
Abstract
Practitioners extending their repertoire to include supervising the practice of others may see it as an additional professional activity which may be accommodated within their current identities. For some, it may also become a turning point that requires/promotes a second order development across personal and professional identities. Positioning theory (Harre and Langhove 1999) offers a framework which practitioners can use in making the intellectual and linguistic distinctions between different activities/identities, including the supervisory relationship. This paper further explores how a reflexive awareness of physical position, and an ability/willingness to move and re-position can facilitate the elaboration of both the activity of supervision and the identity of supervisor at the levels of approach, method and technique (Burnham 1992, 1993)
Keywords
I struggled to create a title for this paper. Early candidates such as ‘Making the move from therapist to supervisor’ suggested that it was a permanent transition from one thing to another. A transition that is permanent is unlikely, and most (if not all) practitioners will extend their practice to include supervision, and move between therapy/therapist and supervision/supervisor in one way or another. Skovholt and Rønnestad (1992) used feedback from their survey of 100 counsellors to map out the evolution of counsellors/therapists from pre-training to retirement. As far as I am aware, no such survey has been carried out for therapist-supervisors’ transition. The present paper looks at this transition.
Turning a practice restraint into a supervisory resource
A supervisor in training was supervising a systemic psychotherapist in the final year of training. The supervisor’s own therapeutic practice was as counsellor in a GP's surgery, working mainly with individual adults, sometimes couples. She had no children herself and had no ambition to work with children. The therapist in training worked in a CAMHS (Child and Adolescent Mental Health Service) unit and was skilled in, and enjoyed working with children and young people with their families. The therapist had brought video examples of her agency practice for training supervision on the course. As the supervisor in training watched the video she began to feel uneasy about her ability to supervise/guide/coach/reflect upon the work she was watching, yet felt obliged to say something. As she made some suggestions the therapist frowned and responded hesitantly, not seeming to appreciate the supervisory suggestions. This interaction developed into what Tomm (2006) might call a ‘pathologising interpersonal pattern’ (PIP). The interaction continued in this way to the frustration of both, not only in this episode of supervision but in others too. Each person began to personalise this pattern. The supervisor characterised the supervisee as resistant and not liking her because of various personal Social GGRRAAACCEEESSS (Gender, Geography, Race, Religion, Age, Ability, Appearance, Class, Culture, Ethnicity, Education, Employment, Sexuality, Sexual orientation, Spirituality.) (Burnham, 1992, 2012; Roper-Hall, 1998), while the supervisee was openly contemplating having a different supervisor.
This kind of situation is not uncommon and may arise in a number of situations where there are significant professional differences within the supervisory relationship.
In ‘supervision of supervision’ (SOS) I invited the supervisee in training to think about what position she was supervising from (this was before I had the benefit of a formal theory about positioning). As the conversation proceeded we constructed/named this as ‘experienced therapist’. The supervisor realised that she was relying on her experience as a therapist to supervise. This position had been ‘fit for purpose’ when supervising counsellors working in similar practice contexts to her own. She knew that it wasn’t going well and that she did not have the practical experience to supervise in that way. However, she felt unable to change what she was doing from within her current supervisory repertoire. She found herself ‘resorting’ to a hierarchical identity as in ‘I am the supervisor … so you have to take what I say seriously’ in order to justify her activity. She was unhappy with this state of the relationship and now dreaded working with this supervisee. We began to generate positions, other than ‘experienced therapist’ that she could act from as a supervisor, and to name those different positions. For example supervisor as trainer, mentor, assessor and so on. Naming different positions meant that she avoided slipping into a tacit (default) position and became more able to be intentionally reflexive and select from a repertoire of positions. The ability to act from different positions was improved further by exploring and developing techniques she could use to show and be experienced as acting from each intentionally selected position. A selection of questions developed to ask from a position of supervisor as trainer included:
Of all the cases you could have brought why choose this one?
As you watch this video now what do you notice that you didn’t notice at the time?
If this was a video of another therapist working what might you suggest that she try?
Which of the usual resources that you would use in a situation like this are you feeling restrained from using?
Encouraged by the reflexive effects these kind of questions generated for both herself and the supervisee, the supervisor in training continued, and reported that she was now able to engage in episodes of supervision from a different position and the supervisory relationship became redefined/extended as/to include trainer/trainee. The supervisor no longer felt that she had to act as if she was experienced as a clinician in this area. The supervisee said that now it felt like the supervisor respected her clinical expertise and was supervising her in ways that allowed her to respond to supervision differently. Their relationship improved in other ways too. The supervisor in training said that the more she extended her practical repertoire, the more she began to feel that she had moved from only doing supervision of clinical work, toward becoming a supervisor across a range of contexts.
The following example occurred early on in my experience of training supervisors. It was part of a process of realising this distinction and prompted a revision both in how I practiced supervision and how I trained/supervised other supervisors. In particular it helped me appreciate how the distinction between activity (doing therapy or supervision) and identity (being a therapist or supervisor) shaped this transition. How a practitioner thinks about and positions themselves within and between these (and other) distinctions is likely to influence how they manage this transition, and will be explored in this paper, borrowing from positioning theory as described by Harré and Langenhove (1999).
Moving between activities/identities
Practically speaking, this kind of movement between therapy/therapist and supervising/supervisor may be experienced as a planned distribution between different parts of the week, or agency. Alternatively it may sometimes be experienced as shuttling between different obligations with little time to breathe and re-orient yourself from one thing to another. Emotionally speaking, the ‘things’ that the practitioner is moving between may also not appear straightforward. A practitioner may primarily regard their professional identity as a therapist and so they do supervision, but do not claim an identity as supervisor. Others may, by ambition or surprise, find they prefer the activity of supervision and come to think that they are not only doing supervision but regard being a supervisor as part of their professional identity. Whichever approach (orientation) to supervision a practitioner adopts (and this may change over time), it is important/useful to have methods (ways of organising) and techniques (particular skills) (Burnham, 1992; 1993), that enable a practitioner to make the distinction between the two positions: position as activity (doing supervision) and position as identity (being a supervisor). Drawing further upon positioning theory, Harré and Langenhove (1999) describe it conceptually as:
a dynamic concept which fits within the framework of an emerging body of new ideas about the ontology of social phenomena;
a discursive construction of personal stories that make a person’s actions intelligible and relatively determinate as social acts and within which the members of the conversation have specific locations;
a procedure of making determinate a psychological phenomenon for the purposes at hand;
a metaphorical concept through reference to which a person’s ‘moral’ and personal attributes as a speaker are compendiously collected;
Lest readers should think they are describing a position as fixed or permanent, they (Harré & Langenhove 1999, pp. 20-23) emphasise that, practically speaking:
The act of positioning ‘refers to the assignment of fluid “parts” or “roles” to speakers in the discursive construction of personal stories that make a person’s actions intelligible and relatively determinate as social acts’;
Positions can and do change. Fluid positionings, not fixed roles, are used by people to cope with situations they find themselves in;
One can position oneself, position others and be positioned by others;
A ‘position’ can be specified by reference to how a speaker’s contributions are heard by themselves and others;
Harré and Langenhove (1999) further provide detailed examples of what they call ‘positioning talk’ (p 9) as expressed and indicated through spoken aspects of conversation. One could say that the supervisor in example one (see above) re-positioned herself linguistically by asking different kinds of questions.
I will now explore the contribution that physical positioning and re-positioning can make to how a practitioner moves into and maintains a supervisory posture with individuals and groups/teams.
Achieving professional positions
The process of working towards a particular professional position, and even when it is eventually bestowed through qualification (e.g. as therapist or supervisor), does not necessarily coincide with the emotional experience of feeling ‘really’ eligible/fit to carry out the newly achieved professional position/status. Many practitioners, including supervisors in training, have expressed similar feelings which Brookfield (1994) calls the fear of ‘impostership’ which emerged as one of the findings from his research into the feelings of teachers in training/newly qualified teachers. I have suggested elsewhere (Burnham, 2010) that speaking/acting in the grammar and vocabulary of education and learning can help a practitioner position themselves and be heard as a supervisor rather than a therapist, and can also help to clearly define the relationship with supervisees as supervisory rather than therapeutic (though also transformational). Actively experimenting (Kolb, 1984) with how and where one positions oneself physically/posturally can emphasise an intellectual or emotional position, as well as extending the ability to maintain a supervisory relationship by showing yourself as a supervisor as well as sounding like one.
This is perhaps most clearly illustrated in the example below in the context of live supervision from behind a one way screen.
Are you sitting too comfortably?
At one mid-year review, one of the things a group of supervisees told me was that I had a particular seat that I sat in and they always left for me, because that was the one that I seemed to prefer. They referred to it as ‘the supervisor’s seat’, and I just thought it was where I sat! Harré and Langenhove (1999) call this non-conscious positioning as ‘tacit’ or ‘first order positioning’ (p. 22) and others refer to it variously as a default position, a habit, something we regularly do without much thought. Indeed I had not given this physical positioning any conscious thought for some considerable time. As soon as we begin to talk about a position we move into second order positioning, and this opens the possibility for our positioning to become ‘intentional’, implying that we have choice. So, looking at ‘the supervisor’s seat’ more closely, it was beside the screen and literally alongside the therapist’s chair on the other side of the screen. We all adopted our usual seats with the intention of considering what I could see from this position. I noticed that I was looking at the family/client (like the therapist). It seemed likely to make me think about the family and draw more on my resources for doing therapy and acting as a restraint to my intention of being a supervisor for the therapist’s work with the family. Actively experimenting with different seating positions opened different possibilities for seeing differently and focussing on different aspects of the session. When I physically re-positioned to keep the therapist in view it helped me to keep them in mind and encouraged me to use my resources as a supervisor/trainer. This meant noticing more about the practice of the therapist/trainee. I was able to write down the observations (comments and questions) for them to reflect upon between sessions, including when they were reviewing recordings of their sessions. Previously I wrote ‘Notes from the supervisor and other supervisees in the team can develop into “narrative means to training ends” [after White and Epston (1991)]’ (Burnham, 1993). Continuing this narrative theme by writing down the noticings for the supervisees may be thought of as a kind of learning letter. I also began to notice that it helped me to move out of the position of ‘frustrated therapist behind the screen’ and into a more ‘attentive supervisor/trainer’. This did not mean that I permanently swapped one position/seat for another. I now, literally as well as metaphorically, had at least two positions to sit in, and movement between them offered what Bateson called ‘double description’ (Bateson, 1979, p. 21) and hence a broader range of possibilities for activity as a supervisor. Making an intellectual re-positioning visible to others by moving physically can make the intentionality of the re-positioning more explicit in relation to the other participants, who then can consider their own opportunities for re-positioning.
According to Harré and Langenhove (1999) positioning is a discursive practice, where psychological phenomena are understood to be situated in and emerging from interpersonal interaction.
‘In any discursive practice, positioning constitutes the initiator and the others in certain ways, and at the same time it is a resource through which all persons involved can negotiate new positions’. (p. 9.)
As I re-positioned so, over time and in different ways, other team members were able to actively experiment, and taking different positions physically promoted different views and relationships with the clinical work and training process.
Becoming aware of this aspect of my own supervisory practice enabled me to notice it in the practice of others during supervision of supervision (SOS) and facilitate others to become aware of the effects of their positioning.
The practical effects of intentional positioning
A supervisor in training presented for ‘tape to tape supervision’ (Burnham, 2001). The DVD featured the supervisor in training providing retrospective supervision for an individual practitioner working with a family. Watching the DVD (in the absence of the supervisor in training) I noticed in particular, and recorded in my audio SOS recording, that a) the supervisor in training drew a family tree on the board without including the therapist in the diagram, and then b) spent most of the time looking at the family tree whilst talking about the work in hand. Both of these aspects potentially keep the supervisor in the position of experienced clinician. The supervisory conversation proceeded to be useful in terms of the thinking about the family, but missed a number of opportunities to discuss the worker-family relationship.
In her reflections on these SOS remarks, (and in contrast to my tacit/default/non-conscious positioning in example 1) the supervisor in training said she was deliberately (intentionally) positioning herself so as not to look at the supervisee. When a positioning is intentional it would seem necessary (in Kolb’s terms) to spend some time reflecting before moving to active experimentation (Kolb, 1984). Our reflections on her positioning prompted the supervisee to say that where she looked was a significant cultural, family and personal issue for her (related to issues of politeness). She was also hesitant to look at the supervisee because of the uncertain nature of the relationship she had with the supervisee, and did not want to appear intrusive or challenging by maintaining her gaze. She had not realised the practical effects of doing her supervisory practice in this way, and felt that this awareness made her more mindful of where she looked. This SOS discussion opened space for her to actively experiment in this area and extend her repertoire of supervisory positions and postures.
For my own, more general learning as a trainer it may be that
a) If a person takes a position unintentionally (e.g. ‘I didn’t realise there were other ways to do it’), then it may be appropriate to go straight to active experimentation with different positions which they may then add to their repertoire. However, during the process of actively experimenting, the practitioner may become aware of aspects of their experience that were restraining them from moving position and then reflection is more necessary as a step towards active experimentation.
b) If a person is already aware that they intentionally take a position regularly then it may be more appropriate to spend some time reflecting on these intentions, at different levels, to explore potential restraints on experimentation.
The examples so far have focussed on supervision as activity and how physical positioning and re-positioning can extend the repertoire of methods and techniques used in the doing of supervision differently. The next example looks at exploring supervisor as identity, which is more related to a practitioner’s approach to the work they do: their values, passions and lived experience, which influence the theories they find attractive and the aspects of practice they feel most committed to, and which express how they prefer to see themselves and be known by others. Examples of these different activities include: therapy; supervision; management; teaching; training; research. In this instance we are looking at therapy and supervision.
Self/position as therapist and self/position as supervisor
Through my own experience as a supervisor, conversations with other supervisors, reading (e.g. Burck & Campbell, 2002), and as a trainer of supervisors, I have come to learn that the relationship between ‘self/position’ as therapist and ‘self/position’ as supervisor is not only an important issue early on in training as a supervisor, but may well continue to be important throughout a practitioner’s career, especially if one continues to be passionate about one’s practice as a therapist. In anticipation of this process I invite supervisors in training groups or during CPD (Continuing Professional Development) workshops to perform the following exercise to bring forth this issue for consideration and development. The example below contains the instructions of the exercise as well as some commentary about its use with a particular supervisee.
Positioning oneself as an ‘Experienced Therapist’ or ‘Novice Supervisor’
I was addressing this issue with members of a group of supervisors in training, and one person volunteered to explore this issue through a non-verbal method ‘paper-play’ (Burnham, 2012) which has a resemblance to miniature sculpting with some interesting differences. In the presence of the other trainee supervisors we went through a process as follows.
I asked him to:
Although I had deliberately used the phrase ‘members of the supervision group’ he had not, as yet, used a piece of paper to include himself, and so was less likely to take a ‘second order view’ in thinking about his position in the group. So I asked him to:
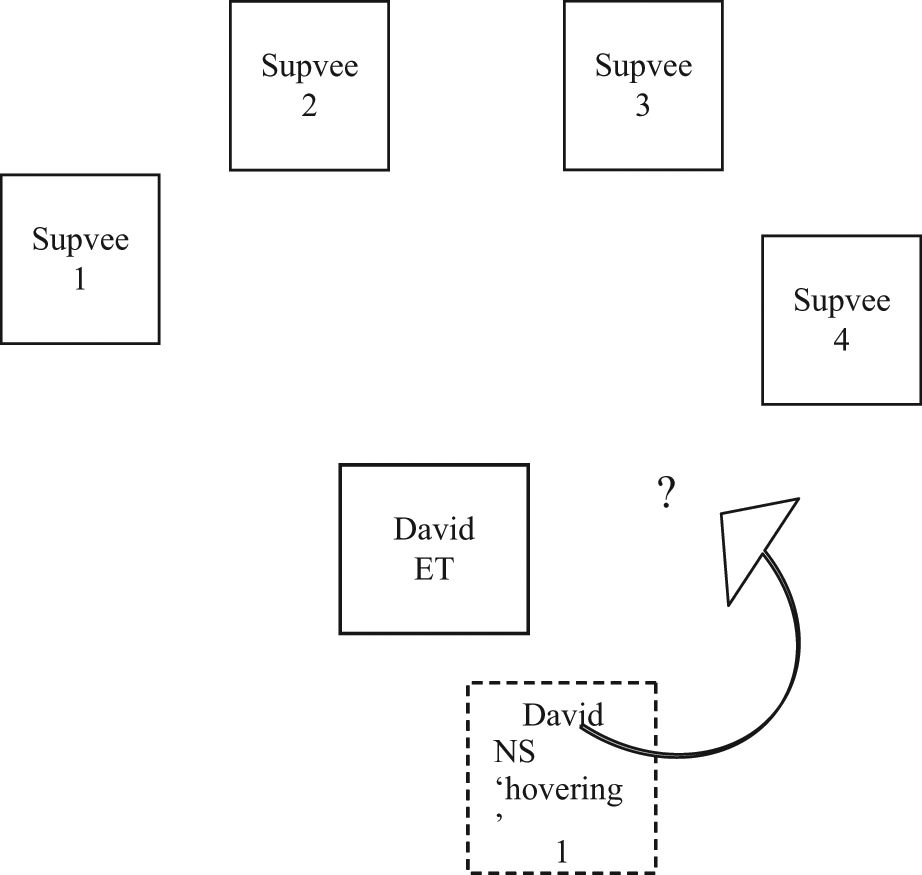
I asked ‘David who.?’ He looked puzzled. ‘David the experienced therapist or David the novice supervisor?’ (Each member of the training group had described themselves as such earlier on in the day). He continued by making two pieces of paper (of equal size, though in retrospect I could have asked him to consider using different sizes if that showed the differences between the two identities more clearly), and writing ‘David the experienced therapist’ in quite bold, confident letters on one piece of paper, and ‘David the novice supervisor’ in less bold writing on the other.
I asked him to position the two Davids in relation to the group. He showed (see Figure 1) David ET as much closer to the group and David NS as positioned behind and to the side of David ET. He described that position as ‘hovering on the edge’.
David gave me permission to move some of the papers as a way of/supplement to asking questions (show and ask). As shown in Figure 2, I slowly began to move the piece of paper marked ‘David NS’ into the supervisory group in front of ‘David ET’, while asking ‘what would happen if David NS was bold enough to choose to take a different position…’ David (in the room) reached out his hand and moved David ET across, effectively ‘blocking’ David NS, whilst chuckling to himself. I asked what does David ET think/feel about David NS? David replied ‘He doesn’t trust him!’ This statement came as something of a revelation to David. He thought that if ‘let loose’ or given more freedom, David NS would want to experiment with some of the things he had been learning on the course and lose focus of what was clinically significant for the client. So he kept David NS ‘in check’.
We went on to discuss the relationship between David ET (associated with safe practice) and David NS (associated with uncertainty). David gradually began to consider that it was more possible that he could position himself in ways that paid attention to both and achieve positions of what Mason (1993) has referred to as ‘safe uncertainty’.
In a recent email exchange with David about this exercise, he commented that:
‘It was good to be reminded as it set me thinking about positioning oneself in other roles too, such as teacher, consultant and, latterly, manager as I have just taken up a more senior lead role in the team I am in. Becoming a manager to team members who were peers before is an interesting challenge for someone who tends to value heterarchy over hierarchy, and collaborative over authoritarian behaviour. You have set me thinking about the importance of marking the change of position, acknowledging the wearing of different hats and the helpfulness of reminding ourselves that labels such as supervisor or expert or manager or clinician are designations that don’t necessarily need to be ‘fixed’ but used as opportunities to see dilemmas from different perspectives’.
Relationship between David as Experienced Therapist (ET) and David as Novice Supervisor (NS).
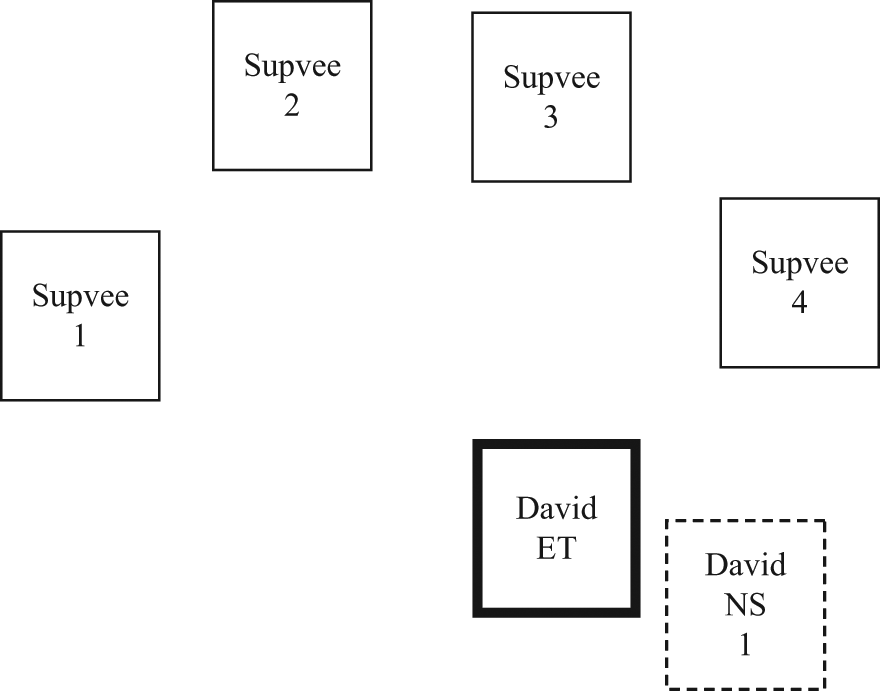
David as Novice Supervisor (NS) makes a move – blocked by David Experienced Therapist (ET).
The examples so far have, perhaps, reflected the common situation where we think about the relative supervisory positions as: the supervisor as the experienced practitioner and the supervisee as the less experienced peer or trainee. In this next example, the positions are reversed and new possibilities are explored using the senior/more experienced therapist in the room as a resource for the supervisor in training to use with the trainees behind the screen during live supervision.
Trainee supervisor and experienced therapist
Recently a supervisor in training was leading a group comprising of a qualified and very experienced psychotherapist/registered supervisor, a nurse trained to intermediate level and a Relate-trained person who was a volunteer within the agency. The group was assembled for the purposes of training. The experienced therapist was in the room with a family whom she knew well and the session was going well with the family reporting improvement. Behind the screen the supervisor continued to supervise the session and was looking and listening for clinical issues. In post-session I suggested that when the therapist could do the session without the ‘need’ for live supervision then the supervisor could have regarded the session as a demonstration interview and shifted to a training supervisor for the two team members behind the screen. Some example questions were:
As you are watching the session, which of your learning/development goals seem most relevant?
As you watch the session, which of the theories are coming to life, helping you to understand the session?
Which practices that you have read about do you see in action? When do you think an opportunity was lost to use a particular practice for the family’s advantage?
Which practice might you feel inspired to use now that you have seen how this family responded to it?
Which theories might help you to understand this family’s situation?
Again this indicates that different supervisory positions generate different kinds of opportunities, and different kinds of curiosities reflexively facilitate different positions.
Further reflections
Initially my own experience as a supervisor led me to observe those times when it is tempting for practitioners to supervise from the tacit/default position (Harré & Langenhove, 1999) of ‘experienced clinician’. This is when a supervisor, at whatever stage of their development, tends towards using their experience of working with clients to guide the work of others, often in a kind of apprenticeship model. This can often be effective especially when the clinical work of the supervisee is in the same agency/discipline/model of the supervisor. This arrangement is often relevant and should be made clear especially when a supervisor has seniority and clinical responsibility for the supervisee’s clinical practice (see Hawes, 1998). Once one moves out of this sameness into difference then a supervisor requires a more extended repertoire of positions from which to supervise. On the other hand, the more I observed and experienced the practice of other supervisors, the more I realised that some supervisors began/worked from the tacit/default position of mentor/coach and underplayed the contribution their own clinical experience could make to the supervisory process. Therefore supervisors may practise from a variety of positions, whether that position is tacit or intentional. Whichever position a supervisor begins from or comes to prefer it is, perhaps, part of their training/CPD to extend their repertoire in order to enhance their ability to create a supervisory relationship with different supervisees through relationally reflexive practices (Burnham, 1993; 2005). The concept of positions and the associated practices of positioning can help supervisors to re-position, in order to consider and actively experiment with different positions intentionally. When active experimentation (Kolb, 1984) and relational risks (Mason, 2005) take place at the levels of approach, method and technique, new positions can emerge and be confirmed. Thus well-developed default positions may well continue to be your favourite resource, but not necessarily restrain you from playing with other, less familiar but in time equally useful positions.
In conclusion to this paper let me reconsider the title that I struggled to create. Phrases such as ‘moving between’ or ‘tacking back and forth’ sound more dynamic than moving from – to. In this way one can work towards being able to use your abilities in each position. It may then become possible to develop a reflexive relationship between these activities/identities. One can use the abilities associated with the identity of ‘experienced practitioner’ to develop but not limit supervisory abilities, and use the abilities associated with the identity of supervisor to enhance clinical practice. One of the things that supervisors at various stages of development have said is that an unexpected benefit of training as a supervisor was that it improved their practice as a therapist. They found that as they became more conscious of practice and theory issues through explicit study of, and explaining to supervisees, so it confirmed their praxis of both therapy and supervision.
Footnotes
Acknowledgements
Thanks go to Alison Roper-Hall, Barry Mason and Sarah Walther for their helpful comments on earlier drafts, and to Andrea Eghartner and David Amias for their contributions to the examples.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
None declared.