
Abstract
The behaviour of children in foster care is influenced by a variety of factors including previous experiences of maltreatment and adverse parenting, as well as the impact of separation from birth parents and placement in care. These factors make it difficult for foster parents to accurately interpret the child’s behavioural cues, a necessary precursor to sensitive parenting. The relational learning framework introduced in this article, drawing on attachment theory, facilitates the foster parents’ access to some features of the child’s mental representations, or internal working model, which may be pivotal in understanding the child’s behaviour and therefore successfully managing it. Recent studies suggest that parents’ ability to understand the child’s psychological perspective, or mental state, is related to the child’s cognitive and social development. This article presents a method to enhance the foster parents’ understanding of the child’s psychological perspective. The model is currently being evaluated for use with foster parents, mental health and social work practitioners.
Keywords
Introduction
The relational learning framework, introduced in this article, was developed as a method to help foster parents consider how their foster child’s past experiences of maltreating and impermanent relationships may influence the child’s ideas, expectations and behaviours in relationships. The framework is derived from attachment theory, and is compatible with the concept of core beliefs and interpersonal schemas, as articulated in Aaron Beck’s cognitive theory (Beck, 1976), relating to the way in which adverse experiences affect children’s views of themselves, others and the world. The relational learning framework has been developed as a cognitive technique to aid foster parents and practitioners to understand the psychological perspective of the child. Thus rather than an attachment intervention aiming to improve foster parents’ sensitivity and attunement, the primary aim of the relational learning framework is to remove barriers parents may have to understanding and empathising with their foster child.
The framework focuses attention on the child’s mental representations, which are considered to be ‘the means through which children package their experiences and carry them forward’ (Dweck & London, 2004, p. 428). It integrates salient information from a child’s history and experiences with information about their current behaviour, providing insight into the child’s mental representations, ideas and expectations about himself or herself and other people. This information can then be used by foster parents to provide the corrective experiences and verbal messages the child needs to develop more positive expectations of future relationships.
As it is presented in this article, the relational learning framework can be used in case conceptualisation, formulation and case reviews. Using it with foster parents as an intervention requires further empirical evaluation, which is in progress (Kelly & Salmon, to appear).
Foster care and mental health
Children placed in foster care show an array of complex behaviours influenced by adverse experiences such as maltreatment, witnessing of violence, parental substance abuse and mental health concerns and impoverished and chaotic environments (Oswald, Heil, & Goldbeck, 2010). The prevalence of clinically significant emotional and behavioural problems such as non-compliance, aggression, problems with impulsivity and attention, anxiety and depression in children involved in child welfare investigations has been found to be 42%−48%, with many of these children not receiving mental health care (Burns et al., 2004; Garland et al., 2001). Children in foster care show rates of externalising behaviour over double than that seen in children in the community, with an average of 42% for children in care, compared to 7%−20% for children in the community (Keil & Price, 2006). Factors related to foster children developing mental health problems include longer exposure to an adverse environment, coming into care at an older age, developmental delay, placement instability and lack of a permanent placement (Tarren-Sweeney, 2008).There have been mixed findings regarding whether entry into foster care in itself has a positive, negative or neutral effect on children’s externalising behaviour problems (e.g. Berger, Bruch, Johnson, James, & Rubin, 2009; Lawrence, Carlson, & Egeland, 2006), but children’s behaviour problems have been shown to both contribute to and subsequently increase after the experience of placement disruption (Oosterman, Schuengel, Slot, Bullens, & Doreleijers, 2007).
Placement instability is common in foster care (Osborn, Delfabbro, & Barber, 2008). In addition to effects on externalising behaviour problems, placement instability has negative effects on children’s inhibitory control, trust in caregivers and sense of security and has been shown to increase indiscriminate friendliness or lack of reserve with unfamiliar adults (Pears, Bruce, Fisher, & Kim, 2010; Unrau, Seita, & Putney, 2008). A minority of children do not achieve a stable placement, and some children with severe maltreatment histories and conduct disorder can experience up to 30 or more placement changes (Osborn et al., 2008). Once children start on a trajectory of placement disruption due to externalising behaviour problems, it is likely to continue, with children who have two or more behaviour-related placement disruptions having only a 5% chance of achieving placement stability 2 years later (Barber & Delfabbro, 2004).
While little is known about how older children form attachment relationships in foster care, toddlers have been shown to have rejecting and avoidant behaviour in response to new caregivers and to take longer to develop stable patterns of attachment security than infants (Stovall-McClough & Dozier, 2004). Some of these behaviours may interfere with the ability of foster carers to provide the child with the warm and responsive care needed to help overcome the effects of previous poor care (Bernier, Ackerman, & Stovall-McClough, 2004). Despite this hurdle, young children in foster care become securely attached to their caregiver at very similar rates to biological parent–child relationships, with just over half of the children developing secure attachment (Dozier, Stovall, Albus, & Bates, 2001). However, young children in care have more difficulty adapting to their foster parents’ parenting style when the parents themselves have an insecure state of mind regarding attachment; thus, these children are more likely than biological children to develop a disorganised attachment (Dozier et al., 2001). This has been shown to be a risk factor in the development of mental health problems (Fearon, Bakermans-Kranenburg, van Ijzendoorn, Lapsley, & Roisman, 2010).
The majority of children in foster care have been maltreated, with subsequent effects on their ability to regulate their emotions and stress responses (Kim & Cicchetti, 2010; McCrory, De Brito, & Viding, 2010). Foster children show low basal levels of the stress hormone cortisol, and a flatter slope across the day, than low-risk children, although not as marked as children who remained with birth parents after a child protective services investigation (Bernard, Butzin-Dozier, Rittenhouse, & Dozier, 2010). Foster children also have poorer visuo-spatial ability, language skills and general cognitive functioning compared to other children living in low-income but not maltreating families (Pears & Fisher, 2005). Since children in foster care often do not receive any specialist mental health care (Burns et al., 2004), it is critical that foster care is as stable and reparative as possible.
Treatment for children in foster care
Most training programmes for foster parents are located within child protective services and focus on the decision to provide care and relevant policies and regulations. These programmes have been criticised for not paying sufficient attention to training parents in behaviour management (Dorsey et al., 2008). The authors note that ‘there is remarkably little empirical evidence for the type of training that foster parents receive’ (Dorsey et al., 2008, p. 1412) but that more recent studies have been more rigorous and have evaluated the use of interventions developed for other populations with foster parents. A Cochrane review found evidence across six randomised control trials that behavioural and cognitive behavioural programmes used with foster carers were not effective (Turner, Macdonald, & Dennis, 2007) and a study of the use of outpatient mental health services for foster children showed little effect of these services for foster children (Bellamy, Gopalan, & Traube, 2010).
A recent review located eight foster parent interventions which had an effect on at least one aspect of the foster child’s functioning in a randomised control trial (Leve et al., 2012). These therapeutic approaches were Attachment and Bio-behavioural Catch-up, which is an attachment-based intervention for pre-schoolers (Dozier, Peloso, Lewis, Laurenceau, & Levine, 2008), behaviour management programmes for school-aged children and the intensive Multi-dimensional Treatment Foster Care used with pre-schoolers and adolescents (Fisher & Kim, 2007). A systematic review found 30 studies involving 20 interventions and identified five types of interventions including wraparound services, relational and non-relational interventions for caregivers and children, caregiver training programmes and interventions for the child (Kinsey & Schlösser, 2013). The study concluded that wraparound services and relational interventions were supported by empirical studies but that most caregiver training programmes were not.
It appears that these differing findings regarding the effectiveness of interventions in foster care may be a result of lack of rigour in early studies (Dorsey et al., 2008), methodological limitations (Rork & McNeil, 2011), the degree to which programmes have tailored their content to the psychological factors thought to be critical in foster care and the adaptation of interventions shown to be effective with other populations (Leve et al., 2012). These authors note that ‘Overall, effective programs are attachment focused or have evolved from parenting interventions, based on social-learning frameworks’ (p. 1206).
A potentially fruitful target of intervention which has not been applied to the area of foster care is the foster parent’s mental representations, or the way the foster parent conceptualises and thinks about the foster child’s perspective and behaviour. Studies using the concepts of mentalisation and mind-mindedness in birth families have shown the impact of parents’ mental representations on an array of socio-emotional outcomes for children (e.g. Meins, Fernyhough, Fradley, & Tuckey, 2001). Studies suggesting that these concepts may be usefully applied to foster care interventions are now addressed and a method to introduce this into foster parent training and professional case conceptualisation is described.
Mental representations and foster care
Researchers have explored the influence of the way a parent thinks about his or her child through the concept of mind-mindedness, and Meins (1997) has proposed that parents’ levels of mind-mindedness may help explain how attachment states of mind are transmitted from one generation to the next. This research has shown that parents who treat their young children as if they have a mind of their own, and who use a high level of mind-related comments in conversation with them, or verbal description of them, have children with secure attachment and an ability to reason about the beliefs and mental states of other people, referred to as theory of mind (e.g. Meins et al., 2001; Meins et al., 2003).
Fostering may affect the ability of the parent to interpret the child’s mental state, or mind-mindedness, as Lawler (2008) notes that foster care relationships ‘rely heavily on a foster mother’s expectations and interpretations of a foster child’s behavior, which usually includes an array of emotional deficits and behavioral problems’ (p. 1131). Some authors have also noted the importance of foster carers not perceiving the child’s difficult behaviour and need for affection as a threat, which may affect the parent’s ability to care for the child in a non-defensive way (Wilson, 2006). It is possible that foster parenting makes higher demands on the parent’s ability to take the child’s perspective and to infer the child’s mental state from their behaviour. Schofield and Beek (2005) found that caregivers who were rated as highly sensitive had an ability to reflect and empathise with the child, believed they were central to the child’s well-being and had developed theories about the child’s past that helped them to explain their present behaviour, which impacted on the child’s progress in the placement.
Children in care may also have mental representations or beliefs which reflect their adverse experiences and negative perceptions of future care. Milan and Pinderhughes (2000) found that children’s negative perceptions or mental representations after maltreatment by their biological mother were related to the severity of maltreatment by the mother and influenced their new relationship with the foster mother. Studies with pre-school children have shown that maltreated children have more negative mental representations about the mother–child relationship than do non-maltreated children and view such relationships as ‘less fulfilling, safe and reliable’ (Stronach et al., 2011, p. 142). In one study, over half of the children who had been in a stable placement since toddlerhood had negative self-perceptions at the age of 5 and 6 years (Ackerman & Dozier, 2005). These were more likely to develop when foster parents were not fully emotionally invested in their foster children (Ackerman & Dozier, 2005).
Attachment theory proposes that the above findings can be explained by the concept of the child’s internal working model, meaning that, over time, children build a representational model of themselves and their caregiver. Bowlby (1973) proposed that ‘each individual builds working models of the world and of himself in it, with the aid of which he perceives events, forecast the future, and constructs his plans’ (p. 203). The idea of the internal working model is inherently a relational one and parents are also proposed to have an internal working model of the child and of the self as an attachment figure (Bowlby, 1973). Furthermore, the relationship between parent and child is influenced by both individuals’ internal working model, and change in one person’s behaviour may bring about resistance in the other and an attempt to return the relationship to old patterns (Bretherton & Munholland, 2008).
A recent study of the causal attributions foster parents, residential caregivers, social workers and mental health professionals make when dealing with foster children’s challenging behaviours showed that individuals have diverse views on the origins of and solutions to the challenging behaviour of children in care (McLean, Kettler, Delfabbro, & Riggs, 2012). Explanations of behaviour were categorised into six themes including conceptualising behaviour as learnt, as carrying meaning and purpose, as a conscious choice or as arising from constant change in the child’s life, from strong emotions and from the child’s attachment history. The authors describe some of the implications of these diverse frameworks for who may be blamed for the behaviour, whether it is seen as amenable to help, and for the ability of workers with different views to collaborate (McLean et al., 2012). The relational learning framework, developed by the first author, uses the concept of the child’s internal working model to provide a way to integrate the various explanations foster parents and professionals have for foster children’s behavioural difficulties.
The relational learning framework
The relational learning framework can be used to assist foster parents to understand how the child’s behaviour provides crucial clues about how his or her previous adverse experiences have changed the child’s view of himself or herself and others.
For example, two siblings may have experienced similar physical abuse with very different outcomes: one sibling may be aggressive and the other may be withdrawn. These two different outcomes may be indicators of each child’s mental representations – one involving notions of power and dominance and one involving notions of further hurt and fear. Research has shown that parents’ beliefs and attributions are related to the quality of care they provide their children (Daggett, O’Brien, Zanolli, & Peyton, 2000). If foster parents are taught to think about the child’s internal working model and how that influences the child’s behaviour, it is possible that this may change the foster parents’ attributions regarding difficult behaviour, particularly blame of self or foster child, and their behaviour management of the child. This knowledge is important as children in care may have beliefs which impact the effectiveness of reinforcement contingencies on behaviour. For example, a hug to a child without an abuse history may be positively reinforcing but to a child in care it may be aversive as it is perceived to be frighteningly intimate. Thus reinforcers may have different meanings for foster children which parents may need to take into account when using behaviour management techniques.
The child’s insecurity and uncertainty about his or her future may influence his or her behaviour and mental health (Tarren-Sweeney, 2008). A foster child who has been moved to several foster homes because of his or her behaviour may learn that increasing negative behaviour is a powerful strategy to influence his or her future. A child whose behaviour is driven by fear, such as a maltreated child who has experienced multiple placements and who fears being abandoned, asked to leave or abused, will need different behavioural responses from his or her foster parent than a child who does not have these fears. For example, a child may become very intrusive of the foster parent, checking emails and letters, going through the parent’s bedroom drawers and questioning the parent. Typical behaviour management techniques such as locking up personal items and giving the child negative consequences for the behaviour may make the behaviour worse. The child’s behaviour may be due to fear that the placement will end or that a letter will arrive with bad news about the child’s future in it. In this case, the fear must be addressed first.
The relational learning framework can be seen as a way of increasing the foster parent’s cognitive understanding of the child or mind-mindedness. Recent authors have noted the importance of assisting foster parents to understand the behaviour of the child in their care, in the light of his or her past history (Wotherspoon, O’Neill-Laberge, & Pirie, 2008). The aim of mental health consultation is to understand the experiences underlying the child’s behaviour, which appears out of context and can seem inexplicable to the caregivers (Wotherspoon et al., 2008). This approach requires the mental health clinician to make an interpretation of the child’s behaviour, in the light of his or her experiences, and then discuss this with the foster parents. The relational learning framework provides an alternative way to teach foster parents to think about the child in care, allowing them to make the connections themselves, with the therapist only highlighting information from theory and scientific knowledge, for example, the effect of maltreatment on brain functioning. This means that foster parents can apply the model to new situations as they emerge and to new children they may foster in the future.
The framework addresses the child’s culture as studies have shown that children who are fostered by a family of a different culture report more internalising problems and the foster parents report more externalising behaviour problems (Anderson & Linares, 2012). In a study of minority adolescents adopted by White parents, Leslie, Smith and Hrapczynski (2013) found that discrimination had a negative impact on the youth but that this was less stressful if their adoptive parents ‘worked to promote cultural pride and prepared them for dealing with racism’ (p. 78).
Clinical experience of the first author shows that children may reject their own culture if they perceive the culture to be inseparable from the maltreatment they have experienced within their birth family. It is thus important to examine what attributions the child has made about his or her culture, and if the child’s foster family is of a different culture, what attributions have been made about this difference. The relational learning framework is currently being evaluated with groups of foster parent and foster care practitioners.
Applying the relational learning framework
The relational learning framework can be used as a case consultation tool, as part of clinical supervision, in multi-disciplinary team meetings and for intake purposes. It takes 1 to 2 hours to complete and can then be reviewed at intervals to update the treatment plan and manage crises. The framework is a work in progress having been used over 200 times in clinical consultations and it is also currently being empirically evaluated (Kelly & Salmon, to appear).
The relational learning framework is presented as a compact visual table (see Table 1) which can be used to consider all aspects of a particular foster child’s experience and the implications for relationships. The purpose of the framework is to bring knowledge about the child together so that the team as a whole has the same information, to make connections between the child’s past history and current experiences, to consider the meaning the child may have made of his or her experiences and to examine what the child’s experiences and behaviour can tell us about his or her beliefs and mental representations. The ultimate aim is to form a treatment plan to gradually change the child’s mental representations over time, emphasising what the child needs to learn through relationships, what the child needs to learn about emotions and how to talk to the child to verbalise both old and new representations, for example, ‘You used to think everyone would hurt you but you have learned we don’t hit here’.
The relational learning framework.
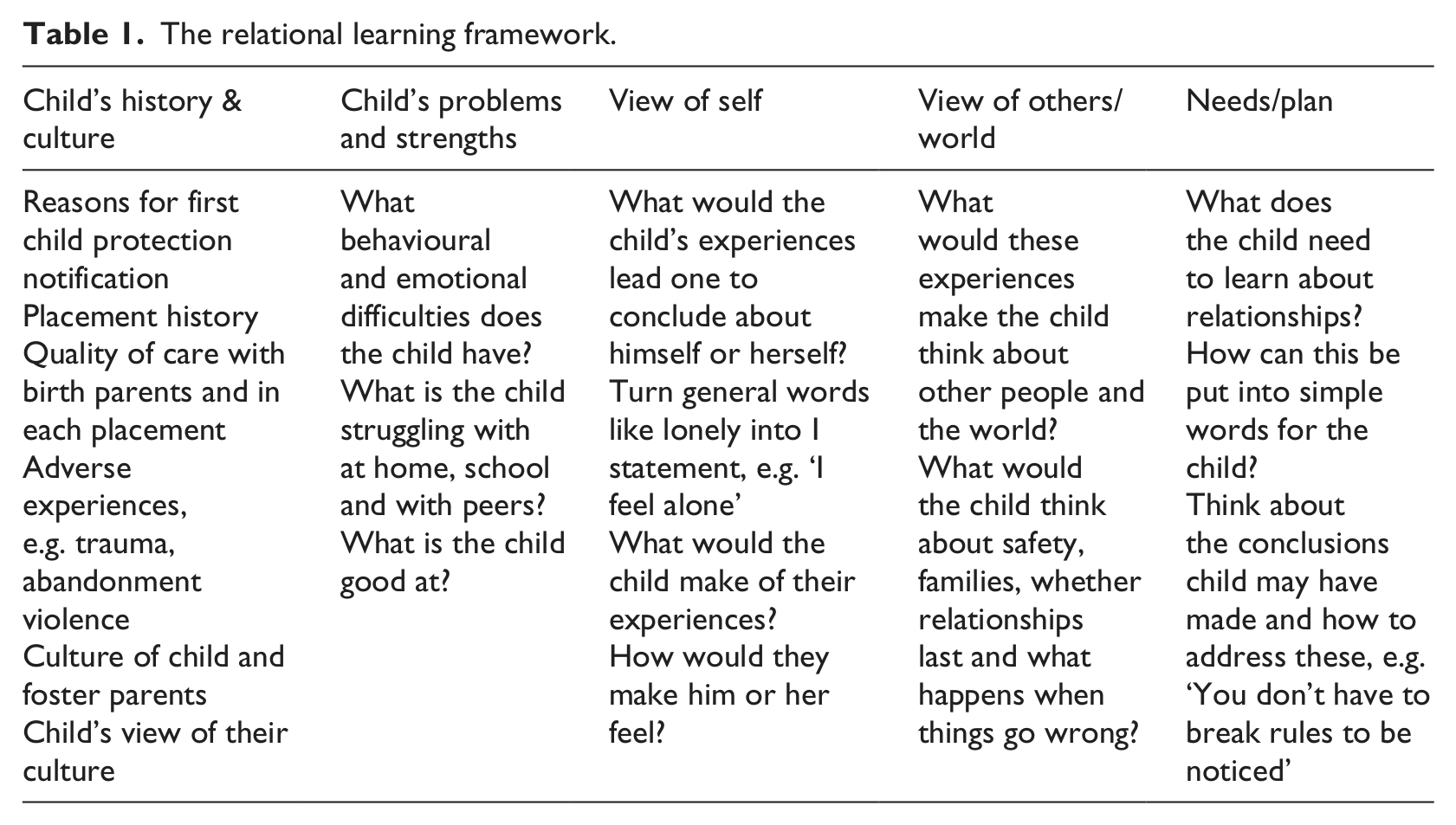
The relational learning framework consists of five columns of information directly relating to a child’s internal working model. The facilitator obtains the information from foster parents and foster care practitioners in the room and highlights important developmental and maltreatment factors (see Table 1). The reader will notice that the child is not involved in the process. The reason for this is that as it stands the method would be overwhelming for the child or young person and requires modification to ensure that it does not have a negative impact.
The framework is worked through according to the following steps.
Step 1: History and culture
The facilitator draws out the child’s history starting with the first care and protection notification, what is known about the child’s life prior to this notification and what occurred as a result of the notification. Emphasis is placed on each of the families the child has lived with, the quality of the care and both positive and negative experiences in each home and the number of changes the child has had. The facilitator draws the group’s attention to the child’s experiences which are likely to impact his or her behaviour and mental health, especially maltreatment, frightening and traumatic events, lack of basic necessities such as food, level of supervision, abandonment and changes of placement, school and neighbourhood. Lastly, the facilitator asks about the impact of these adverse events in the birth family on the child’s perception of his or her own culture and whether maltreatment has changed that.
The role of the facilitator is to use scientific knowledge of child development and the effects of maltreatment to draw attention to formative experiences. The facilitator discusses the impact of events happening at a particular developmental level and what sense the child may have made of the event, given the expected cognitive and language ability at that age. Connections are made between events in the child’s life and his or her behaviour, such as a child who was starved hoarding food in his or her bedroom. The facilitator focuses on the meaning or attributions the child may make about events, so close attention is paid to any times the child was singled out or treated differently from siblings, especially if siblings were returned home but the child remained in foster care, and any events the child may take blame upon himself or herself for, such as a child having to move placement because a foster parent became ill. This information draws attention to the factors which may be affecting the child’s current behaviour and mental health.
Step 2: Problem behaviours and strengths
In this section of the framework, the issues the child is struggling with at home, school and in the community are highlighted. The child’s strengths are also covered as they can provide information about what aspects of the child’s life have not been affected by his or her experiences.
Step 3 and 4: View of self and the world
The foster parents and social workers are invited to consider what the child’s experiences and set of problems/strengths suggest about the child’s beliefs about himself or herself. Any suggestions are written up in the first person, such as ‘I’m not loveable’; ‘I’m the odd one out’; ‘I have to take care of myself’. They are then invited to consider what the child’s experiences and set of problems/strengths suggest about his or her beliefs about other people or the world, such as ‘The world is unsafe’; ‘People leave you’; ‘Relationships don’t last’. Conversely, a child’s pro-social behaviour may suggest the child believes that people and relationships are worth persevering with.
The participants are then asked to consider what this history is likely to have made a child conclude about families, relationships, leave takings, women and men and how you solve problems. The participants are prompted by questions such as ‘What would the child think a family is … Men are … women are …’ This technique brings out important child representations such as ‘Women can be treated however you like’; ‘Families don’t last’; ’If you have a problem, do something so you get to leave’. These representations can have a major impact on the child’s behaviour and need to be changed through a myriad of experiences which negate conclusions formed in an abusive family environment.
Step 5: Emotional and relationship needs
Having completed the sections of the framework outlined above, it becomes clear what corrective experiences the child needs. Participants usually say these in global terms, for example, security or permanence. They can then be asked, ‘What is it about security that the child needs to experience?’ ‘What would they learn from permanency?’ By answering these questions, foster parents begin to clearly see what aspects of care the child would particularly benefit from.
Step 6: Putting it into words
Foster parents are then taught how to frame up the ideas they want their child to learn and to talk to the child about it. For example, a 10-year-old child who has had supervisory neglect and been allowed to roam the neighbourhood, come home at any time and often found the house unoccupied may have difficulty adjusting to family life and appropriate supervision. The group may decide the child would find it hard to keep the rules and may find ordinary family life confining. The foster parent is encouraged to help the child understand his or her predicament. The parent might say,
No wonder you find it hard when I tell you to be home after school, you used to go wherever you wanted to. Families need a rule like that to keep you safe. We have the rule because we care what happens to you.
Case example
This case example is a composite of several real case histories. Floyd is a 13-year-old boy who was placed in residential care after he could not be contained in a foster family setting. In foster care, he absconded for more time than he was actually present, he was brought home several times by police in an intoxicated state and he was being recruited by a local street gang. He had committed several burglaries, including of his grandfather and other family members’ homes. Prior to coming to the attention of child protection services, Floyd had experienced much disrupted care. Until the age of 4 years, he had been in the care of his parents, whose drug taking meant he was not fed regularly, was often left unsupervised and he had witnessed violence and intimidation of his parents due to drug debts. At the age of 4 years, 6 months, Floyd went to live with his maternal aunt but his behaviour was too difficult for her to manage. His grandfather could manage his behaviour but he did this by not setting limits on Floyd and allowing him to do what he wanted. Because of these difficulties with his behaviour, several family members took turns looking after Floyd. When his behaviour worsened, another family member would look after him for a while. Floyd’s father is serving a 5-year jail sentence for assaulting Floyd’s mother, which Floyd witnessed. Because the family had a strong belief in avoiding involving professionals in their lives, a first notification to child protection services did not occur until Floyd was 11 years old. Floyd was placed with an interim carer and had two prospective permanent placements, which both broke down due to his absconding. He fared better with his maternal grandmother for a period of a year but became increasingly threatening towards her, which culminated in an incident where he threatened her with a knife. He was then placed in a residential setting.
Step 1: History and experiences
The aim of doing the relational learning framework for Floyd is to consider what his experience and behaviour can tell us about his mental representations. The salient factors for Floyd include neglect by his parents, witnessing violence, the family passing him around different family members when his behaviour became unmanageable, the family culture of not seeking help or alerting authorities, the number of changes of caregiver and his reaction to being placed (running away, violence). The group is encouraged to consider the developmental impact of Floyd being hungry and unsupervised as a toddler, being moved for difficult behaviour, having no help or involvement of social services until Floyd was 11 years old and witnessing frightening events when he was too young to influence them. The group is invited to think about what Floyd may have made of these events and what conclusions he may have come to about himself and his relationships. The facilitator might summarise Floyd’s experiences as follows:
Floyd was with his mother, then his Aunt, then his grandfather, then moved around their care for short periods, and then had 3 placements with foster families before moving to his grandmother’s and then a residence. That amounts to 7 major changes of caregiver and several periods of unstable care where he moved around every 2 or 3 weeks. What would he learn from that?
Summaries such as this highlight the impact of his family and foster carer’s not managing his behaviours and can be discussed to highlight conclusions he may have drawn from these experiences, such as that he is more powerful than adults and that the way to solve a problem is to leave the situation.
Step 2: Problem behaviours and strengths
The pattern of Floyd’s behavioural strengths and difficulties can inform us about his possible representations of relationships. Floyd’s use of absconding, threatening violence and gang associations suggest that he has learned to value power and control over others and that violence can be an effective strategy for him. One of his strengths is a close relationship with his grandfather, suggesting that Floyd may not have given up on the possibility of getting close to people.
Step 3 and 4: View of self and the world
Given Floyd’s history and behaviour, the group is asked to consider what Floyd might think about himself and the meaning he may have attributed to events, for example, Floyd may have concluded that he was moved between family members’ homes when his behaviour escalated because he is too dangerous to be in a family and that no one can control him. The group then considers what Floyd’s experiences and behaviour tell them about his view of other people and the world such as that adults are not effective and cannot be relied on to keep you safe and that violence is the way to solve problems.
Step 5 and 6: Treatment plan and verbal messages
When participants are asked what a child in foster care needs from relationships, they will invariably say love, care, stability, safety and someone to believe in him or her, such as a mentor. These generalised qualities are deconstructed to examine what Floyd needs to know or understand about each experience: for example, what is it about stability that he needs to learn; what does he need to understand about relationships? Answers may include learning that families can be together without fighting, that relationships can last and that he can be helped to manage his behaviour. The group then comes up with brief messages which can be said to Floyd to assist him to change his negative beliefs, for example, ‘We don’t have to fight’; ’We can solve this’; ‘You don’t have to leave to feel ok’; ’Feeling bad doesn’t need to spoil us having a nice time’ and so on. The aim of these verbal messages is to reinforce the differences in the relationships in the foster home, compared to the child’s previous adverse environment, that the child may not have attended to or understood. Putting these differences into words helps to gradually change the child’s mental representations and understanding of both self and relationships.
Conclusion
There is preliminary evidence that foster parents’ thinking about the child in their care influences the outcome for the child (Bernier & Dozier, 2003; Schofield & Beek, 2005). There is also evidence that children’s thinking and negative mental representations affect their relationship with new foster parents (Milan & Pinderhughes, 2000). The relational learning framework offers a window into the child’s internal working model and mental representations which may modify the foster parents own mental representations, such as increasing understanding of the origins of the child’s behaviour and decreasing self-blame.
The framework can be used to assist foster parents to make sense of what is happening for the child and within the family. It also allows foster parents and social workers to quickly develop a shared view of the young person and their difficulties and can be used to sort out divisions within the caretaking team. Two studies are currently underway to evaluate the effectiveness of using the framework with foster parents, social workers and mental health clinicians who work in foster and residential care.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.