
Abstract
In this study we discuss implications of the dimensional versus categorical approach in the diagnosis of attention-deficit hyperactivity disorder (ADHD) and focus on the educational relevance of an early assessment. In a longitudinal study in a German community sample we investigated the development of ADHD symptoms from kindergarten until the end of Grade 1 as well as the association to pre-academic skills and later academic performance. At three time points in kindergarten, children (original sample N = 793; Mn age 4 years 10 months) were assessed in regard to school-relevant precursors of reading, spelling and mathematical abilities; ADHD symptoms were rated by parents and preschool teachers. In elementary school academic performance in reading, spelling, and mathematics was measured with standardized tests. Results show that stability of ADHD symptoms during preschool was high considering the dimensional approach, whereas in regard to the categorical classification many children crossing the cut-off point at one measurement point did not do so at the next assessment. Furthermore, preschool ADHD symptoms were negatively correlated with all school-relevant precursors. This was more pronounced for symptoms of inattention than for hyperactivity/impulsivity. Observing later development, preschool ADHD symptoms predicted academic achievement in mathematics and reading at the end of Grade 1 even after individual differences in nonverbal intelligence and specific precursors had been statistically controlled for.
There is no doubt that attention-deficit hyperactivity disorder (ADHD) belongs to the most common developmental childhood disorders worldwide, with a prevalence rate of about 5% (Polanczyk, de Lima, Horta, Biederman, & Rohde, 2007). The core symptoms of inattention, hyperactivity, and impulsivity are frequently persistent during adulthood and beyond, and often restrict a child’s ability to succeed in social and academic life (e.g. Barkley, Fischer, Edelbrock, & Smallish, 1990; Biederman, Petty, Evans, Small, & Faraone, 2010). Both the chronic nature of this complex disorder and its relationship to poor long-term school outcomes and academic achievement problems make ADHD a major public health issue.
Although ADHD has been intensely studied during recent decades, controversies regarding diagnosis and appropriate assessment still exist. One major point of discussion refers to the dimensional vs. categorical approach in the diagnosis of ADHD. In this paper, we want to elaborate on this topic in more detail by presenting results of an ongoing longitudinal study investigating the development of ADHD symptoms in the early years. We first present a short overview of this diagnostic issue in general, presenting advantages and disadvantages of both the categorical and dimensional approaches, including empirical findings. Next, we describe our own longitudinal study examining the stability of ADHD symptoms during preschool age as well as the concordance of parents’ and teachers’ reports, considering both diagnostic approaches. In order to explore children’s further development, the interrelation of preschool ADHD symptoms and academic achievement at elementary school was analyzed, taking into account the dimensional approach.
Diagnostic issues
The distinction between categorical versus continuous view of ADHD is one of the most intensively discussed conceptual issues in children’s psychopathology (Bell, 2011; Sonuga-Barke, Auerbach, Campbell, Daley, & Thompson, 2005). The categorical classification approach uses a critical threshold value to define ADHD membership: if a person shows some but not all of the critical symptoms, he or she falls outside the clinical range and will not be considered for treatment. Thus, this approach assumes that ADHD children can be separated from the normal range of behavior by a certain boundary. An alternative conceptualization favors a dimensional view. Here, ADHD is described as a trait on a continuum of increasing symptoms and severity, where children with ADHD are located at one extreme end of this dimension, differing from normality only by degree.
For educational practice this discussion is of utmost importance, considering the noticeable increase of stimulant prescriptions in children with ADHD already affecting preschoolers (Zito et al., 2000). Given that little is known about the impact of long-term stimulant usage on children’s health, especially in the case of an early treatment, a formal diagnosis of ADHD in preschool years should be made with caution. This is only one reason for the heated debate concerning the dimensional vs. categorical approach of diagnosis (cf. Haslam et al., 2006; Hudziak, Achenbach, Althoff, & Pine, 2007).
Given this conflict, it seems important to note that several empirical findings favor the continuum position (Levy, Hay, McStephan, Wood, & Waldman, 1997; Lubke, Hudziak, Derks, von Bijsterveldt, & Doomsma, 2009). For example, Haslam et al. (2006) investigated the issue whether the latent structure of ADHD is best understood as categorical or dimensional using two large samples of school-aged children and adolescents. Their results suggested that ADHD was best modeled as a continuum.
Further support for the dimensional approach was found by Loughran (2003) who investigated the stability of ADHD teacher rating scales at preschool level (Time 1) as well as in elementary school (Time 2). The number of children identified as potentially at risk for ADHD changed considerably over the 4-year interval of the study. According to Loughran, the high number of false-positive indications probably indicates that a considerable number of preschool children outgrew the symptoms which were present earlier in life.
In a large representative sample by Willoughby and colleagues (2012) the heterogeneity in the developmental course of children’s ADHD symptoms rated by parents was tested amongst others. The authors differentiated different groups of children and assessed them repeatedly between the ages of 3–5 years: There were children with persistently elevated levels of symptoms (8.4%), children with initially high ADHD symptoms that remitted over time (16.4%), a small group of children with initially low ADHD symptoms that had increased by the age of 5 (3.5%), and children characterized by persistently low ADHD symptoms (71.7%). The comparably large percentage of children belonging to the remitted group supports the assumption that some children outgrow their ADHD symptoms during preschool age.
One problem with the evaluation of the studies by Loughran (2003) and Willoughby et al. (2012) is that only one source of information, namely, parents’ or teachers’ reports, was applied. Given that ADHD symptoms must occur in more than one situation, that is, both at home and in school, as is demanded in the criteria of the international classification systems, both parents’ and teachers’ reports should be considered at the same time. Thus, it seems important to explore the characteristic features of ADHD symptoms during the preschool years assessed by both sources of information.
Our study tries to fill this gap in a large community-based sample investigating systematically the development of ADHD symptoms of preschool children rated by parents’ and teachers’ reports and thereby considering both the categorical and dimensional diagnostic approaches. We assume that high retest correlations of ADHD ratings can already be found during the preschool years, and that a categorical classification of ADHD symptoms is less stable. In addition, the long-term concordance between parents’ and teachers’ ratings of ADHD symptoms in children will be analyzed. It is supposed that concordance is low to moderate and does not change over time.
Educational relevance
A second major issue addressed on our study concerns the educational relevance of ADHD symptoms. More specifically, the research question raised in our study is whether early ADHD symptoms on the basis of the dimensional approach may serve as a predictor of later academic achievement. We do know from clinical studies using the categorical approach that children diagnosed with ADHD are often impaired in academic functioning (Massetti et al., 2008). Thus, children with ADHD suffer from learning difficulties more often than their classmates, showing higher rates of dyslexia or dyscalculia (Barbaresi, Katusic, Colligan, Weaver, & Jacobsen, 2007). Above all, children with ADHD already show mild impairment in different pre-academic skills before school entry (DuPaul, McGoey, Eckert, & Vanbrakle, 2001; Yochman, Ornoy, & Parush, 2006).
One problem of most studies cited above is that children with ADHD (as identified by the categorical approach) were investigated in comparison with their peers without ADHD. Thus, those children who showed a certain amount of ADHD symptoms but did not cross the threshold for receiving a clinical diagnosis were typically not further considered in such analyses. Accordingly, whereas research gives a comprehensive overview of the development of those children with a clinical diagnosis, we still lack knowledge concerning the future relevance of preschool ADHD symptoms assessed on the basis of the dimensional approach.
To our knowledge, the only study with preschool children based on the dimensional approach was conducted by Willcutt and colleagues (2007), who examined the association between ADHD symptoms rated by parents’ and the child’s pre-reading skills. The authors found that ADHD symptoms, in particular symptoms of inattention, were negatively and significantly correlated to the child’s school-relevant precursors such as phonological awareness or vocabulary.
Given that the evidence is still scarce, it seems worthwhile investigating the association of preschool ADHD symptoms rated by both parents and teachers with other pre-academic skills. In addition, it seems important to explore the question whether ADHD symptoms measured in preschool age based on the dimensional approach are also associated with academic impairment in school. Both research questions are addressed in the following analyses. We assume that ADHD symptoms rated by both parents and teachers are negatively correlated with various pre-academic skills, and that preschool ADHD symptoms may predict academic performance at the end of Grade 1.
Method
Study overview and participants
The study was embedded in a large-scale longitudinal study organized by the Ministry of Culture, Youth and Sports Baden-Wuerttemberg (project “Schulreifes Kind” – school-prepared child) starting about 18 months before children entered elementary school (cf. Hasselhorn et al., 2012). The 63 participating kindergartens were distributed in the South of Germany. Most kindergartens (75%) were located in urban areas. The sample originally consisted of 793 children with a mean age of about 4 years 10 months (SD = 4.4 months). Parents were fully informed about the study and recorded their accordance for their children participating in the study.
The first assessment (T1) took place in spring 2008. The second assessment (T2) was carried out 9 months later in September/October 2008, 1 year prior to school entry. Drop-out was due to the fact that some children moved away, and that other children missed assessments because of illness or holidays. The last measurement in kindergarten (T3) took place shortly before school enrolment in June 2009, about 9 months after T2 (N = 761). Children were again tested 1 year later at the end of Grade 1 (T4). Only 477 of the kindergarten children could be reassessed at school due to organizational and financial constraints of the research project. For instance, we lost several children who attended schools not included in the core sample of the project. Sex ratio was nearly balanced for all measurement points (about 51–53% males). The whole range of social occupation, assessed by the prestige of parents’ occupation (cf. Wegener, 1988) as an indicator of socioeconomic status (SES), was represented (M = 77.0; SD = 37.4; Range = 20–186). About 47.1% of the children had a migration background (in 19.5% of the cases, one parent was born outside Germany, and in 27.2% of the cases both parents were born outside of Germany).
An analysis of group differences between children staying with the study and drop-outs revealed no group differences regarding sex (χ2(1) = 1.46, p > .05), or immigrant background (χ2(1) = 0.83, p > .05). Further, groups did not differ regarding their ADHD symptoms in T3 for parents’ reports (F1,577 = 0.40, p > .05). However, children staying with the study turned out to be older than children in the drop-out group (F1,907 = 35.64, p < .001), came from families with lower SES (F1,768 = 5.41, p < .05), and had lower ADHD-scores based on teachers’ reports at T3 (F1,640 = 6.95, p < .01). ADHD symptoms were evaluated by preschool teachers and parents using ADHD rating scales during the kindergarten period (T1–T3). At T1, 95.0% of the preschool teachers and 84.6% of the parents completed the rating scales. The respective figures were 89.9% and 81.6% for T2, and 81.7% and 73.1% for T3. Complete questionnaire data from parents and teachers covering all three measurement points were available for 392 out of 907 children (43.2%).
School-relevant precursors of reading, spelling and mathematics were assessed in kindergarten. Kindergarten tests were provided in individual sessions. At the end of Grade 1, academic achievement was measured by standardized reading, spelling, and math tests. All school tests were applied in group settings.
Measures and variables
ADHD symptoms
In order to determine the presence of ADHD symptoms in kindergarten, the German short version of the Conners Scale was used for the first three measurement points. This 10-item questionnaire sums up ratings of ADHD-related behavior and has good internal consistency with Cronbach’s α = .88 for all three measurement points. The long version of the Conners Scale is widely used for measuring ADHD symptoms (Conners, Sitarenios, Parker, & Epstein, 1998a; 1998b) and shows high correlations with other scales assessing ADHD symptoms like the Child Behaviour Checklist (CBCL; Achenbach & Edelbrock, 1983) or the Strength and Difficulties Questionnaire (SDQ; Goodman, 1997).
In T2, the FBB-ADHS-V (Döpfner, Görtz, & Lehmkuhl, 2006) was additionally applied. Whereas the Conners Scale presents ADHD symptoms on one factor, the FBB-ADHS-V measure is subdivided into two subscales, namely, inattention and hyperactivity/impulsivity. This symptom checklist is part of a comprehensive diagnostic system for mental disorders in childhood and adolescence (DISYPS-II; Döpfner, Görtz-Dorten, & Lehmkuhl, 2008). The FBB-ADHS-V shows excellent internal consistency (Cronbach’s α = .93).
Parents as well as preschool teachers used both scales (Conners Scale and FBB-ADHS-V) to indicate the severity of specific symptoms on each item. Ratings were based on a 4-point Likert scale ranging from 0 for not at all true to 3 for very much true. In accord with the categorical classification approach, cut-off points were used which indicate a risk of ADHD. The critical threshold for the Conners Scale was located at 15 points with a maximum of 30 points (Steinhausen, 1995). For the 19-item FBB-ADHS-V measure, thresholds were determined on the basis of a German norm group (Döpfner, et al. 2006; Döpfner et al., 2008).
School-relevant precursors (assessed in kindergarten)
School-relevant precursors of reading, spelling and mathematical abilities were repeatedly assessed during the kindergarten period.
We used the first 35 items of the vocabulary test by Kiese-Himmel (2005) as an indicator of language performance. In this task, children were shown pictures of objects (e.g. an umbrella) and persons behaving in some way or another (e.g. sleeping); these objects (noun scale) and actions (verb scale) had to be named by the children (maximum score = 35). Internal consistency of the total score (noun and verb scale) was good to adequate for all measurement points (Cronbach’s α = .79–.88).
Phonological awareness was assessed by a rhyme identification task at T1 (Jansen, Mannhaupt, Marx, & Skowronek, 2002), followed by a sound categorization task at T2 (Bradley & Bryant, 1985). In each case, a maximum of 10 points could be reached. A second rhyming test given at all three measurement points required children to find rhyming partners for five different words (maximum score = 10). Internal consistency for the total score of phonological awareness was scarcely adequate with Cronbach’s α ranging from .68 to .76 (cf. Niklas, 2011).
Quantity-number competencies (QNC) were measured by five different tasks based on the developmental model by Krajewski (e.g. Krajewski & Schneider, 2009) at all three measurement points in kindergarten. To find about basic numerical skills, we assessed children’s knowledge of the precise number word sequence forward and backward. Moreover, children were asked to name Arabic numbers from 1 to 10. In the quantity-number word-linked seriation task, children saw several beetles on a sheet that were arranged in a row with one beetle missing. Each beetle had spots on its back. The number of spots determined the position in the row (the first beetle had one spot, the second beetle had two spots, etc.). In three different experimental trials, children were presented with an incomplete sequence where one of the beetles was missing. The children’s task was to select the missing beetle out of a choice of five beetles and to insert it correctly in the row. In a further task children were required to match Arabic numbers to the corresponding quantities. Finally, number relationships were assessed using calculation tasks (cf. Krajewski, in press). In addition to these tasks, children were asked to guess quantities by showing them two sheets with a different quantity of points (8 and 12) for 3 s. In total, children could reach 30 points on the QNC measure. Internal consistency of the test was good for the first two measurement points (Cronbach’s α = .84–.85) and acceptable for the third measurement point (Cronbach’s α = .75). The slight decrease in internal consistency was probably due to ceiling effects (cf. Niklas, 2011).
The Columbia Mental Maturity Scale served as an indicator of nonverbal intelligence (Esser, 2002). This test requires children to select one odd item in a group of pictures, for example one spoon and four forks (maximum score = 57). Split-half reliability of the test is high, ranging between .92 and .96. Correlations with other intelligence tests in preschool years are high to moderate (Ettrich, 2000).
Academic achievement (elementary school)
Standardized tests were used in elementary school to assess academic performance in reading, spelling and mathematics.
Reading was measured by a silent reading task which required children to read a word in a given line and mark the corresponding picture out of four pictures. Children were instructed to work as quickly as possible on this task. They were given 5 min to complete the test. The maximum score of correct words was 140. The parallel-forms reliability for the first class is .87, the test–retest reliability from 14 weeks is .76 (WLLP-R; Schneider, Blanke, Faust, & Küspert, 2011).
To assess spelling performance, we used the German Spelling Test for first and second grades (DERET 1-2+; Stock & Schneider, 2008). Here, children were given a dictation test consisting of 29 words. The number of errors served as an indicator of spelling achievement. Internal consistency of the test varies between α = .89 and α = .92, parallel-forms reliability between .87 and .88 (Stock & Schneider, 2008).
Mathematical achievement was measured by the German Mathematics Test for Grade 1 (DEMAT 1+; Krajewski, Küspert, Schneider, & Visé, 2002). This test is based on a math curriculum representative of all German states and consists of various tasks measuring amongst others quantity-number competencies and basic arithmetic competencies such as addition, subtraction, and the identification of inequalities. Internal consistency of the total test for the first class is good with Cronbach’s α = .89 (Krajewski et al., 2002).
Results
Analytic strategy
Given that only data of the Conners Scale were available for all three measurement points in kindergarten, this scale was used to analyze stability of ADHD symptoms over time, as well as the concordance between parents’ and teachers’ reports. To analyze the stability of ADHD symptoms during kindergarten based on the dimensional approach, intercorrelations between two adjacent measurement points were calculated separately for parents’ and teachers’ reports. To assess categorical stability, contingency tables were used calculating φ-coefficients. Here, like in most epidemiological studies, all those children exceeding the threshold level of the rating scale were classified as children at risk for ADHD on the basis of the categorical approach. Concordance between parents’ and teachers’ reports over all three measurement points in kindergarten was measured by correlations and φ-coefficients, respectively.
The association between severity of ADHD symptoms and pre-academic skills was assessed by calculating correlations between ADHD reports and performance in language, phonological awareness and QNC as well as nonverbal intelligence. Information on ADHD symptoms based on the Conners Scale was available for all three measurement points. At T2, correlations were also calculated for the “inattention” and “hyperactivity/impulsivity” subscales of the FBB-ADHS-V. Differences in these correlations (pre-academic skills and “inattention” vs. “hyperactivity/impulsivity”) were analyzed using z-values by Olkin (1967; cf. Bortz, 2005).
To predict academic achievement at the end of Grade 1, separate hierarchical regressions were computed for each dependent variable (i.e. reading, spelling and mathematics). Nonverbal intelligence was included in the first block, followed by the corresponding precursors for each criterion variable (phonological awareness, language, mathematical precursors) in the second block. ADHD symptoms collected in T1 and T2 served as predictor variables in the third block. With regard to the assessment of ADHD symptoms in T1, only data of the Conners Scale were used, whereas information for the subscales “inattention” and “hyperactivity/impulsivity” of the FBB-ADHS-V was additionally available in T2. Given that correlations between the Conners Scale and the FBB-ADHS-V were high, ranging between r = .69 and r = .80, we only used the subscales of the FBB-ADHS-V in T2 as an indicator of ADHD symptoms.
In the regression analyses, we handled missing data for ADHD reports by using multiple imputations. We report results for imputed data. The statistical software used was SPSS 18.
Stability of ADHD symptoms and concordance of parents’ and teachers’ reports
Table 1 shows intercorrelations between parents’ and preschool teachers’ reports on the Conners Scale for all three measurement points. As a main result, we found high stabilities in ADHD symptoms with regard to the dimensional analyses for the whole period of time, with intercorrelations between two adjacent measurement points ranging between rtt= .60 and rtt= .69, for parents’ and teachers’ reports.
Correlations between parents’ and preschool teachers’ reports on the Conners Scale for T1 to T3.

p < .01.
Regarding the categorical approach, we found only low to moderate stability over time. The stability obtained for parents’ reports from T1 to T2 was φ = .34, compared with a score of φ = .22 for teachers’ reports. The respective stability coefficients from T1 to T3 yielded scores of φ = .36 and φ = 33, and those from T2 to T3 of φ = .46 and φ = .36. Children who were identified as children at risk at one measurement point did not necessarily cross the threshold at the next assessment. On the other hand, children who were not categorized as children at risk for ADHD at one measurement point often crossed the cut-off point at the next assessment.
An analysis of the concordance between parents’ and teachers’ reports across time showed that correlations were low to moderate for all three measurement points, ranging from r = .26 to r = .31, when the dimensional approach was taken (see also Table 1). When categorizing children at risk for ADHD, concordance (К) between parents’ and preschool teachers’ reports were even somewhat lower, ranging between К = .13 to К = .16. Only seven children were classified as at risk for ADHD at T1, and another six children at risk were found at T2 and T3, respectively, when data from both informant sources (i.e. parents and teachers) were simultaneously considered.
Related to this, another result seemed also remarkable: Contrary to the assumption of trans-sectoral and persistent occurrence of ADHD symptoms, only one single child out of the total sample crossed the cut-off point more than once when both ratings, that is, parents’ and teachers’ reports, were simultaneously considered. This analysis was based on 392 children with complete questionnaire data (parents’ and teachers’ reports for all three measurement points in kindergarten).
Association of ADHD symptoms with pre-academic and academic skills
In the upper part of Table 2, correlations between ADHD symptoms based on parents’ and teachers’ ratings on the Conners Scale and school-relevant precursors of reading, spelling, mathematics, and nonverbal intelligence are given for measurement points T1 to T3. Correlations between ratings and pre-academic skills were all negative and significant for all teachers’ reports and for most of the parents’ reports. The only exceptions concerned the correlations between ADHD symptoms based on parents’ reports, and those between intelligence at T1 and phonological awareness at T3, respectively.
Correlations between ADHD symptoms based on parents’ and teachers’ reports and precursors of reading, spelling and mathematics as well as nonverbal intelligence for T1 to T3 on the Conners Scale.
(a)
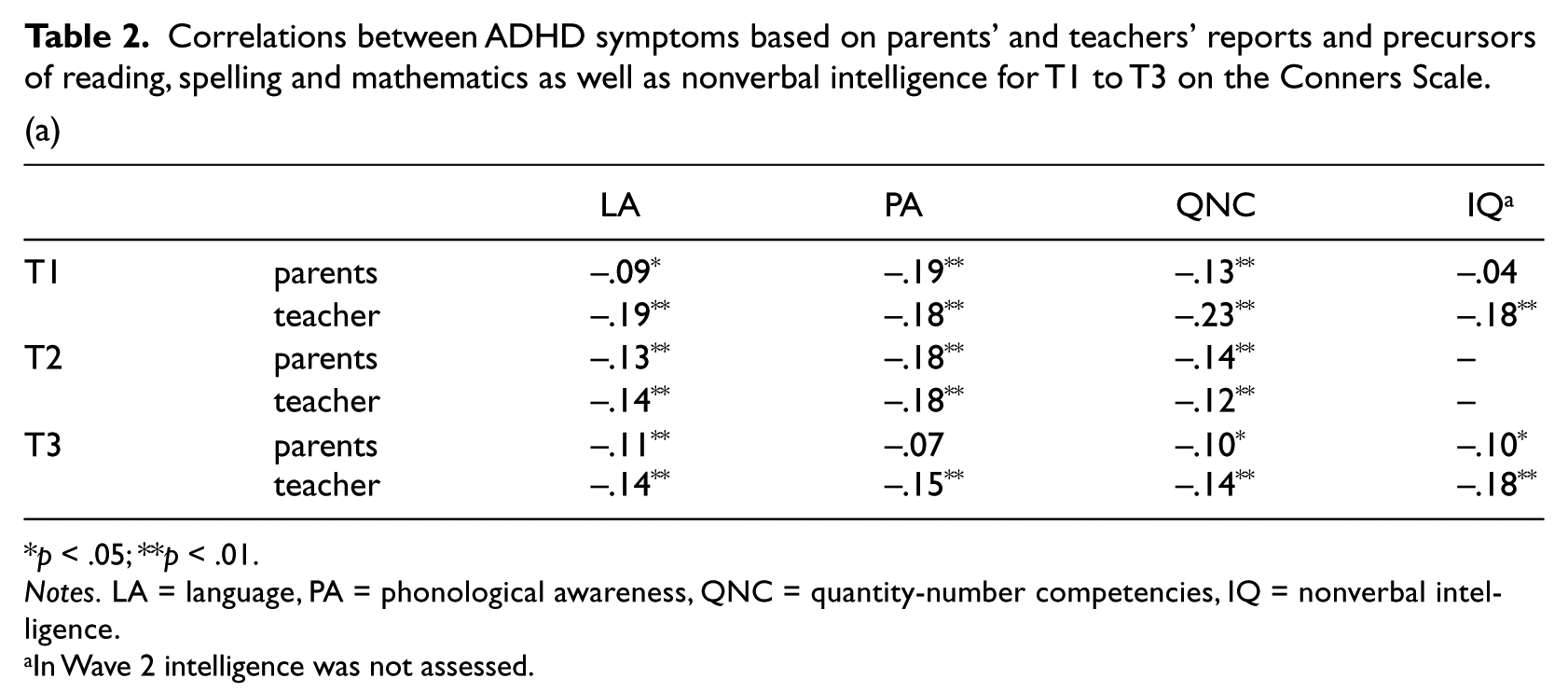
p < .05; **p < .01.
Notes. LA = language, PA = phonological awareness, QNC = quantity-number competencies, IQ = nonverbal intelligence.
In Wave 2 intelligence was not assessed.
(b)

p < .05; **p < .01.
Notes. LA = language, PA = phonological awareness, QNC = quantity-number competencies, IQ = nonverbal intelligence.
Given that in Wave 2 intelligence was not assessed, the performance of Wave 1 was used as an indicator of this variable.
The lower part of Table 2 shows intercorrelations among pre-academic skills and the subscales “inattention” and “hyperactivity/impulsivity” of the FBB-ADHS-V. Here again, all correlations were negative and significant. Overall, correlations were more pronounced for the subscale “inattention” than for “hyperactivity/impulsivity”; the inferential analyses (z-value by Olkin) were significant for all comparisons.
To further investigate subsequent development and the relevance of early ADHD symptoms on later academic achievement, hierarchical regressions were calculated. Results of the regression analyses predicting reading performance at the end of Grade 1 are presented in Table 3, using imputed data. Nonverbal intelligence assessed at T1 and phonological awareness assessed at T2 turned out to be significant predictors, as well as symptoms of inattention rated by parents 1 year before school entry. ADHD symptoms in form of inattention accounted for an additional 3.5% of the variance (p < .05). In total, 16.2% (corr. R2) of the differences in reading performance were explained by these predictor variables.
Hierarchical regression to predict reading performance at the end of Grade 1 by intelligence (IQ, assessed in T1) in block 1, phonological awareness (PA) and language (LA) in block 2 and ADHD symptoms in block 3 as independent measures.

Note. B = unstandardized regression coefficient, SE = standard error, T = t–statistics, p = significance.
As can be seen from Table 4, nonverbal intelligence was the only significant predictor of later spelling achievement. In total, 13.5% (corr. R2) of the differences in spelling performance at the end of Grade 1 could be explained by nonverbal intelligence. ADHD symptoms did not significantly account for additional variance (2.0%, p > .05).
Hierarchical regression to predict spelling performance at the end of Grade 1 by intelligence (IQ, assessed in T1) in block 1, phonological awareness (PA) and language (LA) in block 2 and ADHD symptoms in block 3 as independent measures.

Note. B = unstandardized regression coefficient, SE = standard error, T = t–statistics, p = significance.
ADHD symptoms of inattention rated by teachers played an important role in the prediction of mathematical performance at the end of Grade 1, even after intelligence and quantity-number competencies had been controlled for (see Table 5). ADHD symptoms explained an additional 2.6% of variance (p < .05). The total explanation of variance added up to 23.6% (corr. R2).
Hierarchical regression to predict performance in mathematics at the end of Grade 1 by intelligence (IQ, assessed in T1; block 1), quantity-number competencies (QNC; block 2) and ADHD symptoms (block 3) as independent measures.
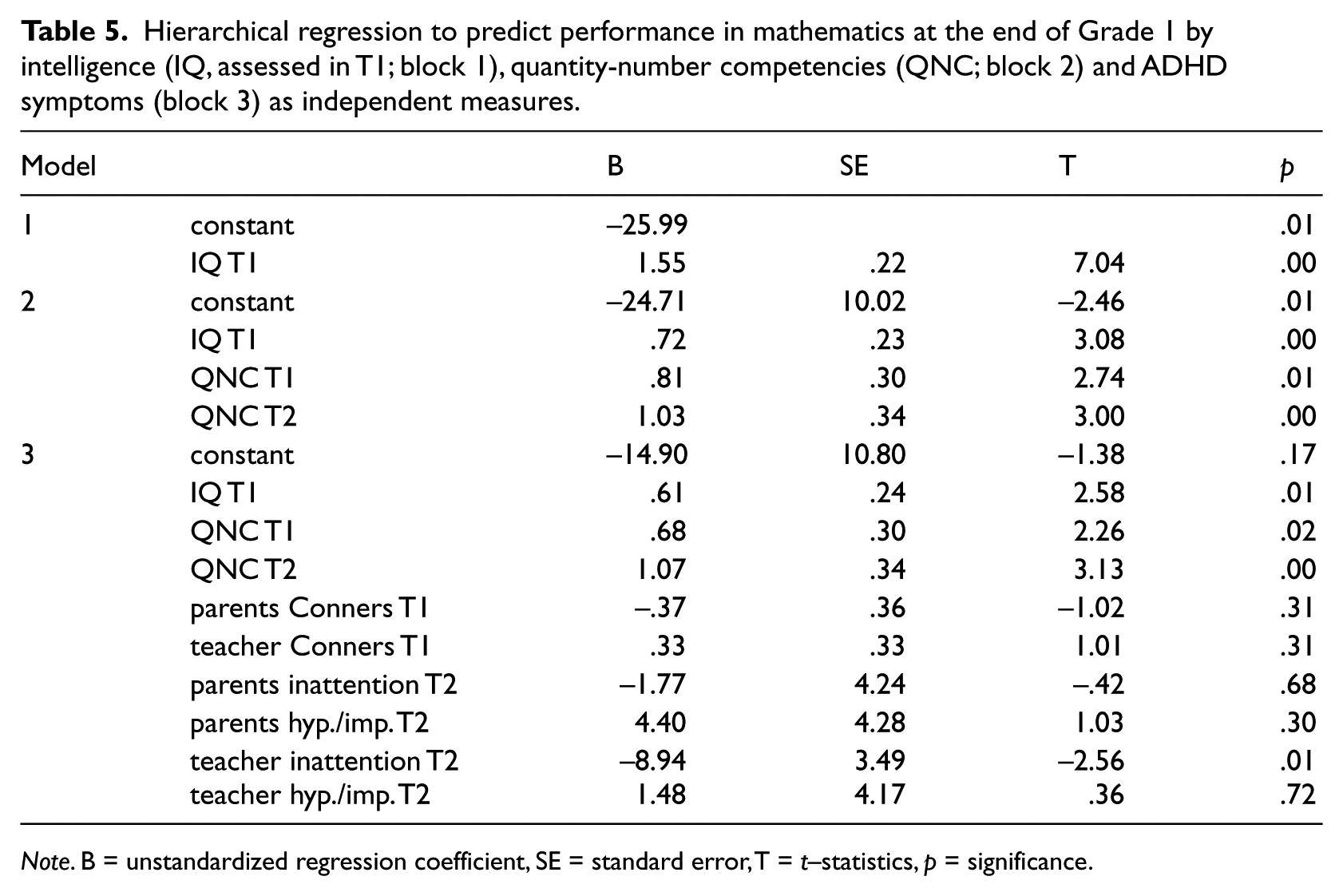
Note. B = unstandardized regression coefficient, SE = standard error, T = t–statistics, p = significance.
Discussion
One of the major goals of this research was to analyze the development of ADHD symptoms based on parents’ and teachers’ reports in a large community sample of preschool-aged children considering the dimensional and categorical diagnostic approaches. In this context, our first aim was to examine the stability of ADHD symptoms in preschool children. As a main result, high symptom stability rated by parents and preschool teachers was demonstrated, with correlations ranging from rtt= .60 to rtt= .69 between two adjacent measurement points. In contrast, only low to moderate stability over time was found when a categorical classification approach was used for indicating children at risk of ADHD, with φ = .34 to φ = .46 for parents’ and φ = .22 to φ = .36 for teachers’ reports, respectively.
On the one hand, this finding indicates an already high stability of ADHD symptoms during the preschool years. On the other hand, however, it also shows that children who passed a critical cut-off point at one particular measurement point did not necessarily do so at the next assessment. Accordingly, there seems to be considerable variation in the “problem zone” of ADHD in early developmental stages. According to further studies, among those preschoolers showing ADHD symptoms in preschool years some seem to outgrow ADHD-related behavior during childhood, presumably as a result of delayed but normal development (cf. Campbell, 1986; Loughran, 2003; Willoughby et al., 2012). One could argue that this finding could also indicate lacking validity of the Conners Scale in that age group. However, the consistence with former studies does speak against this assumption (e.g. Loughran, 2003). Furthermore, correlations of ADHD symptoms as a dimension were high and similar to those reported in other studies investigating the stability of ADHD symptoms in preschool years (LeBlanc et al., 2008). In addition, high correlations between the Conners Scale and the total scale of the FBB-ADHS-V were demonstrated (r = .71 for parents’ reports and r = .80 for teachers’ reports). Thus, we can assume that the short form of the Conners Scale is valid.
Another relevant aspect concerned the concordance of parents’ and teachers’ reports of ADHD symptoms in preschool children across three measurement points, as well as the trans-sectoral persistence of ADHD symptoms. Concordance between parents’ and teachers’ ratings was only low to moderate for all assessments, supporting former findings (e.g. Murray et al., 2007; Re & Cornoldi, 2009). Different interpretations for the low agreement between these sources have been generated. One hypothesis is that parents and teachers differ regarding expectations and tolerance limits concerning the child’s misbehavior. Consequently, they evaluate identical behavior differently. However, it is also possible that children with ADHD actually show different behavior at home and in school settings. Moreover, the interaction style between the adult and the child could cause cross-situational differences in the child’s behavior (cf. Achenbach, McConaughy, & Howell, 1987; Cai, Kaiser, & Hancock, 2004).
Our analyses of trans-sectoral stability and temporal persistence of ADHD symptoms showed that only one single child out of about 400 preschoolers was consistently identified as at risk for ADHD across measurement points. As to the diagnostic process, parents’ and teachers’ reports should always be considered at the same time. Studies investigating the relationship between different ADHD reports are important to further give advice how to combine different reports when concordance is low.
The second major aim of the present study was to examine the association of ADHD symptoms with pre-academic skills in preschool years as well as with later academic functioning. In contrast to other studies analyzing the development of children with ADHD, we did not establish cut-off points of ADHD-relevant behavior. Instead, we focused on ADHD symptoms as a dimension. We assumed that ADHD symptoms assessed in preschool years are negatively correlated with pre-academic skills and suited to additionally predict individual differences in later academic achievement.
We were able to confirm both assumptions. First, ADHD symptoms rated by both parents and preschool teachers were negatively associated with various school-relevant precursors in kindergarten. Overall, this pattern was more pronounced for symptoms of inattention than for hyperactivity/impulsivity. This is consistent with results from Willcutt and colleagues (2007) who reported negative correlations between parents’ ADHD ratings, particularly symptoms of inattention, and pre-reading composites. Our findings confirm these earlier results based on preschool teachers’ reports of ADHD symptoms, and generalize them to early quantity-number competencies. These results highlight the importance caregivers evaluating children’s behavior in terms of ADHD symptoms – with special focus on symptoms of inattention – already in kindergarten.
Furthermore, we found that parents’ and preschool teachers’ reports of ADHD-specific behavior assessed 1 year before children entered elementary school significantly and negatively predicted academic achievement at the end of Grade 1. Symptoms of inattention rated by parents significantly predicted later reading performance even after individual differences in nonverbal intelligence and specific precursors such as vocabulary and phonological awareness had been statistically controlled for. This was not true for later spelling achievement. Here, ADHD symptoms did not account for additional variance in the criterion variable. However, when the goal was to predict mathematical performance at the end of Grade 1, inattention rated by teachers was of the most importance, even when quantity-number competencies and intelligence were controlled for. Whereas former studies indicated that preschool children with a formal ADHD diagnosis based on the categorical approach do show poor cognitive skills in comparison with their peers (e.g. DuPaul et al., 2001; Yochman et al., 2006), our analyses in a community sample showed that studying ADHD symptoms on a dimensional scale give a more specific account of the relationship between ADHD symptoms and school achievement. We suggest that such an approach should be used in future research.
Although we believe that our study addressed theoretically and practically relevant issues related to ADHD, it certainly has several limitations. First of all, we only used the short form of the Conners Scale when analyzing the development of ADHD symptoms at T1 and T3; the broader FBB-ADHS-V measure was only applied at T2. Thus we did not assess the full range of DSM-IV symptoms during the whole preschool age. Moreover, the drop-out rate after school entry was rather high. Thus a certain sample bias cannot be excluded. Although comparisons of drop-outs and children staying with the study did not reveal significant differences in relevant characteristics such as sex, immigrant background, or, ADHD symptoms based on parents’reports at T3, children staying with the study turned out to be older, had lower ADHD-scores based on teachers’ reports at T3 and showed a lower SES than children in the drop-out group. This may be due to the fact that especially younger children and children scoring higher on ADHD-teacher ratings did not enter school regularly and were enrolled 1 year later. Further, it might be that parents with higher SES keep their children one year longer in kindergarten to give them more time for development. Thus, we are not able to generalize the findings to children with a delayed school entry.
Clinical implications
Our analysis yielded two major results. First, our findings indicate that ADHD symptoms, in particular symptoms of inattention, are negatively associated with cognitive skills in children already during preschool years. Thus, whenever such problems are observed in preschoolers, they should be treated systematically early in life. Consequently, educators should be alert with regard to children showing symptoms of inattention at preschool age. Second, an early diagnosis of ADHD on the basis of the categorical classification should be done with caution, given its considerable instability over time. Diagnostic thresholds are pragmatically necessary in clinical practice and cannot be ignored; however, instead of focusing only on these boundaries, greater consideration should be given as to whether the child shows social functional impairment as a result of ADHD symptoms. Furthermore, data from more than one source of information, for example reports from both teachers and parents, should always be considered in the diagnostic process.
Footnotes
Acknowledgements
We thank the Ministry of Culture, Youth, and Sports in Baden-Wuerttemberg for the support of this study as well as all involved investigators, the children, their parents, and teachers for their commitment. Especially we would like to thank our cooperation partners of the scientific advisory team of the project “school-prepared child” in Wuerzburg (Frank Niklas & Robin Segerer), Heidelberg (Eva Randhawa, Isabelle Keppler, Miriam Johnson & Hermann Schöler), and Frankfurt (Katja Krebs, Hanna Wagner, Jan-Henning Ehm & Marcus Hasselhorn). Without their input, planning, and realization of the study, this article could not have been written.
Funding
This study was financially supported by the Ministry of Culture, Youth, and Sports Baden-Wuerttemberg.