
Abstract
Background:
Adolescents with anorexia nervosa rarely present themselves as having a problem and are usually reliant on parents to recognise the problem and facilitate help-seeking. This study aimed to investigate parents’ experiences of recognising that their child had an eating problem and deciding to seek help.
Methods:
A qualitative study with interpretative phenomenological analysis applied to semi-structured interviews with eight parents of adolescents with a diagnosis of anorexia nervosa.
Results:
Parents commonly attributed early signs of anorexia nervosa to normal adolescent development and they expected weight loss to be short-lived. As parents’ suspicions grew, close monitoring exposing their child’s secretive attempts to lose weight and the use of internet searches aided parental recognition of the problem. They avoided using the term anorexia as it made the problem seem ‘real’. Following serial unsuccessful attempts to effect change, parental fear for their child’s life triggered a desire for professional help.
Conclusions:
Parents require early advice and support to confirm their suspicions that their child might have anorexia nervosa. Since parents commonly approach the internet for guidance, improving awareness of useful and accurate websites could reduce delays in help-seeking.
Keywords
Introduction
Subjectively, patients with anorexia nervosa often consider themselves overweight despite objectively having a significantly low Body Mass Index (BMI). Hence adolescents with anorexia nervosa rarely present themselves as having a problem, which puts the onus on adults to recognise the problem and facilitate help-seeking. Delays in help-seeking are important, since a longer duration of eating disorder illness has been related to a worse outcome (Fichter, Quadflieg, & Hedlund, 2006; Steinhausen, 2002; Treasure & Russell, 2011). As recognition and a decision to seek help are prerequisites for treatment and parents are often key to these processes, it is important to explore these areas from the parents’ perspective. A key theme that emerged from a previous qualitative study was delayed parental recognition of the eating disorder, about which parents subsequently felt guilty (Cottee-Lane, Pistrang, & Bryant-Waugh, 2004). We aimed to elicit and better understand reasons for slow parental recognition by investigating parents’ experiences of recognising a problem and the process of deciding to seek help.
Method
Overview
Semi-structured interviews were conducted with eight parents of 11–18-year-olds with anorexia nervosa. The interviews focussed on parents’ views and experiences of recognising that their child had an eating disorder and the process they went through in deciding to seek professional help. Interpretive phenomenological analysis (IPA) was used to guide both the data collection and analysis (Smith, Jarman, & Osborn, 1999). IPA is concerned with gaining insight into a person’s subjective account of their experiences, and is therefore useful for research seeking to explore participants’ experiences, understanding and views (Brocki & Wearden, 2006).
Participants
Parents who were the main caregivers of 11–18-year-olds referred to a specialist child and adolescent mental health service (CAMHS) in one area of the UK were eligible for inclusion if their child had met the Great Ormond Street (GOS) diagnostic checklist criteria (Appendix) for anorexia nervosa within the past 3 years (Bryant-Waugh & Kaminski, 1993). These criteria were chosen because they specify ‘weight loss or failure to gain weight’ without quantification, as opposed to the International Statistical Classification of Diseases and Related Health Problems, tenth revision (ICD-10) and Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV) criteria for anorexia nervosa where females who meet the essential psychopathology and significant self-starvation criteria, but lack either amenorrhea or weight loss below 85% expected are instead classified as either ‘eating disorders not otherwise specified’ or ‘atypical.’ In the UK, a substantial proportion of adolescents who present clinically for evaluation and treatment of eating disturbances do not meet the full ICD-10 or DSM-IV criteria for anorexia nervosa, and the GOS diagnostic checklist provides a useful solution since it is sufficiently flexible to capture real-world eating disorder referrals to CAMHS (Nicholls, Chater, & Lask, 2000). All children had a clinical diagnosis of anorexia nervosa. Parents were excluded from the study if they did not speak conversational English or if their child had a physical illness, autistic spectrum disorder, learning disability or other major mental illness that better explained their symptoms.
Ethical approval was obtained from the local Research Ethics Committee. As required by them, the initial approach to parents was made by the treating clinician who provided information packs to primary caregivers meeting the eligibility criteria. The lead researcher confirmed eligibility criteria with parents upon receipt of their opt-in reply slip.
At the end of the semi-structured interview, each participant completed a main caregiver self-report questionnaire with demographic and clinical details about themselves and their child. In total, eight parents (seven mothers and one father), all from different families took part. Their ages ranged from 30–59 years (one aged 30–39 years, four aged 40–49 years and three aged 50–59 years). All participants were White British or Irish, and all except one were in paid employment. Four lived with the child’s other biological parent, two with a step-parent and two alone. The index children were aged 11–18 years (four aged 11–14 years and four 16–18 years). Six had been referred to CAMHS by their general practitioner (GP), one by a psychologist and one by a paediatrician. Participants identified in hindsight that their child had eating difficulties ranging from 1–57 months before contact with specialist CAMHS (median = 7 months). At the time of the parental interview, the duration of contact with CAMHS ranged from 4–30 months (median = 13.5 months).
Interview
A semi-structured interview schedule that included open questions and prompts was developed for the study. This was used flexibly to ensure that participants had the opportunity to fully describe their own accounts (Smith, 1995). Broad topic areas were identified from a review of the existing literature, the authors’ clinical experience (with backgrounds in child and adolescent psychology and psychiatry) and discussion with other clinicians who work with families affected by eating disorders. Topic guides were divided into two main sections: 1) experience of recognising your child had a problem; and 2) decisions around help-seeking. Section 1 included prompts for observations, describing first concerns, how recognition arose, how understanding changed over time, expectations regarding severity, the meaning that parents attributed to their observations of their child, comparisons and contrasts with their child’s pre-morbid self and personal experiences. Section 2 included prompts for thoughts about concerns, actions following concerns, communications with the child and others (personal and professional), coping, information gathering, weighing up of factors before embarking on help-seeking, concerns about help-seeking and personal experiences. Interviews lasted approximately 1 h and were conducted by the lead researcher either at the participants’ home (n = 2) or at the CAMHS clinic (n = 6). All interviews were recorded and transcribed verbatim. Confidentiality was assured and identifying information was removed from transcripts.
Analysis
Given that this study aimed to explore parents’ views in detail, interview transcripts were analysed thematically in accordance with the principles of Interpretative Phenomenological Analysis (Smith & Osborn, 2003). This inductive form of analysis recognises that the personal preconceptions and individual reflections of a researcher lead to an ‘interpretative’ account of the data (Oldershaw, Richards, Simic, & Schmidt, 2008). Each transcript was analysed individually. Emerging theme titles were noted and themes were then clustered to produce a table of superordinate and subordinate themes along with sample quotes for each transcript. Themes from all eight individual tables were then clustered and integrated to produce a list of major and minor themes which attempted to capture the ‘insider perspective’ of the participants’ common experiences. This whole process was carried out in an iterative manner, with the researcher frequently referring back to the original transcripts to ensure that themes were grounded in the data (Offord, Turner, & Cooper, 2006). Coding interviews began whilst data collection was ongoing, and data saturation appeared to be achieved in that emergent themes were repeating with little new insight by the eighth interview.
In line with guidelines for good practice in qualitative research (Elliot, Fischer, & Rennie, 1999; Smith, 1996; Yardley, 2000), two types of ‘credibility check’ of the analyses were carried out. First, the lead researcher shared random pages of interview transcripts with fellow researchers and compared analyses. Second, an audit trail (Smith, 1996) was conducted to check that a coherent chain of evidence ran throughout the project. This involved ensuring that example quotes for the final set of themes could be traced back to their origins step-wise from original coding through to the final cluster of themes. The primary researcher used supervision with co-authors to track the development of ideas and maintain a ‘reflexive stance’ (Silverman, 2000). Reflexivity is the condition of taking account of the personality and presence of the researcher within the investigation (Ryan, 2005).
Results
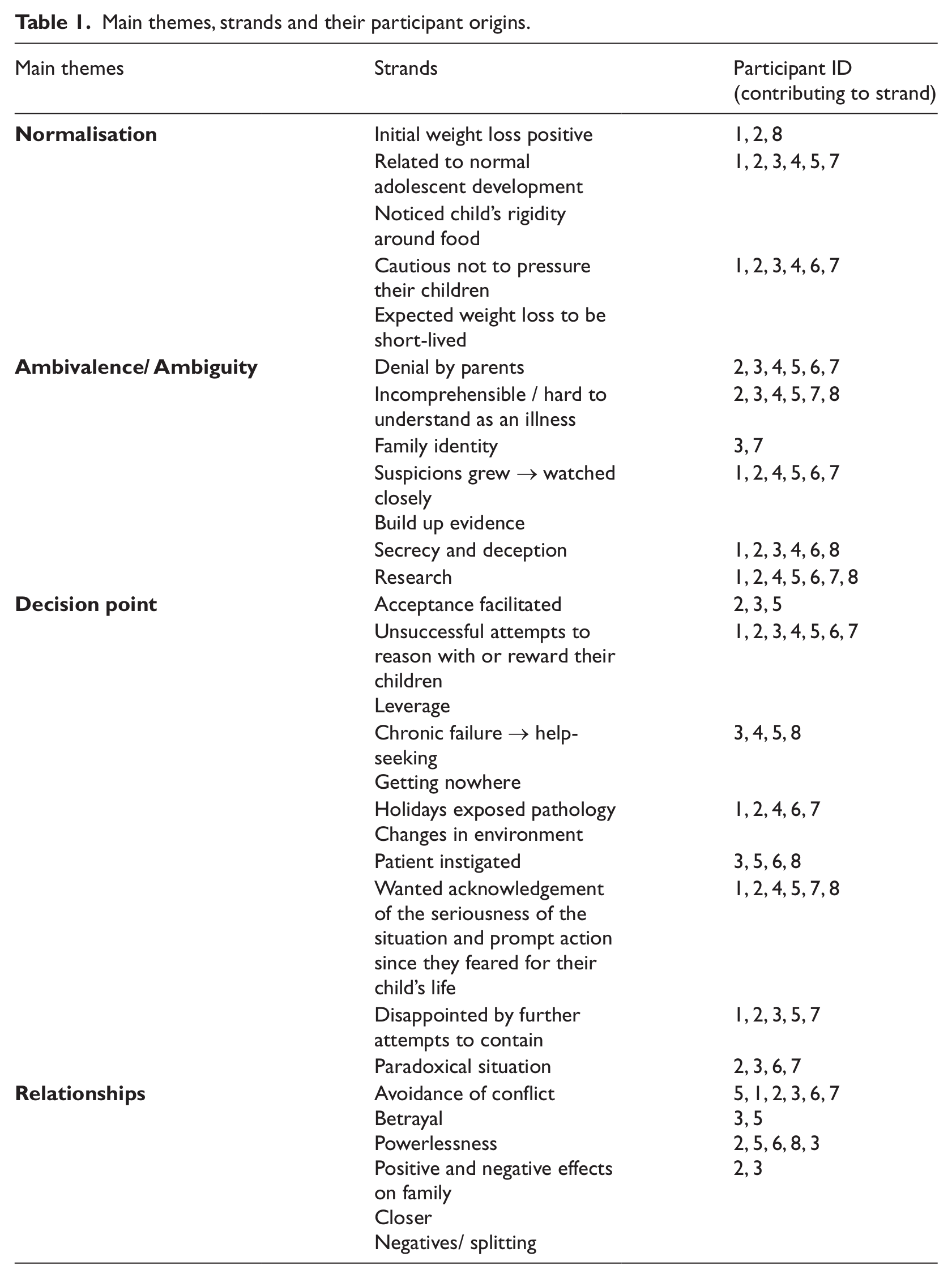
The analysis yielded four key themes, each with sub-strands (Table 1). These themes were
Main themes, strands and their participant origins.
Normalisation
Parents commonly viewed initial weight loss as positive or related to normal adolescent development.
RE: ‘BOY, AGE 16’; ‘MRS F’ I thought it was quite good that he’d done all the sport, previously he had sat in and played on the ‘PlayStation’.
RE: ‘GIRL, AGE 17’; ‘MRS P’ I knew she was wanting to lose a bit of weight but I didn’t mind because x had been one of those children, […] she used to raid, raid the fridge, raid the larder.
RE: ‘GIRL, AGE 13’; ‘MR J’ You know if she wanted to get into exercising properly that I, I’m all for it.
RE: ‘GIRL, AGE 18’; ‘MRS K’ All the time I just attributed that [the observed changes] to growing up and being a teenager.
Parents’ concerns were often aroused through their child’s rigidity around food, with specific and intense self-imposed restrictions on types and quantities of food.
RE: ‘BOY, AGE 16’; ‘MRS F’ I did find it odd in the sense that he was so disciplined and so rigid with it at that age.
However, many were initially cautious not to pressure their children and they expected weight loss to be short-lived.
RE: ‘BOY, AGE 16’; ‘MRS F’ I did think to myself oh that’ll fizzle out, that’s a fad and in two or three months that’ll all be, that’ll all be gone.
RE: ‘BOY, AGE 16’; ‘MRS F’ And I didn’t want to put pressure on….[aware that x was going through social and developmental changes during adolescence].
RE: ‘GIRL, AGE 17’; ‘MRS C’ I just thought it was a, a fad diet…I thought she’d just lose a couple of pounds, half a stone and then stop.
RE: ‘GIRL, AGE 14’; ‘MRS H’ I really didn’t think it was as serious as it was.
Ambivalence and ambiguity
Once parents recognised that their child had an eating problem, they avoided the term ‘anorexia’ since this made the problem seem “real” and “scary” and many parents described a process of denial:
RE: ‘GIRL, AGE 17’; ‘MRS C’ I didn’t want to put a name to it. If you put a name to it, it becomes real, it’s something you’ve gotta deal with and it was scary.
RE: ‘GIRL, AGE 17’; ‘MRS P’ Almost thinking that head in the sand almost sort of thing, that if I didn’t do anything it would get better of its own accord.
Parents found it hard to conceptualise their child’s difficulties as an illness and despite much thought, the cause of the eating disorder remained a mystery.
RE: ‘GIRL, AGE 17’; ‘MRS P’ To actually have anorexia is something none of us could ever comprehend, you know you’d never let it get that far.
RE: ‘GIRL, AGE 13’; ‘MR J’ I still see it as x kicking back…As a way of getting to you. You know she does it through the anorexia. But it’s like what brings that on and what, can’t see it as being a real illness and I still have an issue with that…Err I think I still put it down to a behavioural issue.
RE: ‘BOY, AGE 11’; ‘MRS R’ I couldn’t see any reason for it happening.
RE: ‘GIRL, AGE 12’; ‘MRS G’ The only thing that you can’t identify with her is where it came from, because all of the issues around err factors that start it, around low self-esteem, all of that, she doesn’t have any of that.
This incomprehensibility was compounded by the difference between their perception of their own family identity, and their perception of the ‘type’ of families that have children with anorexia nervosa:
RE: ‘BOY, AGE 11’; ‘MRS R’ The only person I know who had got somebody young who’d got an eating disorder, it was a thirteen year old but her mum was obsessed with being thin and being really glamorous and that and that just didn’t seem like our lifestyle. I couldn’t find, I was looking for reasons for it everywhere but I couldn’t find any.
As parents’ suspicions grew, they began to watch their children closely and attempted to build up sufficient evidence before raising the issue with partners or services:
RE: ‘BOY, AGE 16’; ‘MRS F’ I used to watch him like a hawk, I used to physically sit on the sofa and have to watch him.
RE: ‘GIRL, AGE 17’; ‘MRS C’ We was building up the evidence of what she was doing.
RE: ‘GIRL, AGE 18’; ‘MRS K’ It was like a little dance…Her job was to try to hide things from me and my job was to, to try and find out what was going on (laughs).
RE: ‘BOY, AGE 16’; ‘MRS F’ I knew things hadn’t been right for a while before I even said anything [to partner] because I wanted to be sure of what I was gonna say.
Parental scrutiny exposed widespread secrecy and deception amongst adolescents to conceal their efforts to lose weight:
RE: ‘GIRL, AGE 17’; ‘MRS C’ She would phone me up saying she was going on a bike ride with her friends and it all came out that it wasn’t a friend, she was just riding constantly around the block till I got home from work.
RE: ‘GIRL, AGE 12’; ‘MRS G’ She’d just mix around the bowl so it looked like she had a bowl of Ready brek but actually she’d eaten nothing because she mixed up the tiniest amount and smeared it all over the bowl.
RE: ‘BOY, AGE 16’; ‘MRS F’ Even at sitting at the table he was hiding food in trousers, in pockets.
Parents often searched the internet and found it useful to compare their child against symptom lists. Although they often considered their child’s case less serious than skeletal images that they found, this acted as an incentive to seek treatment to prevent escalation of their child’s difficulties.
RE: ‘GIRL, AGE 17’; ‘MRS C’ We knew what it was when we looked at the internet.
RE: ‘GIRL, AGE 12’; ‘MRS G’ I’ve been on that [internet] loads and so I went on that, read through all the symptoms, sat there and thought well this is, she is absolutely, you could just tick them off, yeah she does that, yeah she does that, yeah she does that, so it was just the whole list really you could identify.
RE: ‘GIRL, AGE 18’; ‘MRS K’ [Referring to skeletal images found on the internet] I had to make sure that she was getting some treatment to stop her getting to that point really.
However, parents also experienced reservations about seeking help on the basis of perceptions that anorexia nervosa had to be severe in order to warrant the input of services.
RE: ‘GIRL, AGE 17’; ‘MRS P’ Also it’s like where do you go to for help? … I think you know you’re probably like, you are anorexic or you’re not, until she’s really suffering with it then you don’t, there isn’t much, there’s no half-way house.
Further ambiguity was experienced by parents as feelings of guilt that they should have been able to make their child better themselves:
RE: ‘GIRL, AGE 14’; ‘MRS H’ Oh I felt terrible. I thought you know how have I let her get like this but you know it was really difficult (cries).
RE: ‘BOY, AGE 11’; ‘MRS R’ Cos I’m his Mum and I should make sure everything’s all right.
Decision point for help-seeking
Parents made serial unsuccessful attempts to reason with or reward their children in order to change their eating habits. The failure to effect change was often the trigger for parents to instigate professional help-seeking:
RE: ‘BOY, AGE 16’; ‘MRS F’ I decided to seek help from my GP when I realised that the discussions that I had with x about eating and trying to bribe him with extra tennis weren’t working.
RE: ‘GIRL, AGE 17’; ‘MRS C’ We tried to talk to her, we spoke to her in tears, we spoke to her sternly, we spoke to her softly, but nothing would get through to her.
RE: ‘GIRL, AGE 17’; ‘MRS P’ It gets to the point where…you know it’s not going away.
Changes in the environment such as holidays sometimes exposed pathology:
RE: ‘GIRL, AGE 12’; ‘MRS G’ We went to x in the summer for two weeks and… That was sort of the first time when I had any sort of significant concerns really….because of course she was with us all the time so I knew what she was eating.
Often adolescents instigated help-seeking themselves, although there were also examples of their denial and resistance:
RE: ‘GIRL, AGE 13’; ‘MR J’ One day she came home from school and said “oh, I’ve made an appointment with the School nurse”.
RE: ‘GIRL, AGE 18’; ‘MRS K’ She agreed that she would like some help.
RE: ‘GIRL, AGE 17’; ‘MRS P’ She wouldn’t admit to it when I said to her that day “you’ve got a problem”. She said she doesn’t have a problem….I asked her to go to the doctors herself and she wouldn’t go.
RE: ‘GIRL, AGE 14’; ‘MRS H’ And she just sat there [at GPs] and wouldn’t say anything.
Where parents took the lead in initiating help-seeking, they commented on how their acceptance that their child had major difficulties facilitated them to seek help:
RE: ‘GIRL, AGE 17’; ‘MRS C’ Till I put the name to it, I wasn’t strong enough to fight.
At this point, parents wanted acknowledgement of the seriousness of the situation and prompt action since they feared for their child’s life:
RE: ‘GIRL, AGE 17’; ‘MRS C’ I even told x, I said “look I can either buy you Christmas presents or the money I’m gonna use buy you a white coffin” trying to drill it home what she’s doing is killing herself.
Parents often experienced disappointment at further attempts to contain the situation by primary healthcare professionals such as GPs:
RE: ‘GIRL, AGE 17’; ‘MRS C’ I felt like the professionals was like “don’t worry, she’ll get over it” and my heart’s breaking thinking I need help fast, I’m seeing my daughter die.
RE: ‘GIRL, AGE 17’; ‘MRS P’ He said “well come back in three weeks and we’ll weigh you again.” Well at that point she only weighed about six and a half stone anyway and I didn’t even think she would go, would last another three weeks at the rate she was going.
In addition, parents reported that both they and GPs often felt trapped in a paradoxical situation, feeling unable to act without the child admitting their difficulties.
RE: ‘GIRL, AGE 17’; ‘MRS C’ I kept telling her over and over, there’s only one person that can cure you, it’s not me, it’s you and her dad was telling her the same.
RE: ‘GIRL, AGE 14’; ‘MRS H’ Quoting GP; “well it does sound like there’s a problem but there’s very little I can do if she won’t admit there’s a problem”.
Parents described the need to be assertive to persuade the GP of the need for help:
RE: ‘BOY, AGE 11’; ‘MRS R’ I said to him “I’m going to take his clothes off and I want you to look at him” and he says “well there’s no need for that”, and I said “well I’m sorry but there’s every need for it” and I just started sobbing and I was really shaking.
In hindsight, most parents expressed a wish that they had sought help sooner and said they would advise others in the same position to do so:
RE: ‘GIRL, AGE 18’; ‘MRS K’ You have to go with your instincts, I wished I’d done it sooner. I should have known, I should have followed my instincts but I waited until I was 99% sure that there was a problem before I acted and I should have, I should have talked to her sooner.
RE: ‘GIRL, AGE 14’; ‘MRS H’ I just think if I’d have probably done something sooner she wouldn’t have got, it wouldn’t have been so severe.
Relationships
Relational aspects were a dominant theme that ran throughout the parents’ accounts. There was considerable avoidance of conflict and a fear of betrayal by approaching services:
RE: ‘GIRL, AGE 17’; ‘MRS C’ You’re forever walking on eggshells, you don’t know which mood to pamper to next.
RE: ‘GIRL, AGE 17’; ‘MRS P’ I wouldn’t rock the boat in a way…but it was a case of if x is not happy then none of us are happy. So in a way I tried to make x happy.
RE: ‘GIRL, AGE 18’; ‘MRS K’ I didn’t want to do anything that would breach her trust.
Parents experienced feelings of powerlessness with respect to managing their child’s eating difficulties:
RE: ‘GIRL, AGE 18’; ‘MRS K’ If a child’s ill or has got an injury, say they’ve got a tonsillitis or a broken limb….You do something about it straightaway but it’s not like that.
RE: ‘GIRL, AGE 14’; ‘MRS H’ I felt sort of a bit helpless really.
Parents described contrasting experiences of the eating disorder acting to either bring the family closer together or pull them apart:
RE: ‘GIRL, AGE 17’; ‘MRS C’ Me and her Dad was constantly crying, it made us tighter and stronger together.
RE: ‘GIRL, AGE 17’; ‘MRS P’ A lot closer. A lot more honest with each other, the three of us.
RE: ‘GIRL, AGE 13’; ‘MR J’ There’s been a split in the house…me and [partner’s name] now post-it [the eating disorder] have not got a relationship.
Many parents felt frustrated and isolated by negative and simplistic appraisals of their situation and the solutions suggested by other people:
RE: ‘GIRL, AGE 17’; ‘MRS P’ Everybody seemed to think it was, the easiest solution was to sit her down with a meal.
RE: ‘GIRL, AGE 12’; ‘MRS G’ Inside you’d feel rubbish cos you think well they just think we’re rubbish parents. You must think that we’re not able to do our job properly. If you really think it’s just about giving (laughs) her a meal then your view of us as parents is very low really.
Parents also perceived stigma and that their friends were embarrassed to talk about their child’s difficulties:
RE: ‘GIRL, AGE 17’; ‘MRS P’ You know people don’t seem to have much sympathy because they see it as a self-inflicted thing.
RE: ‘BOY, AGE 11’; ‘MRS R’ I don’t know why but something like anorexia it’s like nobody wants to know you, you know it’s like you’ve got leprosy or something like that.
Discussion
This study explored the experiences of eight different parents of adolescents with anorexia nervosa, focussing on the process of recognition and decisions to seek help. We focussed on these areas in depth in order to illuminate and better understand previous research findings of slow parental recognition of anorexia nervosa in their children (Cottee-Lane et al., 2004). We found that recognition and decisions about help-seeking were related to parents’ evolving understanding of their child’s difficulties. Relational aspects were experienced by parents as important throughout, both in recognising their child’s difficulties and in deciding to seek help. Our study adds insight into the stages parents go through before seeking help for their child with anorexia nervosa. It highlights that parental avoidance contributes to delayed help-seeking and the central importance of internet research to parental recognition. It also shows that parents want prompt action from their GP at first presentation since they have already delayed seeking help until they fear for their child’s life.
There appeared to be three main stages towards help-seeking. First, there was normalisation of early changes. Parents often appeared to underestimate the significance of early warning signs of anorexia nervosa. Their interpretations included viewing initial weight loss as positive, related to normal adolescent development and likely to be short-lived. They were also cautious not to put pressure on their child because of a perception of the teenage years as developmentally stressful. Second, there was a stage of ambivalence during which parents watched their child carefully and carried out research to help resolve their ambivalence. This stage was characterised by a ‘cat and mouse’ game in which parental suspicions grew by watching their child closely to build up evidence. This often uncovered secrecy and deception by the child, aimed at hiding their methods of weight loss. Internet research was central to parental recognition of illness. However, many parents felt unable to broach the subject with their partner or with professionals until they had gathered sufficient evidence. This may have reflected parents’ desperate hope that their child did not have anorexia nervosa as well as their difficulties in understanding, conceptualising, and coming to terms with the condition. All these factors may contribute to delays in clinical presentation (Nicholls, Lynn, & Viner, 2011). The third stage was the decision point for help-seeking. By this stage, there appeared to be a mismatch whereby the parent appeared to have accepted the presence of a problem but the GP often needed to pass through the same stages as the parent already had (albeit faster) before taking action. The GP often appeared to ‘normalise’ and then contain parental anxiety, reflecting possible ambiguity about severity before accepting that the problem was severe enough to warrant clinical referral. However, these observations reflect eight parents whose children were recruited from specialist CAMHS. It might be that these approaches are effective for most presentations that GPs successfully manage without specialist input.
The process of help-seeking by the parents reflected a cycle of avoidance, underpinned by families’ conceptions of mental health problems and available health services (Biddle, Donovan, Sharp, & Gunnell, 2007; Sayal et al., 2010). Many parents described unpleasant and negative experiences of conflict avoidance, fear of betraying their child, powerlessness, isolation, patronising appraisals by important others and perceived stigma (Sayal et al., 2010). The experiences described by our participants also confirm findings from previous qualitative work with parents of children with anorexia nervosa (Cottee-Lane et al., 2004). First, the significance of initial changes in the child’s eating habits and behaviours were recognised slowly. Second, GPs were usually the first port of call and often delayed onward referral. From the parents’ perspectives, they and GPs often felt unable to act without the child admitting their difficulties. This raises a somewhat tautological position, given the inherent denial of being underweight within the psychopathology of anorexia nervosa. Similar to the paradoxical situation found in our study, previous work (Cottee-Lane et al., 2004) has used the term ‘You can lead a horse to water…’ to indicate how despite parents’ best efforts the patient themselves needed to take active steps towards recovery. Third, parents searched for reasons for the eating disorder but remained confused. This may be a more general finding relating to childhood emotional health problems. For example, parental difficulties in understanding or empathising with self-harming behaviour by their child have been described (Oldershaw et al., 2008). Other parallels with parents of children who had self-harmed include parental feelings of ‘loss of control and helplessness’ and ‘walking on eggshells.’
Methodological issues and future research
There are a number of strengths of this study. The sample was recruited from a CAMHS covering both city and rural areas. The diversity of accounts was increased by using parents at various stages of the treatment process and including the parents of two boys. In addition, the sample size was valid for meaningful interpretation since it has been argued that small participant numbers are particularly valued in interpretative phenomenological analysis to permit the fine-grained analysis required to identify subtle themes and meanings (Collins & Nicholson, 2002). The reliability of themes was strengthened by credibility checks. However, future research could aim to include other family members, the young person themselves and GPs in order to gain a wider perspective on the processes of recognition of anorexia nervosa and deciding to seek help. The focus on GPs’ perspectives may be particularly important, given that GPs appear to go through the same stages as parents in recognising a problem and deciding whether onward referral is warranted. Future research could also explore similarities and differences between parental experiences for anorexia nervosa and other emotional health disorders. Although beyond the scope of this study, parents also talked about their experiences of services after initiating help-seeking and commented that they needed help and support in their own right. Parents also described considerable relief upon help-seeking. However, given both its importance and parents’ willingness to share their experiences here, it represents a suitable area for future study.
As the study focussed on parents of young people referred to CAMHS, the opinions and experiences therefore reflect parents whose children were under the care of specialist services. As a study of real-world referrals to CAMHS, from a research perspective, it was not possible to check the clinical presentation against ICD-10 criteria although all children met the GOS criteria and had received a clinical diagnosis of anorexia nervosa. As the number of parents who declined to participate was not known and only one father took part, it is not clear how far the findings can be generalised to all parents whose children have anorexia nervosa. In addition, the index patients were at different stages of the recovery process and the initial time-lags before recognition and help-seeking were variable. Although our insights reflect the individual nature of each family’s experience, asking parents retrospectively about delays in recognition is subject to recall bias and has the propensity to induce distress and guilt. All participating parents were offered the opportunity to meet with a clinical member of the research team for a debriefing session(s) if they wanted this. Furthermore, given our study design, the utility of any quantitative information about delays in help-seeking would only be for contextualisation of the participants. The retrospective nature of the study means that parental perspectives about delays in help-seeking and clinical recognition can not be validated against clinical data. Furthermore, the constraints of research ethics approval meant that we did not have access to information about the child’s clinical characteristics such as weight, BMI, delayed growth and restrictive or purgative behaviour.
Conclusions
Our findings suggest that parents are able to spot the signs of anorexia nervosa at an early stage. However, they require advice and support to confirm their suspicions. Otherwise parents are left to accumulate concerns and often approach professional help at a late stage. It appears that parents attribute more potential symptoms of anorexia nervosa than is justified to the stresses of adolescence, and healthcare services need to be careful not to collude with this. It also means that other sources of recognition are important, such as schools and especially GPs, since they usually act as gate-keepers to treatment for anorexia nervosa and recovery from anorexia nervosa becomes much less likely the longer the illness has persisted (Von Holle et al., 2008). Secondary healthcare services may wish to target schools and GPs for training in early recognition and prompt referral for treatment so that they do not add to the duration of untreated eating disorder and a worse prognosis.
The availability of reliable sources of information might help parents to clarify early concerns. Furthermore, since parents commonly approach the internet for guidance, improving awareness of useful and accurate websites could reduce delays in help-seeking. Since parents appear to use internet search engines in an ad hoc manner to find information on anorexia nervosa, websites offering accurate information should consider adopting methods to ensure they appear high on search engines’ ‘hit-list.’
Since parents consistently reported that, in hindsight, they either wished that they had sought help sooner or would encourage others to seek help quickly, clinical guidelines aimed at reducing the duration of untreated eating disorder are likely to be acceptable to parents in terms of their motives. Once referred, the relational patterns including avoidance of conflict illuminated in the parent–child interaction, and the parental experiences of helplessness may offer useful foci for therapeutic intervention. Empowering parents again and helping them address avoidance of conflict should be an important part of the therapeutic work with families where an adolescent has anorexia nervosa.
Footnotes
Appendix
Great Ormond Street Diagnostic Checklist:
Acknowledgements
We wish to thank all the study participants, clinicians and transcriber for contributing to this study and the Nottinghamshire Healthcare NHS Trust CAMHS for supporting this study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: KS is partly funded by the NIHR Collaboration for Leadership in Applied Health Research and Care (CLAHRC) for Nottinghamshire, Derbyshire, Lincolnshire.