
Abstract
When children require mental health services, clinicians need to conduct assessments that are developmentally sensitive and that include the child’s point of view. Drawing is a popular tool that is commonly used in clinical settings. Research on drawing in experimental settings has confirmed that the opportunity to draw while talking increases the amount of verbal information that children report during an interview. The present research examined whether drawing also facilitates children’s self reports during a mental health assessment. A total of 33 5–12-year-old children were asked either to draw and tell about their presenting problem or to tell only. Children who drew and told provided twice as much verbal information as children who told only. Further, interviewers in the draw and tell condition used a greater number of minimal responses than did interviewers in the tell only condition. These data have important implications for clinical practice.
Prevalence rates indicate that between 10% and 25% of children and adolescents worldwide will be affected by mental health issues that negatively impact their development (Carr, 2000; Egger & Angold, 2006; WHO, 2003). Some mental health issues disrupt normative developmental trajectories and stop children from fulfilling their academic and personal potential (Bideman & Faraone, 2005; Ford, Goodman & Meltzer, & Meltzer, 2003; Graham, Turk, & Vehulst, 1999; National Scientific Council on the Developing Child, 2007; WHO, 2005). If left untreated, psychopathology during childhood and adolescence can have long-lasting detrimental effects (Althoff, Verhulst, Rettew, Hudziak, & van der Ende, 2010; Holmbeck, Greenley & Franks, 2004; Reef, van Meurs, Verhulst, & van der Ende, 2010; The Sainsbury Centre for Mental Health, 2009; WHO, 2003). In order to alleviate the long-term negative effects of psychopathology, engagement with specialty child mental health services is often required (Carr, 1999; National Scientific Council on the Developing Child, 2007; Royal College of Paediatrics and Child Health, 2003; WHO, 2003, 2005). To be effective, these services should be designed to meet the specific needs of the child (Day, 2008; Holmbeck et al., 2004; MoH, 1997; Salmon, 2006) and should be delivered in a developmentally appropriate way. Before effective treatment can be provided, the first step is to conduct a thorough assessment of the child’s difficulties (AACAP, 1997; Davies & Wright, 2008).
Contemporary practice guidelines recommend that child assessments are multi-modal (i.e. include a range of different tests and measures) and multi-informant (i.e. include interviews with the parent, child and teacher (Holmbeck et al., 2004; Mush & Hunsley, 2005; Rutter, 1997)). Central to this process is the child interview, which is conducted to obtain the child’s perspective of their difficulties (AACAP, 1997; Davies & Wright, 2008; Graham et al., 1999; Rushforth, 1999). Researchers and clinicians, for the most part, agree that it is beneficial to hear a child’s account of their symptoms and that children can provide reliable and valid clinical information (Edelbrock, Costello, Dulcan, Kalas, & Conover, 1985; Holmbeck, Li, Schurman, Friedman & Croakley, 2002; Ialongo, Edelson, & Kellam, 2001; Silverman & Ollendick, 2005; but see Boyle et al., 1993, and Holmbeck et al., 2008; Pelham, Fabiano, and Masetti, 2005 for contrary evidence). Further, a large body of research from developmental studies has established that even young children can recognise and report their experiences and emotions (Boland, Haden & Ornstein, 2003; Lamb & Fauchier, 2001; McGuigan & Salmon, 2004; Peterson, Sales, Reese, & Fivush, 2007; Pipe, Lamb, Orbach, & Esplin, 2004; Principe, Ornstein, Baker-Ward, & Gordon, 2000; Reese & Brown, 2000; Reese & Newcombe, 2007; Rudek & Haden, 2005; Salmon, McGuigan, & Pereira, 2006; Simcock & Hayne, 2003) but children’s self reports are typically brief (Gee & Pipe, 1995; Ornstein, Gordon, & Larus, 1992; Patterson & Pipe, 2009; Pipe & Salmon, 2009; Sutherland & Hayne, 2001), can require adult support (Nelson & Fivush, 2004; Pipe & Salmon, 2009; Pipe, Salmon, & Priestly, 2002) and are more accurate when children generate their responses in answer to open ended questions (Larsson & Lamb, 2008; Orbach, Hershkowitz, Lamb, Sternberg, Esplin, & Horowitz, 2000).
How, then, can clinicians help children to give full accounts of their symptoms and emotions during clinical assessments? Research in clinical contexts has identified a number of ways that clinicians can support children to generate information. First, clinicians need to use developmentally sensitive techniques that will ease the socio-emotional demands of novel interview contexts (Salmon, 2006; Salmon, Roncolato, & Gleitzman, 2003). Second, clinicians may need to introduce and prompt the child to talk specifically about their affective life (Wesson & Salmon, 2001). Finally, as children often give brief responses in the context of optimal prompting, additional prompting may be useful to increase the volume of information that children report (Pipe & Salmon, 2009). Given that children have the capacity to report their personal experiences, the clinician needs to conduct interviews that maximise children’s reports about their presenting problems and symptoms.
Researchers have attempted to identify new interview techniques that augment the amount of information that children report about their experiences without decreasing accuracy and which may be applicable to clinical settings. Drawing is one technique that has attracted a significant amount of interest and for which there is a rich history of use with children in clinical settings (Butler, Gross, & Hayne, 1995; Gross & Hayne, 1998, 1999; Gross, Hayne, & Drury, 2008; Patterson & Hayne, 2011; Rollins, 2001; Willcock, 2004). Traditionally, drawing has been used in one of two ways; either as a projective measure (Buck, 1948; Burns & Kaufman, 1970; Goodenough, 1926; Machover, 1949) or as an informal assessment tool to build rapport and to facilitate children’s verbal reports (Nawal, Glyn, & Jolley, 2005). When drawing is used as a projective measure, the focus is on what the child draws, not what the child says. When drawing is used as a tool to build rapport and facilitate children’s verbal reports, the focus is on what the child says rather than an interpretation of the child’s drawing (see Butler et al., 1995; Gregory, 2004; Gross & Hayne, 1999; Gross, Hayne, & Poole, 2006; Nawal et al., 2005; Pipe & Salmon, 2009; Thomas & Jolley, 1998; Tielsch & Allen, 2005 for discussion of the risks in assessing children’s drawing without taking into account the child’s accompanying verbal communication). The present research focuses on the use of drawing as a tool to facilitate children’s verbal reports.
Over the last decade, researchers have conducted extensive research on the use of drawing to help children describe their prior experiences in experimental and educational settings (Butler et al., 1995; Brooks, 2005; Bruck et al., 2000; Gross & Hayne, 1999; Gross et al., 2008; Patterson & Hayne, 2011; Wesson & Salmon, 2001). These studies have consistently shown that drawing increases the amount of information that children of all ages verbally report about emotional and event-based experiences. The consistent finding is that children who draw and tell about their prior experiences report twice as much information as children who tell only (see Driessnack, 2005; Patterson & Hayne, 2011 for a review). Currently, evidence that drawing facilitates children’s reports has been obtained in experimental settings in which children are primarily asked about benign or pleasant events; when children have been asked about negative events (e.g. a time when they were sad or scared) they are given the opportunity to nominate the event that they will describe. In contrast, in a clinical setting, children are asked about their presenting socio-emotional problems. They may be asked about distressing affective states or events and they may have limited options in terms of what they will discuss. Further, they are asked not only to describe an event but to provide information about what it felt like, what sense they made of it and their unique interpretation of it. Given these conditions, the key question is, would drawing help children to describe their presenting problems in an actual clinical setting during a mental health assessment? To date, whether drawing facilitates children’s reports of their affective experiences in a clinical mental health setting has not been empirically tested.
The aim of the present study was to establish whether drawing facilitates children’s verbal reports of their presenting problem during mental health assessments. We hypothesised that children who are invited to draw and tell about their presenting problem would report more information when compared with children who only tell about their presenting problem. We also examined whether drawing influenced the way in which the clinician conducted the interview. Previous research has shown that interviewers use more verbal prompts in the draw condition when compared with interviewers in the tell condition (see Patterson & Hayne, 2011 for a review). Finally, we were interested in children’s subjective views about the use of drawing in clinical assessments. Given this, we asked children whether they had a preference for drawing or telling and whether they thought that drawing made the task of reporting their presenting problem easier.
Method
A total of 33 children who had been referred to one of four child mental health clinics took part in this study (number of children recruited per site = 17, 8, 7 and 1). The four services all provide mental health assessment and treatment for children. Children were eligible to take part in the study if they were between five and 12 years old, as prior research in developmental settings has shown that children in this age range benefit from the opportunity to draw during interviews (Butler et al., 1995; Gross & Hayne, 1999; Gross et al., 2008; Patterson & Hayne, 2011). Children in the present research therefore ranged in age from five to 12 years old: 5–6 years old, n = 6; 7–8 years old, n = 6; 9–10 years old, n = 14; 11–12 years old, n = 7. There were 15 girls and 18 boys. The majority of children were of European descent (84%) and a range of socioeconomic backgrounds were represented at each mental health clinic. Ethical approval for the study was obtained from a regional Health and Disability Ethics Committee.
All of the children had been referred to the respective services for a mental health assessment. Children were referred due to symptoms of internalising disorder (e.g. low mood, anxiety), externalising disorder (e.g. oppositionality, impulsivity), or developmental disorder (e.g. delays in language, social or cognitive development) and these disorders were represented across the mental health clinics.
We gathered data from clinicians in relation to children’s medication status. Only one child who took part in the study was on an established medication regime for treatment of Attention Deficit Hyperactivity Disorder, but their presentation for this interview was for a separate set of symptoms. In addition, we made arrangements with each service such that when the assessment was complete, we could access information regarding the diagnosis or assessment outcome for each child. The diagnostic outcome was a decision made by the clinician at the end of the assessment and was based on multi-informant (i.e. parent/caregiver/child interviews, teacher interviews when applicable) and multi-modal assessment practices.
Prior to recruitment, the four mental health clinics were approached to ascertain their willingness to be part of the study. They were provided with an outline of the study, as well as the information sheets and consent forms to be used. Each of the four clinics agreed to have the study carried out in their setting. We also invited the clinicians from each service to express their interest in participating in the study; clinicians who did so were given a preliminary overview of the study and those who agreed to participate as interviewers (n = 5) were provided training in the interview protocol. The clinicians who took part in the study were female child mental health practitioners who were qualified and trained in the scope of therapist/counsellor (n = 2), nurse therapist (n = 2) or clinical psychologist (n = 1). Assignment of the child to the clinician was based on each clinic’s admission practice regarding new referrals. At some centres (n = 2), each participating clinician screened their new referrals for suitability, and if the child was identified as suitable (i.e. children in the age range and suitable for an individual assessment rather than a family assessment), they were invited to participate. At other centres (n = 2), where all initial referrals result in an individual child assessment, all children who were newly referred to the service were invited to participate. The children/families who were identified as suitable candidates for the study were sent an information pack for the study alongside the usual documentation sent by the administrator for the initial appointment.
At the initial appointment, the clinician raised the option of participation with the family. If the child and his/her caregiver indicated that they would like to participate in the study, they were recruited to the study and the process of informed consent occurred; verbal assent was obtained from the child and written consent was obtained from the parent. Children were excluded from the study if they were not able to physically manage the tasks involved in the study (i.e. unable to talk or draw). The interviewers reported that a total of eight children and their respective caregivers declined to participate in the study; at that stage, they were thanked for their consideration and the assessment process continued as per usual assessment practices without further reference to the study.
Interviewers recorded the interviews using professional audio equipment. At the beginning of the assessment, the child and his or her caregiver were introduced to the service and to their clinician, and basic background information was gathered (e.g. education, health and family composition). The interviewer spent time building rapport with the child by talking about general events and activities in the child’s life (e.g. about sport, recreation, pets and friendships). When the interviewer observed that the child was at ease, the interviewer suggested that the caregiver might have a break in the waiting area and the experimental phase of the interview commenced.
First, children were asked to provide a verbal account of their presenting problem. Prior to the interview, children were randomly assigned to one of two experimental conditions. In one condition, the tell only condition, the child was asked to tell everything that he or she could about the presenting problem. In the other condition, the draw and tell condition, children were supplied with a pack of 12 coloured felt pens and a piece of white, A3 size paper. The child was asked to draw and tell everything that he or she could about the presenting problem. The experimental phase of the interview started with the interviewer asking the child, ‘Do you know why you have come here to see me today?’ If the child identified a presenting problem, the interviewer and child established the name of the presenting problem (e.g. worry, sadness). If the child did not know why they were attending the clinic, the clinician used the referral document as a guide; ‘Well, I heard that you came along here today because…’ (interviewer stated the presenting problem the child was referred for). Once the child and interviewer established the nature of the presenting problem, the interviewer, using the child’s words for the presenting problem (e.g. angry, scared), invited the child to describe the presenting problem by saying; ‘I’d like you to tell (or draw and tell) me everything you can about [child’s word/s for the presenting problem].’ If the child did not spontaneously narrate about what he or she was drawing, he or she was asked to do so.
Interviewers in both conditions invited more detail by using a general prompt such as ‘Can you tell (or draw and tell) me anything else about the [child’s word/s for the presenting problem]?’ The interviewer could follow up general prompts (e.g. ‘So the police arrived, then what happened?’) with more direct prompts (e.g. ‘What did dad do when the police arrived?’) regarding key topics that the child reported. In addition, to encourage the child to provide additional information, the interviewer used minimal encouragers (e.g. ‘Uh huh’, ‘right’) and paraphrases and reflections of what the child said (e.g. ‘It was very sad when your mother died’). The encouragers, reflections and prompts continued until the child had no further information to report about the presenting problem.
The interviewer then asked the child if there were any other presenting problems. If the child identified other presenting problems, the interviewer repeated the interview protocol described above for the first presenting problem. This sequence continued until the child identified that there were no further issues that he or she wished to report.
Second, after the child had discussed their presenting problem in either the tell only or draw and tell condition, the child was asked two questions about reporting their presenting problem, each with accompanying answer options; one question related to the child’s preference for the use of drawing: 1) ‘There are two ways you can tell me about your [child’s word/s for the presenting problem], you can draw and tell or tell; which would you prefer? Draw or tell?’; 2) the other question related to the child’s ease of reporting: ‘How easy was it for you to tell me about your [child’s word/s for the presenting problem]? Was it easy, very easy or not easy?’ The interviewer provided the child with a written version of the questions with the child’s words for the presenting problem written in a blank space and the accompanying answer options, and read the material aloud to the child. The clinician then asked the child to indicate his/her answer by either circling the option or pointing to an option that the clinician circled on the child’s behalf. Once the child had answered these questions, the experimental phase of the interview was over and the clinical assessment of the child continued as it would usually proceed in the respective treatment setting (e.g. the child and family may reunite and spend time talking with the clinician).
The participating clinicians conducting the interviews could not be blinded to condition (i.e. draw or tell). To minimise bias or expectancy effects influencing how the children were interviewed, the exploratory nature of the study was emphasised to the participating clinicians (e.g. they were told that we are examining differences between the draw and tell conditions, we do not know the impact of draw versus tell in a clinical setting).
The experimental phase of the interview was audio-taped and all interviews were transcribed verbatim and coded in the following way. First, the amount of clinically-relevant information that the child provided was coded. Clinical relevance was defined as information that the child reported about the presenting problem and also included verbal information the child reported that was relevant to a multi-axial assessment (i.e. information about social, emotional, intellectual, communicative and physical functioning). Additional information that was not of clinical relevance was not coded. Consistent with other published research on drawing, the amount of clinically-relevant information that the children provided in both conditions was quantitatively assessed by calculating the number of clauses that were reported (see Gross & Hayne, 1998). A clause was defined as a simple sentence that contained an explicit or implicit verb such that there was one verb per clause. For example, ‘When he died’ ‘I felt I was alone’ ‘and no one was there for me’ would be coded as three clauses. Only verbal information was coded. That is, children were only given credit for things that they said during the interview. The drawings that the children produced were not subjected to analysis. Repeated information was also not counted.
The criterion for determining that a clause was clinically relevant was developed specifically for this study. Coding was carried out by two researchers (one of whom was involved in the data collection process), who were given intensive training in its use. To ensure that the coding scheme was reliable, 33% of coded transcripts were randomly selected and recoded for clauses of clinically-relevant information by an independent, trained coder who was unaware of the purpose of the research and the child’s experimental group. The total number of clause agreements, divided by the number of agreements plus the number of disagreements (agreements/agreements + disagreements) was calculated to get a reliability coefficient for the number of clauses children reported. A reliability coefficient of 94% was established for the number of child clauses.
In addition, we also examined the questions that the clinician asked during the assessment interview. Each question was coded as one of the following:
Open-ended question. The interviewer used open-ended questions to prompt the child for more information (e.g. ‘Tell (or draw and tell) me everything you can about worry’).
Closed question. The interviewer used a prompt that required the child to give a yes, no or choice answer (e.g. ‘Do you stay asleep all night?’).
Leading question. The interviewer used a prompt that suggested the desired answer or contained information that the child had not already given (e.g. ‘I bet that was fun, was it?’ ‘Is that your mum?’ when the child had not already indicated that he or she was drawing about his or her mother).
Minimal response/reflection or encourager. The interviewer used a prompt that encouraged the child to keep talking without asking a question (e.g. ‘Uh huh’, ‘Really’ or ‘Wow’). The interviewer may have reflected/paraphrased something the child said or made a supportive comment (e.g. ‘That was tricky for you’). Interviewer turns that were off task and that were not related to the event that the child was describing (e.g. the interviewer commented on noises outside the room) were not coded. Inter-observer reliability for type of interviewer turn (i.e. open-ended, closed, leading, or minimal responses) was 97% (k =0.94).
Results
Interviews were conducted with 33 children presenting for their first clinical interview at a child mental health clinic. Of these, two interviews were omitted from further analysis. One interview was omitted from inclusion due to sound distortion that rendered the recording inaudible. The second interview was omitted because retrospective information identified that the child spoke English as a second language.
Some children presented with more than one problem (n = 10, range 2–4 presenting problems). Children nominated a similar number of presenting problems across interview conditions (draw and tell M= 1.4, SD= 0.63, tell only M= 1.44, SD= 0.81, t (29) = .89, p > .05, d = .06, power = .05). In order to manage the variable amounts of information that occurred when children have more than one presenting problem, we analysed the reported information pertaining to the first presenting problem only.
Recall that the mental health service providers who conducted these interviews provided us with post-assessment data regarding the formulation and diagnoses of the children who participated in the study. Of the 31 children whose data was analysed in the present study, 90% (n = 28) were found to have met criteria for an Axis 1 psychiatric diagnosis as measured by the Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association, 2000). Specifically, the range of conditions included Attention Deficit Hyperactivity Disorder (n = 5), Tourette’s disorder (n = 1), oppositional defiant disorder (n = 1), pervasive developmental disorder (n = 1), anxiety (n = 6), adjustment disorders (n = 9) and ‘other conditions that may be the focus of clinical attention’ (n = 5; American Psychiatric Association, 2000, p. 27). Two of the group were found to have symptoms that did not reach a clinical threshold. There were no differences in the number of children who met the threshold for diagnosis as a function of interview condition (Fisher’s Exact Test, p > .05).
Preliminary analysis revealed that there were no effects associated with the person who interviewed the child, the gender of the child or the category of the presenting problem (e.g. internalising, externalising or developmental) on the amount of information that children reported. Furthermore, a Pearson product moment correlation showed that there was no association between age and the amount of information that children reported, and there was no association between age and interviewer prompting behaviour (i.e. the number of open, closed, leading or minimal responses). Given these findings, the data were collapsed across interviewer, age, gender and category of presenting problem for all subsequent analyses.
Amount of information reported
In order to assess the effects of drawing on children’s reports of their presenting problem, we conducted a one-way (condition: draw/tell) analysis of variance (ANOVA) on the number of clauses of information reported. This analysis yielded an effect of condition, F (1, 31) = 10.56, p < .01, η2 = .27. Overall, children reported almost twice as much clinically-relevant information when they were allowed to draw during the interview (M= 99.73; SD= 53.33) than when they were not (M = 50.93; SD= 26.83).
Interviewer behaviour
Next, we assessed the number and type of interviewer prompts in each interview. First, we conducted a 2 (condition: draw/tell) × 4 (prompt type; open, closed, leading or minimal responses) ANOVA. This analysis yielded a main effect of prompt, F (3, 87) = 55.98, p < .01, and a main effect of condition, F (1, 29) = 7.09, p = .01. These main effects were qualified by a prompt type × condition interaction, F (3, 87) = 5.32, p < .01, η2 = .15. The prompt type × condition interaction is shown in Figure 1.
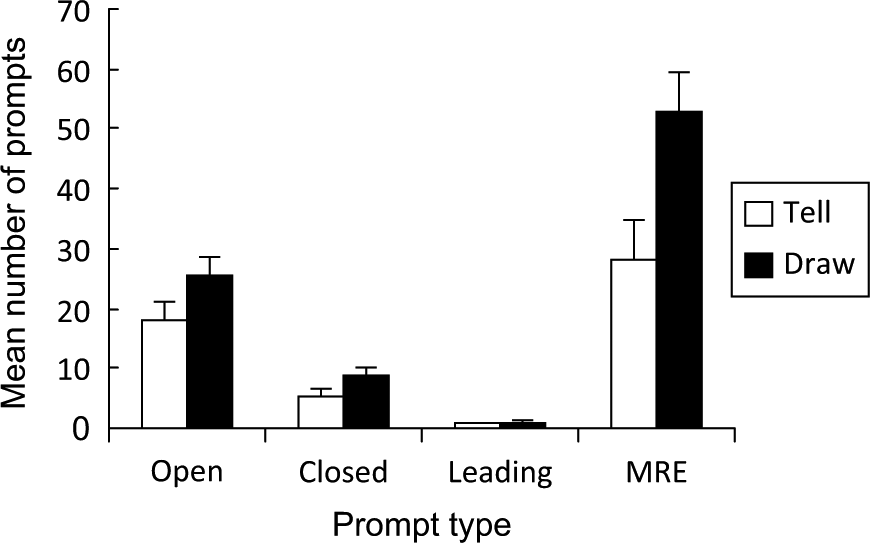
Mean number of adult interview prompts (and standard error) as a function of prompt type and experimental condition.
To evaluate the prompt type × condition interaction, post-hoc t-tests comparing each pair of bars in Figure 1 were carried out using the Bonferroni correction. These analyses revealed that interviewers used more minimal responses (MRE) in the draw and tell condition than did interviewers in the tell only condition, t(18) = 2.53, p < .01, η2 = .19, but there was no effect of condition on the number of open, closed or leading prompts.
In order to assess the relation between the number of interviewer turns and the amount of information children reported, we entered the number of minimal responses, the number of interviewer prompts (i.e. open-ended, closed and leading questions) and the number of clauses that children reported into a hierarchical regression analysis. This analysis revealed that minimal responses alone explained 12% of the variance in the number of clauses that children reported (adj R2 = .122, p< .05). Open-ended, closed or leading prompts did not contribute to variance in the number of clauses children reported. That is, the best predictor of the number of clauses that children reported was the number of minimal responses that the interviewer used.
Drawing-related factors
Research in a variety of contexts (i.e. recreational, experimental and health-related) suggests that children like to draw during interviews presumably because drawing makes them feel more comfortable (Patterson & Hayne, 2011; Pipe & Salmon, 2009; Yuen, 2004). Although the use of drawing is recommended in clinical guidelines (AACAP, 1997; Graham et al., 1999), it is not yet known whether children would actually prefer to draw during interviews in clinical contexts. That is, would children elect to draw during a clinical interview when they are given the opportunity to do so?
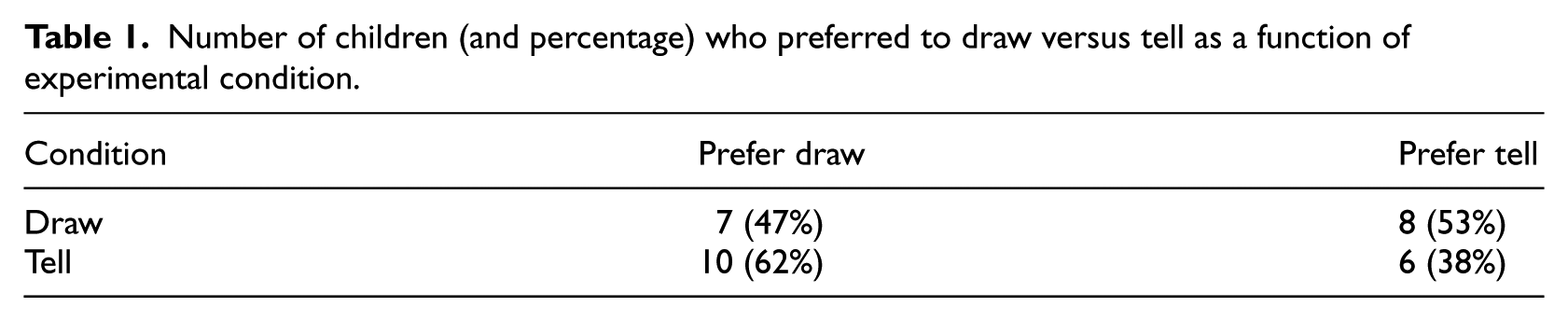
In order to address this issue, the children in the present study were asked post interview whether they would prefer to draw or tell about their presenting problem, if given a choice. Overall, 55% (n = 17) of the children in the sample indicated that they would prefer to draw rather than to tell about their presenting problem. We also examined whether the experimental condition that the child had been assigned to influenced their stated preference. That is, would children in the draw condition be more likely to state a preference for drawing? In order to answer this question, we conducted a Pearson χ2 analysis. As shown in Table 1, there was no association between children’s experimental condition and their stated preference to draw or tell, Pearson χ2 (1, 31) = 0.784, p < .376, w = .16, power = .14. Of the children in the draw condition, 47% expressed a preference for a draw interview and of the children in the tell condition, 62% expressed a preference for a draw interview.
Number of children (and percentage) who preferred to draw versus tell as a function of experimental condition.
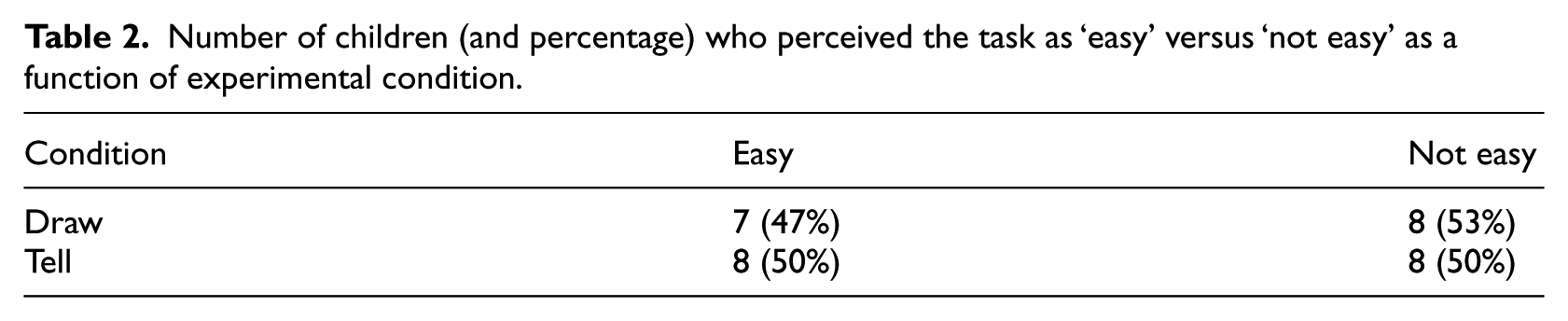
We also examined whether drawing influenced children’s perception of how easy it was for them to report their presenting problem. Recall that after being interviewed, the children were asked how easy it was to talk about their presenting problem (i.e. ‘easy’, ‘very easy’ or ‘not easy’). For the purpose of data analysis, the positive categories ‘easy’ and ‘very easy’ were combined and compared with the negative category, ‘not easy.’ Overall, 48% (n = 15) of children indicated that it was ‘easy/very easy’ to talk about their presenting problem; 52% (n = 16) of children indicated that it was ‘not easy’.
To assess whether children in the draw condition thought that it was easier to talk about their presenting problem than children in the tell condition, we conducted a Pearson χ2 analysis. As shown in Table 2, the proportion of children who perceived the level of difficulty either positively or negatively did not differ significantly between draw condition and tell condition (Pearson χ2 (1, 31) = .034, p < .853), w = .03, power = .05.
Number of children (and percentage) who perceived the task as ‘easy’ versus ‘not easy’ as a function of experimental condition.
Discussion
Research conducted in analogue settings has consistently shown that children provide more information when they are asked to draw and tell during an interview than when they are asked to tell only. Consistent with prior laboratory-based research, we found that children who drew and told about their presenting problem in a clinical setting provided twice as much information as children who told only. Overall, we found that drawing had a large significant effect on children’s reports about their presenting problems. The ability to obtain this effect with a small sample size suggests that in clinical settings, where each case essentially consists of an n of 1, drawing is likely to be useful as an interview aid. In this context, the present study provides preliminary support for the use of the draw and tell technique in clinical interviews.
The opportunity to draw not only increased the amount of clinically relevant information that children reported, but it also had a positive effect on the overall interview process. First, consistent with prior laboratory-based research, drawing increased the number of minimal responses that interviewers provided during the assessment (Patterson & Hayne, 2011; Wesson & Salmon, 2001; Willcock, 2004). Minimal responses such as ‘Oh’ or ‘Mmmmm’ do not add content to the conversation, but rather signal to the speaker that what they are saying is interesting and important. Minimal responses are considered part of optimal interviewer behaviour because they create a supportive context that is helpful for the child (Pipe & Salmon, 2009; Salmon, 2006). In the present study, as in others (Patterson & Hayne, 2011; Willcock, 2004), the number of minimal responses that the interviewer provided was the best predictor of the amount of information that the child reported. Second, interviewers in both conditions adhered to optimal interviewing practices (i.e. asking predominantly open-ended questions) and demonstrated few negative interviewing practices, such as large numbers of closed or leading questions (Lamb, Orbach, Sternberg, Esplin, & Hershkowitz, 2002; Lamb, Orbach, Hershkowitz, Horowitz, & Abbott, 2007; Orbach & Lamb, 2001). The use of a semi-structured interview, as outlined in this study, may prove beneficial by assisting the interviewer to gather information from the child using predominantly open-ended questions and encouragers or reflections.
Because prior research has shown that children like to draw and that they report that drawing helps them to talk in a clinical setting (Davies & Wright, 2008; Patterson & Hayne, 2011; Yuen, 2004), we also examined children’s subjective views about the use of drawing in the clinical assessments. That is, we asked children whether they had a preference for drawing or telling about their presenting problem. We found no evidence supporting the idea that drawing is a preferred activity (e.g. approximately half of the children reported a preference to tell about their presenting problem). Additionally, we examined whether drawing had any impact on children’s perception of how easy or not it was to talk about their presenting problem. We found no evidence that drawing made it easier for children to talk about their presenting problem. The mechanism by which drawing increases the amount of information children report is as yet unknown. However, in this study, the facilitative effect of drawing does not appear to be related to children’s subjective views about the benefits of drawing nor is it related to drawing making the task subjectively easier for the child.
In the present study we did not examine, nor standardise, the rapport building stage of the interview. The interviewers were all clinicians in a clinical setting conducting actual assessments; their primary goal was to establish rapport with the child irrespective of our research protocol. Thus, although rapport-building followed a similar format for all children (e.g. asking the child about activities they enjoyed), the rapport-building was slightly different for each child, depending on their needs. Previous research examining the impact of rapport building on the amount of information that children provide has produced varying results. For example, Davies, Westcott and Horan (2000) found that lengthy rapport building may be counterproductive, with children providing less information following protracted rapport building times. Teoh and Lamb (2010) found no association between the length of rapport building, or the type of prompts used in rapport building, and the informativeness of children’s responses. In contrast, Sternberg et al. (1997) found that rapport building could influence the amount of information children provided by training children to respond informatively to open ended questions. Given that current research does not directly speak to the impact that rapport building has on the amount of information children provide, we recommend that future research take the rapport building stage into account and examine the rapport building stage in relation to the amount of information children provide.
In a clinical setting, the accuracy of the information obtained from the child must also be considered. Accuracy becomes paramount in forensic interviews where explicit and highly accurate information about an event must be obtained. In clinical interviews, the required information often pertains to subjective information from the child’s perspective. In the present study we used the draw and tell technique to elicit the child’s phenomenological account of their symptoms, distress or impairment. Although there was no way to assess the accuracy of the information that children reported, previous research in analogue settings suggests that drawing about past events or experiences does not decrease accuracy, as long as interviewers use open ended questions rather than suggestive or misleading questions (Lamb et al., 2007, 2002; Larsson & Lamb, 2008; Orbach & Lamb, 2001).
Previous researchers have commented that the symptoms of psychopathology may impair a child’s ability to provide a self-report (Tielsch & Allen, 2005). The children who took part in this study presented with a complex range of symptoms, which is typical of the clinical child population. Irrespective of their presenting symptomatology, we found that children meeting criteria for a DSM-IV (2000) diagnosis were able to provide adequate amounts of information about the level of distress or impairment that resulted from their symptoms. Recall that children in the tell condition were able to provide, on average, 50 simple sentences about their presenting problem and that drawing further increased the amount of information they reported to, on average, 100 simple sentences. These findings suggest that even in the presence of psychopathology, children can describe their experiences and that drawing further helps children to talk about their presenting problems.
We acknowledge that our sample size was relatively small, the children were from a broad age range (i.e. 5–12 years of age) and there was a range of presenting problems that children discussed. Despite these potential limitations, the effect of drawing was clear and the findings are highly consistent with prior research on drawing in other interview contexts. Although we found no relation between age or presenting problem and the amount of information reported, additional research with larger samples may reveal such relations (e.g. see Patterson & Hayne, 2009 for the effect of age on the amount of information children provide). As with any new clinical technique, we acknowledge that additional research will be required before definitive statements can be made about the effect of drawing on children of different ages who have different cognitive, emotional and language abilities and who present with different symptomatology. Additionally, although the present study focused on the use of drawing in an individual assessment, it may also be effective in other types of assessment (e.g. family assessment). This possibility remains to be determined.
In conclusion, the present study demonstrates that drawing as a means to facilitate children’s verbal reports is useful in clinical as well as experimental settings. That is, drawing increases the amount of verbal information that children report about their presenting problem and when children draw, interviewers use more minimal responses thereby creating supportive interview contexts. Further, drawing is a cost effective and readily available resource and it is a medium that children find familiar and enjoyable (see Patterson & Hayne, 2011). It is a structured exercise that provides a shared focus of attention for the interviewer and the child. It also allows the interviewer opportunities to observe aspects of the physical, attentional and interpersonal profile of the child in a non-intrusive way (e.g. is the child focused on the task or distractible? Or how does the child interact with the interviewer?). Given the value of drawing as a means to increasing children’s verbal reports about their presenting issues, the present study provides preliminary support for the use of drawing in clinical settings. Ensuring that clinicians have adequate training and are competent and comfortable with the use of drawing as a tool to facilitate children’s verbal reports is a pre-requisite to the use of drawing as part of regular clinical assessments.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.