
Abstract
Background:
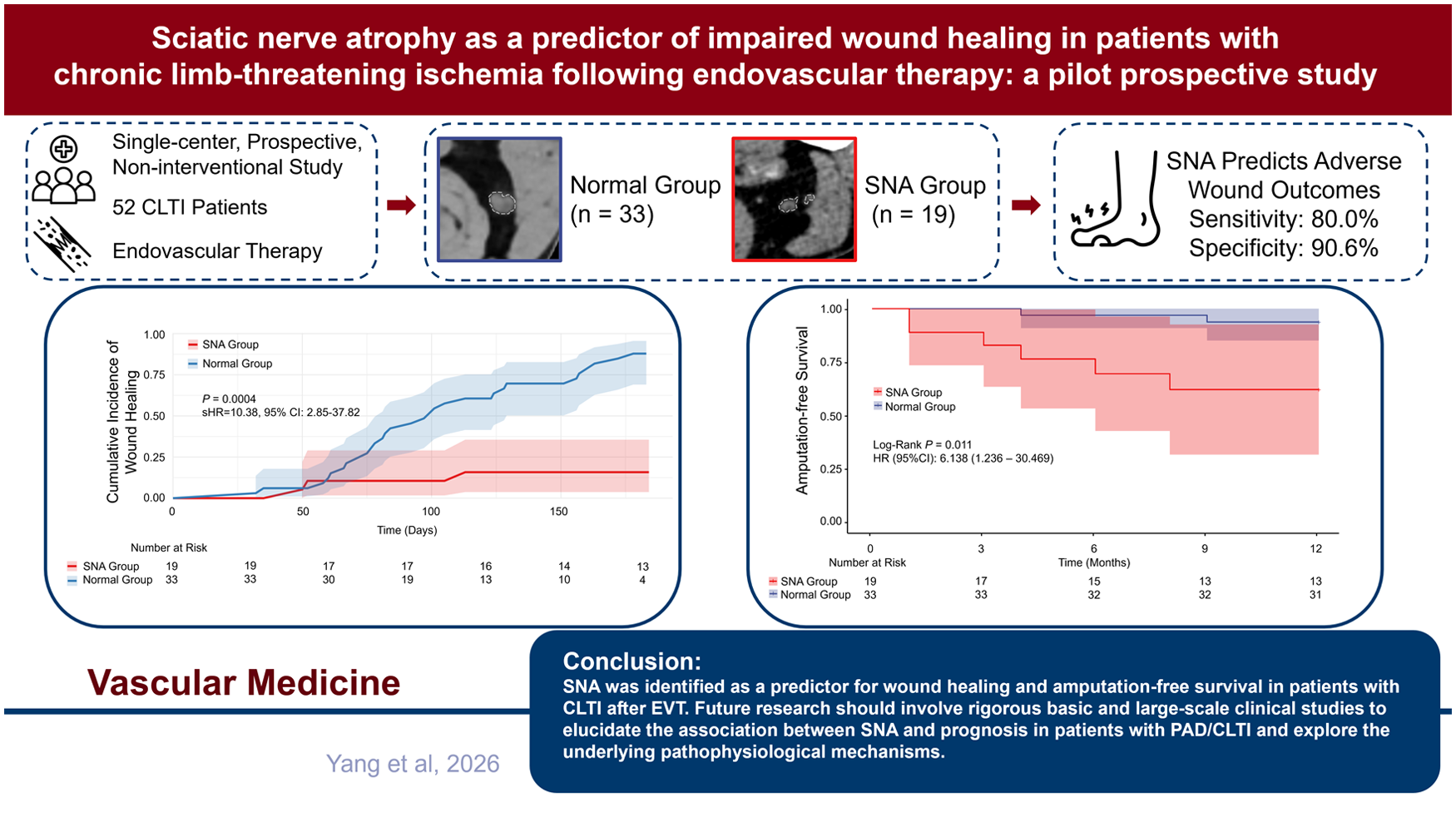
A prior retrospective single-center study involving patients with chronic limb-threatening ischemia (CLTI) demonstrated that sciatic nerve atrophy (SNA) is associated with impaired wound healing (IWH) and reduced amputation-free survival (AFS). We conducted a prospective single-center pilot study to validate the prognostic implications of SNA in predicting wound healing and AFS.
Methods:
Patients diagnosed with CLTI and associated tissue loss were recruited for participation in this prospective, noninterventional study. The cross-sectional area (CSA) of the sciatic nerve at the mid-to-lower femoral quarter was quantified utilizing computed tomography imaging. SNA was identified based on the predefined CSA threshold. Patient outcomes were evaluated through outpatient clinic visits and telephone follow-ups. Outcomes assessed included wound healing rate, adverse wound outcomes (AWO), and AFS.
Results:
In the cohort of 52 limbs with CLTI from 52 patients, 19 individuals were categorized into the SNA group. The 6-month wound healing rate was significantly lower in the SNA group (15.8%) compared to the normal group (87.9%) (p < 0.001). The sensitivity and specificity of SNA for predicting AWO at 6 months were 80.0% and 90.6%, respectively. Patients in the SNA group had significantly lower AFS at 1 year (68.4% vs 93.9%, p = 0.011). Multivariable analysis further established that SNA was an independent prognostic factor for both AWO (hazard ratio [HR]: 0.113; 95% CI: 0.034–0.381; p < 0.001) and AFS (HR: 6.135; 95% CI: 1.236–30.303; p = 0.026) following endovascular therapy (EVT).
Conclusions:
SNA was identified as a predictor for AWO and AFS in patients with CLTI after EVT. Future research should involve rigorous basic and large-scale clinical studies to elucidate the association between SNA and prognosis in patients with peripheral artery disease (PAD)/CLTI and explore the underlying pathophysiological mechanisms.
Keywords
Introduction
Chronic limb-threatening ischemia (CLTI), the most severe clinical manifestation of peripheral artery disease (PAD), is characterized by ischemic rest pain or ischemic tissue loss, which may occur with or without gangrene. 1 Endovascular therapy (EVT) represents an effective and minimally invasive therapeutic option for patients with CLTI, facilitating wound healing and limb salvage postprocedure. 2 However, a significant proportion of patients with CLTI continue to experience adverse wound outcomes (AWO) following EVT, including impaired wound healing (IWH), major amputation, or mortality. These complications not only impair patient quality of life but also contribute to increased healthcare utilization and costs.3,4 Identifying patients with CLTI who are at risk of developing AWO is essential for implementing more precise wound management strategies and determining appropriate amputation levels.5,6 Although numerous studies have identified factors associated with AWO, such as the Global Anatomic Staging System (GLASS), nonambulatory status, and low serum albumin levels, the majority of these investigations have been retrospective and have lacked a simple, reliable biomarker for predicting AWO.7 –9
A prior retrospective study identified sciatic nerve atrophy (SNA) as a risk factor for IWH, amputation-free survival (AFS), and overall survival (OS) following revascularization surgery. 10 Furthermore, our previous animal experiments demonstrated that localized injury to the sciatic nerve can lead to a significant reduction in microvascular perfusion in the distal regions of the nerve, as assessed by super-resolution ultrasound imaging. 11 Building upon this foundation, we conducted a prospective, single-center study to test the hypothesis that the SNA is a predictive factor for AWO and AFS in patients with CLTI following EVT.
Methods
Patients
This prospective, observational, noninterventional pilot study was approved by the institutional review board of Peking University First Hospital. Adult patients with CLTI and lower-limb tissue loss were consecutively recruited from the Interventional Radiology and Vascular Surgery Ward of Peking University First Hospital between February 2024 and September 2024. All participants provided written informed consent prior to enrollment during their hospitalization for EVT. Inclusion criteria required participants to meet the following characteristics: age ⩾ 18 years, diagnosis of CLTI, and presence of tissue loss without prior major amputation (defined as amputation at or proximal to the ankle joint). Exclusion criteria included: acute lower-extremity arterial embolism or thrombosis; history of poliomyelitis; failed EVT (defined as the absence of at least one intact vessel extending to the foot following EVT); contraindications to antiplatelet therapy; prior lower-limb fractures or significant traumatic injuries; an estimated life expectancy of less than 1 year (as determined by a multidisciplinary team of experts); and active malignancy. Herniated nucleus pulposus was diagnosed by orthopedic specialists based on concordant findings from neuroimaging and a characteristic clinical presentation. 12 History of spinal fracture was defined as a clinically or radiologically confirmed vertebral fracture, with documentation in the electronic medical record or verified by imaging reports.
Endovascular treatment and wound management
All patients underwent the GLASS evaluation following lower-extremity arterial angiography. 13 The EVT strategy included conventional balloon angioplasty, implantation of bare-metal stents, drug-coated balloon (DCB) angioplasty, and deployment of drug-eluting stents (DES). The specific therapeutic approach was determined by vascular surgeons, each with more than 5 years of clinical experience. The Geriatric Nutritional Risk Index (GNRI) was used to assess nutritional risk in patients with CLTI. 9
The WIfI (Wound, Ischemia, foot Infection) staging system is employed for comprehensive wound assessment in patients with CLTI following EVT. 5 Wound assessment and management were carried out by plastic surgeons using the TIME framework throughout the follow-up period. 14 Throughout the study, both patients with CLTI and the plastic surgeons were blinded to the group assignments of the participants. In accordance with previously established protocols, standardized wound care procedures were uniformly administered to all participants, regardless of their group classification.15,16 The severity of ulcers, particularly those presenting signs of infection, was rigorously evaluated to guide clinical decision-making regarding the appropriate indications for antibiotic therapy and the optimal timing for amputation, when clinically indicated. Ulcer progression and the time required for complete wound healing were systematically recorded and analyzed.
Evaluation of sciatic nerve atrophy (SNA)
Preoperative computed tomography (CT) angiograms in 1-mm slices were obtained for sciatic nerve evaluation. 10 Three experienced radiologists independently measured the cross-sectional area (CSA) of the sciatic nerve at the level corresponding to the junction between the middle and lower one-quarter segments of the femur on axial CT images. If the sciatic nerve has already bifurcated into the tibial nerve and the peroneal nerve at the given cross-sectional level, the total CSA should be calculated as the sum of the areas of both branches. The average of the measurements obtained by the three radiologists was then calculated. Patients with a CSA ⩽ 23.6 mm2 were classified into the SNA group, and those with a CSA > 23.6 mm2 were categorized as the normal group (Supplemental Figure S1). The threshold of 23.6 mm2 for CSA was established based on prior retrospective studies. 10 Using established methods, axial CT images at the lower border of the third lumbar vertebra were used to measure total skeletal muscle area. 17 The presence of sarcopenia was defined as a skeletal muscle area of < 114.0 cm2 for men and < 89.8 cm2 for women. 17 Peripheral neuropathy was diagnosed based on a Neuropathy Disability Score > 5, in conjunction with abnormal nerve conduction velocity findings. 18
Outcomes
Wound assessment was conducted using the Pressure Ulcer Scale for Healing (PUSH) score, 19 with a score = 0 indicating wound healing and a score > 0 indicating IWH. 8 The primary endpoint of the study was wound healing rate at 6 months following EVT. AWO was a composite endpoint defined as the occurrence of any of the following: IWH, above-ankle amputation, or all-cause death. The secondary endpoint was AFS at 1-year post-EVT. Patients were monitored through outpatient visits or telephone consultations at 1, 3, 6, and 12 months after EVT.
Statistical analysis
The trial design was prespecified according to a time-driven framework. In a previous retrospective study, the wound healing rate was 27% in the SNA group, compared to 87% in the normal group. 10 To account for potential selection bias inherent in retrospective designs, we conservatively estimated the wound healing rates for this prospective study to be 34% in the SNA group and 76% in the normal group. Sample size calculation was performed using a chi-squared (χ2) test for difference in proportions between two independent groups. The significance level (α) was set at 0.05 (two-sided), with a desired power (1 – β) of 0.80. The allocation ratio (SNA group : normal group) was set at 1:1.86. 10 Based on these parameters, a total sample size of 48 participants was calculated, comprising 17 subjects in the SNA group and 31 subjects in the control group. Accounting for an estimated dropout rate of 5%, the final target sample size was adjusted to 51 participants to ensure sufficient power for detecting the hypothesized effect.
Continuous variables were evaluated using either Student’s t-test or the Mann–Whitney U test, contingent upon the distribution of the data, whereas categorical variables were examined using the chi-squared (χ2) test or Fisher’s exact test. Differences in the CSA of the sciatic nerve between the bilateral lower limbs were evaluated using a paired t-test. Survival curves were constructed via the Kaplan–Meier method and compared using the log-rank test. To evaluate the cumulative incidence of wound healing across different patient groups while accounting for the competing risks of death and amputation, we employed Fine–Gray subdistribution hazard modeling. Univariate analyses of clinical characteristics in relation to AWO or AFS were also performed using the log-rank test. For multivariable analyses, the Cox proportional hazards model was utilized to ascertain the independent prognostic significance of clinical characteristics identified as statistically significant in the univariate analysis. The Cochran–Armitage trend test was conducted to assess the existence of a linear relationship between the reduction in the CSA of the sciatic nerve and the proportion of patients with CLTI who experienced AWO. All statistical analyses were conducted using SPSS version 27.0 (IBM Corp.) and data visualization was carried out with R version 4.0.4 (R Foundation for Statistical Computing; 64-bit). A p < 0.05 was considered statistically significant.
Results
In this study, 52 limbs from 52 patients with CLTI following EVT were included (Figure S2). No patients were lost to follow-up. All patients with CLTI exhibited unilateral tissue loss, and the contralateral limb manifested claudication. Therefore, in the analysis of patients with CLTI, a limb-based analytical approach was employed; specifically, the CSA of the sciatic nerve in the limbs with tissue loss was quantified and analyzed. The clinical characteristics of the participants are detailed in Table 1. Patients exhibiting SNA demonstrated a higher prevalence of prior coronary heart disease (CHD) compared to those without SNA. The ankle–brachial index (ABI) assessed before EVT, along with the incidence of peripheral neuropathy and nonambulatory status, were similar between the SNA group and the normal group. No significant difference in the prevalence of sarcopenia was observed between the two groups. Details regarding wound management and EVT outcomes are provided in Table 2. The WIfI stage, GLASS stage, and ABI measured post-EVT, as well as the EVT procedures and wound management strategies, were comparable between the SNA group and the normal group without SNA. None of the patients with CLTI underwent repeat revascularization procedures within 6 months following their initial EVT. All patients were diagnosed with CLTI in only one limb, and the contralateral limb exhibited only claudication. Importantly, there was no significant difference in the CSA of the sciatic nerve between the CLTI-affected limb and the contralateral limb (Figure S3). Furthermore, we investigated the potential association between the CSA of the sciatic nerve and skeletal muscle area in the 52 patients (Figure S4). Curve fitting indicated that neither the linear model (R2 = 0.003122, p > 0.05) nor the exponential model (R2 = 0.00357, p > 0.05) provided a significant fit for the data.
Comparison of etiological clinical characteristics in patients with and without sciatic nerve atrophy (SNA).
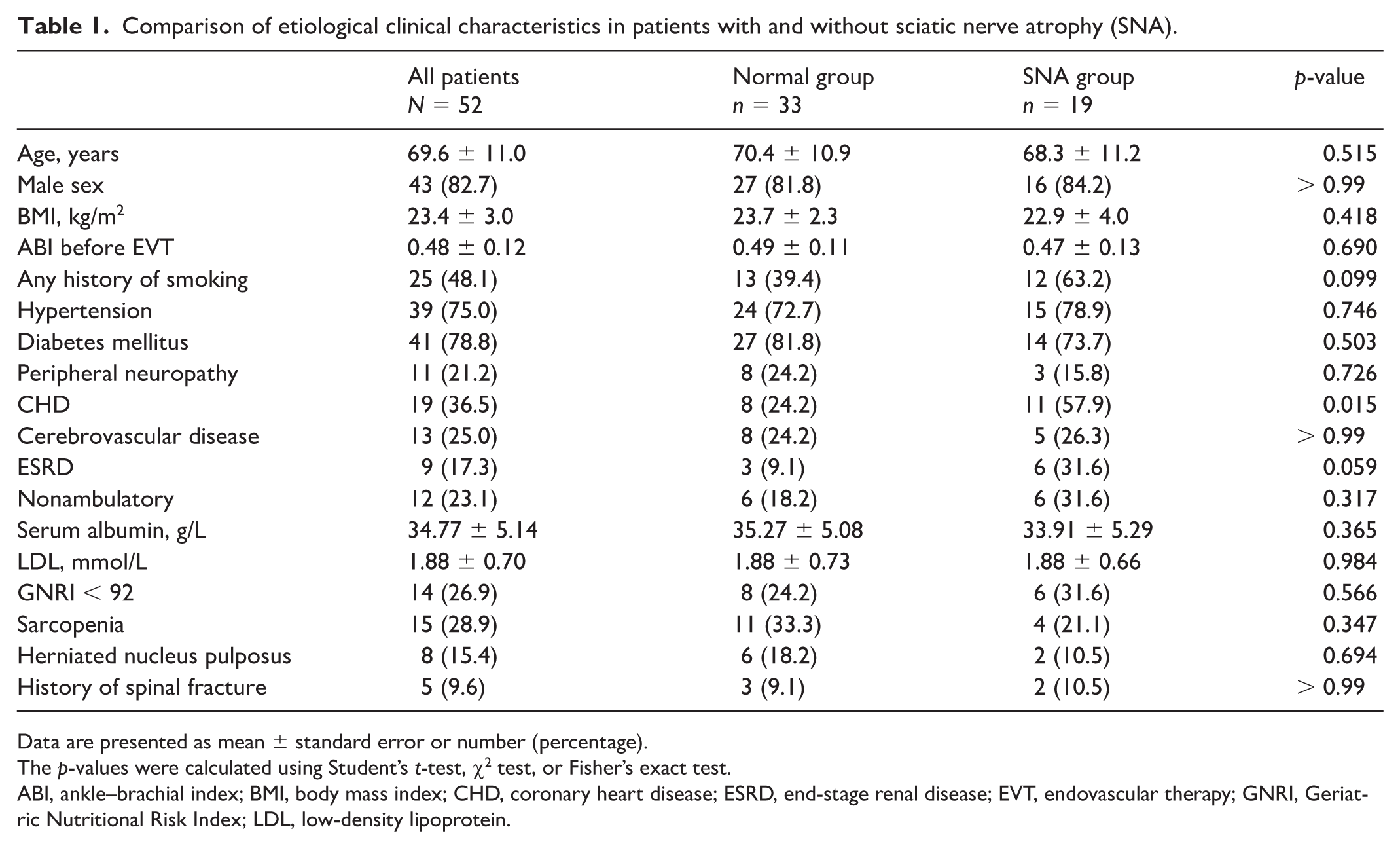
Data are presented as mean ± standard error or number (percentage).
The p-values were calculated using Student’s t-test, χ2 test, or Fisher’s exact test.
ABI, ankle–brachial index; BMI, body mass index; CHD, coronary heart disease; ESRD, end-stage renal disease; EVT, endovascular therapy; GNRI, Geriatric Nutritional Risk Index; LDL, low-density lipoprotein.
Comparison of wound management and endovascular therapy outcomes in patients with and without sciatic nerve atrophy.
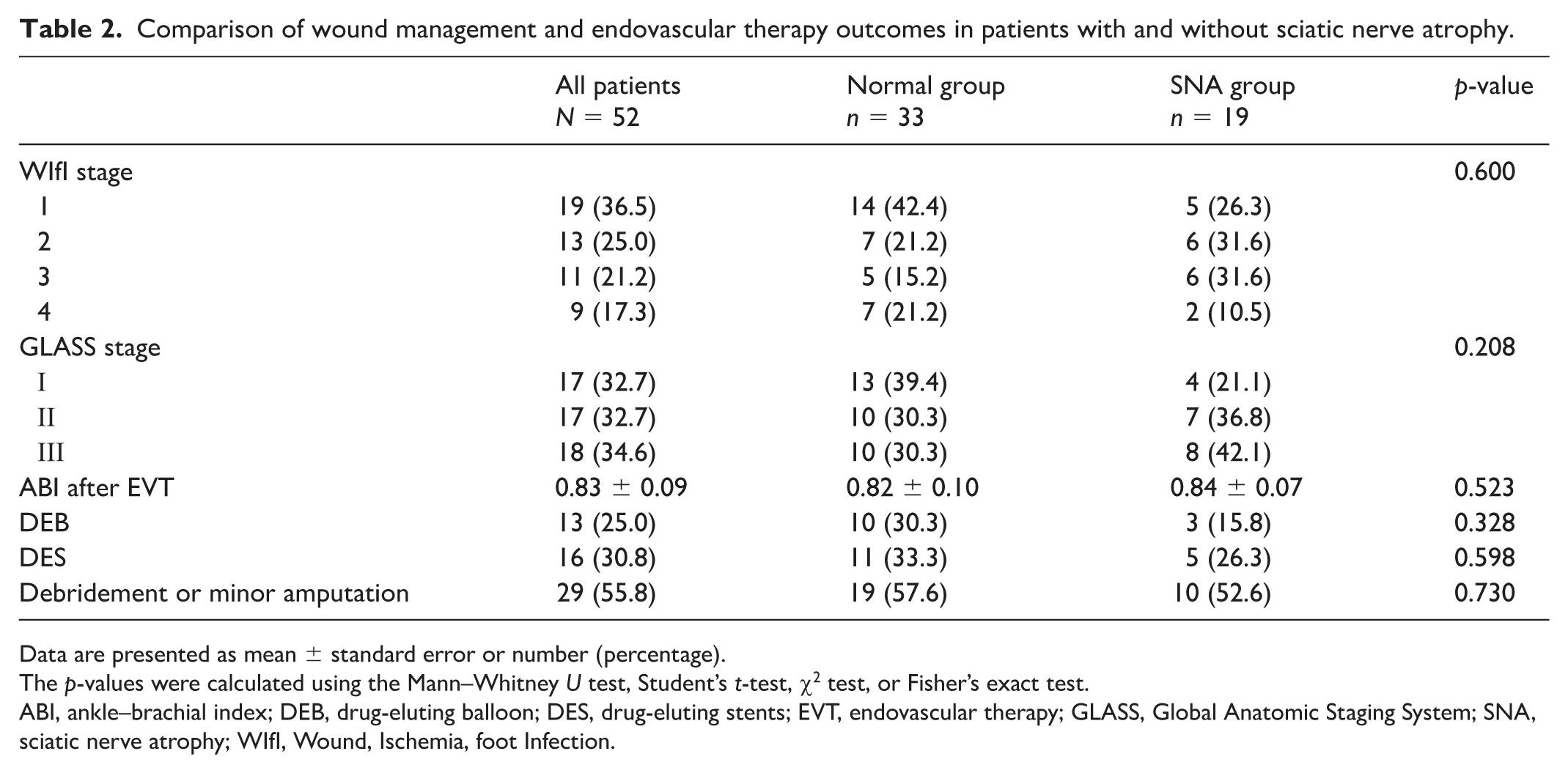
Data are presented as mean ± standard error or number (percentage).
The p-values were calculated using the Mann–Whitney U test, Student’s t-test, χ2 test, or Fisher’s exact test.
ABI, ankle–brachial index; DEB, drug-eluting balloon; DES, drug-eluting stents; EVT, endovascular therapy; GLASS, Global Anatomic Staging System; SNA, sciatic nerve atrophy; WIfI, Wound, Ischemia, foot Infection.
Comparison of wound healing and adverse wound outcome (AWO) rates between patients with and without SNA
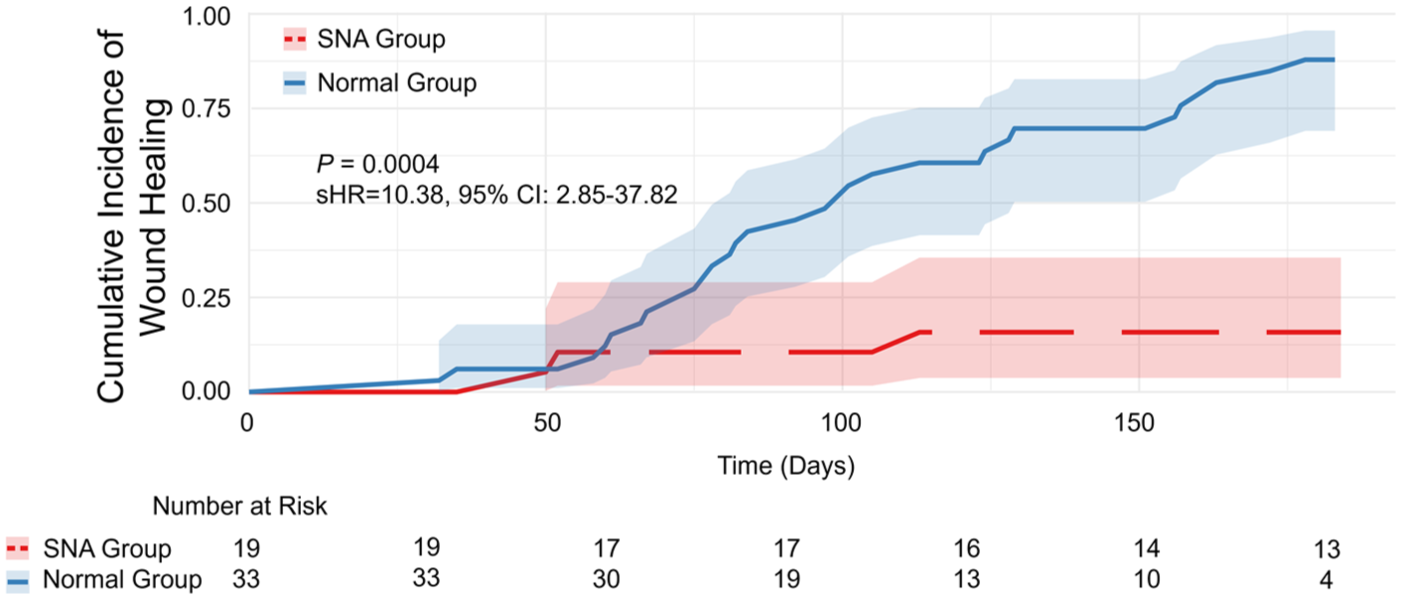
After accounting for competing risks (amputation or death) using the Fine–Gray model, patients in the SNA group demonstrated significantly worse wound healing rate (15.8% vs 87.9% at 6-month follow-up; subdistribution hazard ratio (sHR): 10.38; 95% CI: 2.85–37.82; p = 0.0004) (Figure 1; Supplemental Table S1). Patients with SNA demonstrated a significantly elevated 6-month incidence rate of AWO compared to those without SNA (84.2% vs 12.1%; log-rank test, p < 0.001). After excluding patients with sarcopenia, the SNA group continued to demonstrate a significantly higher rate of AWO compared with the non-SNA group (80.0% vs 13.6%; Fisher’s exact test, p < 0.001). The sensitivity and specificity of SNA as a predictive marker for AWO in patients with CLTI at the 6-month interval were 80.0% and 90.6%, respectively.
The Fine–Gray competing risks survival curve illustrating the cumulative incidence of wound healing over a 6-month period in patients with and without sciatic nerve atrophy (SNA), accounting for the presence of competing events (amputation or death). sHR, subdistribution hazard ratio.
We conducted an evaluation of the risk factors associated with AWO following EVT. Through univariate analysis, end-stage renal disease (ESRD) and SNA were identified as significant risk factors for AWO within 6 months post-EVT (Table 3). Further multivariable analysis, incorporating ESRD and SNA as covariates, corroborated that SNA independently serves as a predictor of AWO in patients with CLTI (HR: 0.113; 95% CI: 0.034–0.381; p < 0.001) (Table 3).
Univariate and multivariable analyses of clinical characteristics associated with adverse wound outcomes after endovascular therapy.
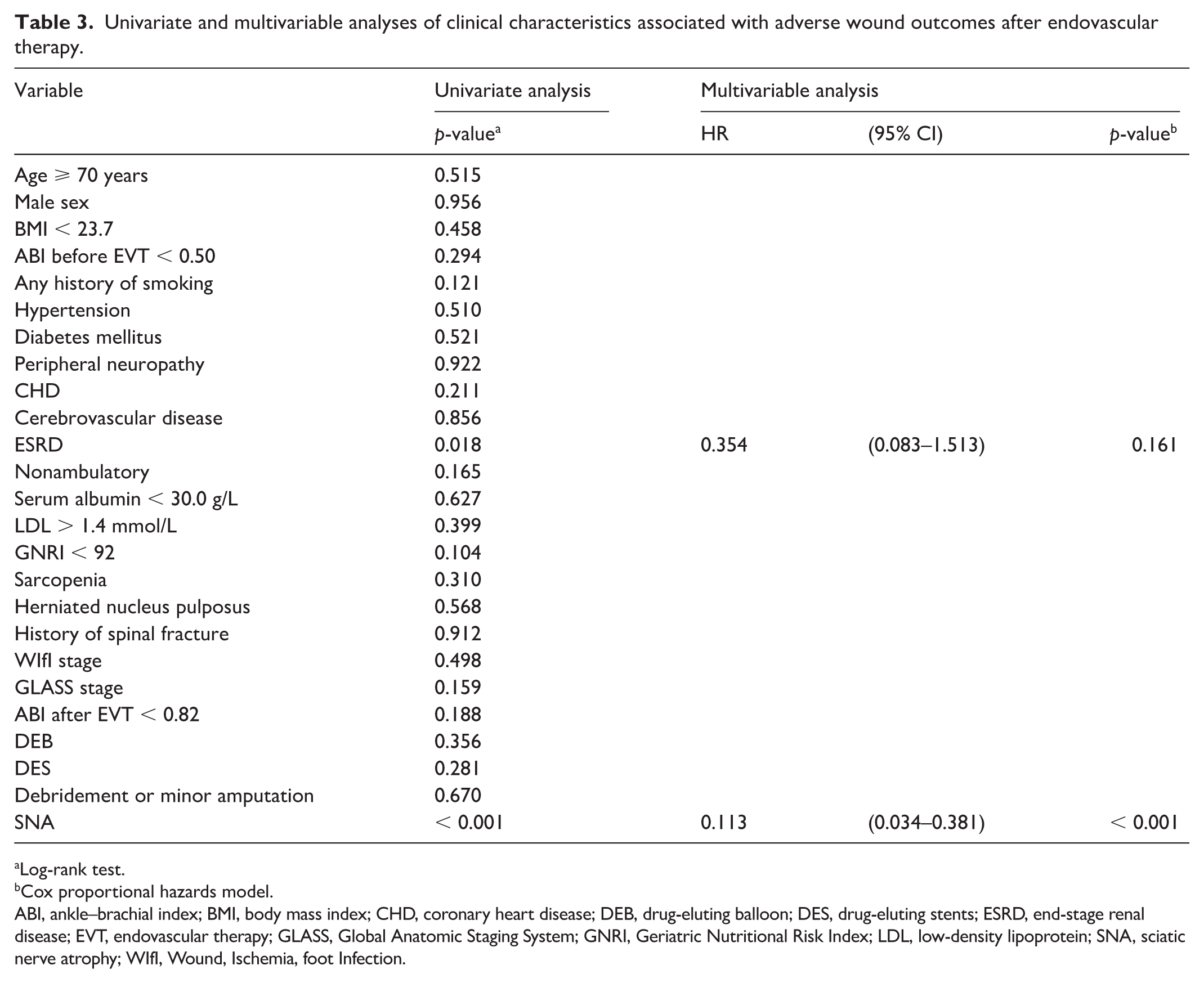
Log-rank test.
Cox proportional hazards model.
ABI, ankle–brachial index; BMI, body mass index; CHD, coronary heart disease; DEB, drug-eluting balloon; DES, drug-eluting stents; ESRD, end-stage renal disease; EVT, endovascular therapy; GLASS, Global Anatomic Staging System; GNRI, Geriatric Nutritional Risk Index; LDL, low-density lipoprotein; SNA, sciatic nerve atrophy; WIfI, Wound, Ischemia, foot Infection.
To further evaluate the association between SNA and AWO, patients with CLTI were stratified into four groups (quartiles) based on the CSA of the sciatic nerve: Q1 (< 21.78 mm²), Q2 (21.78–26.82 mm²), Q3 (26.83–32.08 mm²), and Q4 (> 32.08 mm²). The Cochran–Armitage trend test confirmed a statistically significant progressive increase in the incidence of AWO across the quartiles (AWO rate: 78.6%, 41.7%, 14.3%, and 16.7% from Q1 to Q4; Z = –3.595, p < 0.001). These findings provide strong evidence of a close association between reduced CSA of the sciatic nerve and the incidence of AWO.
Comparison of amputation-free survival between patients with and without SNA
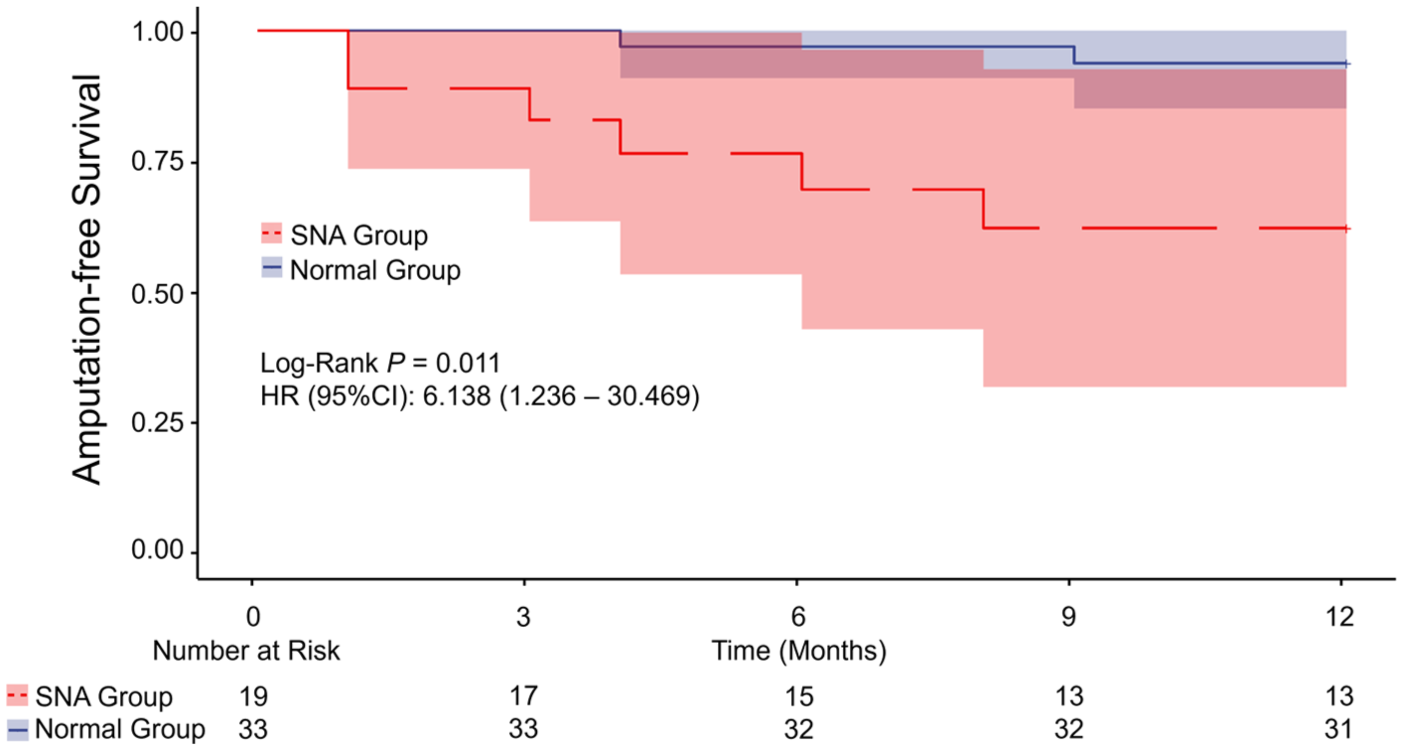
The Kaplan–Meier survival analysis illustrated the AFS in patients with CLTI following EVT (Figure 2). The analysis revealed that patients with SNA had a significantly reduced 1-year AFS rate compared to those without SNA (68.4% vs 93.9%; log-rank test, p = 0.011). A univariate analysis revealed that SNA was the significant risk factor associated with AFS within 1 year following EVT (Table S2). Subsequent multivariable analysis, with adjustment for SNA as a covariate, confirmed that SNA independently predicts AFS at 1 year in patients with CLTI (HR: 6.135; 95% CI: 1.236–30.303; p = 0.026) (Table S2).
Kaplan–Meier estimates of amputation-free survival in patients with and without sciatic nerve atrophy (SNA). HR, hazard ratio.
Discussion
Our findings indicate that SNA functions as an independent predictor of wound healing at 6 months in patients with CLTI post-EVT, in addition to demonstrating a decreased AFS rate at 1 year. The results of this prospective pilot study corroborate and validate those observed in a prior retrospective study. 10 Our research findings provide a thorough elucidation of the considerable impact that SNA has on wound healing and long-term survival outcomes in patients with CLTI.
Wound healing represents a critical outcome following EVT in patients with CLTI. 2 Although previous studies have identified various indicators as risk factors for IWH, the retrospective nature of these studies and the complexity of their indicator systems limit the generalizability of the findings and their practical application in clinical assessment.5,7 –9 Matsubara et al. and our study have identified SNA as a promising marker for predicting IWH, demonstrating high sensitivity and specificity, and convenient to measure in clinical practice. 10 Although existing studies have highlighted the significant role of peripheral nerve injury in suppressing immune responses and promoting tumor progression, the relationship between peripheral nerve and peripheral vascular disease remains poorly understood.20,21 Our study provides the first prospective evidence demonstrating that peripheral nerve atrophy has substantial predictive value for the prognosis of peripheral vascular disease, representing a novel and potentially transformative insight into the neurovascular interactions underlying this condition.
The etiology of SNA remains incompletely understood. In the present study, no statistically significant differences were observed between the SNA and normal groups with respect to neurogenic insults—including peripheral neuropathy, herniated nucleus pulposus, and prior spinal fracture—as well as markers of physical frailty, such as GNRI scores, nonambulatory status, or sarcopenia. However, in a prior retrospective cohort study by Matsubara et al., patients with SNA exhibited significantly higher prevalence rates of nonambulatory status, ischemic heart disease, cerebrovascular disease, and ESRD, along with significantly lower serum albumin concentrations. 10 Collectively, these findings suggest that SNA is strongly associated with systemic frailty and overall poor physiological reserve—rather than being solely attributable to localized neural pathology. Further large-scale, prospective, and multimodal investigations are warranted to elucidate underlying pathophysiological mechanisms, establish causal relationships, and identify modifiable risk factors.
Although neither this study nor prior investigations have identified a statistically significant difference in age between patients with and without SNA, the potential modulatory role of age in neurodegenerative or neuroanatomical changes—particularly peripheral nerve atrophy—warrants careful consideration.10,22 Notably, the cohort reported by Matsubara et al. exhibited a higher mean age and a greater prevalence of comorbidities compared with the present study—differences that may reflect distinct disease stages or population selection biases. One plausible interpretation is that SNA may manifest early in the natural history of PAD, whereas frailty, malnutrition, and functional decline tend to accrue progressively over time. Thus, reduced CSA of the sciatic nerve may represent not merely an epiphenomenon of late-stage systemic deterioration, but rather an earlier, more proximal biomarker of underlying neuropathic or myoneurovascular pathology. Future longitudinal studies should therefore rigorously characterize the temporal evolution of sciatic nerve CSA in relation to PAD progression, symptom onset, functional decline, and clinical outcomes.
Intriguingly, in patients with CLTI, no significant difference was observed in the CSA of the sciatic nerve between the two lower limbs. This observation is consistent with prior retrospective studies, which have demonstrated that the contralateral limb in patients with unilateral CLTI often experiences worse clinical outcomes. 23 These findings underscored that CLTI represents a systemic disease state rather than a purely unilateral manifestation, highlighting the importance of comprehensive bilateral lower-extremity assessment and treatment following the diagnosis of CLTI. Therefore, in subsequent studies analyzing patients with CLTI and bilateral tissue loss, using the mean CSA of the bilateral sciatic nerves may represent a methodologically sound and clinically appropriate approach.
Two potentially valuable theories may explain our significant research findings. First, SNA may serve as an objective indicator of the extent of ‘lower-limb frailty’. Prior studies have shown that frailty is a significant risk factor for amputation events in patients with CLTI. 24 Factors such as low serum albumin levels, sarcopenia, and nonambulatory status—each associated with frailty—could reflect disease severity and predict adverse outcomes in patients with PAD.8,25,26 SNA may result from the combined influence of these contributing factors. 10 In addition, SNA may serve as an indicator of a patient’s muscular and physical activity status. It is well established that physical exercise promotes peripheral nerve terminal branching and enhances motor unit recruitment efficiency, thereby delaying the progression of muscle atrophy. 27 It is therefore hypothesized that patients with SNA may exhibit reduced physical activity levels and be more prone to sarcopenia. These factors—diminished mobility and loss of muscle mass—may collectively contribute to poorer clinical outcomes, suggesting that altered SNA may indirectly act as a predictor of adverse prognosis. Moreover, prior studies have demonstrated that the reduction in CSA of peripheral nerves is predominantly attributable to axonal atrophy rather than loss of Schwann cells. 28 Axonal atrophy leads to diminished synthesis and retrograde transport of neurotrophic factors, thereby impairing neurotrophic support to target tissues. 29 This deficit compromises peripheral nerve regeneration and adversely affects wound healing, particularly in contexts of CLTI or diabetic foot ulcers. Given these findings, future research should focus on elucidating the individual and interactive impacts of SNA, frailty, and hypoalbuminemia on clinical outcomes in CLTI. Investigating the interplay among these factors could enhance risk stratification and inform personalized therapeutic strategies to improve wound healing and limb salvage rates.
Second, our findings may underscore the crucial role of neurovascular coupling in the pathophysiology of PAD and the wound healing process. 30 Although neurovascular coupling has been extensively studied in the contexts of neurodegenerative diseases, major psychiatric disorders, and bone regeneration, its role and implications in PAD remain unexplored and have not yet been documented in the literature.30 –32 In both PAD and wound healing contexts, the restoration of local blood flow is essential for the alleviation and management of these pathological conditions.2,4 Previous in vitro and in vivo studies have demonstrated that peripheral nerve injury induces persistent vascular dysfunction, and results in reduced blood flow perfusion at nerve terminals.11,33 SNA may impede wound healing and compromise long-term limb survival, potentially by diminishing blood flow perfusion to the lower limbs. However, within our cohort, peripheral neuropathy was not identified as a risk factor for either IWH or AFS. In the central nervous system, cerebral small vessel disease induces a spectrum of histopathological alterations (including oligodendrocyte injury, demyelination, axonal damage, and reactive gliosis), which manifest on magnetic resonance imaging as white matter hyperintensities (WMHs). 34 In patients with PAD, a parallel microvascular pathobiology may underlie peripheral neuropathy, particularly in those with advanced systemic microangiopathy. SNA may therefore serve as an in vivo imaging biomarker reflecting the severity of underlying distal microvascular dysfunction in the lower extremities. Overall, the mechanisms underlying neurovascular interactions in PAD and their influence on wound healing remain poorly understood, representing a plausible yet largely hypothetical framework due to insufficient empirical evidence. Further elucidation requires rigorous basic science investigations and large-scale, prospective clinical studies to validate these potential pathophysiological pathways.
Our findings may have significant implications for the refinement and optimization of clinical wound management strategies. Patients with CLTI and concomitant SNA necessitate more sophisticated wound management strategies and rigorous follow-up in wound care. 35 The identification of SNA is also crucial for determining the appropriate level of amputation. Conventionally, transcutaneous oxygen pressure (TcPO2) values between 20 and 40 mmHg are regarded as a ‘gray zone’ in the decision-making process for selecting the optimal amputation level. 36 Nonetheless, for patients with CLTI and concomitant SNA, a more aggressive surgical approach may be justified. In these cases, opting for higher amputation levels may be advantageous to ensure adequate tissue viability, facilitate wound healing, and ultimately enhance clinical outcomes. However, this hypothesis remains to be confirmed through prospective, large-scale studies.
The present study has several limitations that warrant consideration. First, as a single-center prospective study with a relatively small sample size, the generalizability of our findings may be limited. This study is subject to potential confounding factors, including the absence of objective electrophysiological assessments (such as nerve conduction studies and needle electromyography) to rigorously evaluate sciatic nerve function. However, it is noteworthy that despite the modest cohort, the magnitude of the between-group differences in clinical outcomes was striking. The robust effect size supports the biological plausibility of SNA as a potent prognostic marker in patients with CLTI. 10 Second, the study cohort included only patients with CLTI who underwent EVT, excluding those who received surgical bypass. Third, estimating sample size based on conservative adjustments of retrospective data may have introduced bias. The imbalance between groups (1:1.86 ratio) reduced power in the smaller SNA group (n = 19). These limitations require careful interpretation and validation in larger, more balanced cohorts. Fourth, this study did not standardize measurements of the CSA of the sciatic nerve for potential confounding variables—including age, sex, body mass index, and skeletal muscle mass. Future large-scale, population-based studies should employ multivariable regression or other appropriate statistical methods to adjust CSA estimates for these covariates, thereby improving the accuracy and generalizability of normative reference values. Finally, although this study determined that peripheral neuropathy is not a risk factor for IWH or AFS, it did not incorporate comprehensive evaluations of lower-limb neurological function, which could have provided additional insights into the underlying pathophysiology. 37
Conclusions
Sciatic nerve atrophy (SNA) was identified as a predictor for wound healing and AFS in patients with CLTI after EVT. Future research should involve rigorous basic medical studies and large-scale clinical investigations to further elucidate the association between SNA and prognosis in patients with PAD or CLTI, as well as to explore the underlying pathophysiological mechanisms.
Supplemental Material
sj-docx-1-vmj-10.1177_1358863X261439148 – Supplemental material for Sciatic nerve atrophy as a predictor of impaired wound healing in patients with chronic limb-threatening ischemia following endovascular therapy: A prospective pilot study
Supplemental material, sj-docx-1-vmj-10.1177_1358863X261439148 for Sciatic nerve atrophy as a predictor of impaired wound healing in patients with chronic limb-threatening ischemia following endovascular therapy: A prospective pilot study by Xinzhi Yang, Gong Cheng, Pengyu Li, Ziguang Yan, Bihui Zhang, Kang She, Jue Zhang, Guochen Niu and Min Yang in Vascular Medicine
Footnotes
Data availability statement
The raw data underlying this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed the following financial support for this research. Min Yang received funding from the Beijing Natural Science Foundation (grant no. 7242280) and the Capital’s Funds for Health Improvement and Research (grant no. 2024-2-4077); Bihui Zhang was supported by the National Natural Science Foundation of China Youth Fund (grant no. 82200537); and Guochen Niu was funded by the National High-Level Hospital Clinical Research Funding Program (Interdisciplinary Research Project, Peking University First Hospital; grant no. 2023IR02).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.