
Abstract
Access to needed mental health services can be particularly difficult for newly arrived refugee and asylum-seeking adolescents, although many attend school. This study examined young refugees’ impressions and experience of mental health services integrated within the school system. Semi-structured interviews were conducted with 40 adolescent refugees discharged by three school-based mental health services across the United Kingdom. Two-thirds preferred to be seen at school. Rumination and worry about insecurity in the asylum process had a negative impact particularly on the adolescents’ social functioning and ability to focus at school. The important role played by teachers in supporting and mediating contact with mental health services was valued by those interviewed. The study confirms that schools offer an important location for mental health services for adolescent refugees and provide an important portal for integration of services.
Background
It has been estimated that over 90% of migrant and refugee children deemed in need of mental health services never receive them (Ellis, 2011) due to factors both specific to refugee populations and general to all vulnerable populations. There are two main, overlapping categories that these barriers to receiving mental healthcare can fall into: service accessibility and stigma. In considering service accessibility, refugee populations might have little prior knowledge of mental illness and mental health services. Equivalent services are poorly available in low- and middle-income countries (Eaton et al., 2011; Patel et al., 2007), from where the majority of refugees/forced migrants come, and so it is difficult to expect these newly arrived populations to understand the potential role services can play. Difficulties might arise with knowing how to access services and for which problems. Language barriers are particularly important to overcome in mental health assessments and asylum seekers might have concerns as to whether their asylum applications might be negatively influenced by accessing services. Furthermore, mental health services might be poorly prepared to ensure they are accessible and culturally competent to meet the needs of young refugees and their families, with, for example, little integration with other relevant teams such as those helping with education, housing and legal services as well as other community and voluntary organisations (Dura-Vila, Klasen, Makatini, Rahimi, & Hodes, 2013; Hughes, 2014).
All of these difficulties can be compounded by the stigma associated with mental illness, making it even harder to access services. Stigma is a complex term that explains experiences broadly in the areas of social, institutional and self-stigma (Livingston & Boyd, 2010). All these aspects of stigma are potentially relevant to refugee children when trying to address their mental health needs within schools. For example, they might be concerned that their family, peers or teachers might judge them differently if they are seen to have a mental illness – social stigma. They might be worried that their asylum application or educational opportunities will be disadvantaged if they have a mental illness – institutional stigma – and finally, they might devalue themselves and anticipate social rejection if they have a mental illness: self- or internalised stigma (Corrigan, Kerr, & Knudsen, 2005; Livingston & Boyd, 2010).
Schools offer a potential location for mental health services as the majority of young people spend considerable time at school where they interact with their peers as well as engage in academic activities (Cheney, Schlosser, Nash, & Glover, 2014; Fazel, Hoagwood, Stephan, & Ford, 2014). Existing research has explored the contribution school-based mental health services might make towards addressing children’s and young people’s psychological needs, but the evidence base from which to draw is limited (Weare & Nind, 2011; Wolpert, Humphry, Belsky, & Deighton, 2013). Some studies have explored young people’s impressions and found that many would welcome confidential access to mental health support within the school environment (Kidger, Donovan, Biddle, Campbell, & Gunnell, 2009). The most extensive UK project, the Targeted Mental Health in Schools (TaMHS) initiative, highlighted the importance of mental health services working within the school setting to improve management of behavioural difficulties (Wolpert et al., 2013). Many different mental health interventions have been delivered in schools with studies of both universal and targeted interventions, as well as specific treatment modalities such as cognitive behavioural therapy (CBT) (individual and group) to treat disorders including depression, anxiety and post-traumatic stress disorder (PTSD) (Fazel, Hoagwood, et al., 2014; Fazel, Patel, Thomas, & Tol, 2014; Neil & Christensen, 2009; Silverman et al., 2008; Stein et al., 2003; Tyrer & Fazel, 2014).
Schools are likely to be an important location for mental health services to access refugee populations as they potentially carry less stigma than clinic-based services and schools are often better accessed by families than other institutions (Dura-Vila et al., 2013; Hughes, 2014). A systematic review of school and community-based mental health interventions for refugee children noted the breadth of interventions offered in schools for this population (Tyrer & Fazel, 2014). The strongest evidence for effectiveness was for therapies that treated psychological difficulties utilising verbal exposures to previous traumatic events. It was also noted that an emerging evidence base is developing on multimodal interventions where a range of different services are offered to help address the spectrum of needs that young refugees present with.
This study aims to address the absence of data on the actual experience of adolescents directly seen by services by asking those seen by school-based mental health services about their experience of being seen within the school location, how they perceived the therapy, whether or not it helped them and finally about any worries and preoccupations that might be impacting their time at school. The impressions of young refugees seen in three school-based mental health services across the United Kingdom were studied by conducting semi-structured in-depth interviews with those most recently discharged by their respective services.
Method
Sample and recruitment
Three school-based mental health services for refugee children were identified out of nine potential services funded by a charity in partnership with local child mental health services. They were chosen to reflect differences in service design and location: one was embedded within child and adolescent mental health services (CAMHS) from its outset, another was set up privately and then incorporated within CAMHS and the third was set up in a university department of psychiatry with links to CAMHS (Fazel, Doll, & Stein, 2009). They were located in Oxford, England; Glasgow, Scotland; and Cardiff, Wales. Purposive sampling was used to identify the most recent adolescents, aged 16 years and over, consecutively discharged from their service. All those identified could speak sufficient English, but interpreters were needed to talk to parents/carers. Ethical approval for the study was granted by the Oxfordshire Research Ethics Committee and the South East Wales Local research ethics committee.
The mental health worker who had been involved with the identified refugee advised on who would be best placed to introduce the study to the young person, be that either themselves or a teacher at the school (especially if there was an indication of poor engagement with the service). All the schools were formally approached asking permission to contact their students and the identified professional was then asked to approach the specified young person.
When the young person was approached, they were given an information sheet on the project; when the reply slip was returned, the investigator made an appointment to obtain consent from the young person and if under 18, also their parent/carer. For the unaccompanied minors, the consent of the relevant social worker was obtained. The interviews took place at the schools when possible but also at community centres, the local mental healthcare facility or in homes, depending on individual circumstances.
We tried to include 10 young people from each location, but as 8 were recruited in Cardiff, 2 more were identified in Oxford. During the study, a therapeutic group for refugee children came to its planned end in one of the schools and it was decided to interview an additional 10 of the group participants to learn about the group process.
The qualitative interviews followed an in-depth interview approach with a topic guide for areas to be covered (Green & Thorogood, 2004). The focus was on the young person’s experience of the school-based mental health service. Topics covered included their views on the school-based service, its location and impressions of its usefulness, as well as their experience of the asylum application process. The interviews were conducted by M.F. and were audio-recorded and transcribed.
Analysis
Framework analysis was used with a thematic analysis of content in order to identify and categorise recurrent or common themes (Green & Thorogood, 2004). This analysis includes familiarisation with the transcribed interviews, indexing key themes and sub themes, charting, mapping and interpretation. The transcripts were compared to assess similarities and dissimilarities. Framework analysis is commonly used for multi-disciplinary health services research as it provides a systematic and flexible framework for analysing qualitative research (Gale, Heath, Cameron, Rashid, & Redwood, 2013). The process included creating an ‘analytical framework’ of jointly developed codes followed by a reflection on emergent codes with a clustering of interrelated ideas and concepts into ‘categories’. The process of analysis was assisted using MAXQDA 2007 and was conducted in 2008–2009. This helped in indexing the data and developing themes through interrogating the data.
The transcripts were initially read and coded (M.F.). Following this, six transcripts were randomly selected and coded by a second coder (J.G.). The coding schemes were compared and new categories were discussed and added. All the transcripts were then recoded according to the new framework. The main categories which emerged were impressions of being seen by a mental health team in the school setting, understanding and impression of the therapeutic intervention received, contact with family, and impact of the asylum process and ethical issues including confidentiality. The key themes relating to the location of the service, impression of receiving mental healthcare and the impact of the asylum application process are presented below.
Results
Participant recruitment
In total, 51 adolescents and young people were contacted in the three locations. Of these, 11 did not respond, and of those who did respond, 8 did not attend the first appointment but did attend a subsequent appointment. Forty participated in the final interviews: 22 in Oxford, 10 in Glasgow and 8 in Cardiff. Interpreters were needed to meet with two sets of parents. The interviews were conducted in a number of different locations: in the schools (20); hospital clinics (12); homes (5) or social services premises (3). All completed the consent or assent forms and five did not agree to audio recording of their interview. Thirteen of those interviewed were unaccompanied minors. All the interviews were completed on the first meeting with the young person, and none requested or needed to stop the interviews. Basic participant information is included in Table 1.
Basic participant information.
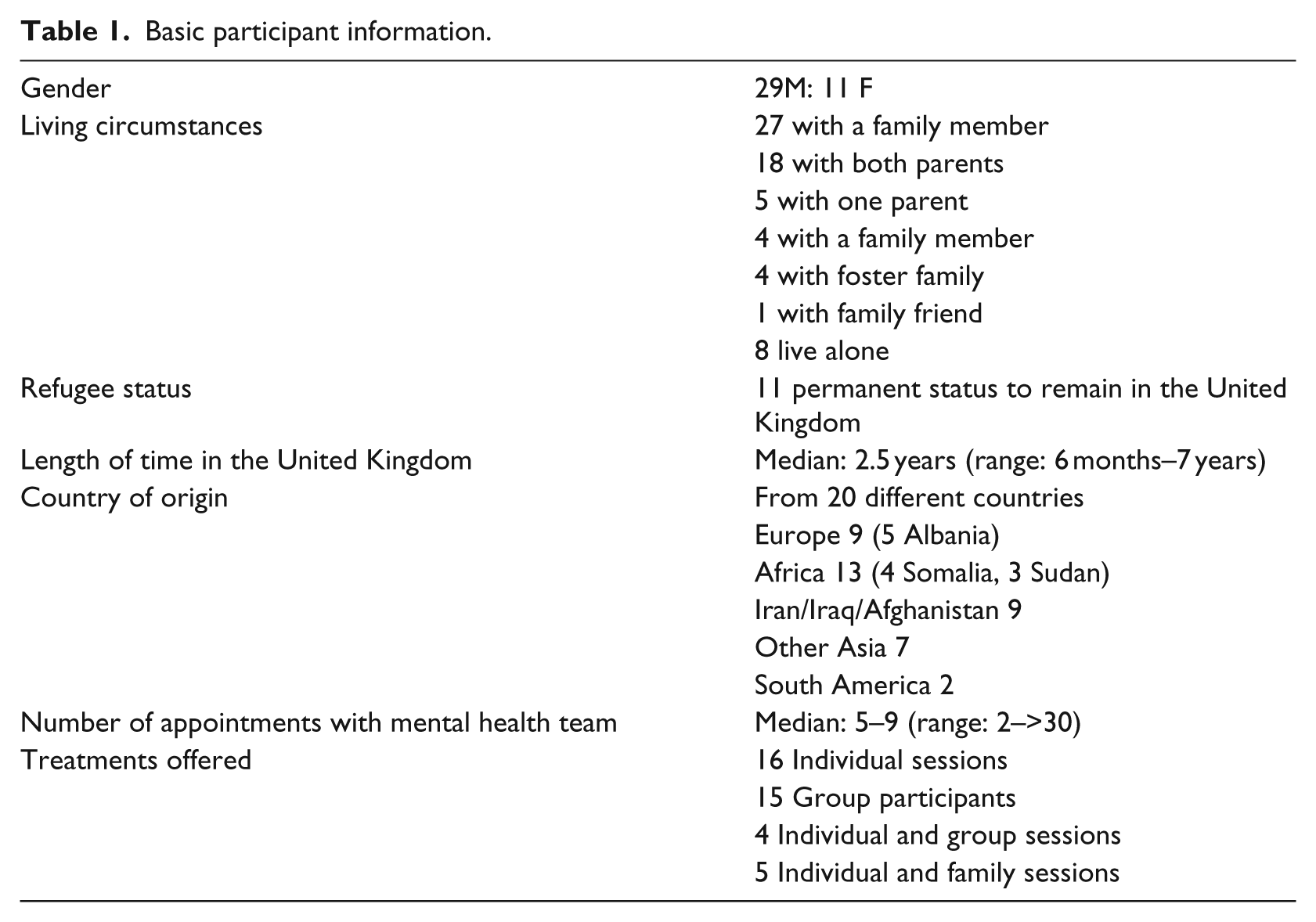
Twenty-nine of those interviewed were male and 11 female. Twenty-seven were living with a family member, eight were living alone, four were in foster families and one was living with a family friend. Eleven had permanent status to remain in the United Kingdom. The median length of time they had been in the United Kingdom was 2.5 years. The participants came from 20 different countries. Their age range was from 15 to 24 years, with a median of 17 years. The intervention they had received was individual (n = 16), group (n = 15) or a combination of individual, group and family work (n = 9). The number of appointments they had attended ranged from 2 to over 30, with the median falling within the 5–9 session range. They had all been discharged from the school-based mental health service within 8 months of their interview. All were still studying, with 26 at school and 14 having moved to various further and higher education establishments.
Impressions of receiving a mental health service in the school location
The majority of young people interviewed stated that they preferred to be seen by the service at school when compared to either their home or the hospital/clinic setting. Of the 38 who answered the question, 27 (two-thirds of the total sample) said school was their preferred location, 9 preferred outside of school and 2 had no preference.
At the core of why many of the respondents preferred the school location was a feeling of safety and familiarity in the school setting. They felt safe at school and it was often easy to find the therapist. In addition, it was convenient as they could easily get back to lessons. As stated in their own words, I don’t know why I just get this sense of feeling free when I’m around this school . . . More at ease. Outside, don’t know who you can trust.
Many preferred the school setting because finding a new location could be difficult and possibly frightening. In particular, many did not like the idea of attending a hospital because of its lack of familiarity both in its setting and of unfamiliar people encountered; confounded by the stigma associated with seeking mental healthcare: I don’t know maybe it would be more complicated or something . . . Maybe just to find it and maybe she doesn’t know who you are, where you come from, . . . I don’t know it’s just different. I think in the school is better. Cos I, I’m not ill. Good to have it in school, if come to hospital it is scary, what are you doing there in the hospital, I don’t know if I would go if it was in a hospital. Yeah no one likes hospitals.
The disadvantages of being seen in the school setting were primarily regarding privacy and not wanting peers to see them and potentially make fun of them or ask questions. Furthermore, school was often perceived as busy and hectic and so appointments outside of school would probably be calmer: Cos in school, there are so many peoples about as well and I wasn’t feel too comfortable. Because I don’t like to come in school.
Role of teachers
Another important difference when delivering mental health services in schools is the opportunity for teachers to play a more active role in referring to and collaborating with services. The young people interviewed described the important role that teachers played in mediating or supporting their contact with the mental health service: When I joined the high school yeah . . . I tell my the teacher . . . I have this problem which can make me not concentrate . . . and she advised me to see X. He [teacher] made me understand, these teachers won’t harm you. They won’t abuse me. Yeah, he wanted to help me. He want to understand me, and when [sic] I’m coming from, he want to know a little bit of me, d’you know I mean. And how is your life . . . You know, he saw me the last two years, you know how I was suffering all the years. And he knew it really deep down what was going on in my life. So, um, the teacher, he made it really easy for me, you know and he find a nice room for us.
Understanding of and impressions of the therapeutic intervention received
Many of the young people described in some detail what they felt actually happened to them during the therapeutic process. They described how having someone to talk to enabled them to get their problems ‘out’ and they no longer felt lonely. They were able to talk about themselves in the sessions but seemed to have mixed feelings about talking about their past experiences. Some wanted to avoid the subject but knew they needed to remember the past in order to then ‘forget it’ and others just thought it would be better not to think about bad past experiences. Of those who felt the need to speak about the past, they often did this in order to ‘unload’ their past experiences which then enabled them to ‘feel free inside’ or ‘calm down’: I don’t know, I think it was just like a tumour . . . and she was operating and she took away the tumour.
Table 2 shows how the young people thought that therapy had helped them. All 40 respondents answered this question and some stated they had been helped in more than one arena.
How therapeutic intervention helped the individuals seen.
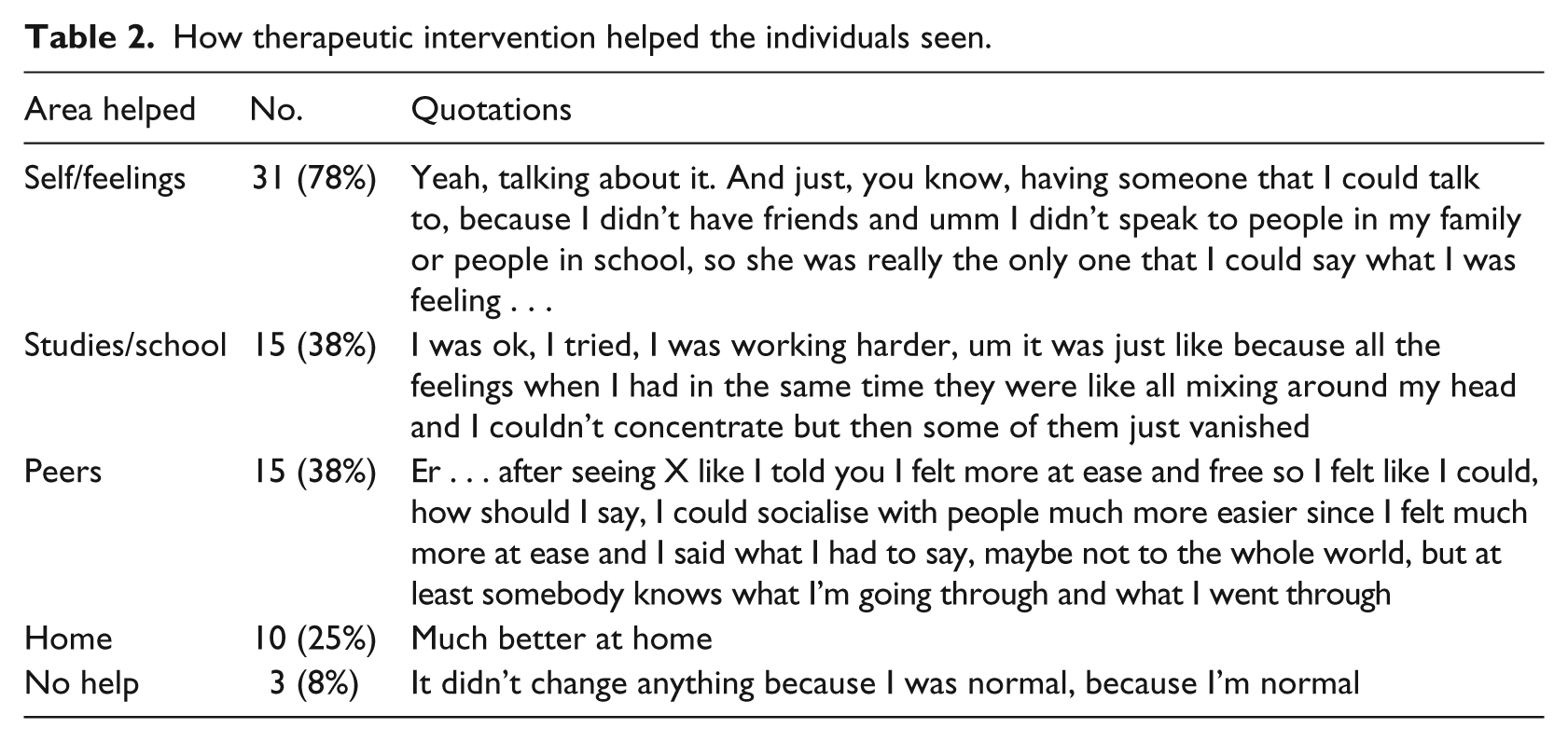
The majority had found the intervention helpful for themselves and their feelings. They felt less worried about things, more confident and grateful for explanations about some rules in society and how to talk to others. They often said they felt more relaxed as a result, and this had an effect on many other aspects of their lives. Many seemed to appreciate certain techniques they were taught in order to help them relax, for example, breathing exercises, writing feelings down, counting to 10, going out to see a friend or talking to another person.
Equal numbers of young people said that they were helped in their studies/at school and with their peers. For those finding benefit at school, most of this was from an improved ability to concentrate and feeling calmer in themselves and so therefore more able to focus on the school work (see quotations in Table 2). The therapeutic intervention helped with peer relationships in a number of ways. It opened the door to start talking to friends, especially for those who attended therapeutic groups where the main friendship benefits were with other members of the group. In general, many said that feeling calmer and better in themselves had helped them to get on better with friends.
As the majority of the time the therapeutic services were working from a school base, the young people were asked about whether they had missed school lessons in order to attend appointments and their thoughts about this. Most had had to miss the occasional lesson, but the majority of appointments were made in free periods, break times and after school. Some students did not want to miss any lessons, but the majority were happy to miss a few, especially in subjects they did not enjoy. In addition, some thought that the therapeutic sessions were so important that it was worth missing lessons in order to attend them.
Impact of the asylum application process
The asylum process was a prominent theme in many of the interviews. Of the 40 young people seen, only 11 had permanent status to remain in the United Kingdom, all of whom were living with a family member. The remaining 29 had undetermined status, the majority of them were awaiting an initial decision (21), five had temporary status until their 18th birthday and three had had an asylum appeal rejected and were unsure what would happen next.
In describing their experience of being an asylum seeker or refugee, the young people discussed their past experiences, their concerns about other people’s perceptions of their status, the impact of the asylum applications on them personally, how their therapist had helped with their asylum application and pre- and post-displacement stressors. One of those interviewed had been detained in an immigration detention centre.
The difficulties of living with undetermined immigration status were described by all in negative terms, especially with regard to their mental health. None had any idea as to how long they would be waiting, and those who had status until the age of 18 years were all anxious and worried as to what might happen to them after this birthday:
I’ve been here nearly five years
Five years and do you have status?
No I’m still waiting
I got three years, erm.. Temporary, yeah.
And then what happens?
I mean, they might, might extend it or just, I just go back.
Their descriptions of how the insecurity made them feel highlighted the constant preoccupation this issue held for many. They reported always being conscious of the asylum application, that it made it difficult for them to concentrate on their school studies and that in general they felt less able to cope with problems. They were unable to attend university, apply for a job or open a bank account without permanent status to stay, and at times, this caused them to feel ‘guilty’ that they had come to the wrong place. Some described fear whenever a letter arrived as they might be receiving notice of a negative application decision. Many felt very alone in the asylum process and one young person described how his initial interview with the immigration authorities had been conducted on his arrival when he did not understand what was happening. At the time, he had felt unable to describe his past traumatic experiences and he had felt under pressure to sign his interview statement. He had then felt powerless in the subsequent court hearing as he had not been asked any direct questions, only his statement had been read. Both his initial immigration decision and appeal had been rejected: You know most of them for example, don’t know their position to remain in this country and it’s very difficult to study. I think when I came here I was 15, two years, 17 now, that’s why I’ve got this leave to remain in this country until 18 but I don’t know what’s happen after that. But after 18 that’s why and then I am thinking about the decision I can’t study, I’m not in school, I don’t want to leave school or something like that, it’s difficult . . . it makes me crazy We’ve settled down here, we’ve gotten used to the people, we’ve worked hard, when we see the other people got um, status and um, freedom of life, you know, we feel they’ve been accepted, d’you know I mean, but you, you haven’t been accepted, just been waiting and waiting and waiting. There is something wrong with you or, you know within society. Stop them thinking about being deported. Because all of, all the people in school, go ask anyone you like, they will be scared of being deported . . . Yeah. They think they are next. And so how does that change the way they behave or act? They will lose concentration on school subjects, secondly they won’t be themselves. I know this girl and like that day my friend got deported she was just frozen, she did not speak to nobody and I don’t know what happened, . . . They walk around like a ghost. They are just totally miserable and you cannot talk to them, unless you talk about something else. Yeah you cannot go to somebody. ‘this is going to be alright’, ‘you’re not going to be deported’, I didn’t even mention ‘D’ in the sentences I was using.
Pre- or post-displacement stressors
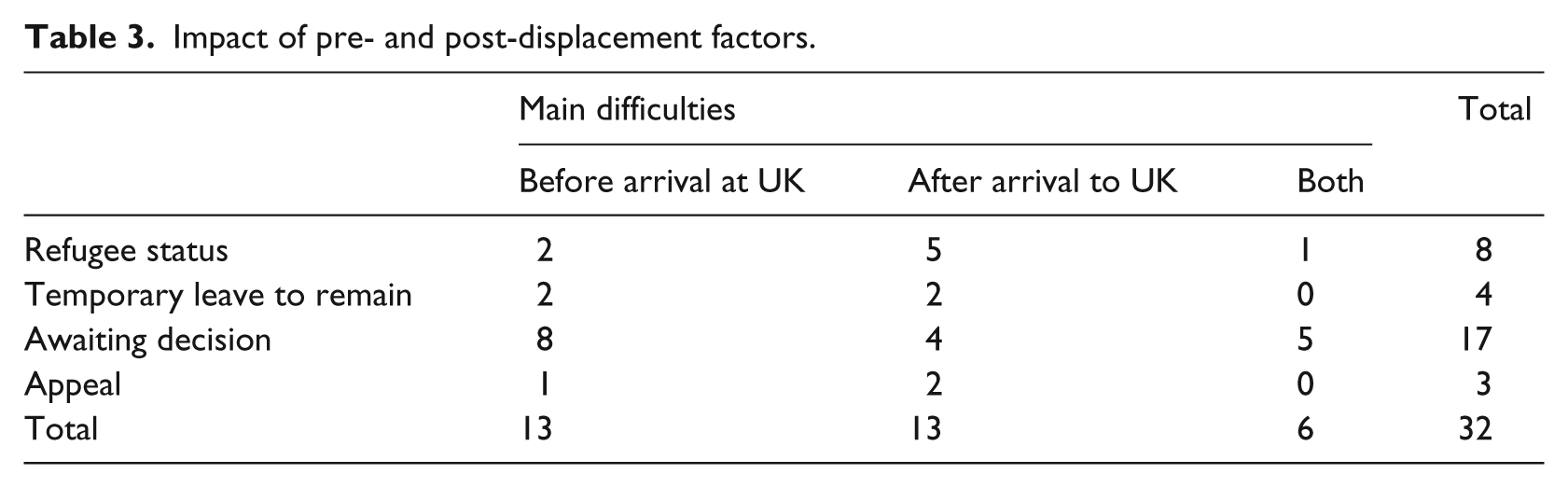
As demonstrated in Table 3, of the 32 young people who answered whether the majority of their problems were because of pre- or post-displacement factors, the results are shared evenly between both categories. Thirteen answered that their main problems were before arrival and the same number after arrival, with six stating that both had contributed to their mental health problems. These were distributed across all immigration statuses.
Impact of pre- and post-displacement factors.
Discussion
The importance of understanding the impact of interventions in real-world settings and the opportunity provided by schools to work in an integrated manner with vulnerable populations are questions which we aimed to address in this study. The qualitative interviews with 40 refugees and asylum seekers who had been seen by the school-based mental health service suggest that most students preferred to be seen within the school environment by mental health services. They had a realistic understanding of why they had been referred to the service and felt that their problems had been helped. Many were reluctant to initially engage and had found the support of a referring teacher valuable. They reported that the main use of the therapy was to help them solve problems, and many doubted the need to delve into their past experiences. Pre-migration and post-migration stressors were identified by the young people as affecting their well-being to an equal extent. This raises the importance of addressing post-migration factors, as they seem to be playing a negative role in the lives of the young people. Insecurity emerged as a prominent post-migration experience. The insecurities were predominantly regarding their asylum status but also because of bullying, racism and negative media stereotyping of asylum seekers which impeded attempts to connect with their schools and communities (Fazel, 2015). The majority were constantly preoccupied by concerns about the outcome of their asylum application, making it difficult to concentrate at school, engage in everyday activities or plan their future.
The potential role that schools can play is therefore important to consider. The young people thought that, in most aspects, schools were a good location for mental health services to work from; they felt safe and convenient for the students. There were concerns raised about privacy and trust in the school setting, but these concerns were outweighed by the positive impressions of working in the school environment.
The valuable role teachers played in supporting and mediating contact with the mental health team was important, especially when considering that many of these young people have no immediate family, as families commonly assist young people to approach mental health services (Ryan, Jorm, Toumbourou, & Lubman, 2015). The role of teachers can therefore be especially important as some data suggest young people find it difficult to discuss personal matters with a ‘stranger’, thereby inhibiting their professional help-seeking behaviours (Rickwood, Deane, Wilson, & Ciarrochi, 2005). This suggests that efforts to increase young people’s use of mental health services may benefit from strategies also aimed at developing trusting and supportive professional relationships between schools and other organisations and institutions. For example, teachers could potentially better help young people access services if good relationships with local services exist with clear referral routes. Mental health services can offer support to schools and teachers through a range of different services including improved channels of communication, offering supervision to the school’s pastoral care system, providing mental health services on the school site and enabling easier access and referral to services elsewhere (Fazel, Hoagwood, et al., 2014; Wolpert et al., 2013).
Although some adolescents were managing, many ruminated and worried about the asylum process and the unresolved and insecure aspects of their future. This is important because of the strong evidence that rumination and worry interfere with everyday social and cognitive functioning such as problem solving (Watkins, 2008), and so supporting young people and giving them strategies to manage their concerns about their asylum application would be important.
Clinical implications
There are a number of potential clinical implications to consider. These include two areas of note: the location of services and what the mental health services can offer in support to teachers and students.
The location of the service, being school-based, is an important factor to consider as so many of the young people welcomed being seen at school. This was mainly because they felt safe at school. Compared to formal institutions outside of school, the school was familiar and unthreatening as well as convenient. They did not mind missing the occasional lesson and particularly valued private rooms away from the main school areas. Many of the students recognised their therapist from their presence in the school and, if needed, would on occasion ask their therapist at school for assistance outside of their specific appointments – facilitated by the context and familiarity with the therapist. Furthermore, as attendance at school is mandatory and schools are located throughout rural and urban areas, making services accessible through schools democratises access to services and helps address children’s educational, emotional and behavioural needs in a coordinated and integrated manner (Fazel, Hoagwood, et al., 2014; Little & Akin-Little, 2013).
Mental health services can support the role of teachers in the school setting, by working together to better understand the presentations of the children of concern in the classroom. Teachers spend more time than most other professionals with these children and so are well placed to observe any behaviours of concern. Many of the young people interviewed described difficulties in concentration, fighting with peers and family members or just a change in their usual mood when the mental health service became involved in their care.
Limitations of the study
This study involved only 40 respondents at three of nine possible centres. The sample was specifically selected to represent a broad range of experiences of services rather than be representative of all refugee adolescents. The rigour of the findings could have been strengthened if more than one method of data collection had been utilised, for example, by conducting a focus group, and if some cross-checking of the interim research findings had been made with respondents. In addition, further valuable and complementary information could have been gathered from interviews with teachers and parents or carers. Although the study used purposive sampling, it was not possible to interview all those identified as some did not come for interview. The small group who did not attend might have had different and possibly more negative experiences of the service. It is also unknown how many refused initial access to the school-based service as they might be a group who might want to access mental health services but not within their schools. The data have not been investigated for gender differences, differences in unaccompanied minors compared to those who had arrived with their families or for the different locations because of the relatively small numbers. Of note, the study interviewed participants from 20 different countries focusing on the general experience of the service, its delivery and how it might be improved. The study tried to capture the reality of schools with heterogeneous groups of children arriving, and so all young people were interviewed. There are, however, significant cultural differences to appreciate when interviewing young people coming from so many different societies and cultures. The data have not been explored for cultural differences in attitudes and approaches to healthcare; however, it would be essential to note that such an analysis could provide important information on how best to reach specific minority groups. These limitations open up new horizons for future research and further qualitative work can ensure the perspectives of refugee adolescents are appreciated and incorporated in many aspects of planning for optimal mental healthcare provision.
Conclusion
The opportunity to provide mental health services within the school can potentially support children not only in their academic pursuits but also in their overall sense of well-being, belonging in the school and for refugee children, inclusion in a new host country (Fazel, Reed, Panter-Brick, & Stein, 2012; Kia-Keating & Ellis, 2007; Murray, Low, Hollis, Cross, & Davis, 2007; Taylor & Sidhu, 2012). The findings from this study highlight that many adolescent refugees preferred accessing mental health services within their schools than elsewhere. There are some advantages to locating mental health services in schools. Most adolescents attend schools and are generally there; there can be contact with teachers who observe students in a number of structured and unstructured settings and can, with consent, provide information that is complementary to parents or other substitute carers. Furthermore, in the absence of parents, teachers can provide crucial information on the mental state of a young person. Many are preoccupied with their insecure asylum status and the school has the potential to provide a safe space for them. Furthermore, these findings are potentially of relevance for all children receiving mental health services within school settings.
With the rates of global forced displacement reaching unprecedented levels (United Nations High Commissioner for Refugees (UNHCR), 2015), it is important to understand how best to support the mental health of refugee children and adolescents arriving in high-, middle- and low-income countries. Across the world, schools are providing a system of care to young people while access to mental health services is likely to be limited, particularly in low- and middle-income countries (Cortina et al., 2008; Patel, 2013). The mental health trajectories of refugee children are diverse, and although some are likely to suffer significant mental health problems, others demonstrate high social and academic functioning and psychological resilience (Ellis, 2011). It is therefore important to focus on strategies that can be utilised to promote positive outcomes in these children and understand the perspective of young refugees as well as the locations where they might best access services.
Footnotes
Acknowledgements
We thank the students who generously agreed to be interviewed and the schools, teachers and mental health services who assisted in contacting the students and providing facilities for the interviews to be conducted.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by Oxford University Medical Research Fund (MRF/1642).