
Abstract
Background:
Iloprost has been proposed as a pharmacological option for patients with chronic limb-threatening ischemia (CLTI) in whom revascularization is either not feasible or has been unsuccessful. This pilot study aimed to evaluate the safety and effectiveness of intravenous iloprost at low infusion rates via an elastomeric pump at home (EP-iloprost) versus higher infusion rates via a peristaltic pump in the hospital (PP-iloprost) for 1 year.
Methods:
This was a cohort study conducted in ‘no-option’ patients for revascularization with CLTI. The follow-up was 3 years. The primary endpoint was the incidence of drug-related adverse events (AEs); the secondary outcome was the composite of all-cause death and major amputations.
Results:
We enrolled 56 patients who received EP-iloprost as a pilot study. Their outcomes were compared with a cohort of 48 patients who had received PP-iloprost. AEs were reported in 15 (31.3%) patients who received PP-iloprost and in eight (14.3%) who received EP-iloprost (p = 0.038), with the exposure-adjusted incidence rate being 22.7/100 patient-years in the PP-iloprost group and 8.3/100 patient-years in the EP-iloprost group. Although the two cohorts were not well-suited for comparison due to age differences, there were seven (12.5%) deaths and four (7.1%) major amputations in the EP cohort compared with 11 (22.9%) deaths and 13 (27.1%) major amputations in the PP cohort.
Conclusions:
These hypothesis-generating data suggest that low-rate infusion of EP-iloprost at home is better tolerated and potentially more effective than high-rate infusion with PP in a hospital setting.
Keywords
Background
Peripheral artery disease (PAD) is characterized by arterial stenoses and occlusions in the arteries of the limbs. PAD of the lower extremities is a common manifestation of atherosclerosis and can be asymptomatic or symptomatic. Claudication is usually the first symptom and remains stable in most patients with PAD, whereas 15% of these patients develop rest pain or skin lesions. 1 The presence of ischemic rest pain or gangrene has been defined as chronic limb-threatening ischemia (CLTI), a condition associated with high morbidity and mortality. 2 In CTLI, the resting perfusion of the leg is inadequate to sustain viability in the more distal tissues. If not treated promptly, CLTI can worsen rapidly with 1-year outcome rates that exceed 20% for both mortality and major amputation. 3 The first-line treatment consists of open or endovascular revascularization. 2 However, a small but significant proportion of patients with CLTI are ineligible or not suitable for lower-extremity revascularization due to comorbidities or anatomic reasons (‘no-option’). 4 For these ‘no-option’ (or ‘nonrevascularizable’) patients, medical treatment is the only therapeutic alternative and amputation rates are very high. Recently, transcatheter arterialization of the deep veins seems promising for limb salvage and for improving clinical symptoms in no-option patients with CLTI. 5
For over three decades, the only pharmacological option for such patients with CLTI has been represented by prostanoids. 6 Prostacyclin (PGI2) is a prostanoid that inhibits platelet activation and has a vasodilator effect. 7 Iloprost, administered by intravenous infusion, is a potent PGI2 analogue that has been proposed as a therapeutic agent that could favorably alter the otherwise inexorable downhill course of CLTI. 8 In the past, some clinical studies, mainly conducted in ‘no-option’ patients, suggested a significant beneficial effect of iloprost on reducing major amputations.8,9 However, a recent cohort study did not find any benefit of iloprost in patients with CLTI and even suggested a possible deleterious effect. 10 There are different protocols for iloprost infusion, which require different settings. It can be administered via intravenous infusion for 6 hours per day over 28 days, usually in the hospital, with increasing dosage to achieve a maximal dose of 2.0 ng/kg/min, or at a lower dosage for 16 hours per day for 7 days to achieve a maximal dose of 1.5 ng/kg/min. 11 Lower dosages seem to be better tolerated and are possibly more effective. 12 Different iloprost dosages may explain the discrepancy in outcomes of different clinical studies with iloprost. The aim of our pilot study was to evaluate the safety and effectiveness of low-dose intravenous iloprost administration by elastomeric pump (EP) for 24 hours at home.
Methods
Study design
Patients were diagnosed with CLTI if they had all the following: (i) an ankle pressure ⩽ 50 mmHg; (ii) clinical symptoms of PAD, defined by stages 4 to 5 of the Rutherford-Becker classification; and (iii) significant stenosis/occlusion of limb arteries confirmed by duplex ultrasound examination (DUS). Patients with CLTI were considered ‘no-option’ patients if they did not receive revascularization procedures during hospitalization prior to enrollment, or if no revascularization was planned because it was deemed not feasible. We enrolled only ‘no-option’ patients with CLTI when the wound (amount of tissue loss) was < 3 based on the Wound, Ischemia, and foot Infection (WIfI) classification. 13 No-option patients were enrolled if the etiology of CLTI was atherosclerotic PAD or embolic PAD or thromboangiitis obliterans. All patients underwent ankle–brachial index (ABI) determination and bilateral DUS of limb arteries before enrollment, as previously described. 14
During the 3-year follow-up period for each cohort, each patient was seen after 1, 3, and 6 months and then every 6 months at our clinics. For patients enrolled in 2023 (n = 11), the follow-up was 2 years. Board-certified vascular medicine physicians performed DUS at every visit. After enrollment, every patient received a statin plus ezetimibe and a platelet aggregation inhibitor (aspirin or clopidogrel) if not already on therapy. The use of rivaroxaban for the prevention of atherothrombotic events in adult patients with PAD was authorized for use by the European Medicines Agency in 2018, but its use was reimbursed by the Emilia-Romagna health system only beginning in 2020. From Dec 1, 2020, low-dose rivaroxaban plus aspirin was prescribed if the patient was not already undergoing therapy with other anticoagulants or clopidogrel. Antihypertensive therapy was started or increased in the case of blood pressure ⩾ 140/90 mmHg. We advised any smokers to quit smoking for limb outcomes at every visit.
The primary endpoint of the present study was iloprost-related adverse events (AEs). The secondary outcome was the composite of all-cause death and major amputations. Minor amputation (digit and transmetatarsal amputation) was defined as occurring when the functional foot remnant allowed standing and walking without a prosthesis. Major amputations were all other amputations. Information about hospitalizations and cardiovascular events was deduced by reviewing hospital discharge reports.
All procedures involving human participants were performed in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. All patients provided informed consent to the study. This study was approved by the local ethics committee.
Patient data and definition
Patients enrolled in the study were considered to have hypertension if: (i) blood pressure was ⩾ 140/90 mmHg repeatedly, or (ii) documented in the patient’s history, or (iii) the patient was already receiving antihypertensive therapy. Patients were considered to have diabetes if they used glucose-lowering agents or had fasting blood glucose levels ⩾ 126 mg/dL. Obesity was defined as a body mass index (BMI) ⩾ 30 kg/m2. Coronary artery disease (CAD) was considered present in the case of a previous episode of stable angina, or a previous hospital admission for unstable angina, or myocardial infarction, or coronary artery bypass grafting, or percutaneous coronary intervention/angioplasty.
Diagnosis of thromboangiitis obliterans (Buerger’s disease) was made according to the criteria of the International Consensus of the VAS-European Independent Foundation in Angiology/Vascular Medicine. 15 Embolic PAD was diagnosed in the case of an arterial embolus of cardiac origin (mostly atrial fibrillation) or the embolization of an atherosclerotic thrombus from aorto-iliac and popliteal segments.
Infusion at hospital with peristaltic pump (PP)
The device used for hospital infusion of iloprost was a PP. The infusion scheme consisted of one vial of iloprost (a vial of 0.5 mL of solution contains 67 μg of iloprost trometamol, equivalent to 50 μg of iloprost) diluted in saline solution, for a total volume of 250 mL, administered over 6 hours. The target rate of infusion was 40 mL/h if tolerated. Iloprost was administered the first time at the standard dose of 0.5–2 ng/kg/min according to tolerability for 6 hours, reaching the maximal tolerated dose. From the second infusion, patients received the total dose of iloprost by PP in 6 hours and remained in the hospital for the entire 6 hours. Treatment adherence and AEs were measured by direct observation: the nurse in charge of the patient recorded them.
Infusions at home with elastomeric pump (EP)
Patients received intravenous iloprost administration by EP at home according to the presence of a caregiver/family support. The EP had a 100 mL disposable reservoir. It allowed ample mobility and normal day-to-day activities during the infusion. The infusion scheme consisted of one vial of iloprost (a vial of 0.5 mL of solution contains 67 μg of iloprost trometamol, equivalent to 50 μg of iloprost) diluted in saline solution, for a total volume of 100 mL. After the infusion started, patients were observed for 1 hour and then they were free to go home. The length of infusion was 24 hours. Treatment adherence at home was measured indirectly: patients reported the time when infusion finished or if they stopped the EP too soon. In case of symptoms during the iloprost infusion, patients were recommended to stop the infusion and report to our outpatient service.
In the first month, patients with PP-iloprost and those with EP-iloprost received three infusions per week (Figure 1). After 30 days, a clinical examination and DUS were performed. Stable patients continued to receive three infusions per week and were reassessed after 60 days. In cases of clinical improvement, the iloprost infusion was reduced to one infusion per week and continued for 10 months or until the ulcer healed or the rest pain disappeared. In cases of clinical worsening, patients were referred back to the vascular surgery unit, and the iloprost was stopped.
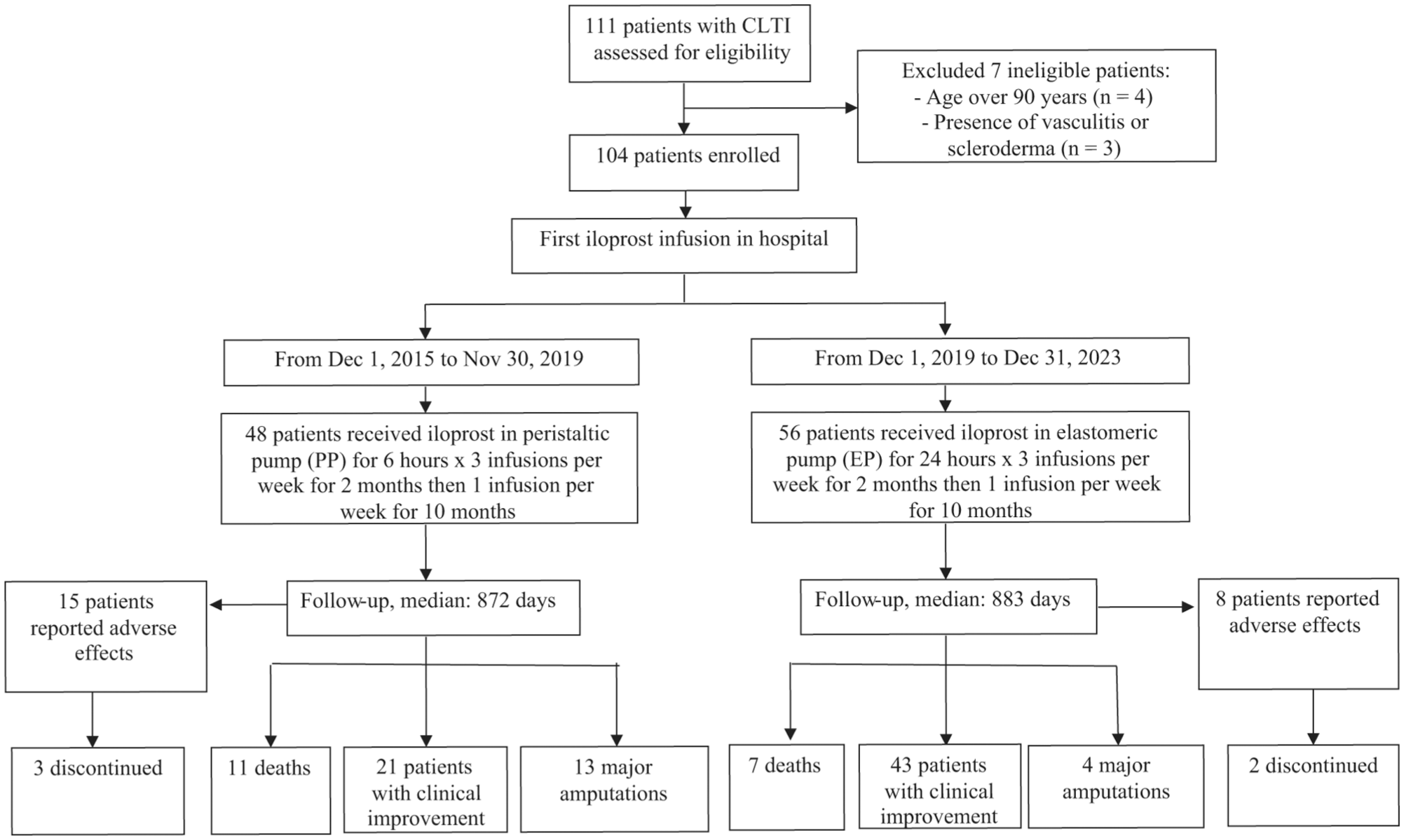
Study flow chart.
Statistical analysis
Continuous variables are expressed as mean (SD), categorical variables are presented as frequencies and percentages. Categorical variables were compared using the chi-squared test or Fisher’s exact tests (two-tailed). Student’s t-test was used to compare means among groups for normally distributed variables. Statistical comparison of the duration of follow-up was performed with the nonparametric Mann–Whitney test for unpaired data. For AE reporting, we used the incidence, calculated by dividing the number of patients experiencing a specific event by the total number of patients exposed to iloprost, and the incidence rate (IR) was calculated by dividing the number of patients experiencing an event by the total exposure time of all patients at risk. For the time-to-first-AE analysis, cumulative endpoint curves were estimated with the Kaplan–Meier procedure, adjusting the data using a fitted Cox model that included age and sex. To test associations between study population characteristics and the secondary endpoint, the Cox proportional hazards model was used. A parsimony model with predictors associated with p < 0.10 was presented to improve precision and avoid overfitting; predictors considered confounders by clinical judgment, though with a p ⩾ 0.1, were also included in the multivariable model. Statistical significance was defined as p < 0.05. The analysis was performed using IBM SPSS (version 26.0; IBM Corp.).
Results
We screened 111 patients: four patients were excluded because they were older than 90 years and three patients were excluded because of the presence of vasculitis or scleroderma (Figure 1). All 104 patients enrolled in the current study had rest pain or acral necrosis. The etiology of CLTI was atherosclerotic PAD in 84 (80.8%) patients, embolic PAD in five (4.8%), and thromboangiitis obliterans in 15 (14.4%) patients; 33 (43.3%) patients had already undergone revascularization by surgery or angioplasty in previous years and five (4.8%) had a previous major amputation. The mean age was 68.7 ± 14.7 years, and men represented 56.7% of the population. The most frequent risk factor was hypertension (72.1%), and diabetes was present in 28.8%, active smoking in 36.5%, former smoking in 28.8%, overweight in 52.9%. Coronary artery disease was present in 28 (26.9%) patients and atrial fibrillation in 13 (12.5%). At enrollment, only 16 (15.4%) patients had low-density lipoprotein (LDL) cholesterol < 55 mg/dL and only 57 (54.8%) were receiving a statin. Regarding treatment, 88% of patients were on antiplatelet agents and 32.7% were on rivaroxaban 2.5 mg BID.
Among the 104 consecutive patients with CLTI, 48 received iloprost by PP and 56 by EP (Figure 1). As shown in Table 1, the patients who received iloprost by PP were older than those who received iloprost by EP (71.9 ± 14.2 vs 65.9 ± 14.7, p = 0.037), whereas BMI, blood pressure, cholesterol, and creatinine levels were similar in the two groups. The frequency of diabetes, smoking, atrial fibrillation, coronary artery disease, and thromboangiitis obliterans was similar between the two groups (Table 1). The WIfI score distribution was similar between the two groups. Rivaroxaban use was more frequent in the EP-iloprost group compared with the PP-iloprost group both at enrollment (41.1% vs 22.9%, p = 0.049) and during follow-up (73.8% vs 22.9%, p = 0.001), whereas the use of anticoagulant agents other than rivaroxaban was more frequent in the PP-iloprost group compared with the EP-iloprost group (31.9% vs 14.3%, p = 0.032).
Characteristics of the study population according to intravenous iloprost administration by elastomeric pump or administration by peristaltic pump.
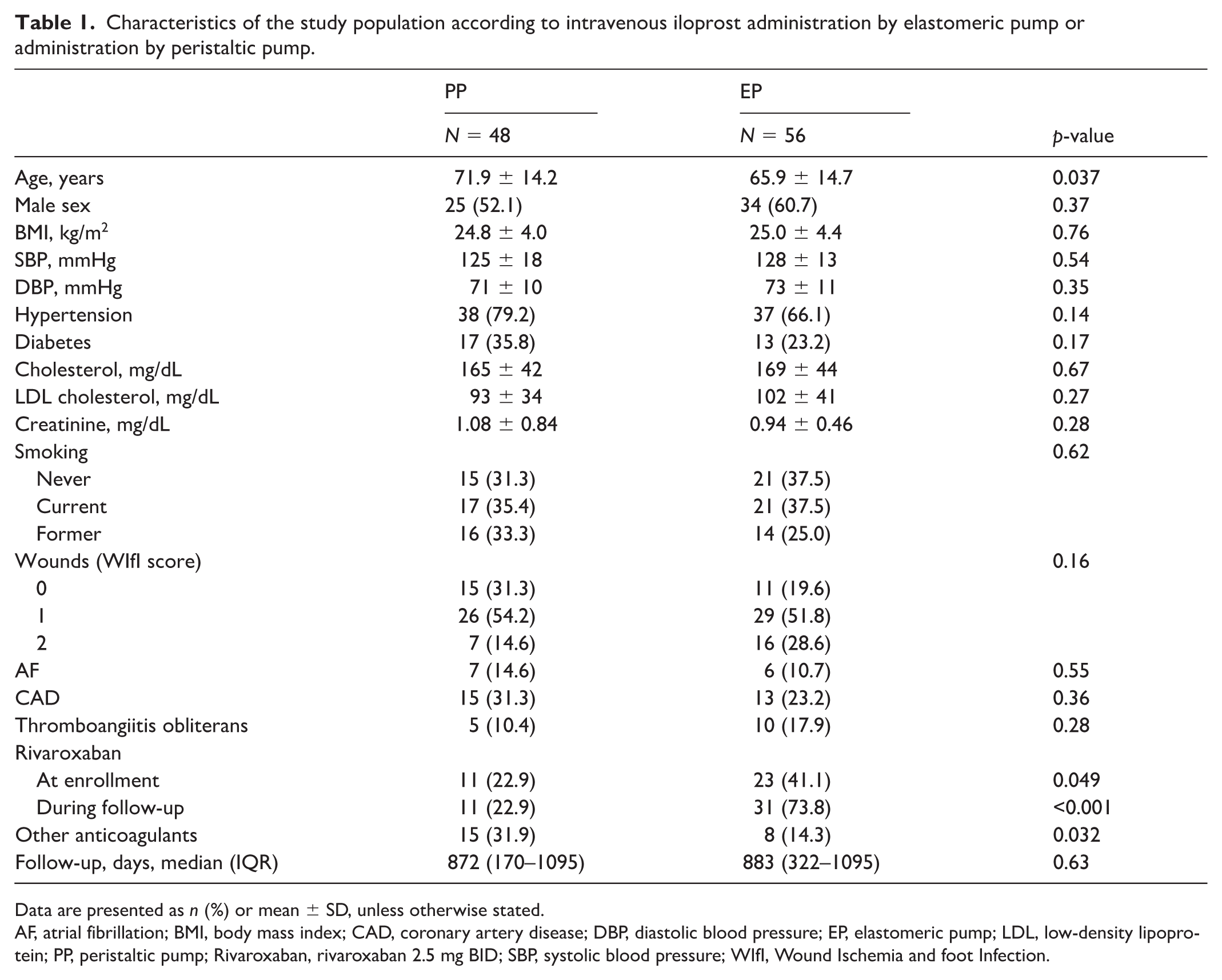
Data are presented as n (%) or mean ± SD, unless otherwise stated.
AF, atrial fibrillation; BMI, body mass index; CAD, coronary artery disease; DBP, diastolic blood pressure; EP, elastomeric pump; LDL, low-density lipoprotein; PP, peristaltic pump; Rivaroxaban, rivaroxaban 2.5 mg BID; SBP, systolic blood pressure; WIfI, Wound Ischemia and foot Infection.
As shown in Table 2, AEs occurred in 15 (31.3%) patients who received iloprost by PP and in eight (14.3%) who received iloprost by EP (p = 0.038). The most frequent side effects were headaches, which were mostly mild and did not interfere with day-to-day activities, and hypotension. All AEs were mild, except for five AEs that led to the discontinuation of iloprost therapy (three in the PP-iloprost group and two in the EP-iloprost group, as shown in Figure 1). Treatment adherence was the same in the two groups. Only one patient in the EP-iloprost group stopped infusion at home, but this was due to the occurrence of an adverse effect (syncope). The AE-IR was 22.7/100 patient-years (95% CI: 14.3–34.2) in patients who received iloprost by PP and 8.3/100 patient-years (95% CI: 4.2–15.4) in those who received iloprost by EP. As reported in Figure 2, the Kaplan–Meier estimated curves for AE-free survival adjusted for age and sex according to the type of iloprost administration show that patients in the EP-iloprost group have a lower risk of AEs than those in the PP-iloprost group (HR 0.39, 95% CI: 0.16–0.96; p = 0.040). The unadjusted cumulative end-point curves estimated with the Kaplan-Meier method showing censoring/events (assuming no systematic differences between censored and uncensored cases) are reported in the upplemental material.
Incidence of common and uncommon adverse events according to intravenous iloprost administration by elastomeric pump or peristaltic pump in patients with chronic limb-threatening ischemia.
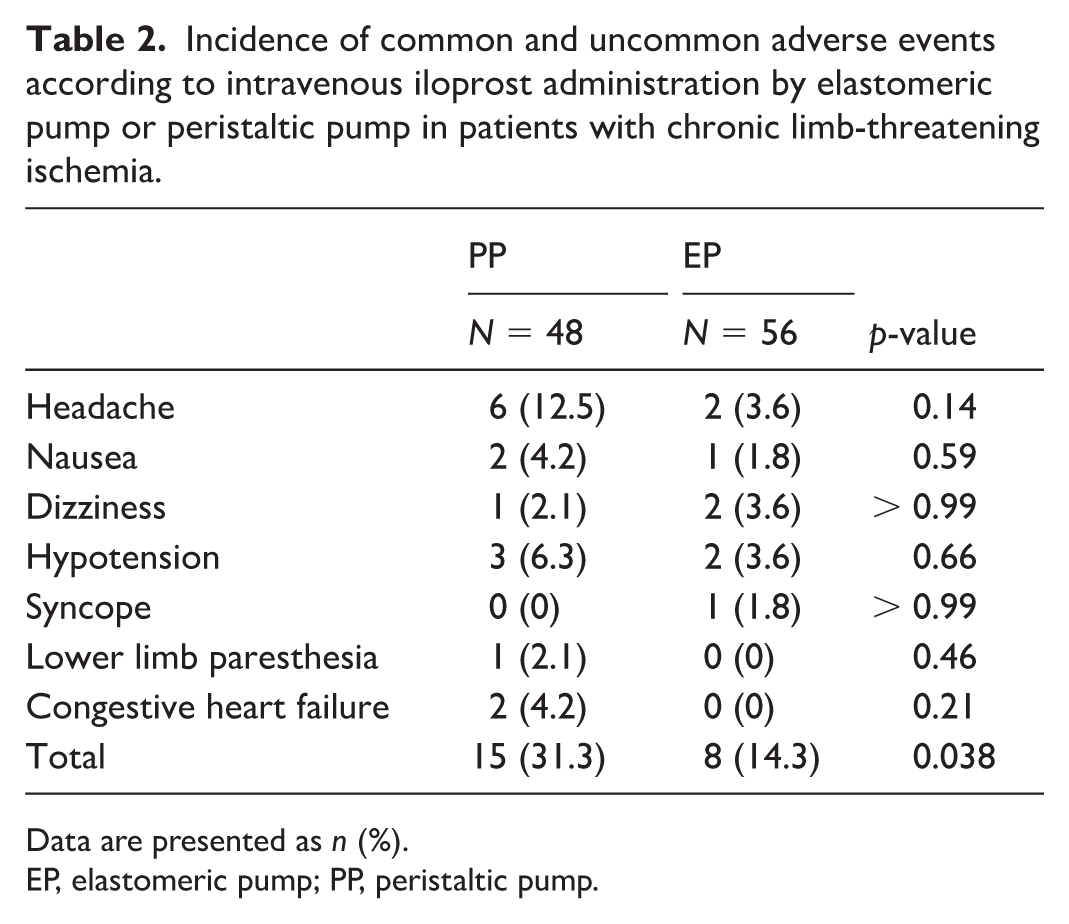
Data are presented as n (%).
EP, elastomeric pump; PP, peristaltic pump.
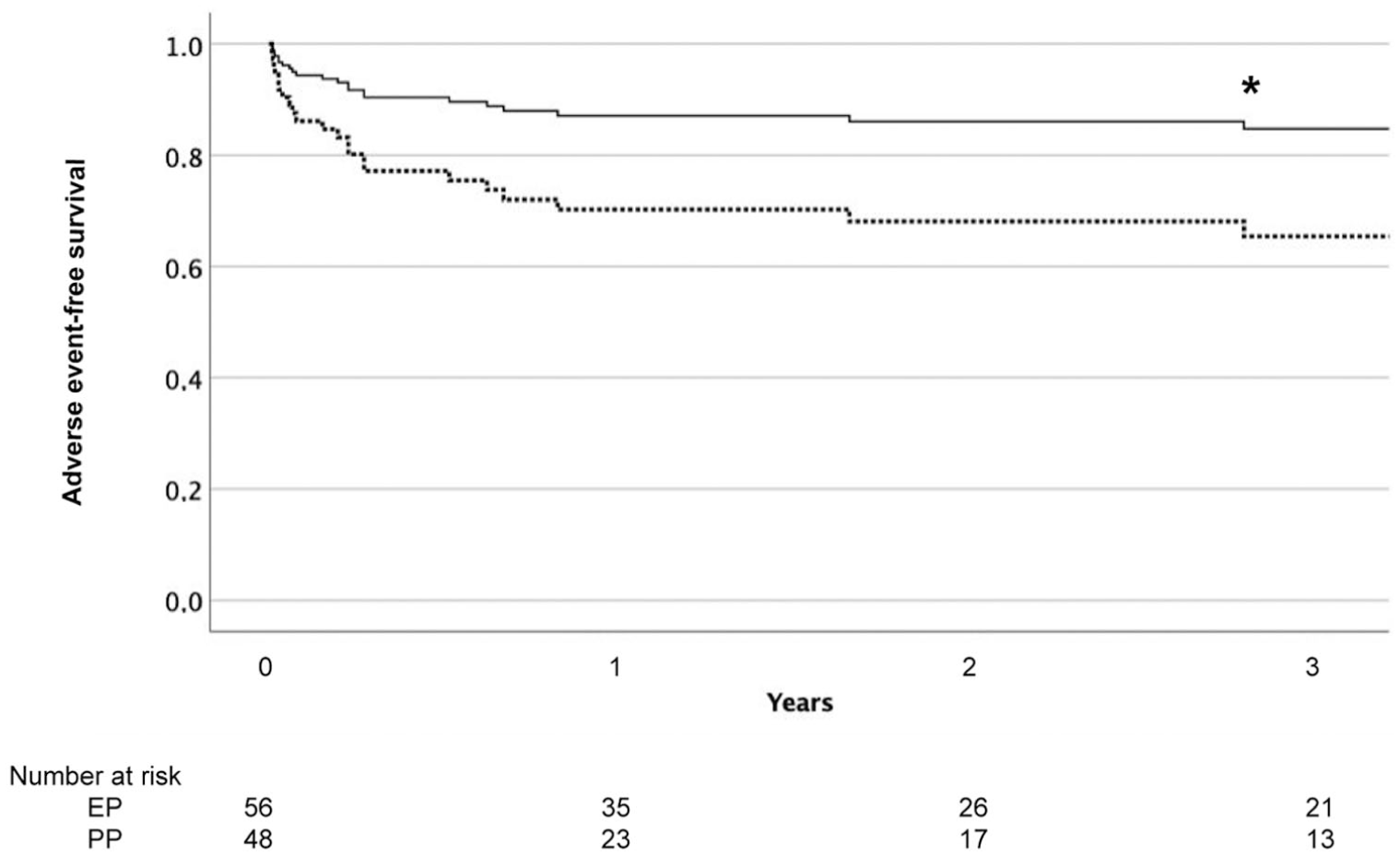
Adverse event-free survival curves adjusted for age and sex in patients with chronic limb-threatening ischemia who received intravenous iloprost administration by elastomeric pump at home compared with those who received intravenous iloprost administration by peristaltic pump in the hospital setting.
During the follow-up, there were 11 deaths (22.9%), 13 major amputations (27.1%), four (8.3%) myocardial infarctions, and three (6.3%) strokes in the PP-iloprost group, whereas seven deaths (12.5%), four amputations (7.1%), two (3.6%) myocardial infarctions, and one (1.8%) stroke occurred in the EP-iloprost group. The incidence of all-cause death and major amputations (composite secondary endpoint) was 26.1/100 patient-years (95% CI: 18.2–35.9) in patients who received iloprost by PP and 9.8/100 patient-years (95% CI: 5.6–16.7) in those who received iloprost by EP. Among patients with thromboangiitis obliterans, there were no deaths or major amputations. In contrast to PAD caused by atherosclerosis, the life expectancy of patients with thromboangiitis obliterans is comparable to that of age-matched controls. For this reason, we excluded patients with thromboangiitis obliterans from the secondary endpoint analysis (univariable and multivariable analysis of the factors associated with secondary end-point reaching during the follow-up in the whole population are reported in the Supplemental Material).
After excluding patients with thromboangiitis obliterans, 68.6% of patients who received iloprost by PP reached the secondary endpoint compared with 31.4% of those who received iloprost by EP. The incidence of major amputation was 16.9/100 patient-years (95% CI: 10.1–26.8) in patients who received iloprost by PP and 4.4/100 patient-years (95% CI: 1.7–10.7) in those who received iloprost by EP. As shown in Table 3, several factors were associated with a higher probability of reaching the secondary endpoint. At univariable analysis, age (HR 1.09, 95% CI: 1.05–1.13; p < 0.001), diabetes (HR 3.14, 95% CI: 1.61–6.11; p < 0.001), and creatinine (HR 1.81, 95% CI: 1.32–2.48; p < 0.001) were predictors of reaching the secondary endpoint, whereas BMI (HR 0.92, 95% CI: 0.84–0.99; p = 0.047), LDL cholesterol (HR 0.99, 95% CI: 0.98–0.99; p = 0.011), and iloprost by EP (HR 0.38, 95% CI: 0.19–0.78; p = 0.008) were associated with a better outcome. At multivariable analysis (Table 3), age (HR 1.10, 95% CI: 1.05–1.16; p < 0.001), diabetes (HR 2.32, 95% CI: 1.10–4.89; p = 0.028), and creatinine (HR 1.77, 95% CI: 1.19–2.65; p = 0.006) were predictors of reaching the secondary endpoint, whereas iloprost by EP (HR 0.41, 95% CI: 0.19–0.88; p = 0.022) was associated with a lower risk of reaching the secondary endpoint.
Univariable and multivariable analysis of the factors associated with the secondary endpoint (composite of all-cause death and major amputations) in patients without thromboangiitis obliterans.
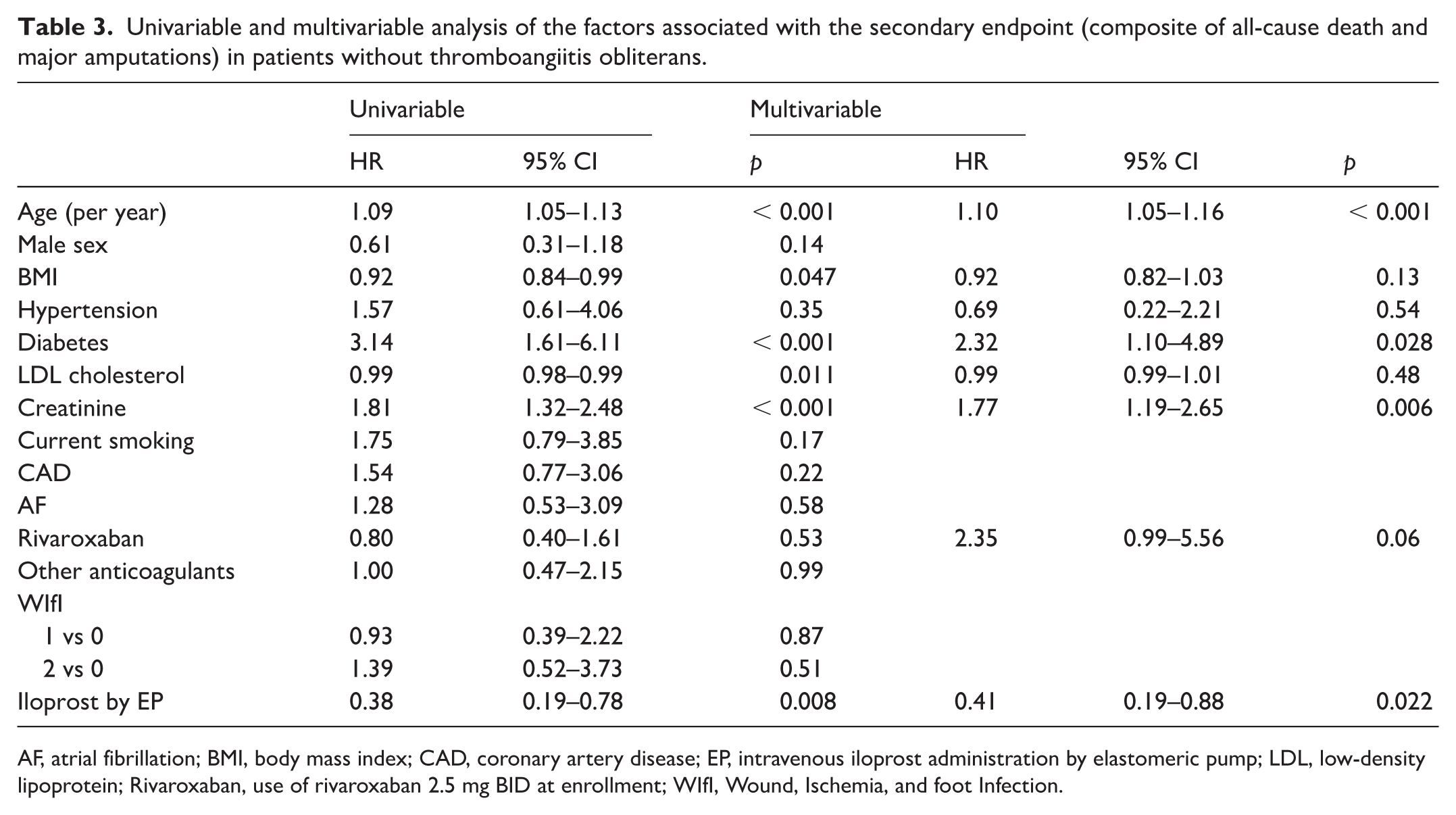
AF, atrial fibrillation; BMI, body mass index; CAD, coronary artery disease; EP, intravenous iloprost administration by elastomeric pump; LDL, low-density lipoprotein; Rivaroxaban, use of rivaroxaban 2.5 mg BID at enrollment; WIfI, Wound, Ischemia, and foot Infection.
Discussion
In this pilot cohort study, the use of EP to administer iloprost continuously for 24 hours at home had fewer side-effects than infusion of iloprost for 6 hours in the hospital setting. The effectiveness on CTLI outcome seemed to be better with the longer infusion at home than for the 6-hour infusion in the hospital, but the two groups were not well-suited for comparison because of the 6-year difference in mean age, so the real impact of the use of EP on CTLI outcome cannot be established.
The first-line treatment for CLTI consists of open or endovascular revascularization. 2 Despite the progress of revascularization techniques, about 20% of patients with CLTI are treated with conservative therapy. The ultimate goal of medical treatment for CLTI is pain relief and avoidance of major amputations.
The use of prostanoids in CLTI is a matter of debate: the European Society for Vascular Medicine (ESVM) guidelines on PAD suggest considering the use of iloprost in patients with CLTI when they are not eligible for revascularization or when revascularization has failed. 16 According to guidelines on the management of CLTI, there are no data to support their use to reduce the risk of major amputation in patients with CLTI. 2 For the multisociety guideline on the management of PAD, the usefulness of prostanoids is uncertain, but their use may be considered when no other treatments are available. 17 Furthermore, a Cochrane review found no benefit of prostanoids in CLTI with regard to both minor and major amputations. 9
Nevertheless, prostanoids are used in everyday clinical practice as a medical treatment for CLTI, mostly because of the lack of alternatives in patients who are not eligible for revascularization or where revascularization has failed.
The term ‘prostanoids’ is somewhat generic because it includes several different therapeutic agents whose actions are not the same. Prostaglandin I2 (PGI2) and thromboxane A2 (TxA2) activate the IP (receptor for prostanoid I) and TP (receptor for prostanoid TxA2) receptors, respectively. 6 Prostaglandin E2 (PGE2) has four receptor subtypes: EP (the receptor for prostanoid E) 1, EP2, EP3, and EP4. Notably, EP2, EP4, and IP receptors are coupled to Gs, and increase intracellular cyclic adenosine monophosphate (cAMP) concentrations. 18 Iloprost is a stable analogue of PGI2 acting on the IP receptor that is expressed on endothelium, smooth muscle, kidneys, neuronal cells, megakaryocytes/platelets, and lymphocytes. 18 In the vascular system, iloprost has vasodilatory effects and platelet antiaggregatory properties. 19 In patients with CLTI, iloprost may reduce thromboxane-dependent platelet activation and platelet-derived pro-inflammatory sCD40L, as well as lipid peroxidation and endothelial dysfunction, leading to a favorable effect on leg perfusion. 20
Several randomized controlled trials have evaluated the effectiveness of intravenous iloprost on ulcer healing or pain relief in patients with PAD21–25 and showed that outcomes were better in the iloprost arm compared with the placebo arm in more than 700 patients. Other types of prostanoid failed to achieve such results. 8 It is important to note that only intravenous iloprost infusion has shown positive results in CTLI, whereas oral administration has demonstrated no effect. 26 Furthermore, an Italian retrospective study showed that iloprost significantly reduced mortality (31% vs 53%) and amputation rates (6% vs 21%) at 5 years compared with untreated patients. 27 For all these reasons, we are using intravenous iloprost in daily clinical practice for ‘no-option’ CTLI.
A recent French cohort prospective study including 201 patients with CLTI who received iloprost did not find any benefit. 10 In fact, it was associated with an increased risk of death and major amputation. 10 The results proposed by the French study are not generalizable: the doses, the routes, and the frequency of iloprost administration were not reported. Moreover, it is unknown how many patients did not complete the entire cycle of iloprost treatment. About 25% of patients enrolled in the French study had extensive deep ulcers or gangrene (wound WIfI = 3). In contrast to the French study, we enrolled patients with rest pain or initial acral lesions (WIfI wound < 3), as it is plausible that the amount of tissue loss should be limited – otherwise there is little that ilopost can do.
The standard therapeutic protocol used in the iloprost trials consisted of intravenous administration by PP at a dosage of 0.5–2.0 ng/kg/min for 6 hours per day in a hospital setting. The hospital setting was deemed necessary to ensure patient safety due to the risk of hypotension during iloprost intravenous infusion. Hypotension is a well-known side-effect occurring during iloprost infusion. 28 In a hospital setting, blood pressure is usually monitored during the infusion, whereas it cannot be monitored at home. However, portable devices for home infusion, such as EPs, are commonly used in oncology for their safety, ease of use, and patient acceptance, and were already proposed for CLTI. 29 Home infusion is better accepted by patients in terms of improved quality of life, it is economic, and reduces overcrowding in hospital facilities. In our study, we did not find more episodes of symptomatic hypotension in patients who received iloprost at home. As expected, the most frequent side effect was headache, which was mostly mild. 30
Until now, there has not been a single accepted protocol for home infusion treatment. We performed this pilot study to evaluate the use of the EP for 24-hour home infusion. A previous Italian retrospective study that enrolled 56 patients with CLTI showed that a portable elastomeric infusion system was similar to or more effective than iloprost administered for 6 hours for 14 consecutive days in the hospital setting. 29 Our data support the use of iloprost home infusion because it is better tolerated and has a lower risk of AEs. This is probably due to the lower infusion rate at home in comparison to hospital infusion. In contrast to the aforementioned Italian retrospective study, in our series, the elastomeric infusion system also had a positive effect on amputation-free survival. Our study was longitudinal, whereas the latter was retrospective and included half as many patients as the present study. We can speculate that the possible benefit of iloprost home infusion on CLTI outcomes may be ascribed to the longer exposure to the drug: our patients received iloprost for several months, whereas in the previous study, patients received iloprost for less than 4 weeks. Moreover, exposure to the drug during the first 2 months was 36 hours per week in patients who received intravenous iloprost at a low infusion rate by EP, which is the double the exposure of the PP-iloprost group (18 hours per week). However, the EP-iloprost group and PP-iloprost group were not well-suited for comparison because of fundamental differences in their age, and therefore the effectiveness of the use of EP on PAD outcome cannot be determined.
Several limitations should be acknowledged. The study population was small, as this was a pilot study. It was not a randomized trial but a cohort study, and this approach could result in several biases. Specifically, patients who received iloprost by PP were older than those who received iloprost by EP. Age was strongly associated with outcome, which can account for the better amputation-free survival rates observed in the EP-iloprost group.
We started using rivaroxaban in 2018, and more patients in the EP group compared with the PP group received it; nevertheless, rivaroxaban was not associated with a better outcome. It should be noted that only 205 patients enrolled in the COMPASS trial had rest pain or ischemic ulcers (5.0% of participants), and only 15 of them reached the endpoint. 31 Similarly, in the VOYAGER-PAD trial, patients with CLTI were a minority (23%). 32
Thromboangiitis obliterans was slightly more prevalent in the EP-iloprost group compared with the PP-iloprost group and patients with thromboangiitis obliterans had a lower mortality and a lower amputation rate than patients with atherothrombotic PAD. However, we excluded patients with thromboangiitis obliterans from the secondary endpoint (composite of all-cause death and major amputations) analysis. The subgroup of the no-option patients with CLTI is not well defined, even though a classification of the no-option patient with CLTI has been proposed. 4
Treatment adherence was measured indirectly for patients who received iloprost at home, and indirect methods tend to overestimate adherence in comparison to direct methods. We cannot exclude lower adherence in patients treated at home, and this could lead to fewer AEs. Finally, some AEs occurred at home and may not have been reported by study participants. It should be noted that the most frequent side effects of iloprost are headache, nausea, fatigue, and dizziness; it is unlikely that the participants did not report or were unaware of these side effects.
Conclusion
The infusion of iloprost via an elastomeric pump for the treatment of CLTI is feasible, safe, and might be more effective than infusion via a peristaltic pump in the hospital. Given these promising preliminary results, future randomized trials are warranted to examine the effectiveness of 24-hour iloprost infusion at home in patients with CLTI.
Supplemental Material
sj-docx-1-vmj-10.1177_1358863X261447258 – Supplemental material for Home-based intravenous iloprost by portable elastomeric pump in chronic limb-threatening ischemia: A pilot study
Supplemental material, sj-docx-1-vmj-10.1177_1358863X261447258 for Home-based intravenous iloprost by portable elastomeric pump in chronic limb-threatening ischemia: A pilot study by Michelangelo Sartori, Elisabetta Favaretto, Elisa Zanata, Sofia Cavara, Alessia Libra, Alessia Sonetto, Enrico Gallitto, Mauro Gargiulo and Benilde Cosmi in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
The data underlying this study are available upon reasonable request to the corresponding author after approval by our ethics committee.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.