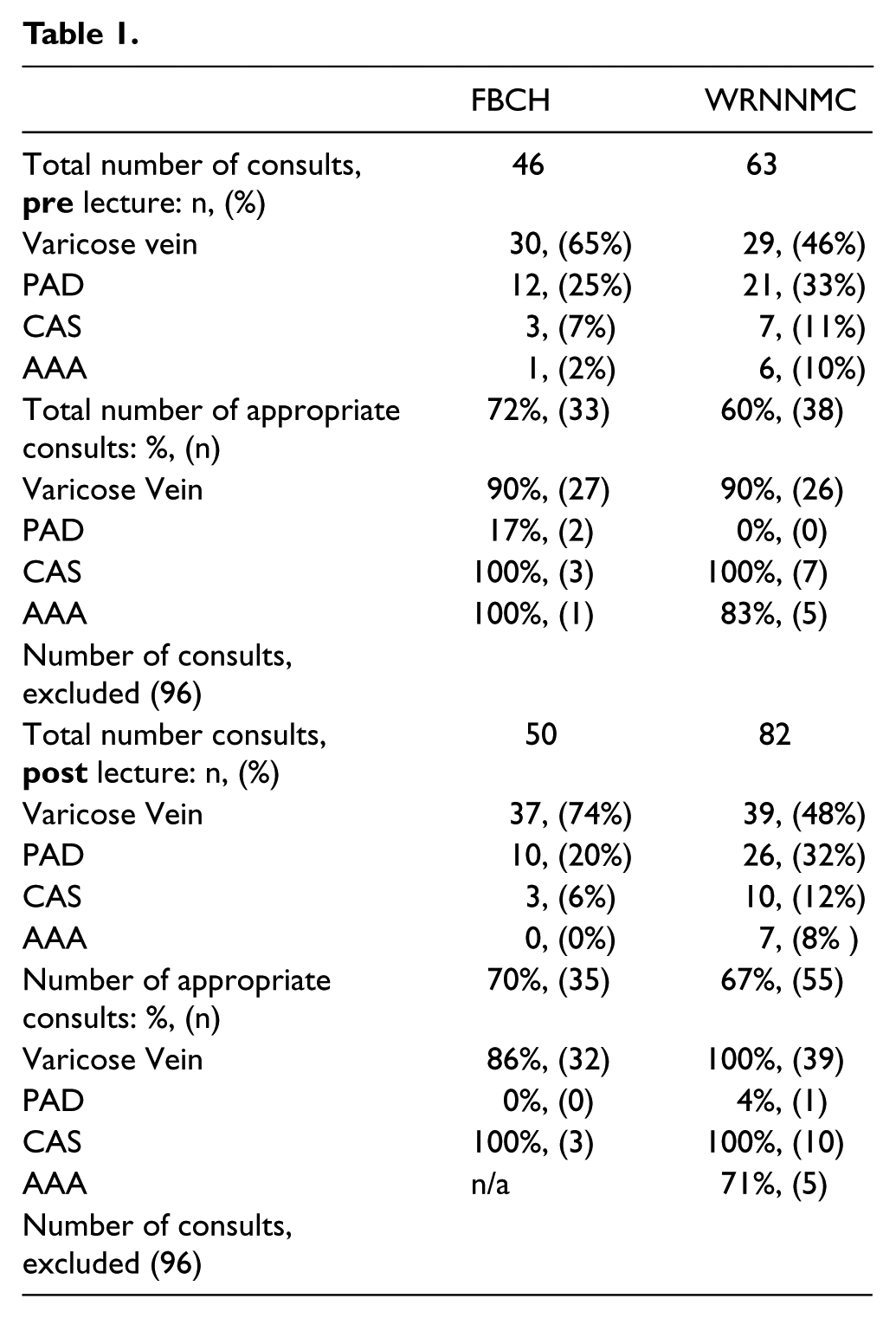
Objective: We report the results of an education program directed at improving the referral pattern for vascular patients from two large primary care clinics in the military health care system.
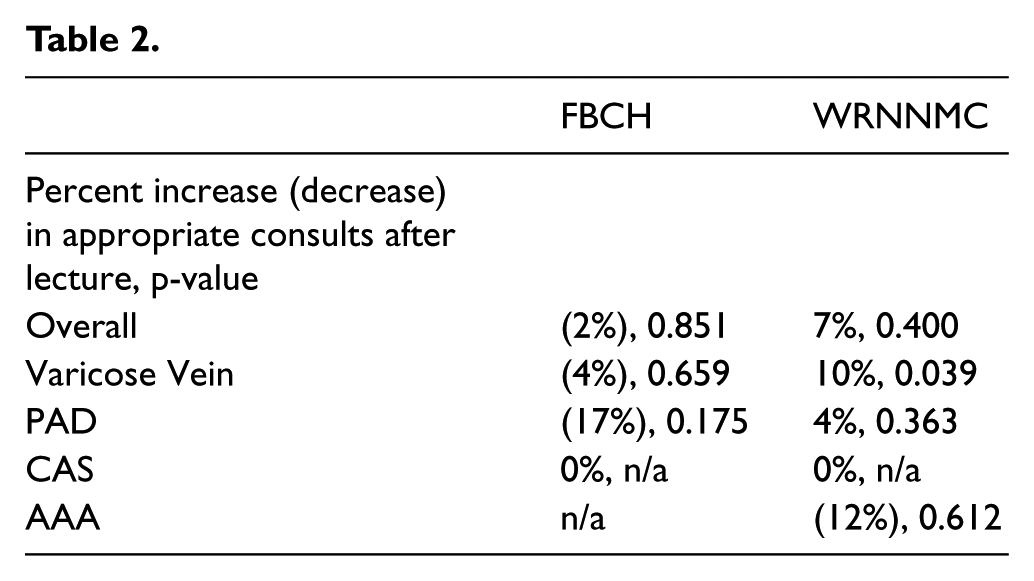
Methods: We retrospectively reviewed the records of all patients referred from two primary care clinics to the vascular division, two months before a single lecture and two months after. Four diseases were examined: abdominal aortic aneurysm, carotid artery stenosis, peripheral arterial disease, and varicose veins.
Results: A total of 205 consults (pre) and 228 consults (post) were examined from the two referring clinics, of which 109 and 132, respectively, met the criteria for inclusion in our study. Prior to the lecture, our study criteria classified 72% and 60% of the referrals from FBCH and WRNMMC respectively, as appropriate. Overall, a 2% decrease in appropriate consults was seen at FBCH after the lecture, while a 7% increase in appropriate consults was seen at WRNMMC, neither was statically significant. When looking at the specific disease processes, only the varicose vein consults from WRNMMC showed a statically significant improvement after the educational lecture (increase of 10%, p=0.039). All other categories did not show a significant change. Of the 25 PAD patients from both clinics referred without an ABI in the pre-lecture period, 72% did not receive a diagnosis of peripheral arterial disease after examination by the vascular surgeon.
Conclusion: There are opportunities to improve the referral patterns between the primary care system and the vascular subspecialists within a regional military health system. One of which is the use of appropriate testing such as ABI before initiating referral.
Poster 19
Strange Connections: Case Series of Coronary Arterial-Venous Fistulas Seen at the Philippine General Hospital
Philippine General Hospital, Manila, Philippines
Introduction: Coronary vascular fistula is rare. It can be congenital or acquired abnormality with an incidence of 0.3-0.8%.
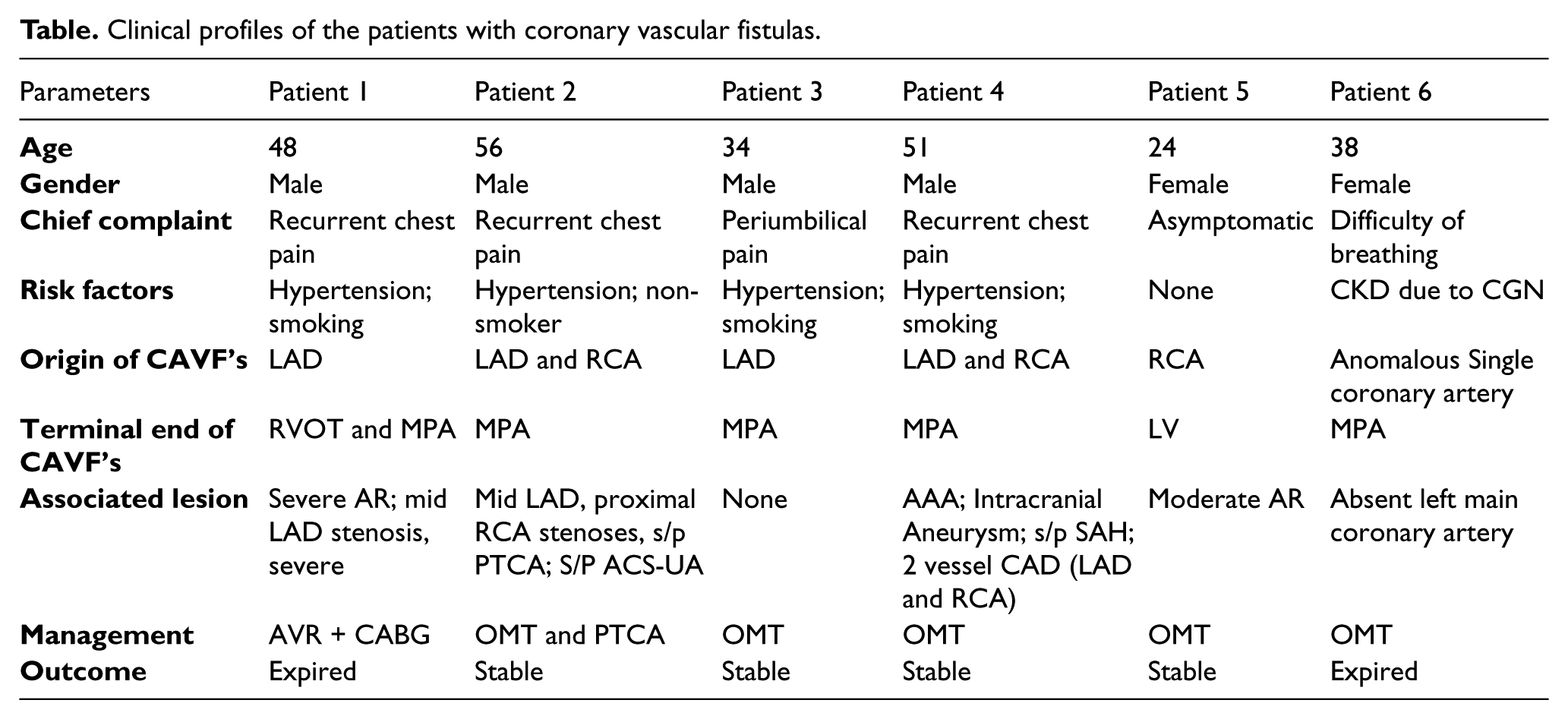
Clinical Presentation: The six patients were middle-aged, 24-56 years old, including four males and two females. Four presented with recurrent chest pain; the 24-year-old female was asymptomatic, and the 38-year-old female had difficulty of breathing. All four males were hypertensive; three were smokers. The fistulas were seen on coronary angiogram. Only one patient underwent surgery but succumbed due to massive blood loss. The other 4 patients were stable, the 6th patient died of hypovolemic shock secondary to alleged intra-abdominal ruptured vascular aneurysm.
Diagnostics: All six patients underwent coronary angiography, which characterized the location and drainage of the fistula and the associated findings. Patient one underwent CT angiogram for further evaluation because his fistula drained to two terminal ends, making his case unique and structurally complex. Patient 1, 5, and 6 had cardiomegaly on chest X-ray, and Patient 1 and 5 had severe and moderate aortic regurgitation on transthoracic echocardiogram, respectively. Patients 1, 3, 4, and 6 had LVH by voltage in their 12-lead ECG, while patient 2 and 3 had non-specific ST-TW changes. Only patient 1 showed first degree AV block.
Treatment: Patient 1 underwent AVR and coronary artery bypass, however he expired. The other three male patients are in optimal medical therapy for chronic hypertension and coronary artery disease; patient 5 is under surveillance. Patient 6 expired due to volume loss. All four were advised surgical intervention and aggressive lifestyle and dietary modifications.
Significance: Due to its rarity and complexity, coronary vascular fistulas remain a challenge. It requires optimal use of multiple diagnostic imaging and multidisciplinary management. In this series, atherosclerosis and hypertension were common risk factors, highlighting the importance of its vascular sequelae other than the usual coronary artery disease.
Clinical profiles of the patients with coronary vascular fistulas.
Poster 20
Effect of Exercise Training on Immune Dysfunction in Patients with Stage 3-4 Hypertensive Kidney Disease
1University of Illinois at Chicago, Chicago, USA, 2University of Minnesota, USA
Introduction: The uremic milieu present in patients with kidney disease results in immune system dysfunction leading to chronic inflammation and frequent infections. Exercise training improves immune system function in other chronic disease populations. We therefore conducted a pilot study to test the hypothesis that exercise training would improve immune system markers associated with deteriorating kidney function and CVD in patients with CKD.
Methods: Blood samples for CBC with differential were obtained in a subsample of patients with stage 3-4 hypertensive kidney disease who took part in a larger exercise training study. Participants were randomized to either a 12-week, 3x-week, 30-minute moderate intensity exercise training program (n=8) or usual care (n=8).
Results: ANCOVA adjusting for baseline exercise and kidney function indicated that exercise significantly reduced monocyte [-0.23 (0.5), p=0.02] and neutrophil [-1.9 (0.3), p=0.02] counts compared to usual care (mean diff -0.21, 95% CI -0.4 to -0.04, and -1.4, 95% CI -2.5 to -0.3, respectively). Percent lymphocyte count was increased in the exercise group [6.4% (2.1), p=0.05], but absolute lymphocyte count did not reach statistical significance. Exercise significantly reduced monocyte/HDL ratio (p=0.03), with a trend for reduction in neutrophil/lymphocyte ratio (p=0.07). There were no statistically significant differences between groups in eosinophil or basophil counts.
Conclusion: Exercise training favorably modulates markers of immune dysfunction that are associated with chronic inflammation, deteriorating kidney function, and increased CVD risk in patients with hypertensive kidney disease. Future studies are needed to investigate the effect of exercise on immune system subpopulations, cell activation, and signaling.
Thrombosis and Hemostasis
Poster 21
Treatment of Massive Pulmonary Embolism During Cardiopulmonary Collapse and Pulseless Electrical Activity with Low-Dose Systemic Thrombolysis
1Arizona Cardiovascular Consultants & Vein Clinic, Mesa, Arizona, USA, 2A.T.Still University, Arizona, USA
Background: Development of pulseless electrical activity (PEA) and cardiopulmonary collapse due to massive pulmonary embolism ( PE) portends a very poor prognosis. No established guidelines for the treatment of such patients exist because almost always it is a fatal disease. We report on 19 patients who were successfully treated with low dose thrombolysis with an excellent clinical outcome.
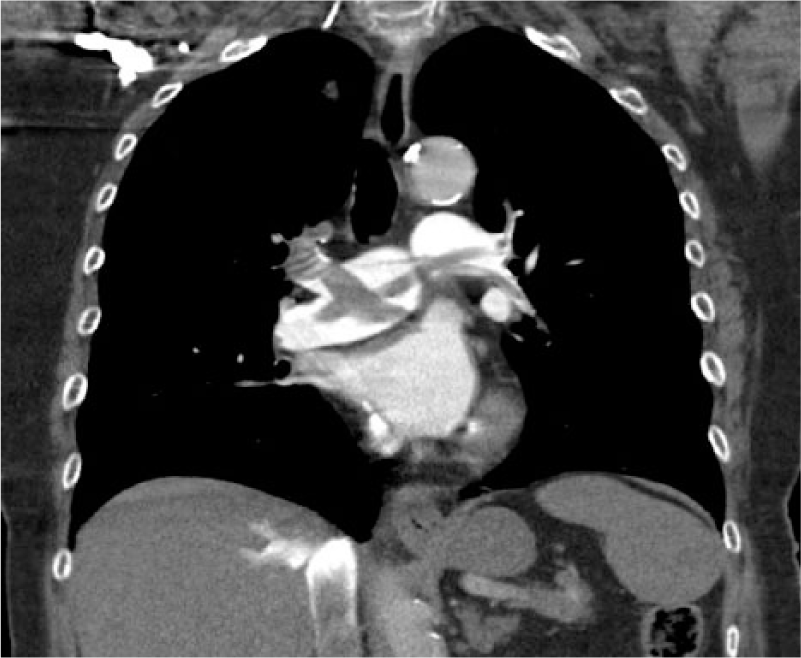
Methods: We treated 19 consecutive patients who had sustained PEA and cardiopulmonary collapse due to massive PE with tissue plasminogen activator (tPA). A total of 50 mg of tPA was given in 1 minute while cardiopulmonary resuscitation (CPR) was ongoing. In 14 patients, the diagnosis was established with computed tomographic pulmonary angiography (CTA) (Figure); in 3 patients, it was made with evidence of large clot in the right heart; and in 2 patients, an initial diagnosis of PE was made (severe right-sided chamber enlargement and pulmonary hypertension), which was later confirmed with CTA. Heparin was given at a bolus of between 2000-5000 units, and the patient started on an initial maintenance drip of 10 U/kg/h as soon as tPA was given.
Results: In all patients, PEA changed to sinus tachycardia and pulse reestablished. Almost immediate spontaneous circulation and hemodynamic stability was achieved within the first 15 min of tPA administration. Despite restoration of spontaneous circulation, 1 patient developed permanent hypoxemic encephalopathy due to prolonged CPR and late arrival. All other 18 patients recovered fully. There was no minor or major bleeding, despite chest compression.
Conclusion: We conclude that systemic administration of 50 mg of tPA in one minute while CPR is ongoing is highly safe and effective in the treatment of PEA and cardiopulmonary collapse due to massive PE, with restoration of spontaneous circulation and hemodynamic stability within a short period of time.
Poster 22
Noninvasive Thrombolysis Using Microtripsy in a Porcine Model
University of Michigan, Ann Arbor, Michigan, USA
Background: Histrotripsy is a novel therapeutic technique that uses ultrasound generated from outside the body to create controlled cavitation in a target tissue, and fractionates it into acellular debris. We have developed a new histotripsy approach, termed microtripsy, to improve targeting accuracy and to avoid collateral tissue damage. This in vivo study evaluates the efficacy and safety of microtripsy thrombolysis in a deep vein thrombosis (DVT) model.
Methods: Acute thrombi were formed in the left femoral veins of pigs (~35 kg) by occluding the vessel using two balloon catheters and infusing with thrombin. Guided by ultrasound imaging, microtripsy thrombolysis treatment was conducted in 14 pigs. 10 pigs were euthanized on the same day (acute) and 4 at 2 weeks (subacute). To evaluate the vessel damage, 30-min free-flow treatment (no thrombus) in the right femoral vein was also conducted in 8 acute pigs.
Results: Blood flow was restored or significantly increased after treatment in 13 out of the 14 pigs. One treatment was not effective due to a technical issue with clot formation. The flow channels reopened by microtripsy had a diameter up to 64% of the vessel diameter (~6 mm). The average treatment time was 16 minute per cm-long thrombus. Minor hemolysis was observed in both thrombolysis and free-flow treatments. Histology showed no vessel damage and only microscopic hemorrhage outside the veins for the free-flow treatments with nothing abnormal observed for the subacute treatments.
Conclusion: Microtripsy is a safe and effective treatment for DVT in a porcine model. Further studies are warranted to study the role of this promising noninvasive thrombolytic method in human subjects.

Poster 23
The Predictive Ability of Various Risk Scores for Bleeding in Warfarin-Treated VTE Patients
1University of Michigan, Ann Arbor, Michigan, USA, 2William Beaumont Hospital, Michigan, USA, 3Huron Valley Sinai Hospital, Michigan, USA, 4Henry Ford Hospital, Michigan, USA, 5Spectrum Health, Maryland, USA, 6Hurley Medical Center, Michigan, USA
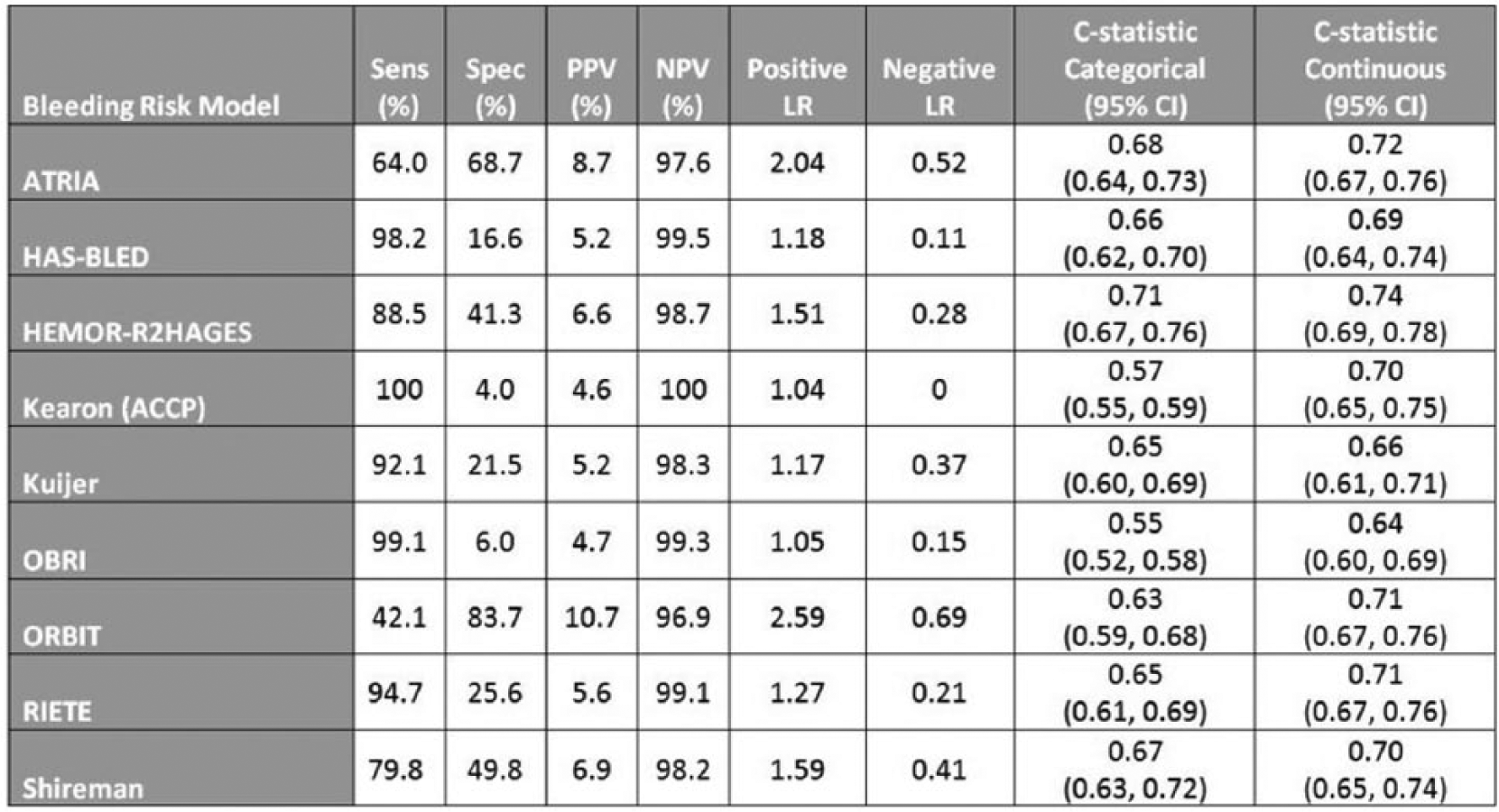
Background: Multiple risk assessment models (RAM) are available to estimate the risk of bleeding in warfarin-treated patients with atrial fibrillation (AF) or venous thromboembolism (VTE). There are relatively little comparative data in patients with VTE. We sought to quantify the predictive value of 9 RAMs.
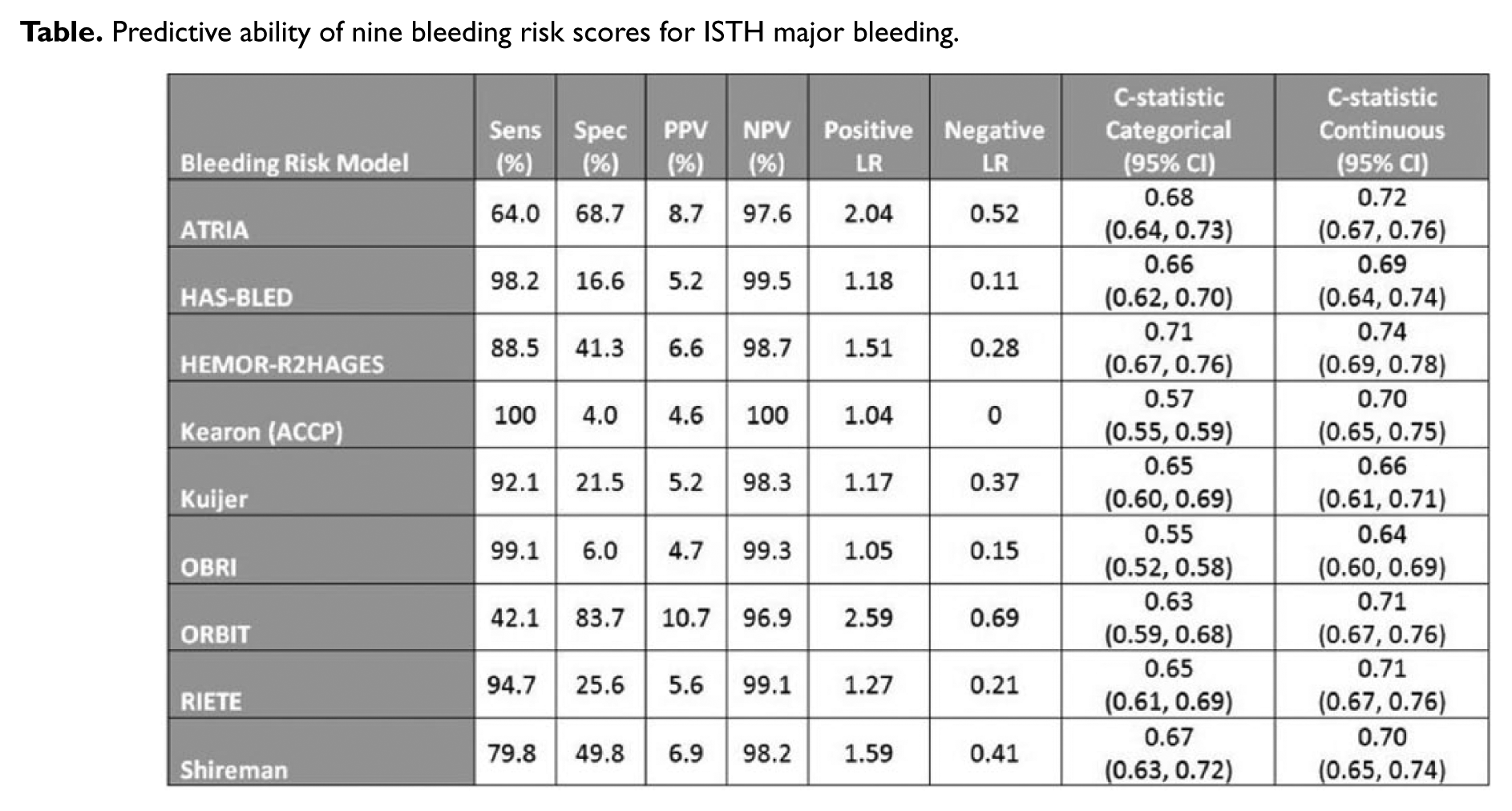
Methods: The Michigan Anticoagulation Quality Improvement Initiative (MAQI2) collaborative follows an inception cohort of warfarin-treated patients. Using chart abstracted data, individual bleeding risk scores and rates of International Society of Thrombosis and Hemostasis (ISTH) major bleeding were assessed for MAQI2 patients, with an INR goal of 2-3 for treatment of VTE and at least 3 months of follow-up. Predictive test characteristics were calculated as well as c-statistics for continuous and categorical (low vs. intermediate/high) scores.
Results: Between 2009 and 2015, 2567 VTE patients experienced 114 major bleeding events. Mean age was 59.6±16.7 years, with 53.3% of the cohort being female. Mean TTR was 53% and mean follow-up was 1.23±1.27 years. Predictive characteristics of the RAMs are reported in the Table.
Conclusion: Bleeding RAMs developed for patients with AF or VTE had a modest ability to predict major bleeding in our cohort of warfarin-treated VTE patients. With low PPV, none of the models were able to consistently predict bleeding among those patients with intermediate/high scores. The high NPV of low-risk scores allowed for a reasonable degree of certainty in excluding patients at risk of a major bleeding event. Overall, such scores may reassure providers regarding the risk of warfarin use in low-risk patients, though their poor PPV precludes consistent prediction of major bleeding in intermediate/high-risk patients.
Predictive ability of nine bleeding risk scores for ISTH major bleeding.
Poster 24
Utility of a Clinical Risk Score to Limit Therapeutic Anticoagulation in Suspected Cases of Heparin-Induced Thrombocytopenia (HIT) After Cardiac Surgery
University of Virginia, Charlottesville, Virginia, USA
Background: Heparin-induced thrombocytopenia (HIT) in cardiac surgical patients has a high rate of mortality and complications. Empiric therapeutic anticoagulation while awaiting confirmation of suspected HIT must be balanced against the risk of postoperative hemorrhage. We evaluated risk stratification methods to diagnose HIT in this population.
Methods: Patients undergoing cardiac surgery with cardiopulmonary bypass from 2008-2014 in our institutional Society of Thoracic Surgeons (STS) database were analyzed. Platelet factor 4 antibody (PF4) and serotonin release assay (SRA) results were reviewed. Patients were stratified as low or high clinical suspicion using platelet trend, cardiopulmonary bypass duration, and time since surgery as described by Louet, et al. The predictive value of the clinical risk score and PF4 results were compared to SRA results.
Results: Of 4829 patients, 263 (5.5%) had laboratory assays for HIT; 152 patients underwent SRA testing, and only 28 (18%) and 20 (13%) were PF4 and SRA-positive, respectively. The Louet score classified 88/152 (58%) of patients as high risk. For PF4 (-) and low clinical risk, 94% of patients are SRA (-). The positive (PPV) and negative (NPV) predictive values of the clinical score and PF4 assay are shown in Figure 1.
Conclusion

Poster 25
Secular Trends in Incidence and Mortality of Thromboembolism: The AB-VTE Population-Based Study
University of Alberta, Edmonton, Canada
Background: Venous thromboembolism (VTE) is a major cause of morbidity and mortality, and comprehensive studies profiling the epidemiology and pattern of health services use are needed. In this study we provide contemporary estimates of VTE incidence and case fatality over the past decade.
Methods: We developed a population-based VTE dataset by linking six administrative health databases in Alberta, Canada from April 1, 2002, to March 31, 2012. We defined acute symptomatic cases using a validated algorithm, and used Poisson regression to model annual VTE counts.
Results: We identified 31,656 cases of acute symptomatic VTE between April 1, 2002, and March 31, 2012. The age and sex adjusted incidence rate of VTE was 1.38 (95% CI: 1.37, 1.40) per 1,000 person-years. For pulmonary embolism (PE), it was 0.38 (95% CI: 0.36, 0.40) per 1,000 person-years, and for deep vein thrombosis (DVT) it was 1.0 (95% CI: 0.99, 1.1) per 1,000 person-years. The adjusted model showed no significant change in the incidence of VTE during the study period. The 30-day case fatality rate of VTE was 2.0% (95% CI: 1.89, 2.21), and was almost doubled in patients with PE 3.9% (95% CI: 3.50, 4.33). The 1-year case fatality was 9.2% (95% CI: 8.88, 9.52) for VTE, and 12.9% (95% CI: 12.2, 13.6) for patients with PE. The case fatality increased with increasing subject age. The 1-year and 5-year survival after first acute VTE were similar in patients with unprovoked and provoked events. However, in patients with cancer-associated thrombosis, the 1-year and 5-year survival was 66% (95% CI: 64.71% to 67.29%) and 46% (95% CI: 43.28% to 48.72%) respectively.
Conclusion: The incidence of acute VTE remained unchanged over a 10-year period. However, the case fatality of VTE is substantial.
Poster 26
Comparing Risk Predicting Models and High-Risk Features in Pulmonary Embolism to Evaluate Short-Term Mortality: A Tertiary Care Center Experience
University of Virginia, Charlottesville, Virginia, USA
Background: The heterogeneity seen in pulmonary embolism (PE) outcomes, ranging from no symptoms or complications to sudden death, necessitates a method to appropriately risk-stratify these patients. Studies have correlated early (30-day) mortality in PE based on high-risk features including certain clinical features, imaging findings, and laboratory biomarkers of right ventricular strain or ischemia.
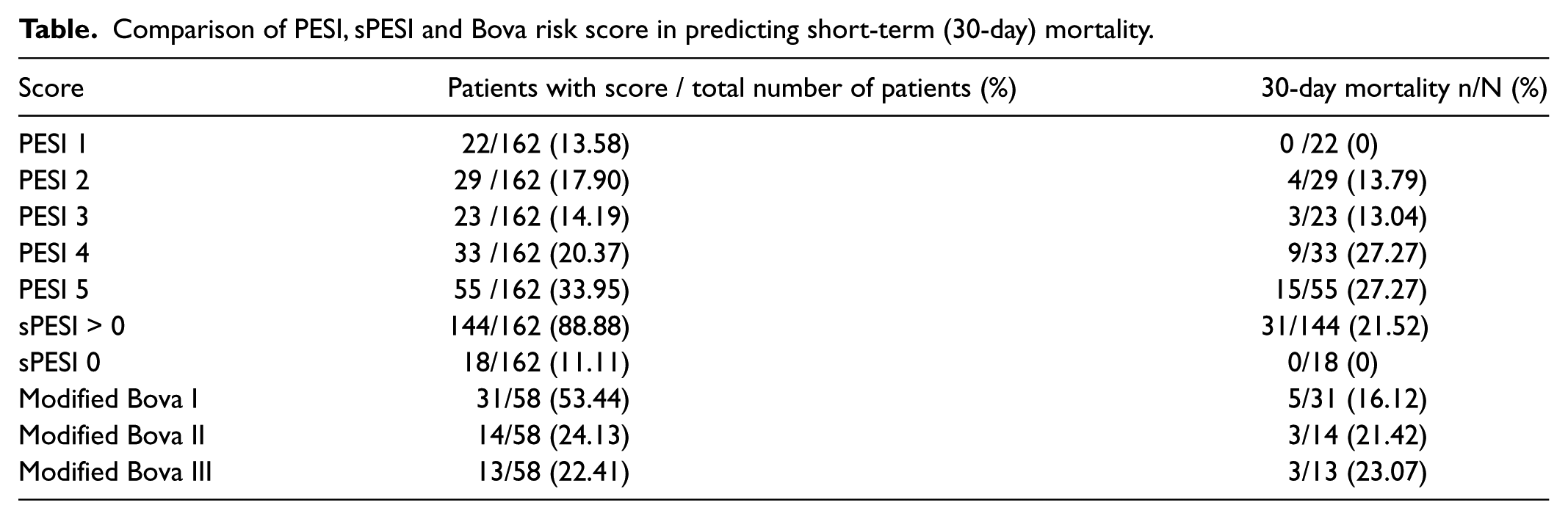
Methods and Results: We sought to retrospectively collect these high-risk clinical, laboratory, and imaging parameters among patients admitted to the University of Virginia from January 2013 to July 2015. The initial analysis of 162 patients admitted between January 2015 to July 2015 is as follows: 53.70% (87/162) were men, mean age was 60.50 years (range: 19-94), 62.34% (101/162) were unprovoked PE’s, and 30-day mortality was 19.13 % (31/162). PE in the setting of malignancy carried a particularly high mortality of 30%. Mortality by stratifying to the three scoring systems: pulmonary embolism severity index (PESI) score, simplified PESI (sPESI) and modified Bova score are shown in the Table. Patients with PESI score of 1 or sPESI of 0 had a 0% mortality. Even PESI scores 1, 2, and 3 combined had a negative predictive value of 90.54% for mortality. High PESI of 4 and 5 and modified Bova III correlated with increased mortality.
Conclusions: Risk scoring systems such as PESI and sPESI on initial analysis appear to risk-stratify patients adequately, especially low risk patients. Ongoing data collection of the remaining patients (~500) will likely provide more data for adequate validation and comparison of risk scores, as well as further assessment of cardiac biomarker and imaging of right ventricular strain in predicting early mortality.
Comparison of PESI, sPESI and Bova risk score in predicting short-term (30-day) mortality.
Venous Disease (Other than Thrombosis)
Poster 27
A Chronic Venous Disorder Wearable Sensing Platform
1University of California, Davis, Davis, California, USA, 2UC Davis Vascular Center, Davis, California, USA
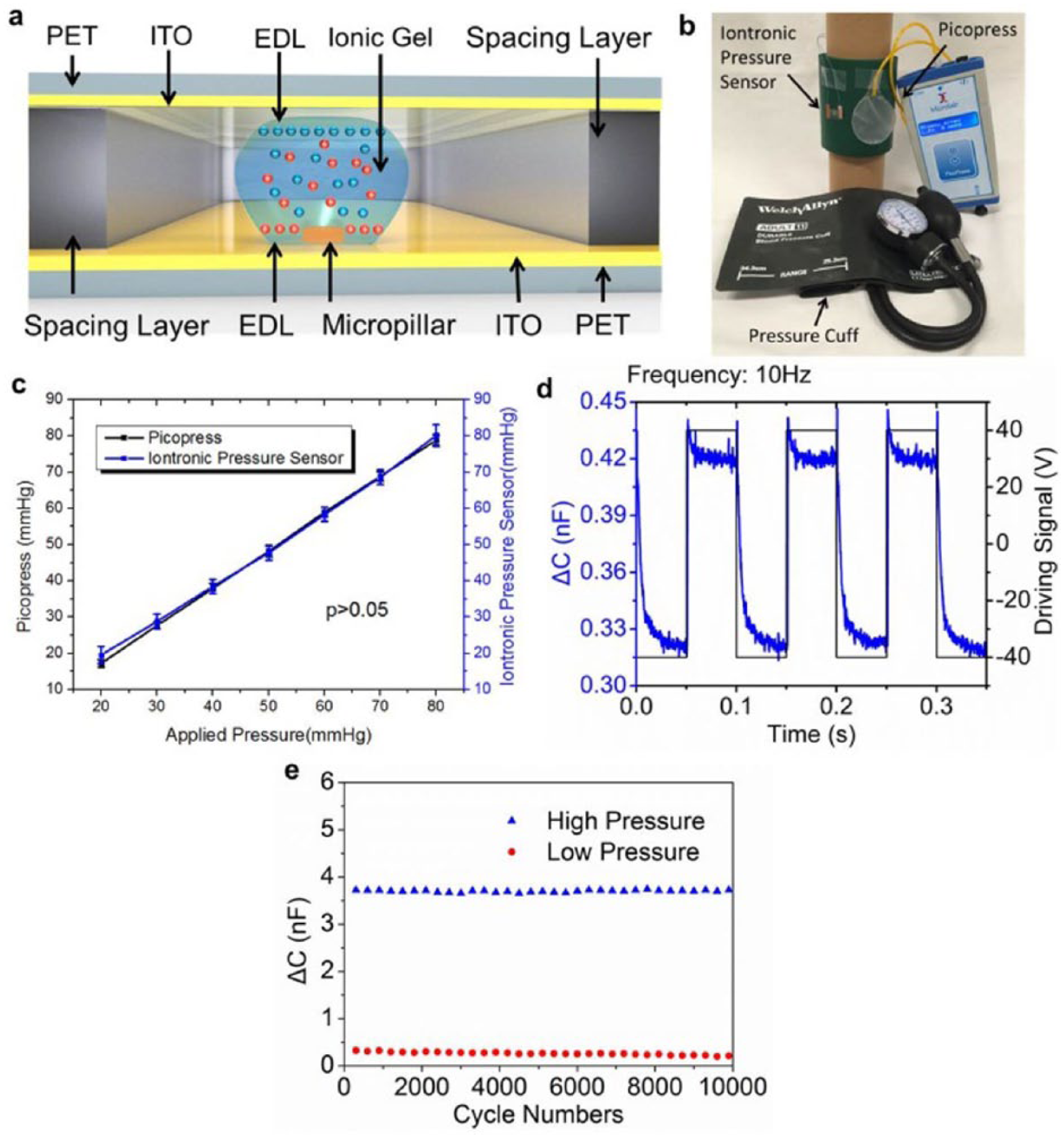
Objectives: Achieving therapeutic interfacial pressure via compression therapy is the cornerstone of chronic venous disorder management. This project intends to a) use iontronic pressure sensing technology to obtain interface pressure, and b) compare device performance with Picopress™.
Method: The study was conducted in May 2015. The iontronic pressure sensor was composed of ionic gel droplet sandwiched between two polyethylene terephthalate (PET) membranes (Figure 1a). Under external pressure the PET deformed, leading to the expansion of ionic gel droplet and change in capacitance. This was captured by a readout circuitry, which consisted of an analog front, microcontroller and Bluetooth 2.0 transmission module for data acquisition and wireless transmission. A manometry device Picopres® (MediGROUP, Australia) via a pressure cuff mannequin model was used for device characterization and comparison (Figure 1b). Two-sample t-test was used for statistical analysis.
Results: Iontronic pressure sensor sensitivity (0.046nF/mmHg) was characterized as capacitive change (ΔC) versus pressure load (P) with exact linearity up to 80 mmHg. Two-sample t-test demonstrated no difference between the two systems (Figure 1c) (p>0.05). Device mechanical response was in the millisecond range (Figure 1d), with repeatability less than 2% variation during 10,000 testing cycles (Figure 1e).
Conclusion: The novel iontronic pressure sensor demonstrated high sensitivity to interface pressure change with minimal repeatability variation, and was comparable to the gold standard, Picopress®.