
Abstract
Introduction:
Venous thromboembolism (VTE) is a common, potentially life-threatening condition. To improve care, a multidisciplinary Adult Outpatient Thrombosis Service (TS) was implemented in one region of Newfoundland and Labrador, Canada. This study evaluated the clinical effectiveness of the TS compared to usual care (UC) for patients with newly diagnosed VTE.
Method:
We conducted a retrospective cohort study of adults with objectively confirmed VTE between 2017 and 2019. Patients managed by the TS were compared to those receiving UC. Data were obtained from linked administrative and clinical databases. Propensity score matching was applied to control for confounding. Primary outcomes included recurrent VTE and major bleeding. Secondary outcomes were all-cause hospitalizations, emergency department visits, and all-cause mortality. Incidence rate ratios (IRR) and 95% CIs were calculated using Poisson regressions; Cox models were used for mortality.
Results:
A total of 1499 patients were included (TS: n = 464; UC: n = 1035). The TS group experienced significantly lower rates of adverse outcomes. VTE recurrence (IRR = 0.65, 95% CI: 0.29–0.67, p = < 0.001) and major bleeding (IRR = 0.33, 95% CI: 0.19–0.53, p = 0.011) were significantly reduced in the TS group, as were hospitalizations (IRR = 0.76, 95% CI: 0.64–0.92, p = 0.009). No significant difference was found in emergency department visits (IRR = 1.02, 95% CI: 0.79–1.32, p = 0.848). All-cause mortality was also lower (HR = 0.62, 95% CI: 0.48–0.81, p = 0.0004).
Conclusion:
Management of VTE within a multidisciplinary TS was associated with significantly lower rates of complications, hospitalizations, and all-cause mortality compared to UC. These findings suggest that a structured, specialized outpatient thrombosis care model may be associated with favorable clinical outcomes in real-world settings.
Keywords
Introduction
Venous thromboembolism (VTE), which encompasses deep vein thrombosis (DVT) and pulmonary embolism (PE), continues to be a significant health concern in Canada. 1 The annual incidence of VTE is estimated to be between one and two cases per 1000 individuals,1–3 and more than 25% of patients with PE may die before hospitalization. 2 Beyond its clinical burden, VTE imposes substantial economic costs; in 2011, the average hospitalization cost for a DVT patient in Canada was estimated at CAN$5180, totaling approximately CAN$2.59 million in annual expenditures. 4
Effective management of VTE requires coordinated diagnostic evaluation, prompt initiation of anticoagulation, and structured follow-up. However, patients—particularly those with PE—frequently experience fragmented transitions of care, variability in anticoagulation management, and inconsistent follow-up, which may increase risks of recurrence, bleeding, and avoidable healthcare utilization.2,5–10 Organized thrombosis services have emerged as a strategy to address these gaps by standardizing care processes and improving the safety and continuity of anticoagulation management.2,11–17
Evidence-based guidelines suggest that structured, team-based approaches to VTE care and anticoagulation management can improve clinical outcomes.2,5 Several organizations recommend establishing specialized anticoagulation management services to standardize and optimize the management of anticoagulated patients.2,11,12 These services aim to improve safety, ensure adherence to evidence-based practices, support provider education, and promote continuous quality improvement.
To improve the health of patients with thrombosis and those requiring anticoagulant therapy, a multidisciplinary outpatient thrombosis and anticoagulation management program, called the Adult Outpatient Thrombosis Service (TS), was established in October 2017 in the largest health authority in Newfoundland and Labrador (NL). This service was designed to enhance care continuity and improve patient outcomes by integrating consultation and management pathways primarily for individuals with VTE.18–20 Between October 2017 and December 2024, the TS operated under a physician–pharmacist collaborative care model. The TS consisted of several interrelated clinics: an Emergency Thrombosis Clinic, which provided comprehensive and specialized care to people with an acute episode of VTE; Thrombosis Clinics, which focused on patients with complex needs and those requiring follow-up; Anticoagulation Management Clinics for the management of patients requiring long-term anticoagulation; and a Perioperative Anticoagulation Management Clinic for patients receiving anticoagulation who required planned surgery or procedures.
Specialized thrombosis services are designed to reduce practice variability and improve safety through standardized anticoagulation protocols, pharmacist-supported dose verification, drug-interaction review, and coordinated transitions of care. These structured processes may reduce preventable complications such as recurrence, bleeding, and avoidable hospitalizations; however, evidence evaluating whether such models improve hard clinical outcomes in real-world settings remains limited. Early evaluations of the TS in NL demonstrated high patient satisfaction (85%) and strong adherence to prescribed anticoagulation therapy (88%) during its first 2 years of operation.19,20 Although these findings highlight the acceptability and quality of the service, they did not assess its impact on clinical outcomes. A rigorous evaluation of the TS model was therefore needed to determine whether these care-process advantages translate into improved outcomes for patients with acute VTE. In this study, usual care (UC) refers to all VTE management delivered outside the TS within the Newfoundland and Labrador Health Services (NLHS) Eastern Zones. This study therefore compared clinical outcomes among patients with acute VTE managed in a multidisciplinary TS versus those receiving UC.
Methods
Study design and setting
We conducted a retrospective cohort study using linked health and administrative databases in NL, Canada, to evaluate the clinical effectiveness of a specialized TS on patients diagnosed with acute VTE. The study period spanned from October 2017 to March 2021.
The TS operated within the Eastern Zones of the NLHS, serving a population of over 300,000—approximately two-thirds of the province’s residents. 21 The NLHS Eastern Zones provide a full continuum of care, including public health, long-term care, community services, and hospital-based services. Healthcare services are publicly funded through the NL Medical Care Plan (MCP), which assigns each resident a unique personal health number used for data linkage across provincial systems.
Data sources
Data for this study were compiled by Data and Information Services, Newfoundland and Labrador Health Services, using several linked administrative health databases containing patient demographics, healthcare utilization records (e.g., hospital admissions, emergency department [ED] visits, ambulatory care), diagnostic and procedural codes, and mortality data. Mortality data were obtained derived from the provincial mortality system, which captures all deaths occurring in Newfoundland and Labrador. The mortality system provided date of death but not cause of death; therefore, cause-specific mortality could not be evaluated. Cancer status was also not available in the datasets, limiting adjustment for malignancy-associated mortality. Medication dispensing records were not consistently aligned with diagnosis dates, preventing reliable ascertainment of anticoagulant type, dose, duration, or regimen changes. Outpatient follow-up visits were available only as fee-for-service billing counts and were not linked to indication, preventing comparison of follow-up intensity between TS and UC groups. To identify patients with objectively diagnosed acute VTE, a search of the Picture Archiving and Communications System (PACS) was conducted. This system stores digital diagnostic imaging and reports across NL hospitals. A structured search strategy developed by one of the researchers (KB) was applied to PACS to identify imaging studies indicative of acute VTE (e.g., computed tomography [CT], CT pulmonary angiography [CTPA], and compression ultrasound [CUS]) conducted between October 2017 and August 2019. Diagnostic imaging reports were manually reviewed by two clinicians/researchers (SY, KB) to confirm the presence of acute VTE. Cases deemed inconclusive were reviewed by a thrombosis physician (RC) for final adjudication. The resulting list of patients with confirmed acute VTE was linked via MCP numbers to additional administrative datasets at NLCHI to obtain longitudinal data on healthcare use, outcomes, and covariates. All data were linked using unique identifiers and de-identified prior to analysis. Ethics approval was granted by the NL Health Research Ethics Board (HREB #2023.113).
Study population
The cohort included patients aged ⩾ 18 years with newly diagnosed, objectively confirmed acute VTE between October 2017 and August 2019. Patients were excluded if they had no subsequent healthcare utilization data following the VTE diagnosis, died on the date of diagnosis, experienced their first VTE event prior to October 2017, were not residents of NL at the time of diagnosis, or had isolated superficial vein thrombosis. Patients were followed for clinical outcomes from the time of their initial VTE diagnosis (index event) to March 31, 2021. Patients were identified using positive diagnostic imaging results (compression ultrasonography for DVT or CTPA for PE). The index date was defined as the date of diagnostic imaging. Because many imaging studies occurred during an inpatient encounter, the index hospitalization was counted in the total number of hospitalizations.
The study population was divided into two groups (Fig. 1):
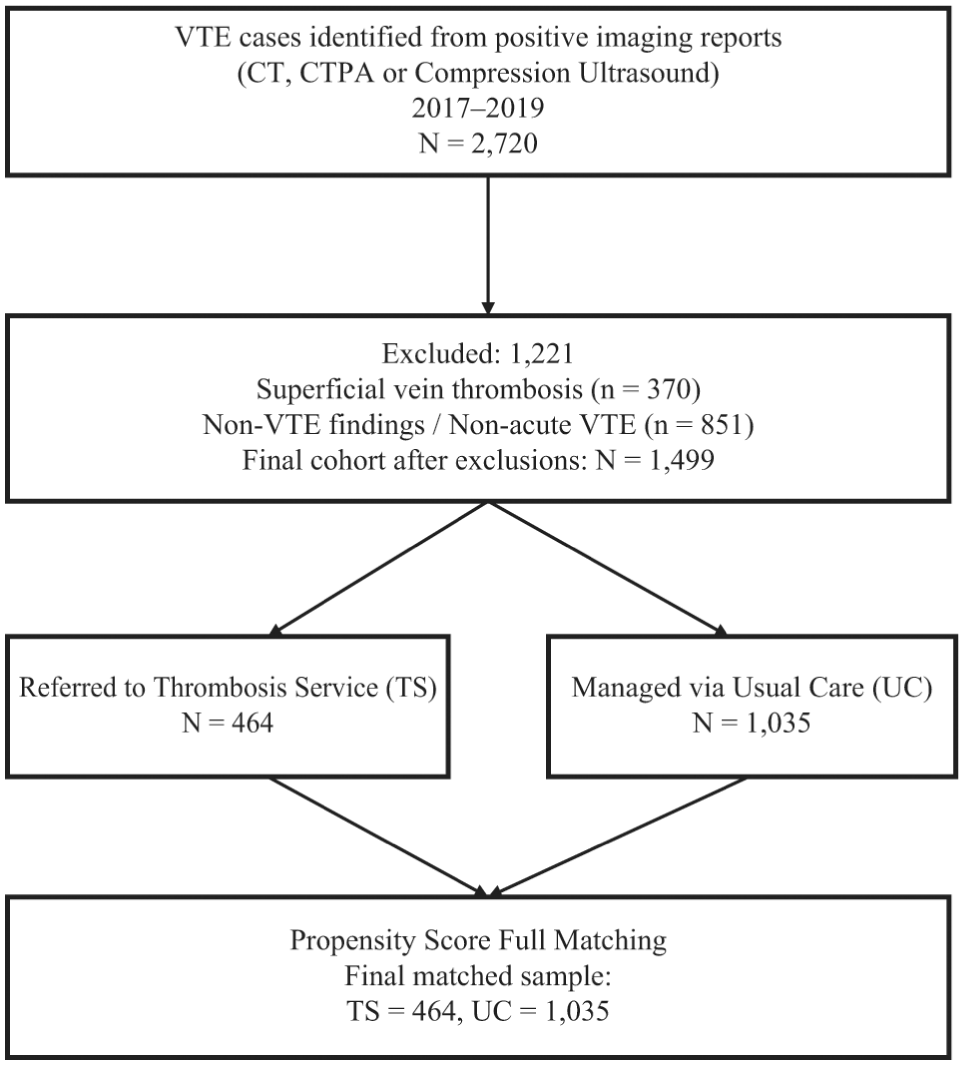
Study flow diagram showing cohort identification.
Propensity score matching
To control for confounding, we estimated each patient’s propensity score for receiving TS care using logistic regression based on baseline characteristics: age, sex, residence (urban/rural), and comorbidities. 22 Full matching on the propensity score was applied to create matched sets that included at least one TS and one UC patient. Full matching was chosen because it retains the entire sample, thereby maximizing statistical power while reducing bias. Unlike fixed-ratio matching, full matching pairs treated and control subjects in variable ratios within matched sets, achieving superior covariate balance. Covariate balance was assessed using standardized mean differences (SMD), with an absolute SMD < 0.1 considered acceptable. 23 SMDs were evaluated but are presented only in the Love plot (Supplemental Figure S1) for clarity; Table 1 reports baseline characteristics without SMDs to avoid redundancy. Data elements distinguishing active cancer (e.g., ongoing treatment or metastatic disease) were not available in an analysis-ready format at the time of cohort assembly and extraction from the administrative data system. Consequently, cancer status could not be incorporated into the primary propensity score specification or outcome models. We acknowledge this as a source of potential residual confounding and address its impact in the discussion on limitations.
Baseline characteristics of the thrombosis service (TS) and usual care (UC) groups.
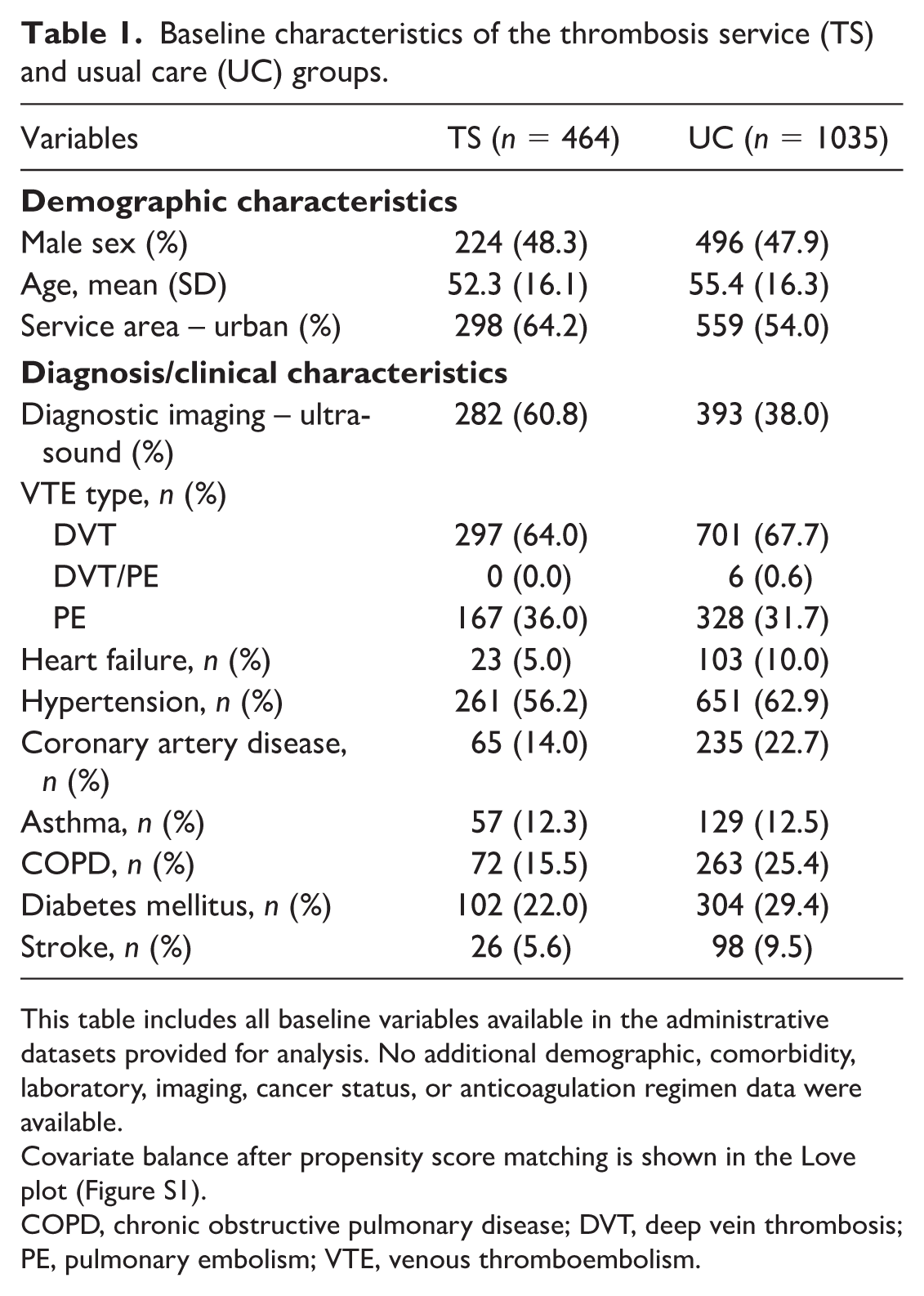
This table includes all baseline variables available in the administrative datasets provided for analysis. No additional demographic, comorbidity, laboratory, imaging, cancer status, or anticoagulation regimen data were available.
Covariate balance after propensity score matching is shown in the Love plot (Figure S1).
COPD, chronic obstructive pulmonary disease; DVT, deep vein thrombosis; PE, pulmonary embolism; VTE, venous thromboembolism.
Outcomes and follow-up
Patients were followed from the index VTE event to death or end of the study period (March 2021). Primary outcomes were recurrent VTE and major bleeding, defined using International Society on Thrombosis and Haemostasis (ISTH) criteria. 24 Recurrent VTE was identified using objectively confirmed positive diagnostic imaging reports (CUS, CT, or CTPA) extracted from the provincial PACS system during the follow-up period, after the index event. PACS was used because the International Statistical Classification of Diseases and Health Problems, Tenth Revision (ICD-10) codes for recurrent VTE are not reliably captured in hospitalization data. Major bleeding events were identified from hospitalization records using ICD-10 codes mapped to ISTH criteria for major bleeding. Only hospital encounters that met ISTH-aligned diagnostic codes were classified as major bleeding.
Secondary outcomes included hospitalizations, all-cause ED visits, and mortality, identified through administrative health data. Hospitalizations and ED visits were analyzed as all-cause events. ED data do not include diagnosis, and hospitalization data cannot reliably distinguish VTE-related admissions. Because follow-up began on the date of diagnostic imaging, index hospitalizations were included for patients diagnosed during an inpatient stay. Mortality was obtained from the NL mortality system, which provides date of death but does not include cause of death information. As a result, mortality was analyzed as all-cause mortality, and it was not possible to classify deaths as VTE-related, bleeding-related, cancer-related, or due to other etiologies. Follow-up time was summarized in person-years, and incidence rates were reported.
Statistical analysis
Incidence rate ratios (IRR) with 95% CIs were estimated using Poisson regression models for all outcomes except mortality. Major bleeding and recurrent VTE events were analyzed as rates rather than through time-to-event methods. This approach was selected because event incidence was low and several patients experienced multiple events. Time-to-event analysis would have required censoring after the first event, leading to additional loss of information and further reducing the number of analyzable events. For mortality, a Cox proportional hazards model was used to estimate the hazard ratio (HR), accounting for time-to-event data and censoring. As part of the sensitivity analysis, we also computed unadjusted IRR using crude event counts and person-time to assess consistency with model-based estimates. To further evaluate the potential impact of unmeasured confounding, we calculated E-values for all primary outcomes. The E-value represents the minimum strength of association that an unmeasured confounder would need to have with both the treatment assignment and the outcome to fully account for the observed association, conditional on the measured covariates. E-values were calculated for both the point estimate and the lower bound of the 95% CI for each outcome, demonstrating a statistically significant protective effect. No imputation was applied as the dataset had complete information on the variables included in this analysis. All statistical analyses were performed using R version 4.2.2 (R Foundation for Statistical Computing).
Results
A total of 1499 patients with newly diagnosed VTE between 2017 and 2019 were included in the analysis, with 464 (31.0%) managed through the TS and 1035 (69.0%) receiving UC. Baseline characteristics of patients in the TS and UC groups are summarized in Table 1. Prior to matching, notable imbalances were observed across several covariates, including age (SMD = 0.204), diagnostic imaging modality (SMD = 0.468), COPD (SMD = 0.249), and coronary artery disease (SMD = 0.224). After applying full propensity score matching, all SMDs were reduced to below 0.1, indicating excellent covariate balance. These improvements are visually supported by the Love plot (Figure S1), which shows a clear shift of all covariates into the acceptable balance range postmatching. The propensity score distribution plot (Figure S2) illustrates adequate overlap in scores between the TS and UC groups, confirming strong common support and appropriate match quality. Total follow-up was 3459.6 person-years (mean 2.31 years). TS patients contributed 1114.9 person-years (mean 2.40) and UC patients contributed 2344.7 (mean 2.27), indicating a comparable follow-up duration across groups.
Clinical outcomes and healthcare utilization
In the propensity score-matched cohort, patients managed by the TS experienced significantly lower rates of several adverse outcomes compared to those receiving usual care. For the primary outcomes, the rates of VTE recurrence (IRR = 0.65, 95% CI: 0.29–0.67, p < 0.001) and major bleeding (IRR = 0.33, 95% CI: 0.19–0.53, p = 0.011) were significantly lower in the TS group. For the secondary outcomes, the rate of all-cause hospitalizations (IRR = 0.76, 95% CI: 0.64–0.92, p = 0.009) and all-cause mortality were significantly reduced in the TS group (HR = 0.62, 95% CI: 0.48–0.81, p = 0.0004) (Figure 2). No significant difference was observed in the rate of ED visits (IRR = 1.02, 95% CI: 0.79–1.32, p = 0.848). These findings suggest that structured management through the TS was associated with improved clinical outcomes. Table 2 includes crude incidence rates for each outcome to aid interpretation of the adjusted IRR and HR estimates.
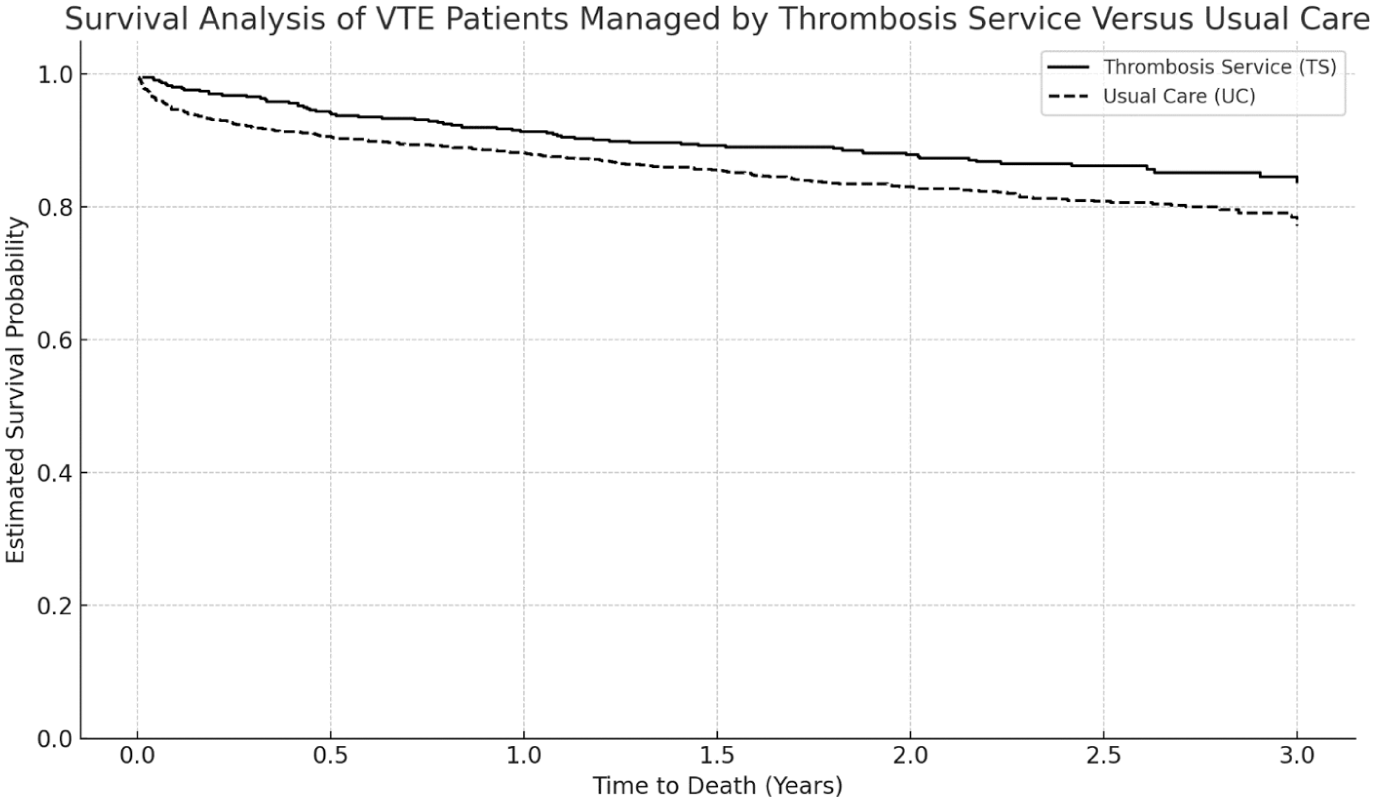
Kaplan–Meier survival curves for patients with venous thromboembolism managed by the thrombosis service versus usual care.
Crude incidence rates presented alongside adjusted incidence rate ratios and hazard ratios comparing the thrombosis service (TS) with usual care (UC).
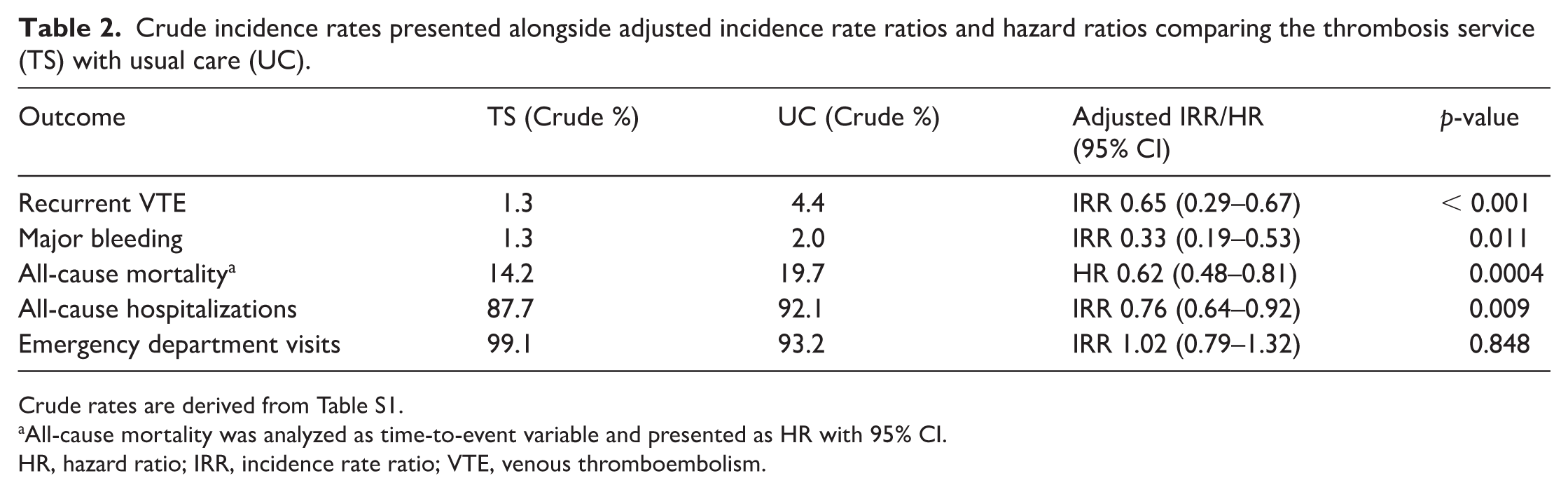
Crude rates are derived from Table S1.
All-cause mortality was analyzed as time-to-event variable and presented as HR with 95% CI.
HR, hazard ratio; IRR, incidence rate ratio; VTE, venous thromboembolism.
Sensitivity analysis
Crude event rate analyses were consistent with model-based estimates (Table S1). E-values suggested that unmeasured confounders would need to be strongly associated with both treatment and outcomes to explain the observed effects. For example, the E-value for major bleeding was 5.51 (lower CI: 10.00) and for mortality was 2.61 (lower CI: 3.59) (Table S2).
Discussion
This study found that management of patients with newly diagnosed VTE through a specialized TS, structured under a physician–pharmacist collaborative model, was associated with lower rates of adverse clinical outcomes compared to usual care. Over a more than 2-year follow-up, TS patients had notably lower rates of recurrent VTE, major bleeding, hospitalizations, and mortality, with similar ED utilization. These results reinforce prior evidence that outpatient VTE care, when structured and protocol-driven, is safe and often superior to inpatient or uncoordinated care.6,7
Despite strong evidence supporting the safety and feasibility of outpatient VTE management, such models remain underutilized in many healthcare systems.6–10 The TS model was designed to address gaps in follow-up, anticoagulation oversight, and patient education. In this study, statistically significant differences were observed between the TS and usual care groups with lower rates of adverse events and mortality observed over extended follow-up in the TS group. These findings should be interpreted cautiously. A cautious interpretation is warranted for two reasons. First, the study design is observational. Even with propensity score full matching and good balance on measured variables, residual confounding and selection effects may remain. Second, the dataset did not include direct measures of potential mediators such as adherence to anticoagulants, follow-up timing and intensity, dose verification, pharmacist interventions, care-transition quality, or specialist involvement. As a result, statements about why TS care was associated with better outcomes should be considered plausible hypotheses rather than demonstrated mechanisms.
The TS model emphasizes structured follow-up, multidisciplinary expertise, and coordinated transitions of care across EDs, inpatient services, primary care, radiology, and clinical pharmacy, each of which may influence processes known to affect clinical outcomes in VTE. Such integrated care structures may be associated with reduced practice variability, more standardized anticoagulation management, and improved continuity during care transitions. In turn, these processes may offer plausible explanations for differences in emergency care use, prescribing practices, dose adjustments, and longer-term anticoagulation safety. Although these mechanisms were not directly measured, they are consistent with prior literature and provide contextual support for the associations observed in this cohort. Prior studies have rarely examined longer-term outcomes; this analysis adds to the literature by describing associations over more than 2 years of follow-up.7–9
Recurrent VTE was 35% lower in the TS group. We hypothesize that elements typical of multidisciplinary thrombosis programs—consistent follow-up, standardized anticoagulation protocols, and pharmacist-supported oversight—could contribute to reduced recurrence.13,20 However, these elements were not evaluated in this study. Specialized thrombosis services have been shown to promote higher adherence to antithrombotic therapy, including direct oral anticoagulants (DOACs). In a recent cross-sectional study conducted within the same health region, patients managed in the TS demonstrated high and consistently maintained DOAC adherence. 14 A second evaluation found similarly high adherence to antithrombotic therapy among TS patients. 20 Although adherence and anticoagulation management were not measured in the present study, these factors are known to be associated with recurrence risk and may provide contextual support for the observed associations with recurrent VTE and hospitalizations. Multidisciplinary thrombosis services also emphasize consistent anticoagulation oversight, dose review, and identification of patients at elevated risk for progression or recurrence. Similar associations between structured anticoagulation management and lower recurrence rates have been reported in pharmacist-led and multidisciplinary care models.13,15 Collectively, these findings suggest that adherence, coordinated care, and specialized monitoring represent plausible, but unmeasured, factors that may be associated with the lower recurrence rates observed among TS-managed patients.
A lower rate of major bleeding was observed in the TS group. Multidisciplinary thrombosis services routinely emphasize bleeding risk assessment, dose verification, drug–drug interaction review, optimization of anticoagulant dosing, early identification of complications, and ongoing patient education. Although these care processes were not directly measured in this study, they represent plausible contextual factors that may be associated with safer anticoagulation practices and could help explain the observed differences in bleeding rates. Prior studies of multidisciplinary and pharmacist-supported anticoagulation management have reported lower bleeding rates in similar care models.9,13,15 These findings are consistent with structured anticoagulation oversight as a plausible, though unmeasured, factor associated with lower major bleeding rates in the TS group.
Fewer all-cause hospitalizations were observed among TS-managed patients, with similar ED visit rates between groups. Thrombosis services frequently provide timely and coordinated outpatient review, including early assessment of symptoms, reinforcement of adherence, optimization of anticoagulant selection and dosing, and early identification of complications. Early follow-up has been shown to improve patient-reported experience and continuity of care, as demonstrated in our TS-specific patient satisfaction survey, where patients reported high satisfaction with communication, accessibility, and overall care quality. 19 Such structured follow-up and early outpatient management may allow complications to be addressed before hospitalization becomes necessary, consistent with prior evaluations of clinic-based VTE management models.9,10,13,15,16 Outpatient visit data in the administrative sources included only fee-for-service physician encounters without information on specialty type or indication. Although the TS group had more outpatient physician contact than usual care, this difference was not statistically significant in aggregate billing data. More granular information on specialist visit type and purpose might have clarified differences in follow-up intensity between the two groups and provided additional context for the observed differences in clinical outcomes. Unfortunately, these data were not available in the health administrative datasets used in this study.
All-cause mortality was lower in the TS group. This may be related to differences in recurrence, anticoagulation management, or broader effects of regular specialist contact. Similar trends towards lower mortality have been reported in other thrombosis service and pharmacist-led anticoagulation models, although most prior studies were underpowered to detect survival differences.13,15 The absolute mortality rates in this cohort were higher than those reported in many VTE registries. This may reflect the demographic and clinical characteristics of the NL population, which is among the oldest in Canada and has a high burden of comorbidity. Nevertheless, mortality was assessed without cause of death information, and cancer status was not available in an analysis-ready form for adjustment. Given these limitations, we avoid inferring specific pathways and emphasize that the mortality finding represents an association that should be confirmed in settings with richer clinical covariates and detailed cause-of-death data.
The success of the TS could be attributed to its multidisciplinary, collaborative care model and the structured processes it employed.17,25 This collaboration is a core strength of many anticoagulation quality improvement programs.13,17,25 By engaging multiple specialists (thrombosis physician, hematologists, and clinical pharmacists) in an integrated service, the TS leveraged a breadth of expertise that no single provider in usual care could offer. Each component of the TS addressed a critical aspect of VTE care: the Emergency Thrombosis Clinic provided prompt follow-up after an acute diagnosis, the Thrombosis Clinic offered physician consultation for complex cases and longitudinal follow-up, the Anticoagulation Management Clinics managed routine therapy monitoring, and the Perioperative Anticoagulation Management Clinic guided safe interruption and resumption of anticoagulation for procedures. These structured processes created a safety net that caught potential errors or gaps in care. The TS’s comprehensive service—from acute care to perioperative planning—ensured continuity, a key strength often missing in usual care. Together, these components offer a comprehensive framework for continuity of care that is often less structured in usual care settings. Although the specific contributions of individual service components could not be evaluated in this study, the organization and coordination inherent to the TS model represent factors that may be associated with the lower rates of bleeding and recurrence observed.
Importantly, the multidisciplinary TS model was not associated with increased healthcare utilization in other domains, such as ED visits. This pattern suggests that the observed differences in clinical outcomes were not accompanied by higher overall service use. From a health system perspective, these findings are encouraging and are consistent with the potential efficiency of team-based outpatient thrombosis care. Although cost-effectiveness was not evaluated in this study, the results support further investigation of coordinated, specialist-led care pathways for VTE management. 8
E-value analyses were conducted to assess the sensitivity of the observed associations to unmeasured confounding. The associations for hospitalizations (IRR 0.76), recurrent VTE (IRR 0.65), major bleeding (IRR 0.33), and mortality (HR 0.62) yielded E-values ranging from 1.96 to 5.51 for the point estimates, and from 2.50 to 10.00 for the lower confidence limits. These values indicate that unmeasured confounding of moderate strength, and of substantial strength for major bleeding, would be required to fully attenuate the observed associations. These values indicate that only moderately strong (or, for bleeding, very strong) unmeasured confounding could fully account for the observed differences. Although residual confounding is possible given the limitations of administrative data, the E-value results suggest that the observed associations are relatively robust to unmeasured confounding. The observed associations between TS management and clinical outcomes are unlikely to be attributable solely to unmeasured confounding.
Strengths and limitations
This study has several notable strengths. First, it leveraged a large cohort drawn from an entire regional health system, capturing real-world patterns of care and outcomes across diverse clinical settings. This enhances the external validity and relevance of the findings for health system planning and service design. Second, the study evaluated outcomes over an extended follow-up period of more than 2 years, allowing assessment of long-term safety, recurrence, and mortality—domains that are rarely examined in evaluations of thrombosis service models. Third, the use of linked administrative datasets enabled comprehensive capture of objectively defined, clinically meaningful outcomes, including recurrent VTE, major bleeding, hospitalizations, and mortality. These outcomes are less prone to misclassification than subjective or self-reported measures. Fourth, we employed robust methods, including propensity score full matching to balance measured covariates between groups and E-value sensitivity analyses to assess the potential influence of unmeasured confounding. This combination strengthens the internal validity of the study and supports the credibility of the observed associations. Fifth, the evaluation of an integrated, multidisciplinary TS in a real-world context provides novel insight into how structured outpatient anticoagulation models perform at scale. Few studies have examined the full continuum of care—emergency access, rapid follow-up, pharmacist-led anticoagulation oversight, physician consultation, and perioperative management—within a unified system.
The study builds upon and aligns with prior regional work demonstrating high adherence, high patient satisfaction, and improved care coordination within the TS model, offering a cohesive body of evidence supporting its effectiveness. Finally, the study population reflects a relatively high level of clinical complexity compared with VTE cohorts described in other jurisdictions. NL has a documented high burden of multimorbidity and chronic disease, which contributes to greater baseline risk and higher rates of adverse outcomes. Additionally, because follow-up began at the date of diagnostic imaging, many patients diagnosed during inpatient admissions were included, and their index hospitalization contributed to the all-cause hospitalization total. These structural factors result in higher absolute rates of hospitalization and mortality than typically reported. Although this limits generalizability beyond similar high-burden health systems, the internal comparison between TS-managed and UC-managed patients remains valid. Replication in other settings with different population risk profiles is warranted to confirm external applicability. These strengths position the study as one of the most comprehensive real-world evaluations of a multidisciplinary thrombosis service to date, providing a strong empirical foundation for further implementation and scalability efforts.
Despite these strengths, the study also has limitations. First, the observational design and use of administrative data introduce the potential for residual confounding and selection bias. Although propensity score full matching improved balance on all available variables, unmeasured factors such as functional status, disease severity, clinician judgment, or social determinants may still influence outcomes. To address this, we conducted E-value sensitivity analyses to quantify the strength of unmeasured confounding needed to fully explain our findings. The large E-values for major bleeding, recurrent VTE, and mortality indicate that only moderately strong and, in some cases, very strong unmeasured confounding could negate the observed effects, supporting the robustness of the associations.
Second, the administrative datasets available for this study contained a limited set of comorbidity and clinical variables. Important prognostic factors such as active cancer, laboratory values, vital signs, and symptom severity were not available. Cancer status was also unavailable in an analysis-ready format at the time of cohort creation, limiting our ability to adjust for this major prognostic factor. We mitigated this limitation by focusing on hard clinical endpoints (recurrent VTE, major bleeding, hospitalization, death), avoiding overinterpretation of processes not captured in administrative data, and explicitly framing mechanistic explanations as plausible rather than definitive. We also reported E-values to assess whether missing cancer data or other unmeasured variables could plausibly account for the observed differences between groups.
Third, prescription and diagnosis dates were not aligned, preventing accurate assessment of anticoagulant choice, dose, timing, or adherence. As a result, we did not attempt to infer treatment appropriateness from administrative data. Instead, interpretation of adherence-related pathways was grounded in robust published evidence including regional studies showing high adherence among patients managed within thrombosis services rather than relying on potentially misleading administrative proxies.
Fourth, ED data did not include clinical indication, precluding identification of VTE-related or bleeding-related presentations. Similarly, hospitalization records did not reliably distinguish encounters due to VTE recurrence, and therefore recurrent events could not be inferred from admission data alone. To ensure accurate outcome capture, recurrent VTE was instead identified using diagnostic imaging reports, which provide a more reliable method for detecting objectively confirmed events in administrative datasets. Furthermore, because follow-up began on the date of diagnostic imaging, index hospitalizations were included in the hospitalization count for many patients, contributing to the high overall hospitalization rate. To mitigate these limitations, we analyzed all-cause hospitalizations and ED visits, an approach commonly used in health services research, and contextualized the findings by describing diagnostic workflows, patterns of care delivery, and plausible mechanisms that may have reduced preventable admissions among TS patients.
Fifth, outpatient billing data captured only fee-for-service encounters without provider specialty or visit reason, preventing assessment of differences in follow-up intensity or specialist involvement. To address this gap, rather than drawing inferences from crude visit counts, we interpreted the findings using established literature on multidisciplinary thrombosis and anticoagulation services, including evidence demonstrating improved satisfaction, adherence, and continuity of care among TS patients.
Sixth, the study was conducted within a single regional health system in NL, which may limit generalizability to other settings. We addressed this by clearly characterizing the study context and emphasizing that the core components of the TS—rapid access assessment, standardized anticoagulation protocols, pharmacist-led monitoring, and structured longitudinal follow-up—are broadly transferable. We also highlight the need for multisite evaluations to assess scalability and resource requirements. In addition, cause-of-death information was unavailable, precluding attribution of mortality differences to VTE, bleeding, cancer, or other causes; accordingly, mortality was analyzed as an all-cause outcome and mechanistic interpretations were avoided. Despite these limitations, the study benefits from a large real-world cohort, extended follow-up, rigorous propensity score matching, and sensitivity analyses. The consistency and robustness of the observed associations contribute real-world evidence regarding multidisciplinary thrombosis service models.
Implications and future research
Taken together, the results provide real-world evidence that a coordinated, multidisciplinary thrombosis model was associated with favorable clinical outcomes across several domains without an apparent increase in ED utilization. To move from association to explanation, future evaluations should incorporate prospectively collected process-of-care measures (e.g., time to first follow-up, adherence trajectories, dose changes and verification steps, drug-interaction checks, and formal care-transition metrics), richer clinical covariates (including cancer status, laboratory values, and severity indicators), and linkage to cause of death data. Multisite studies and pragmatic trials would help assess reproducibility, scalability, and cost-effectiveness, and clarify which specific components of multidisciplinary care yield the greatest benefit.
Conclusion
The multidisciplinary, physician–pharmacist collaborative thrombosis service (TS) model was associated with substantially lower risks of recurrent VTE, major bleeding, hospitalization, and all-cause mortality compared with usual care. These associations were observed over more than 2 years of follow-up and were consistent across sensitivity analyses evaluating potential unmeasured confounding. Although causal inference cannot be made, the findings suggest that coordinated, protocol-driven outpatient thrombosis care may be associated with favorable clinical outcomes. Further research is needed to assess cost-effectiveness, patient experience, and scalability of structured thrombosis services across diverse healthcare settings.
Supplemental Material
sj-docx-1-vmj-10.1177_1358863X261430616 – Supplemental material for Clinical effectiveness of a multidisciplinary thrombosis service versus usual care in the management of venous thromboembolism: A retrospective cohort study
Supplemental material, sj-docx-1-vmj-10.1177_1358863X261430616 for Clinical effectiveness of a multidisciplinary thrombosis service versus usual care in the management of venous thromboembolism: A retrospective cohort study by Kwadwo O Bonsu, Rufaro S Chitsike, Tiffany A Lee, Hai V Nguyen, Cindy Whitten and Stephanie W Young in Vascular Medicine
Footnotes
Declaration of conflicting interests
Rufaro Chitsike received speaking honoraria from Pfizer Canada. Tiffany A Lee has received investigator-initiated unrestricted research funding from Shoppers Drug Mart Inc. unrelated to this work. The remaining authors have no conflicting interests.
Funding
The development, implementation, and evaluation of the Thrombosis Service, including this study, was supported by an unrestricted grant from Sanofi Canada and Bayer Canada (Drs Bonsu, Chitsike, and Young). Funders had no role in the study design, analysis, or manuscript preparation.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.