
Abstract
Several studies have earned Attachment Based Family Therapy (ABFT) the designation of a promising empirically supported treatment for adolescents with depression. This study evaluated the feasibility of importing ABFT into a hospital-based outpatient clinic in Norway. This article documents the challenges of initiating and conducting research in a real world clinical setting and training staff therapists. It also reports on outcomes of a pilot randomized clinical trial. Implementation barriers rapidly emerged in relation to hospital administration, infrastructure development, and therapists. Despite these barriers, 20 clinic-referred adolescents were randomly assigned to ABFT (n= 11) or to Treatment as Usual (TAU) (n= 9). Adolescents in ABFT showed significantly better symptom reduction compared to adolescents in TAU with an effect size of 1.08. While preliminary, this study suggests that Norwegian clinical staff therapists could be engaged in learning and delivering ABFT, and in producing promising treatment results. The importance of institutional support for dissemination research is highlighted.
Introduction
Major Depressive disorder (MDD) affects about 5% of adolescents (Birmaher et al., 2007; Costello, Erkanli, & Angold, 2006; Lewinsohn, Clarke, Seeley, & Rohde, 1994) and is on the rise both internationally and in Scandinavia (Lewinsohn et al., 1994; Wichstrom, 1999). Not surprisingly, depression is the largest reason for referral to specialty mental health services for adolescents (13–17 years) in Norway (Krogh & Bukten, 2011). To date, anti-depressant medication and Cognitive Behavioural Therapy (CBT), alone and in combination, have received the most research attention for treatment of this population (Brent et al., 2009; Goodyer et al., 2007; March et al., 2004). However, in the largest and most rigorous study to date – the Treatment for Adolescent Depression Study (TADS; March et al., 2004) – combined treatment only produced a recovery rate of 37% at 12-week post-treatment (Kennard et al., 2006). These disappointing results have encouraged the leaders of the field to promote testing of alternative treatments that could stand alone or augment CBT and/or medication. (Brent, 2006; Jensen, 2006).
Family factors in treating youth depression
Several reasons suggest that family therapy could make a substantial contribution to treating depressed youth. First, negative family functioning (e.g., lack of parental support, high levels of conflict, poor communication, over-controlling parenting, and increased rejection) is a strong risk factor for youth depression (Restifo & Bogels, 2009; Sheeber, Hops, & Davis, 2001). In contrast, family cohesion, emotional support, and appropriate parental supervision are protective factors that can buffer against the stressors that lead to or exacerbate depression (Sheeber et al., 2001). Second, family conflict is frequently a negative moderator of treatment outcome (Asarnow et al., 2009b). For example, in TADS, parent reported mother–child conflict predicted poor outcome at 12 weeks of treatment; youth that reported parent–child conflict did not fare well with CBT (Feeny et al., 2009). Third, parental depression and other psychopathology affect the family context and are risk factors for the onset and maintenance of depression in children and adolescents (e.g., Cummings & Davies, 1994; Rutter & Quinton, 1984). Treatments that target these contextual/relational problems could reduce family tension and create a better learning enviroment for CBT skills. Some CBT treatments have added family psychoeducational components (March et al., 2004), but these augmentation studies fail to help families work through their conflicts that might fuel interpersonal hostility and thus depression (see Diamond & Josephson, 2005).
Attachment Based Family Therapy – a promising family treatment
One promising family treatment is Attachment Based Family Therapy (ABFT) (Diamond, Reis, Diamond, Siqueland, & Isaacs, 2002; Diamond, Siqueland, & Diamond, 2003; Diamond et al., 2010). ABFT is a manualized, empirically-based, brief (i.e., 12 to 16 week) approach designed and developed specifically to treat depressed and suicidal youth. ABFT emerges from interpersonal theories that suggest that adolescent depression and suicide can be precipitated, exacerbated, or buffered against by the quality of interpersonal relationships in families (Gotlib & Hammen, 1992; Joiner & Coyne, 1999). ABFT is a trust-based, emotion-focused psychotherapy model that aims to repair interpersonal ruptures and rebuild an emotionally protective, secure-based, parent–child relationship.
The treatment focuses on two key processes: first, on repairing or strengthening attachment and second, on promoting adolescent autonomy. The model is emotionally focused, but provides structure and goals, thereby increasing the therapist’s intentionality and focus. This treatment aims to specifically target important attachment processes such as a) increasing parental availability and emotional attunement, b) improving the family’s capacity for affect regulation, c) resolving experiences of loss or trauma (defined broadly), and d) improving communication and interpersonal problem-solving in the parent–adolescent dyad. These reparative processes rest on the assumption that attachment strategies or expectancies are open to revision, based on new experiences across the lifespan (Bowlby, 1969; Crittenden, 2005).
Empirical support for ABFT is growing. One study randomized 32 clinically depressed youth to ABFT or a wait-list control condition (Diamond, et al., 2002). Eighty-one percent of the patients receiving ABFT no longer met criteria for major depressive disorder (MDD) compared with 47% of the wait-list cases. At six months, 87% of patients treated with ABFT did not meet criteria for MDD (no control group at that time). Generally about 40% of youth treated for depression do not seem to receive adequate treatment gains (Birmaher et al., 2007), thus the outcomes achieved with ABFT in this study were preliminary but promising.
Another study was funded by the Center for Disease Control and Prevention and aimed to reduce adolescent suicide ideation (Diamond et al., 2010). Sixty-six youth with clinical levels of suicide ideation and depression were randomized to ABFT or Enhanced Usual Care (EUC). The results of this study were promising: those treated with ABFT had better treatment retention and significantly greater and faster reductions in suicidal ideation at post-treatment. Additionally, they were four times more likely to report BDI (Beck Depression Inventory) scores in the non-clinical range at mid-treatment at an average of six weeks after onset of treatment and also 2.3 times more likely at follow-up, compared to EUC. Finally, the data have indicated that ABFT is effective for more severely depressed adolescents and those with a history of sexual abuse (Diamond, Creed, Gilham, & Gallop, 2011; Diamond et al., 2010), factors that predicted poor response in earlier CBT studies (Asarnow et al., 2009a; Barbe, Bridge, Birmaher, Kolko, & Brent, 2004; Curry et al., 2006). These studies have earned ABFT the status of “promising” empirically supported practice (David-Ferdon & Kaslow, 2008; Proven Practice Network Newsletter, 2011).
Barriers to disseminate empirically supported treatments (EST) in community clinics
A 10 year up-scaling of the Child and Adolescent Mental Health Service (CAMH) in Norway shows that patients now receive an average of 11 therapy sessions (see Krogh & Bukten, 2011). However, we do not know the type or effectiveness of these interventions. In the UK context, although there are national guidelines (e.g., the National Institute for Health and Clinical Excellence (NICE) guidelines, 2005), use of psychological interventions as first line treatment and level of training and competence to use ESTs in clinics are being debated (see Hodes & Garralda, 2007; Murray & Cartwright-Hatton, 2006). Disseminating ESTs in community care settings is challenging (Weisz, Donenberg, Han, & Weiss, 1995). The conditions under which ESTs are developed and tested (efficacy trials) differ widely from the real life clinics. Thus the treatments, or the methodologies to test the treatments, do not often fit well within the clinical culture (Addis & Krasnow, 2000; Weisz & Gray, 2008). Only 5.6% of depression trials reviewed by Weisz, Doss, and Hawley (2005) reported conditions that are representative of usual clinical practice, namely: a) routinely referred patients, b) treatment provided by practicing clinicians, c) in a typical clinical care setting. Beyond methodological challenges, organizational barriers can impede this research. For example, implementing an EST means ensuring that clinicians get additional training and supervision, which results in lost productivity. Alternatively, administrators may mandate the training of ESTs, but practitioners may resist its use because it bears little resemblance to their current treatment skills. Conversely, practitioners may be interested in implementing ESTs but receive little support from administration. Given these challenges, testing dissemination with pilot studies that explore the feasibility of this work has been highly encouraged as a means to better prepare for large scale dissemination (Schoenwald & Hoagwood, 2001).
Aims of the study
Building upon the promising outcomes of ABFT and considering the challenges of dissemination, this study had three aims. First, we explored the feasibility of setting up a research evaluation program in a hospital based, public, outpatient, mental health clinic in Norway. Second, we selected regular staff therapists for training in ABFT. Third, we piloted a small randomized clinical trial to test the effectiveness of ABFT delivered by staff therapists. The pilot study had elements of an efficacy trial (e.g., narrow inclusion criteria, training, supervising, and credentialing therapists), and elements of an effectiveness trial (e.g., conducting the research in community clinics, getting referrals from the intake office, and training current hospital staff therapists). The target population was depressed adolescents between the ages of 13 and 17 years. For the pilot, the Hamilton Depression Rating Scale (HAM-D) (Hamilton, 1960; Williams, 1988) and the Beck Depression Inventory (BDI) (Beck, Steer, Ball, & Ranieri, 1996) were used to assess symptom reduction. The reliable change index (RCI) (Jacobson & Truax, 1991) was calculated to assess meaningfulness of clinical change. Treatment retention was used as a proxy for treatment acceptability to adolescents.
Method
Inclusion criteria
Clinic-referred adolescents (13–17 years) were included if they scored 14 points or more on the Hamilton Depression Rating Scale (HAM-D) and met diagnostic criteria for major depression on the Kiddie-Schedule for Affective Disorders and Schizophrenia (K-SADS-PL) (Kaufman et al., 1997). Although scores of 16 or 18 on the HAM-D are often used as study entry criteria, we lowered the threshold for this first study. This allowed us to take more patients and have more practical relevance for the clinic, assured we met our recruitment goals, and allowed us to test the model on a broader depressed population. Referred patients who were on anti-depressant medication were required to have been on the medication for eight weeks and still meet criteria for depression to be included in the study. At least one parent had to agree to participate either in the family treatment or in the assessments.
Exclusion criteria
Youth were excluded if they had a primary or comorbid disorder of bi-polar disorder, hypomania, mental retardation, eating disorder, schizophrenia, substance dependency, pervasive developmental disorder, significant medical/neurological disorders, or current sexual/physical abuse. These conditions were assessed by clinical interview and medical records review. Youth in need of hospitalization (e.g., acute suicidal behavior) were excluded and referred to appropriate services. Youth on probation, court referred, in short-term foster care, or pregnant were not recruited. There were no exclusion criteria for parents.
Procedures
Patients were recruited over an eight-month period between August 2008 and March 2009. Referrals were sent to the project research assistant (RA) from the participating clinic. If the youth scored above 16 on the BDI during a phone screen, the youth and family were invited to the clinic for the full assessment. At the pre-treatment assessment, the RA described the study in detail, obtained written consent, and administered the intake assessments. If the patient met criteria on the HAM-D and on the K-SADS for MDD, they were enrolled in the study. The BDI was administered bi-weekly. Only the HAM-D was administered at 12 week post-treatment assessment. Patients assigned to ABFT started therapy within two weeks of randomization. Patients assigned to Treatment as Usual (TAU) were immediately referred to central intake for scheduling with a clinic therapist. The RA informed the clinic directors of the treatment assignment. The project was approved by the Regional Ethics Committee (REK-III), Norway.
Treatment
Attachment Based Family Therapy (ABFT)
Five treatment tasks comprise ABFT. Task 1 (one session). The relational reframe sets the foundation for therapeutic work: Through reframing, there is a shift from viewing the adolescent as the problem to improving trust and communication between family members as the primary focus of the solution. Task II (2 to 3 sessions). During the alliance-building session with the adolescent, the therapist helps the adolescent identify what gets in the way of him/her talking to his/her parents when he/she is feeling depressed. The therapist aims to motivate and prepare the adolescent to talk with his/her parents about those barriers. Task III (2 to 3 sessions). Through the alliance-building session with the parent(s), the therapist helps parents build empathy for their child, partially through a reflection of their own experiences. This also encourages parents to reactivate their parenting instinct to love and protect. In addition, the therapist provides parent(s) with the skills necessary to improve effective, emotion-based communication with their adolescent. In Task IV (3 to 4 sessions), the reattachment task builds on the previous sessions where the therapist facilitates in vivo family conversations about past attachment ruptures, guiding the family members to be honest, share vulnerable emotions, use respectful speech, and active listening. These conversations create in-session, corrective attachment experiences, where parents provide and adolescents seek comfort and support from each other. In Task V (4 to 6 sessions), as attachment needs are being met more effectively, therapy focuses on promoting competency. By promoting competency, the therapist aims to strengthen parent–adolescent interpersonal problem-solving skills and help the adolescent to re-engage in age appropriate activities in and outside the home.
Treatment as usual
Staff therapists provided outpatient treatment in the host clinics. In general, treatment provided to youth in Norwegian outpatient clinics is individually focused (Israel, Thomsen, Langeveld, & Stormark, 2007). Four patients were assigned to staff psychologists, none of whom were family therapists, and started treatment within three weeks post-randomization. One adolescent in the TAU group was admitted to in-patient care one week after randomization. This adolescent received two weeks of in-patient care over the 12-week study period and seven outpatient sessions that included medication. However, the number of in-patient treatment sessions was not available and could not be included in this study. Assuming number of sessions as proxy for treatment dose, one adolescent (11%) received seven sessions, one adolescent (11%) received six sessions, and two youth (22 %) received one session.
Measures
Hamilton Depression Inventory (HAM-D)
The HAM-D 17 (Hamilton, 1960) was the primary outcome measure in this study. For research purposes, the HAM-D is currently the most widely used clinical measure of depression, with acceptable internal reliability (from .46 to .97) and test–retest reliability (from .81 to .98). The first author served as the gold standard and used video-recorded HAM-Ds of non-trial cases to train two clinical psychologists that were blind to treatment assignment. Inter-rater reliability for the total score (±2 points) was acceptable (k= .74). The first author conducted six baseline HAM-Ds (pre-randomization) but all post treatment HAM-Ds were administered by the two treatment blind-raters.
Beck Depression Inventory-II (BDI-II)
The BDI (Beck et al., 1996) is a widely-used, 21-item self-report instrument designed to assess the severity of depressive symptoms in adults and youth. The BDI has high internal reliability (α = .91) and high correlation with other measures of depression.
Kiddie-Schedule for Affective Disorders and Schizophrenia (K-SADS)
The K-SADS (Kaufman et al., 1997) is a semi-structured diagnostic interview for children ages six to 17 designed to assess current depressive episodes. The K-SADS was developed specifically for diagnosing child and adolescent depression in research protocols (Rutter, 1988) and remains the instrument of choice for this population. Short-term test–retest reliability of diagnosis ranges from kappa values of .24 to .70. In this study, the K-SADS (only the present state depression module) was administered at baseline by one of three ABFT therapists in the project. As with the HAM-D, the first author served as the standard and used video-recorded, non-trial cases to train the raters. The raters met regularly, reviewed the interviews and subsequent disagreement was resolved by consensus. Diagnosis of all youth in the trial was unanimous.
Youth self-report (YSR)
The YSR (Achenbach, 1991) was used to document co-occurring problems and syndromes. This widely used questionnaire comprises of three scales assessing the child’s competence (Activities, Social, and School), eight narrowband syndrome scales (Anxious/Depressed; Withdrawn/Depressed; Somatic Complaints; Social Problems; Thought Problems; Attention Problems; Rule-Breaking Behavior and Aggressive Behavior), and two broadband scales of Internalizing and Externalizing disorders in addition to a total problem scale. YSR was administered only at baseline.
Random assignment
In order to ensure balanced distribution between the two treatments, an independent statistician, not connected to the study, prepared a randomization table and treatment assignment that was sealed in envelopes and numbered. Youth were stratified on their age, gender and depression severity (HAM-D >25). After pre-treatment evaluation, the research assistant (RA) opened the appropriate envelope to designate treatment assignment.
Data analyses
Feasibility and acceptability of importing ABFT
Feasibility was evaluated by ongoing observation and documentation of the implementation process. Our focus was on setting up the outcomes evaluation system and on training therapists to do ABFT. Acceptability was evaluated by retention of adolescents in treatment. We used a non-parametric analysis (Mann–Whitney U test) to test for group difference between the number of sessions attended by adolescents in ABFT and the TAU group.
Outcome analysis
The primary dependent construct was depression, which was measured using self-report (BDI) and clinician report (HAM-D). Since the BDI was also administered bi-weekly during the treatment period, the latest BDI score was carried forward for the outcome analysis. Kolmogorov–Smirnov’s test showed normal distribution of the variables. However, due to the small sample size a non-parametric test (Mann–Whitney U test) was used. Post-treatment scores on HAM-D and BDI were the test variables and the treatment arm was the grouping variable. Further, effect sizes (Cohen’s d) were calculated using the means of the two groups and pooled standard deviation (d= M1-M2 / Spooled) and (Spooled = S1 + S2 / 2).
Results
Final participants
Twenty youth between ages 13–17 years (M = 15.6, SD = .99) and their families were included over a six-month period between August 2008 and March 2009 from three outpatient clinics in Norway. Over half (55 %) of the participants were girls (see figure 2). Only one adolescent was on antidepressant medication at the time of randomization, and had been for longer than eight weeks.

Percentage of completers and refusers (n= 20).
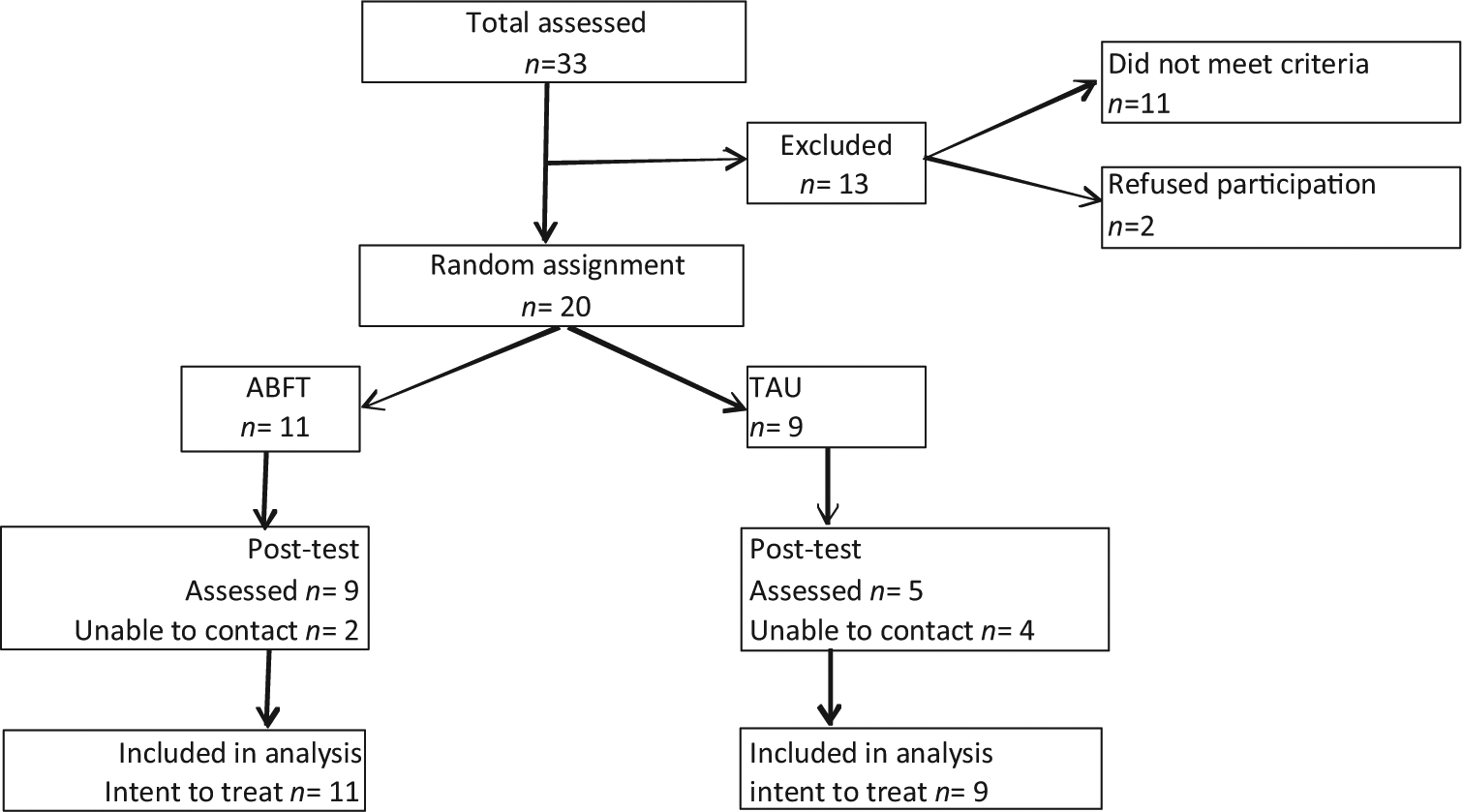
Participant flow through the study.
Baseline scores
At study start, subjects in ABFT (n=11) had a mean score of 31.9 (SD = 9.1) on BDI and 20.6 (SD = 4.6) on the HAM-D. Subjects in TAU (n=9) had a mean score of 29.7 on the BDI (SD = 11.2) and 19.7 (SD= 5.5) on the HAM-D. Four TAU cases received treatment (TAU-Tx) and five did not (TAU-wait list; TAU-WL). A comparison of these two sub-groups at baseline showed that TAU-Tx subjects had an average of 34.2 (SD = 14.2) on BDI and 22.7 (SD = 6.3) on HAM-D and TAU-WL subjects had an average of 26 (SD = 7.8) on BDI and 17.2 (SD = 3.6) on the HAM-D. There were no statistical differences between the two TAU sub-groups at baseline on the BDI (z = −.98, p= 0.32) or the HAM-D (z = −1.37, p= 0.17).
Clinical characteristics
The Youth Self Report (YSR) was used to obtain a glimpse of co-morbid clinical problems in the sample (table 1). As expected, 85% scored in the clinical level for internalizing disorders. Consistent with samples in other studies (e.g., Kessler et al., 2005), 55% scored in the clinical range for externalizing problems and 40% also reported attention problems. T-tests for continuous scores and chi-square test for dichotomous variables (clinical vs. non-clinical range) showed no significant differences between the treatment arms on these co-morbid variables.
T-scores of Youth self-report (YSR). Clinical cut-off for attention problems >70 and clinical cut-off for other broadband problems >64.

Feasibility of ABFT
Acceptability of ABFT to adolescents
Adolescents in the ABFT group attended significantly more therapy sessions (M= 8.3, SD = 2.2) than those in the TAU group (M= 3.2, SD = 3) (z = −2.43, p= .01). Of the youth randomized to TAU, one (11%) received seven sessions, one (11%) received six sessions, and two (22 %) received one session each. The patient that received seven sessions also received two weeks in-patient care and medication. At 12 weeks post randomization, five TAU youth (56 %) were still waiting to be assigned a staff therapist.
Institutional barriers
The study was originally planned by the first author in collaboration with two other senior clinical psychologists in the clinics, who also had advanced training in family therapy. The program took several years of planning with the hospital leaders and in seeking funding. The Department of Child and Adolescent Psychiatry at the Hospital had never participated in clinical trials research before, but support for this study was strong. The hospital offered to supply a 50% research assistant, office space, and the mandate to set up the referral and treatment structure. After a couple of submissions to secure financing, eventually a post-doctoral grant from the Norwegian Research Council was obtained to cover the first author’s salary plus incidental expenses.
Shortly into the study, senior leadership changed. The new leadership was less invested in the project and enthusiasm for the study decreased, as did the promise of additional resources. Many of the research functions (e.g., post treatment HAM-D) were conducted by volunteer staff from other clinics. More importantly, there was an inconsistent stream of referrals and assignment of TAU cases to clinic therapists. TAU families waited longer than planned to start treatment. At the post-treatment assessment, five patients were still on the waiting list for treatment as usual. This impacted data collection, as patients on long waiting lists were more likely to refuse post-assessments (see figure 1).
ABFT therapists and training
Therapists selection and characteristics
During the start up year, the two clinical (family) psychologists that were part of the original research team with the first author left the hospital for other employment. To replace them, the new hospital administrator selected and mandated two other therapists to participate in the study. One was enthusiastic about learning a family therapy model and the other skeptical. The average age of the three therapists providing ABFT was 41.7 years (SD = 10, range 31–52 years). Two were male. One therapist was a clinical psychologist with six years of clinical experience and identified eclectic approach as the primary orientation. The second therapist was an educational therapist who identified individual psychodynamic orientation as the primary orientation and had 10 years of clinical experience. The third therapist was a clinical psychologist who identified family therapy as his primary orientation and had 10 years of clinical experience. The two staff therapists carried a normal clinical caseload and scheduled the research cases on two weekdays when they had protected research time.
Therapist training
All three therapists attended a three-day didactic training seminar led by the treatment developer (the second author). Additionally, one therapist (the first author) spent a year in the United States with the developer of ABFT (the second author) and received extensive training. Once the trial began, the first author provided weekly supervision and, in turn, had bi-weekly phone supervision with the second author for the duration of the trial. Prior to treating study cases, all the three therapists treated two training cases each and then an ABFT trainer from the United States spent three days in Norway doing an advanced training that involved case reviews (verbal and tape review) and live supervision of the cases. Due to lack of funding, the American team was unable to review transcribed tapes. Therefore, based on live supervision of most sessions, the local supervisor (PI) informally used ABFT adherence measures to judge the fidelity of the therapist. In general it ranged from adequate to very good.
Therapist barriers
Therapists’ receptivity to ABFT varied by therapist. Two therapists were enthusiastic while one was skeptical about doing family work and training in ABFT. The latter was trained and experienced as an individual, dynamically-oriented child therapist and, although curious, had some difficulty learning to incorporate families into the treatment. The other therapist was eclectic in her approach and considered herself comfortable with family therapy, yet tended to do more individual therapy in her general caseload. Both therapists, other than the first author, carried a full caseload and thus missed the standards typically expected by the model in an efficacy trial (e.g., an additional session in a given week if needed, rescheduled missed appointments within the same week, monthly review of therapy tapes, etc.). Still, all three therapists had more training and ongoing supervision than was typical for the clinic.
Pilot outcome analysis
Symptom reduction
Pre-treatment and post-treatment scores for clinician-rated depression (HAM-D) and self-reported depression (BDI) is presented in Table 2. On the HAM-D (clinician rated depression), youth in ABFT demonstrated significantly greater improvement during treatment (12 weeks) than youth in TAU (z = -2.05, p= 0.04). At post-treatment there was an eight-point difference on BDI scores between the treatment groups, but it was not statistically significant (z = −1.02, p= 0.23) (see figure 3). To monitor if receiving treatment had an effect, we compared the two subgroups of TAU: those who received treatment (TAU-Tx) and those on the waitlist (TAU-WL). There was no statistical difference on TAU-Tx and TAU-WL on the BDI (z = −.49, p= 0.62) or the HAM-D (z = −.61, p= 0.53).
Pre-treatment and post-treatment scores with effect sizes (Cohen’s d).

ABFT: Attachment Based Family Therapy; TAU: Treatment As Usual; HAM-D: Hamilton Depression Rating Scale; BDI: Beck Depression Inventory.
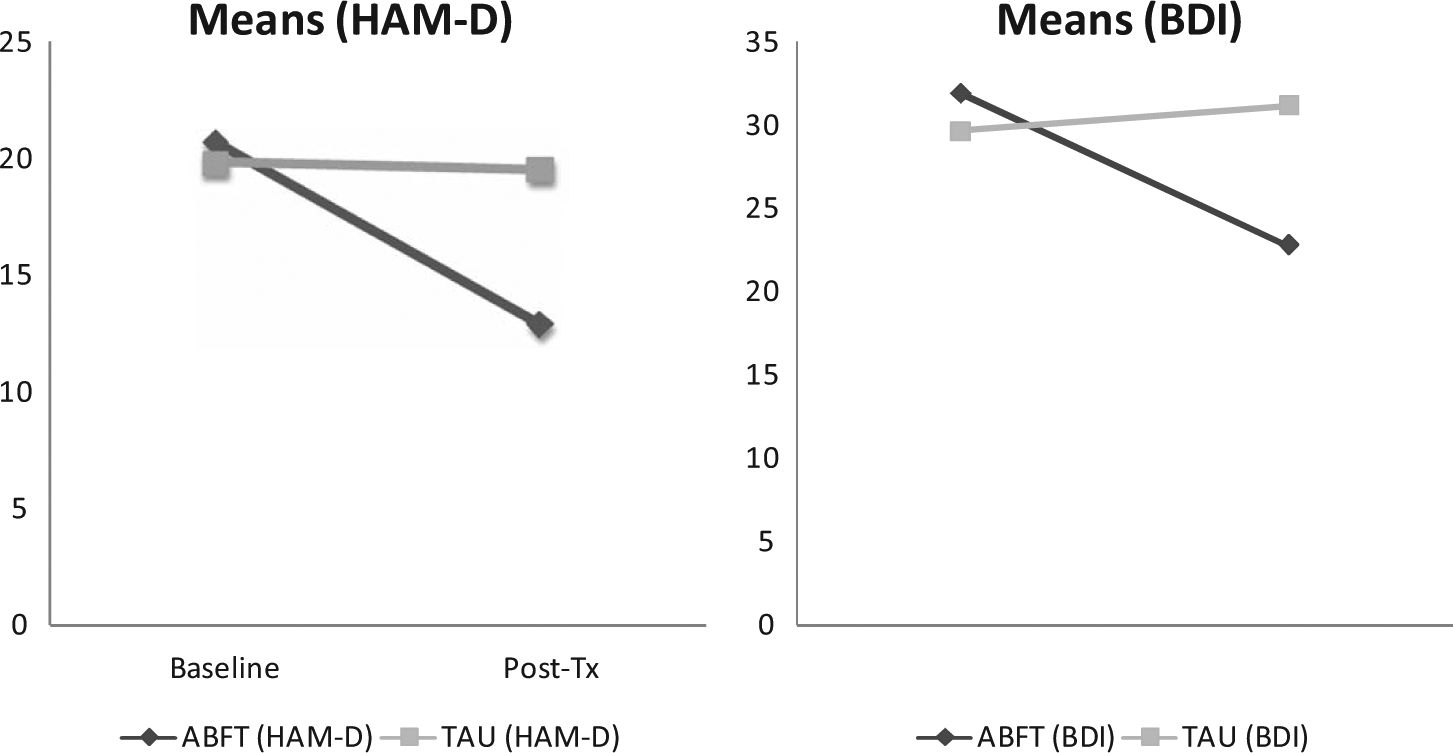
Mean scores of outcome measures at baseline and post assessment.
Significantly more youth in ABFT (55%) reported HAM-D scores below the cut-off for inclusion (14 points), compared with youth in TAU 11 % (χ2 [df1]= 4.1, p= 0.03). With a cut-off HAM-D score of less than nine as an estimate of clinical recovery, 27% of youth in ABFT reported recovery and 11% youth in TAU reported recovery. Although the average BDI scores for ABFT youth were moderately high (22 points), 3 ABFT youth (27 %) reported BDI scores below the cut-off (16 points). No youth from the TAU group were below the BDI cut-off post-treatment. This between-groups difference approached significance (χ2 [df1] = 2.88, p= 0.08).
Reliable Change Index
Seven of eleven youth (63 %) that received ABFT reported a reliable change index score (RCI) on HAM-D, compared with one of nine youth (11 %) in the TAU group (χ2 (df1) = 5.69, p= 0.02). Similarly, four of the eleven youth (36 %) in ABFT reported RCI on BDI scores, compared to TAU (χ2 (df1) = 4.09, p= 0.04).
Effect size
To see if a larger sample size might product more significant findings, we calculated effect size using between-group outcome scores. Scores on the HAM-D at 12-week assessments between the ABFT group (M = 12.5, SD = 7.3) and TAU group (M = 19.4, SD = 5.2) yielded an effect size of 1.08. Additionally, BDI scores of ABFT group (M = 22.82, SD = 12.02) and TAU group (M = 31.22, SD = 8.8) yielded an effect size of 0.8. Effects sizes above 0.8 are considered “large effect.”
Discussion
Like others, we found significant barriers to introducing a new, manualized treatment into a real world clinical setting (Fixsen, Naoom, Blase, Friedman, & Wallace, 2005). Despite several years of building decision-making coalitions with the hospital administration, enthusiasm for this study was not sustainable through leadership changes. Elements of successful recruitment and continuation of this evaluation study (e.g. using standardized screening tools, identifying and making referrals to the project, treating TAU cases) lost much of their administrative support. Without a strong institutional mandate that requires change in workflow procedures, these kinds of program evaluation structures cannot be sustained (Rosenheck, 2001). Though some of these procedures are unique to a research study, others have become standard components of dissemination contracts in development and training of empirically supported treatments. Increased training and supervision, collection of outcome data, smaller caseloads, and targeted populations, are all common characteristics when importing ESTs. These system changes require a re-evaluation of the structure and cost of service delivery. The data suggest that the increased quality of care can lead to lower services use and thus cost saving to the system (see La Greca, Silverman & Lochman, 2009), however more studies are needed to confirm these conclusions.
Feasibility of ABFT, based on therapist receptivity to treatment, was mixed. Therapists were mandated by leadership, rather than volunteered to adopt the ABFT treatment model. Receptivity to a new, brief, family-based model, and measuring outcomes, was met with mixed enthusiasm. In the Treatment of Adolescent Depression Study (TADS) – a NIMH funded effectiveness study (NIMH, 2010) – therapists were screened and selected either for experience in the model or enthusiasm to learn. However in real world dissemination, this selectivity may be unrealistic. Would the training look different for motivated therapists who already have a similar skill-set compared to unmotivated therapists who may not want to change their practice philosophy and techniques? Future dissemination studies might focus on these and similar questions of protected time for training and supervision and selection of appropriate therapists.
The data show that families and adolescents were receptive. Retention rates for participants in ABFT were similar to Norwegian national rates of treatment dose for this population, (M= 9.7 sessions) (Israel et al., 2007) and similar to retention rates in a recent clinical trial for suicidal and depressed youth in the USA (Diamond et al., 2010). Interestingly, ABFT patients achieved this dose in 12 weeks, while clinical impressions, based on the first author’s 10 years of working in this agency, suggested that most cases achieve this dose over nine to 12 months. The clinical and cost implication of this extended or brief treatment course is worthy of more research. It is possible that the expectation of brief treatment is increasing retention and not the ABFT model itself. However, ABFT has very specific, built in procedures to engage the adolescent and the parents. Several studies suggest that a good parent–therapist alliance is predictive of treatment completion while the adolescent–therapist alliance predicts outcome (Hawley & Weisz, 2005; Shelef, Diamond, Diamond, & Liddle, 2005).
Results of the pilot randomized study are promising. Between the treatment the groups, differences were statistically significant on the HAM-D with an effect size of 1.08 at post-treatment. This is especially promising as interview data is usually the primary outcome (e.g., TADS) and considered more reliable for assessment of depression (Zimmerman, Pfohl, & Stangl, 1986). Additionally, 27% of participants who received ABFT showed recovery, according to analysis of the interview data. These findings show promise, as they are close to the recovery rate of 37% reported in the TADS study of patients using a highly trained and supervised therapist providing CBT plus medication (Kennard et al., 2006).
No significant difference was found between the groups at post-treatment on the self-reported depression on the BDI, though there was an effect size of 0.8. This large effect may indicate that a larger sample might produce more consistent results. However, we must be cautious about estimating effect sizes from such small samples and a weak control group of limited or no therapy (Kraemer, Mintz, Noda, Tinklenberg, & Yesavage, 2006). A comparison of clinically meaningful change yielded results that were more consistent on both measures: Patients in ABFT were significantly more likely to experience reliable change in depression than patients in TAU, on self-report and interview measure of depression. The findings of this study are promising, yet the limitations of this study must also be evaluated.
Limitations and future directions
The small sample size prohibits making conclusive statements about the treatment effectiveness. Still, strong effect sizes are promising and similar to other studies of ABFT (Diamond et al., 2010). Additionally, half of the control group did not receive active treatment and those that did receive treatment had a low dose. This questions whether ABFT or an adequate dose of treatment is producing the results. While this is always a threat to internal validity when using TAU as a comparisons treatment (Spirito, Stanton, Donaldson, & Boergers, 2002), this is often the first step in programmatic research. A larger trial with a stronger control group would strengthen our confidence in the positive results.
Adherence to the model was not formally conducted. The local supervisor (the first author) assessed adherence through clinical supervision, discussion with the developers of the model, and review of recorded and live therapy sessions using the ABFT adherence measure. This limitation of the study may reflect the realistic limitation of treatment dissemination in many real world settings. Provider agencies may not be able to afford the high cost of credentialing in an EST, often in the range of $30,000 a year for a small team of providers (Northey & Hodgson, 2008). Whether credentialing therapists is necessary for improving the quality of service delivery and outcome is an empirical question. Comparing different types of training, dose of training and supervision, and the most efficient methods for training trainers, should be the focus of future research.
The discrepancy in dose of treatment between the treatment arms complicates interpretation. Only the more severe TAU cases (reporting higher HAM-D and BDI) were assigned to a therapist, reflective of the clinic’s triage policy to more rapidly assign treatment to more severe patients. Over half of the comparison group was functionally a wait-list control. Between subgroup analysis showed that there was no difference in outcome between TAU-Tx and TAU-WL, yet it raises the question of whether these promising results can be attributed to ABFT or an adequate dose of therapy.
Complications in data collection also limit the strength of these findings. Although no formal data was collected, families that did not receive ABFT and did not complete post-assessment reported a general dissatisfaction with TAU clinic services. Many participants in the TAU condition refused to complete post-treatment assessments. Additionally, the study was under-funded, with only one full-time post doctoral researcher (the first author). Consequently, the entire research project was conducted in 14 months and included setting up the referral structures, training therapists, blind-raters, and the research assistant, and eight months for patient recruitment, treatment and follow up data. Better funding and a longer funding period would have provided a better context for conducting this feasibility study.
Conclusion
The movement towards dissemination of empirically supported treatments to real world clinical settings is highly encouraged by the research community and service consumers. This process involves a broader systems change approach that should involve input from administration, therapist, support staff, and consumers (Schoenwald & Hoagwood, 2001). The introduction of brief, structured treatment, regardless of the model, can set up challenges for clinical staff and administrators. However, buy-in from the broad range of stakeholders will increase the likelihood of the sustainability and financial feasibility of these changes (Bickman & Noser, 1999). This study provides initial support that we can train Norwegian therapists in ABFT and that it will improve retention and outcomes over usual care in the clinic. Given the prevalence and consequence of adolescent depression, the equivocal research findings about current individual treatment models from this population, and the important role families can play in buffering against depression, further exploration of ABFT is warranted.
Footnotes
Acknowledgements
We acknowledge the invaluable contribution of the adolescents that participated in the study, their parents and the department of the Child and Adolescent Psychiatry, Stavanger University Hospital (BUPA) who participated in this study. Ms. Gro Peck from Stavanger University Hospital and Dr. Magne Maehle, Regional Center for Child and Adolescent Mental Health, Bergen, provided encouragement and support in launching this work. We also appreciate the constructive comments of the anonymous reviewers.
Declaration of conflicting interests
The authors declare that they do not have any conflict of interest.
Funding
This research was supported by a post-doctoral grant from the Norwegian Research Council to the first author.