
Abstract
We report here on a case of severe pervasive refusal syndrome. This is of interest for three reasons. Firstly, most reported cases are adolescent girls; our case is regarding an adolescent boy. Secondly, he was successfully treated at home and thirdly, the serology showed an apparent infective pre-cursor to the illness with evidence of possible autoimmune serology.
A 14-year old boy deteriorated from a picture where diagnosed CFS/ME developed into Pervasive Refusal Syndrome. This included the inability to move or speak, with closed eyes, multiple tics, facial grimacing, heightened sensitivity to noise (hyperacusis) and touch (hyperaesthesia), and inability or unwillingness to eat anything except small amounts of sloppy food. Successful rehabilitation is reported.
Finally the issue of nomenclature is discussed, raising the question whether Pervasive Refusal Syndrome would be better renamed in a way that does not imply that the condition is always volitional and oppositional, as this can distract focus away from an alliance between family and clinicians.
Introduction
Young people who are affected by chronic fatigue syndrome have symptoms of fatigue affecting both cognitive and physical function associated with other somatic symptoms such as muscle and abdominal pain and sleep disturbance (CFS/ME Working Group, 2002). It is a condition that is thought to be heterogeneous in its nature (Wright & Cottrell, 1999). There is a subgroup of severely affected young people who are bed-bound, may require naso-gastric feeds, and may have heightened sensitivity to sound (hyperacusis) and photophobia. They may also have symptoms of autonomic dysfunction with alteration in temperature control, postural hypotension and major disturbance of circadian rhythms (See Figure 1).
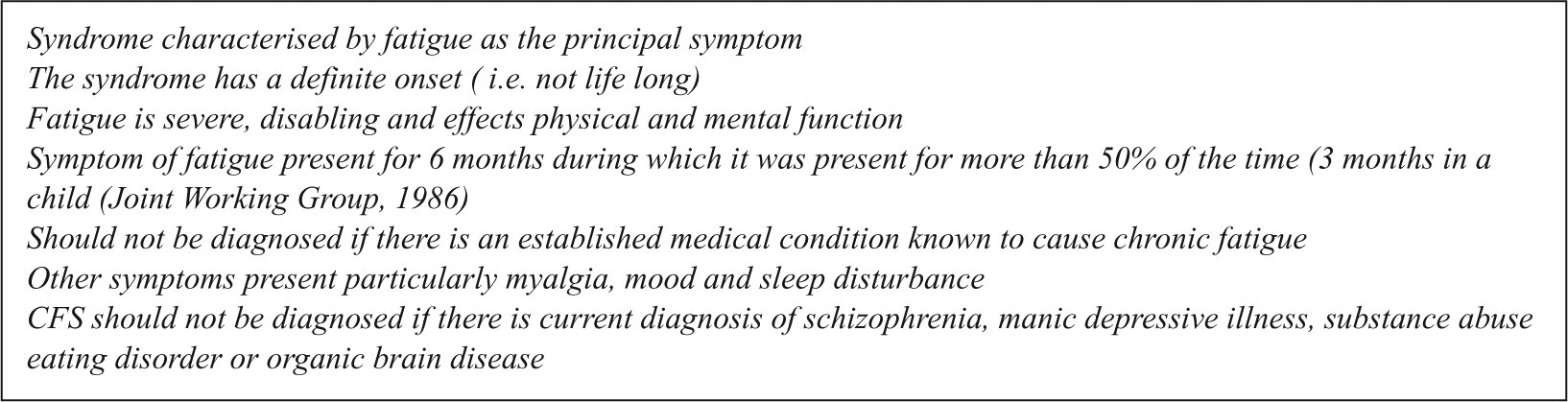
Oxford Criteria for Diagnosis of Chronic Fatigue Syndrome (Sharpe et al, 1991)
We describe a patient who met all the criteria for CFS/ME and in whom the diagnosis was made early; but he subsequently went on to deteriorate to the point where he met the criteria for Pervasive Refusal Syndrome (PRS) (Lask, 2004). This involves a persistent disengagement from those around them with a significant reduction in eating, drinking, moving and speaking (see Figure 2). Its incidence is as yet unknown (Lask, 2004).
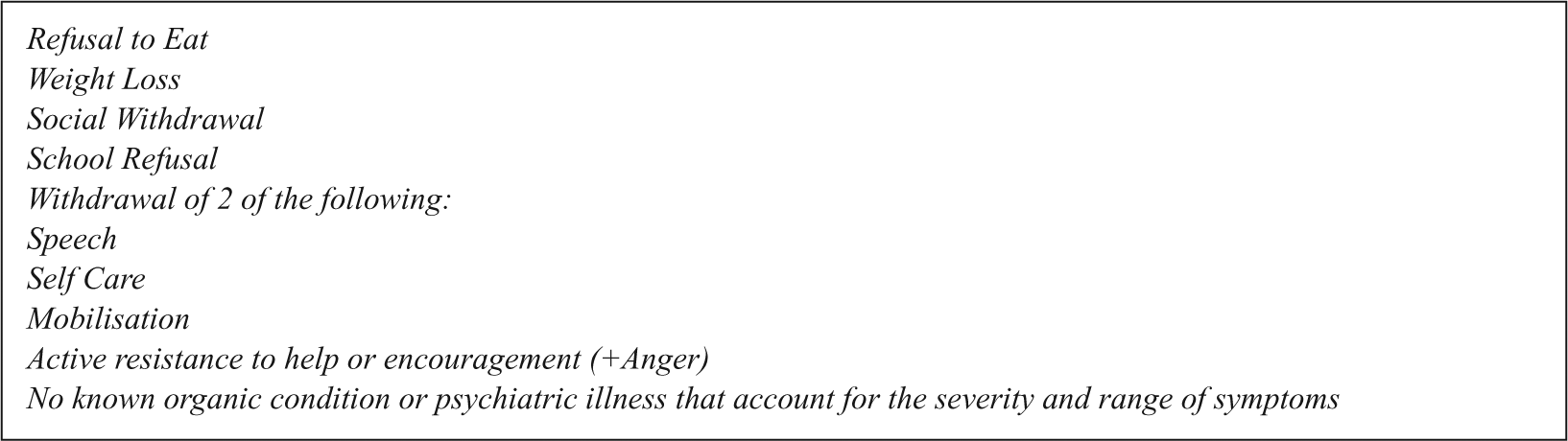
Criteria for Pervasive Refusal Syndrome (Thompson & Nunn, 1997)
Investigation of this teenager found serological evidence of post-streptococcal infection and autoimmune antibodies to parts of the brain responsible for aspects of movement. This throws up a number of questions about whether children with conditions of this nature are a heterogenous group, whether we fully understand their aetiology and how best to provide treatment and support.
Case report
A young man presented at the age of 14 with an influenza like illness. He was unwell for two weeks but was unable to return to full time education because of decreased energy. He gradually deteriorated and was admitted to his local paediatric ward three months later with extreme tiredness, exhaustion after exercise, unrefreshing sleep and an inability to attend school because of the symptoms. There was no evidence of clinical depression. Examination and investigations were normal: these included full blood count, inflammatory markers, renal and liver function tests, thyroid function tests, creatinine kinase, lumbar puncture, viral studies, ECG and EEG, abdominal ultrasound, brain CT and urinary vanillylmandelic acid (VMA). After two weeks he was discharged home with reassurance and encouragement to engage in gentle and limited activity. He was managed in primary care and after a fluctuating course his condition deteriorated further.
He was referred to our paediatric service seven months after his initial illness, and a home assessment revealed that he was unable to use his arms and feed himself, was sleeping down stairs and had to be carried upstairs to be bathed, had to be lifted onto a commode for toileting, and was only awake for an hour each day. He was photophobic wearing sunglasses indoors and had hyperacusis (hypersensitivity to sound). He had little communication with his parents, and no speech.
He was admitted to the inpatient paediatric ward for further evaluation. At this point he had developed facial grimacing and was bed bound and dependent on parents for all his day to day needs. Formal neurological examination did not elicit any other abnormal signs. Investigations at this stage were all normal apart from his ASO titre which was elevated at 480 (normal range <200) and his AntiDnase B 360 (normal range <240). Basal ganglia antibodies were positive as were neurone specific enolase. Consent at this stage was not given by his parents for a repeat lumbar puncture or MRI scan. Encephalitis lethargica was ruled out because while there was lethargy and sleep disturbance there was no evidence of extrapyramidal movements, parkinsonism, oculogyric crisis, ophthalmoplegia, ptosis or central cardiorespiratory features such as hiccough.
The child mental health liaison team was involved. History showed no evidence of trauma or bullying, and school had apparently been going well. He was a high achiever and while not perfectionistic was academically competitive. He enjoyed playing on the computer and had a number of friends, although not close. Having been in a sporting excellence academy he had been let go a few months before. He had been disappointed by this but his parents did not think seriously so. There was no prior history, signs or symptoms suggestive of psychosis, stupor or catatonia.
He lived with his parents and two elder sisters, being very close to one of them. They lived in a detached house in a village. His mother ran her own retail business and his father worked as a skilled worker in a manufacturing business. The family were supportive and protective, but able to engage with clinicians in discussions about his illness and care. There had been marital tensions which their son had worried might lead to separation. Family work took place exploring the pressures he had been under and discussing the conditions necessary to support recovery. A therapeutic trial of Lorazepam and then L-Dopa led to no benefit and were stopped.
He was discharged home with a rehabilitive package of care involving a large multidisciplinary team. He remained mute, bed-bound and his care took place in a darkened room. He wore sunglasses because of the photophobia and those looking after him had to whisper because of his hyperaccusis. It was apparent that despite this care his condition was not improving. A trial of Fluoxetine 20mg daily for 10 weeks made no difference and was gradually withdrawn.
Sessions with his parents allowed open discussion of the mechanism of illness including initial stressors, personality function, family dynamics, physiological consequences of prolonged inactivity, infection and potential autoimmunity.
Because of poor progress consent was given for readmission for revaluation 13 months after the onset of this illness. An MRI scan was normal; in particular there was no evidence of basal ganglia damage. A lumbar puncture was normal, including viral studies and oligoclonal bands. Repeat streptococcal studies showed an anti-DNAse B of 2880. After discussion, it was agreed during this admission that he should receive 2 grams / Kilogram of immunoglobulin over two days.
At this point he was eating only limited amounts of sloppy food. The clinicians agreed he could not go home until he was eating healthily. This was communicated to him and his eating improved the next day. He was discharged home, again with continued multi-disciplinary supportive care. This was planned at a multi-professional meeting and formalized into a multi-disciplinary care plan. A book was kept at the home logging professional visits and recording action plans agreed between the psychiatrist / paediatrician and family working together. These plans were made around seven domains including nutritional intake, mobility and activity, sleep wake cycles, cognitive and educational, emotional and psychological, family and finally the social domain following the Stairway to Health programme of rehabilitative care (Wright et al, 2005). He had visits from a large multi-disciplinary team which included the Paediatrician, Child Psychiatrist, Dietician, Physiotherapist, District Nurse, GP, Community Paediatric Nurses and a Child and Adolescent Mental Health Nurse. At this stage he started to gradually improve and began to communicate his needs initially by facial expression, then by non-verbal vocalization, whispering and subsequently by speech. Concomitant with this he became more tolerant of light and sound. His physical status also started to improve and over a period of many months he started to become more mobile. Individual sessions complimented work with parents (and sometimes parents and siblings) and focused in a cognitive behaviour therapy style on issues to do with aspects of lifestyle, attitudes and coping that would be likely to promote recovery. As progress was made, team members withdrew, and home tutors became involved. When assessed nearly two years after initial presentation he was communicating normally, eating normally, no longer wearing dark glasses, and able to tolerate normal levels of sound. He was socially interacting with his friends and starting to walk his pet dog 250 metres. Individual therapy was stopped although some limited parental support remained. His improvement has continued at a steady pace since then.
Discussion
Most cases of PRS are treated on in-patient wards because of the severity of the problems and the complexity of the treatment. However, as Lask points out (2004) “children experience the therapeutic efforts as coercive” and prolonged admission can promote much conflict both in the family system and between child or parents and clinicians. This case demonstrates that home treatment is possible if good multi-disciplinary care is well planned and co-ordinated, and if nothing else can be achieved in hospital. While it is expensive (professionals visited five days per week) it is cheaper than in-patient care, and allows the child to be in their own environment. We also believe that it removes from the systemic interactions areas of potential dispute than can occur between the different health care professionals concerning who has responsibility for which aspect of care with a chronically ill child with a complex problem in a hospital setting. It brings the parents back into direct contact with the illness and the predicament and gives them a clear role. The fact that he was at home meant that conflicts were not between child/parents and nurses/clinicians, but were more appropriately centred around family interactions, which clinicians supported them to manage. We believe that the desire to be at home was a motivational factor in the recovery of this young man. This is one of few case reports of a child so ill being treated at home.
The diary with entries from family and clinicians provided a narrative of his illness (which was useful during recovery), a helpful way of communicating between professionals, and enabled the family to raise issues promptly for problem solving.
Given that most reported cases of PRS are in girls (Lask, 2004), this also represents one of very few cases seen in boys (Nourse et al, 1999; Taylor et al, 2000; Anonymous parent, 2001). In previously reported cases in boys a severe depressive reaction seems likely in at least two cases of social transplantation and trauma in a fleeing refugee situation (Bodegard, 2005). In one case the child’s young age makes a range of other diagnoses likely (Taylor et al, 2000). In our teenager, depression was absent in the recovery and there was no response to a serotonin re-uptake inhibitor when he was at his most uncommunicative.
We were fascinated by the biochemical findings and felt this merited discussion in the literature. The streptococcus is known to be an organism that is strongly linked with autoimmune disorders. The streptococcus is associated with other conditions such as rheumatic fever, carditis and glomerulonephritis (Cunningham, 2000). In rheumatic fever it is accepted that between 10-20% of patients will develop a clear movement disorder (chorea) between one-six months after infection (Guidelines for the diagnosis of Rheumatic Fever, Jones Criteria 1992 update). This is thought to be through a mechanism where surface antigens from streptococci, which closely resemble human tissue, bind with tissue from the brain as well as heart, skin and joints, as in Sydenham’s Chorea (Husby et al, 1976).
The relationship of the streptococcus with other central nervous system mediated movement disorders has been widely described. In about 10% of cases of acute demyelinating encephalomyelitis (ADEM) (Dale et al, 2001), the streptococcus is thought to be the causative organism, and this form appears to be associated with a higher frequency of movement disorders from other forms. Encephalitis lethargica (EL) (Von Economo, 1931) was original described in 1916 as a condition associated with encephalopathy and sleep disorders with basal ganglia signs. In a recent study of 20 such patients, 65% of patients had evidence of streptococcal infection and all but one had positive basal ganglia antibodies (Dale RC, et al, 2003). Arising from this research paediatric autoimmune neuropsychiatric disorders associated with streptococcal infections (PANDAS) has been characterized as presenting after proven recent streptococcal infection (Murphy & Pichichero, 2002), and has been seen in children where either obsessive compulsive disorder (OCD) or a tic disorder developed post infection (Hoekstra et al, 2005; Swedo, et al., 1997; 1998). This is thought to be autoimmune, in response to attack on the brain. It has been found that raised anti-basal ganglia antibodies have a sensitivity of 95% and specificity of 93% in acute Sydenham’s Chorea (Church et al, 2000) and occur in about 70% of cases. Pavone and colleagues (2004) compared uncomplicated streptococcal infections with those associated with PANDAS and found that 10% of the former and 60% of the latter had raised anti-basal ganglia antibodies. Conditions where movement control is affected have also been subject to reported association including atypical movement disorders (Edwards et al, 2004), encephalitis lethargica (95% compared to 2-4% in differing control groups) (Dale et al, 2003), dyskinesias (Dale, et al, 2004) and restless leg syndrome (Matsuo et al, 2004). There have also been suggestions of an association with anorexia (Sokol MS et al, 2002) which is interesting given some similarities between PRS and eating disorders noted by Lask (2004). However many of these studies report only small numbers of children and have invariably used different ways of examining anti-basal ganglia antibodies and thus reproducibility of these studies has been poor, making (Singer et al, 2004) interpretation difficult. In a review by Martino and Dale (2006) the potential mechanisms by which the streptococcus can cause autoimmune brain dysfunction are discussed with direct attack on movement centres in the brain implicated.
With a high degree of caution it could be postulated that our child’s presentation may have been an autoimmune post infectious disorder of the brain, similar to PANDAS, although this presentation has not previously been reported as associated with PANDAS. He had clear evidence of a streptococcal infection in that his ASO titres and anti Dnase B were elevated and both his basal ganglia antibodies and his neuronal specific enolase were elevated. The response to immunoglobulin in our report may be a therapeutic effect in this context although it could also have been a coincidence. The research evidence for immunoglobulin treatment in severe CFS/ME is equivocal (NHS Centre for Reviews and Dissemination, 2002).
Our patient fulfilled the Oxford (Sharpe, 1991) criteria for the diagnosis of CFS/ME initially in that he had progressive fatigue affecting both cognitive and physical functions and no underlying condition which could account for his symptoms. Other diagnoses were considered including acute demyelinating encephalomyelitis and encephalitis lethargica but these were discounted either because of lack of corroborative investigations or physical features. The diagnosis of pervasive refusal syndrome became the working diagnosis made by the paediatrician and paediatric neurologist after marked deterioration of his symptoms when he met the criteria for this condition.
Whilst our instinct is to be cautious about making any links between PRS and an autoimmune aetiology, we believe it important to report this case. We believe that further research is warranted. It would be helpful to have a systematic study exploring whether there is a subgroup of young people with severe chronic fatigue syndrome and / or pervasive refusal syndrome who have auto-antibodies to brain tissue.
Some believe that PRS is a type of conversion disorder rather than a volitional disorder. Interestingly Thompson & Nunn (1997) make a distinction noting that children with CFS/ME find rehabilitation and treatment “difficult and at times distressing” but do not refuse in the way that children with PRS do. An alternative is to postulate that they are two different expressions of a similar condition as a result of the child’s temperament or the situation in which they find themselves. Our experience is that subtle resistance to rehabilitation in CFS/ME is common. In PRS it is clearer. This young man’s change in symptoms may be a demonstration of change over time, showing two aspects of the same condition as it evolves. How severe stress and illness interact, and how their interactions relate to the finding of anti-basal ganglia antibodies, needs more sophisticated research designs than have been carried out to date.
The role of mental health professionals is to work alongside clinicians in child health services to provide an integrated service. The paediatricians, nursing staff, physiotherapists and dieticians provide aspects of the physical care plan, and liaise with each other and the family. The mental health professionals bring the biopsychosocial model (Wright & Cottrell, 1999) to the fore providing a formulation that brings the attributional, systemic, emotional, social and psychological together with the physical. Good communication and care planning can be systematically discussed with problems being worked through as they arise (Ashby et al, 2006)
Finally, it may well be worth the medical community considering new terminology in the place of pervasive refusal syndrome. Families we have seen report that whilst they value the sensitive way in which the label is applied by clinicians, they can feel stigmatized by it. In some instances family and friends believe it to be suggesting that the child is being wilful, which runs counter to their beliefs about their child or illness in many instances. We suggest a better terminology could be developed once further research is available. This could include a neutral label such as the descriptive Pervasive Withdrawal, Pervasive Inactivity or Pervasive Inertia or a label such as Pervasive Conversion Disorder if research shows a similar aetiology to other conversion disorders. Clearly, were there a subgroup to be found to have an autoimmune aetiology on further research this would be reflected in the diagnostic terminology. Lask (2004) suggested that some cases of PRS may be classified within an as yet undefined category of conditions in which refusal is a key feature, that would also involve selective mutism and school refusal. However he also noted that conversion disorder had “much in common” but was usually less severe.
In this context there needs to be some good methodological research on diagnosis, nomenclature and treatment. The overlap between severe CFS/ME, PRS, neurasthenia, fibromyalgia, and encephalomyelitis lethargica is great and the variability by which clinicians use diagnostic terms is often difficult for families to understand, creates unhelpful conflict between clinicians, and can lead to alteration of therapeutic management that is at best confusing for the patient and at worst potentially damaging. For example, we have seen the “diagnosis” of encephalomyelitis lethargica used as a justification for very limited rehabilitation planning whilst clinicians and family “wait for the illness to spontaneously improve” and this process was damaging for the child until more active management prompted gradual recovery. Terminology that allows sensitively planned and holistic rehabilitative treatment is to be commended.
Footnotes
None.