
Abstract
Background:
The assessment of children and young people with history of complex developmental trauma presents a significant challenge to services. Traditional diagnostic categories such as post-traumatic stress disorder (PTSD) are argued to be of limited value, and while the proposed ‘Developmental Trauma Disorder’ definition attempts to address this debate, associated assessment tools have yet to be developed. This review builds on a previous review of assessment measures, undertaken in 2005.
Aim:
To identify trauma assessment tools developed or evaluated since 2004 and determine which are developmentally appropriate for children or adolescents with histories of complex trauma.
Method:
A systematic search of electronic databases was conducted with explicit inclusion and exclusion criteria.
Results:
A total of 35 papers were identified evaluating 29 measures assessing general functioning and mental health (N = 10), PTSD (N = 7) and trauma symptomatology outside, or in addition to, PTSD (N = 11). Studies were evaluated on sample quality, trauma/adversity type, as well as demographic and psychometric data. Distinction was made between measures validated for children (0–12 years) and adolescents (12–18 years).
Conclusion:
Few instruments could be recommended for immediate use as many required further validation. The Assessment Checklist questionnaires, designed with a developmental and attachment focus, were the most promising tools.
Introduction
Substantial numbers of children experience adversity in the form of abuse, neglect and maltreatment (Radford et al., 2011). The impact of childhood adversity can be extensive (for review, see D’Andrea, Ford, Stolbach, Spinazzola, & van der Kolk, 2012), and these children often present with varied emotional and behavioural difficulties frequently prompting multiple co-morbid diagnoses from professionals (Ackerman, Newton, McPherson, Jones, & Dykman, 1998; Spinazzola et al., 2005). Current diagnostic constructs have been criticised for failing to provide adequate conceptualisation of these children’s difficulties (van der Kolk, 2005), while popular standardised measures may have limited scope to capture the pervasive and complex range of difficulties displayed by this population (Achenbach, Dumenci, & Rescorla, 2003; Tarren-Sweeney, 2013a). These issues complicate the challenge of undertaking meaningful assessment of children and young people exposed to multiple traumatic experiences during early development (Tomlinson & Philpot, 2008).
A diagnosis of developmental trauma
The traditional psychiatric label given to pathological distress following a traumatic event is post-traumatic stress disorder (PTSD). The Diagnostic and Statistical Manual of Mental Disorders–Fifth Edition (DSM-V; American Psychiatric Association (APA), 2013) defines a traumatic event as exposure to actual (or threatened) death, serious injury or sexual violation and is largely conceptualised as contained within a single incident (Davidson, Hughes, Blazer, & George, 1991). This fails to capture that child victims of physical, sexual and emotional abuse, or indirect witnesses of domestic violence, often experience multiple forms of abuse on frequent occasions (Cook et al., 2005; DeJong, 2010; Dong et al., 2004; Finklehor, Turner, Ormrod, & Hamby, 2009; Streeck-Fischer & van der Kolk, 2000). Moreover, high proportions of children reporting multiple abuse do not meet the criteria for PTSD in childhood (Pynoos et al., 2008 as cited in van der Kolk et al., 2009; Spinazzola et al., 2005) and experience difficulties in adulthood which exceed PTSD criteria such as affect regulation, memory, attention, self-perception, interpersonal relationships, somatisation and systems of meaning (Roth, Newman, Pelovitz, van der Kolk, & Mandel, 1997; van der Kolk et al., 1996).
To address these issues, van der Kolk (2005) proposed a new diagnostic classification called ‘Developmental Trauma Disorder’ (DTD). DTD captures the multiple or ongoing exposure to interpersonal violence and disruptions in protective caregiving (van der Kolk et al., 2009) within a framework of developmental change and disrupted attachment, a position supported by biological and neurological research (Glaser, 2000). Therefore, behaviours which would have previously been given separate ‘co-morbid’ diagnostic labels are understood to be a complex, disorganised, but interrelated pattern of symptoms (D’Andrea et al., 2012; Praver, DiGuiseppe, Pelcovitz, Mandel, Gaines, 2000). Cook et al. (2005) proposed a similar diagnosis but labelled it ‘Complex Trauma’. Children with Complex Trauma also meet the criteria for DTD in addition to responding to every novel experience as a potential threat (Cook et al., 2005). Complex Trauma and DTD have similarities in their defined domains of difficulty (for a comprehensive discussion of both constructs, see Strickler, 2011). As we feel the DTD terminology best captures the dynamic developmental context of the traumatic experiences of children and adolescents, this review will utilise the phrase ‘developmental trauma’ to define multiple or chronic exposure to interpersonal violence, emotional abuse, sexual abuse and impaired caregiving in childhood or adolescence. Nonetheless, it is important to note that some children will not reach these criteria and thus formulation remains an important alternative to diagnosis. Clinical formulation integrates the child’s symptoms and context in order to provide a shared understanding of the child and a framework for developing the most suitable interventions.
Assessing children and adolescents with developmental trauma
Studies suggest that children with histories of developmental trauma are given co-morbid diagnoses (Spinazzola et al., 2005), meet sub-threshold levels for a range of disorders (DeJong, 2010) or display an array of behaviours outside of diagnostic categories, for example, faecal smearing, sexualised behaviour and food hoarding (Iwaniec, 2006). Children with complex trauma histories commonly meet the criteria for a number of internalising and externalising DSM-IV disorders (Ackerman et al., 1998). For example, in one study, up to 40% of these children had at least one other co-morbid mood, anxiety or disruptive behaviour disorder diagnosis in addition to symptoms of PTSD (Copeland, Keeler, Angold, & Costello, 2007).
Although children who have experienced childhood or adolescent trauma require a comprehensive, broad and accurate formulation of their difficulties, there are often contextual factors which impede this process. They are frequently placed in local authority care where their foster carers have limited knowledge of the child at the point of assessment – a problem particularly on measures which require symptom ratings for the preceding 6 months (e.g. Child Behaviour Checklist (CBCL); Achenbach, 1991). While younger children can struggle to articulate their internal emotional experience using verbal expression (van der Kolk, 2005), older children can experience high levels of shame and distress (Hughes, 1998) and may be reluctant to complete the measures. Finally, the DTD debate is relatively new, and as such standardised assessment measures have yet to be developed. Measures commonly utilised have a theoretical basis with the PTSD literature (Hawkins & Radcliffe, 2006) or cover broad psychopathological perspectives such as the CBCL or the Strengths and Difficulties Questionnaire (SDQ; Goodman, 1999); neither of which were designed for a traumatised population.
Purpose and aims of this review
A recent review by Strand, Sarmiento, and Pasquale (2005) discussed the practical properties of screening and assessment tools for trauma. The review failed to consider age-specific tools and combined symptomatic and abuse screening tools. Therefore, the purpose of this review was twofold: (1) identify trauma assessment measures developed or evaluated since 2004 and (2) determine which measures are developmentally appropriate for children and adolescent populations who have suffered developmental trauma.
Method
Search strategy
The following electronic bibliographic databases were searched: MEDLINE, PsycINFO, PsycARTICLES, Psychology, Behavioural Sciences Collection, PsycBOOKS and Web of Science. All searches were restricted to work published in English between January 2004 and May 2015. The following search terms were used: (measure* OR questionnaire OR checklist OR instrument OR self-report OR observation) OR (assessment AND validity OR reliability OR standardisation OR comparison OR evaluate AND (abuse OR neglect OR maltreatment OR complex trauma OR developmental trauma OR adversity OR PTSD OR post traumatic*) AND (child OR children OR adolescent OR juvenile OR welfare OR looked after). Searches were also undertaken for the symptomatic measures listed in Strand et al.’s (2005) review.
Inclusion criteria
Studies included in the review evaluated the psychometric properties of assessment measures in participants:
Aged 0–18 years;
Exposed to multiple traumas including sexual, physical and emotional abuse, witnessing or experiencing domestic violence, and neglect.
Exclusion criteria
Studies excluded from the review evaluated:
Adults (18 years or above);
Retrospective instruments of childhood trauma;
Measures screening for traumatic experiences;
Participants only with experiences of single-event trauma such as road traffic accident;
The use, but not evaluation, of assessment measures;
Papers published before January 2004;
Cross-cultural validation of questionnaires or measures outside of the United Kingdom, United States, Canada, Australia and Europe.
Quality assessment
The papers were evaluated against a range of criteria including psychometric rigour, sample demographics, trauma/adversity demographics and the clinical utility of the tool for the assessment of children and young people with a history of developmental trauma.
Results
A total of 2273 papers focussed on children aged 0–11 years, and 1997 papers focussed on young people aged 12–18 years were identified. After screening, 35 papers evaluating 29 measures met the inclusion/exclusion criteria. Demographic information (Tables 1, 3 and 5) and quality of the measures (Tables 2, 4 and 6) are presented in tabular form. The measures are summarised in three categories: (1) general functioning and mental health, (2) measures of PTSD and (3) measures of trauma symptomology outside, or in addition to, PTSD diagnostic criteria, each of which will be discussed in turn. Distinction is made between measures validated for children (0–11 years), adolescents (12–18 years), or across the whole age range. Information regarding studies’ sample size and gender can be found in Tables 1, 3 and 5 and will not be discussed within the text of the review.
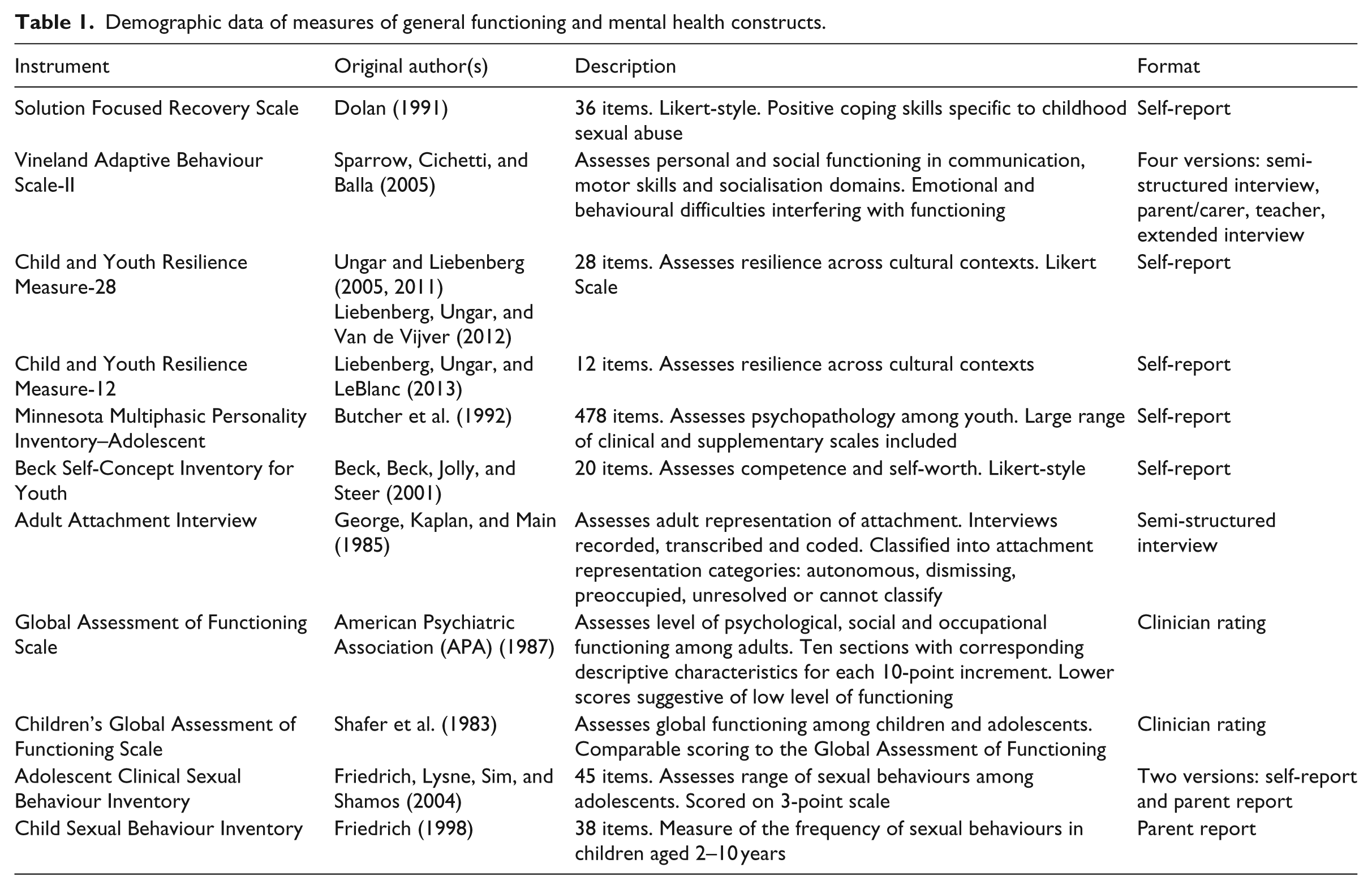
Demographic data of measures of general functioning and mental health constructs.
General functioning and mental health
Ten measures were identified for the assessment of general functioning and mental health (Tables 1 and 2). Of these, one measure (Child Sexual Behaviour Inventory (CSBI); Baker et al., 2008) was validated for use with children, six (Solution Focused Recovery Scale (SFRS; Kruczek & Ægisdóttir, 2005), Child and Youth Resilience Measures (CYRM-28; Liebenberg, Ungar, & LeBlanc, 2013; CYRM-12; Liebenberg, Ungar, & Van de Vijver, 2012), Minnesota Multiphasic Personality Inventory–Adolescent (MMPI-A; Murray, Glaser, & Calhoun, 2013), Adult Attachment Interview (AAI; Bailey, Moran, & Pederson, 2007; Madigan, Vaillancourt, McKibbon, & Benoit, 2012), Adolescent Clinical Sexual Behaviour Inventory (ACSBI; Friedrich, Lysne, Sim, & Shamos, 2004; Wherry, Berres, Sim, & Friedrich, 2009), Beck Self Concept Inventory for Youth (BYI-S; Runyon, Steer, & Deblingerm, 2009) were validated for use with adolescents and three were validated for both age groups (Global Assessment of Functioning (GAF; Blake, Cangelosi, Johnson-Brooks, & Belcher, 2007), Children’s Global Assessment Scales (CGAS; Blake et al., 2007) and Vineland-II (Becker-Weidman, 2009)).
Quality data of the measure of general functioning and mental health constructs.
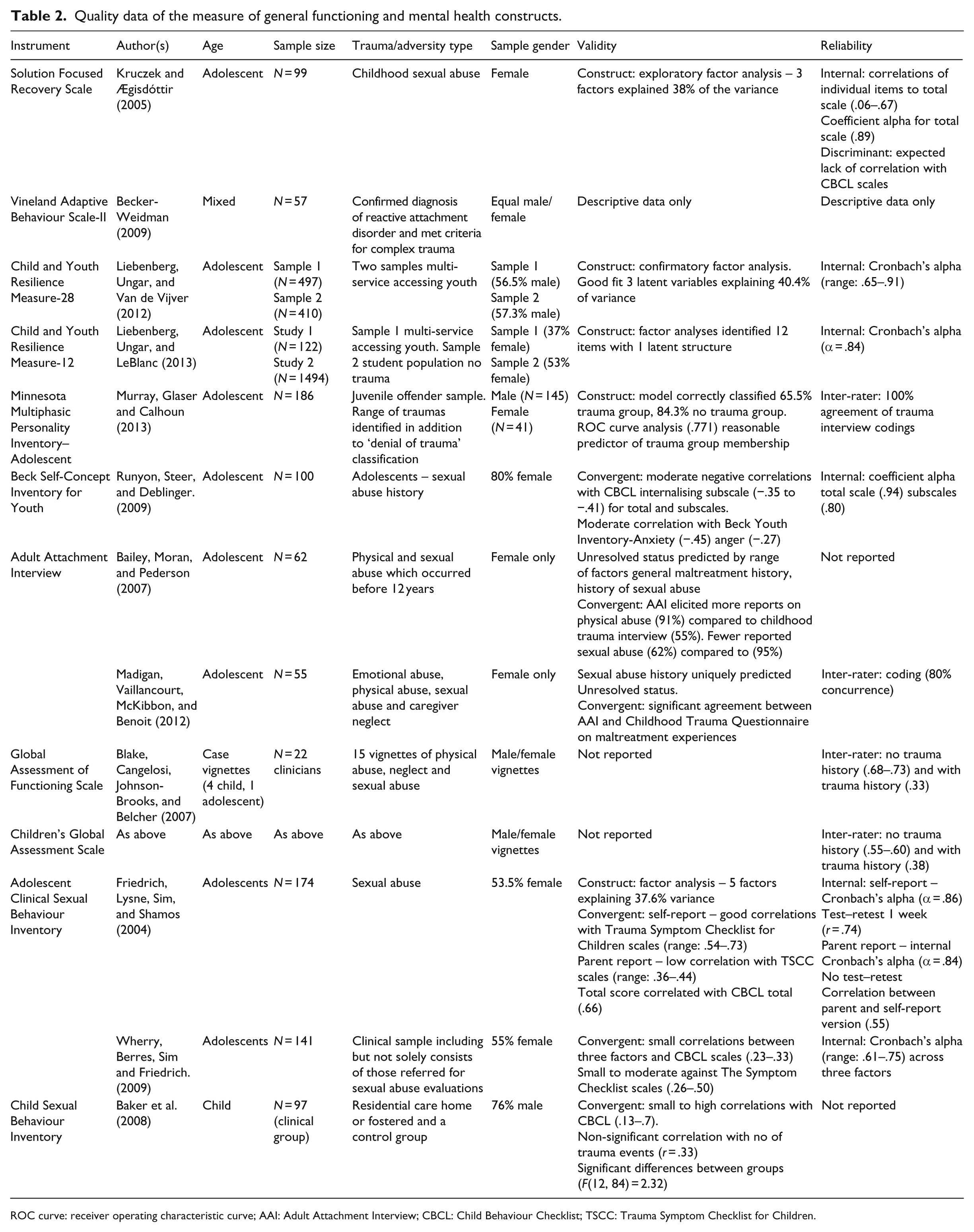
ROC curve: receiver operating characteristic curve; AAI: Adult Attachment Interview; CBCL: Child Behaviour Checklist; TSCC: Trauma Symptom Checklist for Children.
Sample quality
Sample age
The majority of measures were validated against adolescent samples (i.e. participants aged more than 12 years) with the exception of the CSBI (Baker et al., 2008) which was validated against a looked after children (LAC) sample and a control group aged between 10 and 12 years, thus limiting its generalisability to children of other ages. Blake et al. (2007) investigated the GAF and CGAS using a variety of vignettes, but only one of the child trauma case vignettes featured a child over 12 years.
Trauma/adversity type
Demographic information about the adversity experiences of participants was limited across all studies. Predominantly measures were evaluated using participants who had childhood sexual abuse experiences, for example, the CSBI (Baker et al., 2008). Most authors failed to document the severity of exposure to trauma and whether other forms of abuse had occurred. For example, the ACSBI (Friedrich et al., 2004) was evaluated with participants who had been referred for sexual abuse evaluations. Less than half of the sample (24.1%) reported unwanted sexual experiences, but these were not defined in terms of type, frequency or age at occurrence. While Runyon et al. (2009) did provide sufficient demographic information about the sexual abuse experiences of participants in their evaluation of the BYI-S, they did not report whether the sample had other abuse or adversity experiences which could have confounded their results.
Other studies mixed participants with single- and multiple-incident traumas. The AAI studies (Bailey et al., 2007; Madigan et al., 2012) utilised samples with mixed trauma experiences, some of which did not reflect developmental trauma. For example, Madigan et al. reported higher numbers of single-incident non-caregiver perpetrated sexual abuse among their participants. The CYRM study samples included ‘multiple-service-using-youth’ supported by a range of mental health, child welfare and education services (Liebenberg et al., 2013; Liebenberg et al., 2012). A proportion of the sample included participants with experiences of single-incident trauma, but the lack of demographic data makes it difficult to determine whether participants would fit the DTD definition. Given that the CYRM measures were not designed for a developmental trauma population, they are unlikely to be valuable for clinical assessment.
Three studies attempted to account for developmental trauma in their sampling with arguably limited success. While Murray et al. (2013) acknowledged that the effects of developmental trauma may extend beyond the traditional PTSD diagnoses, the MMPI-A was only validated with a specific population (Juvenile Offenders). Baker et al.’s (2008) evaluation of the CSBI utilised a sample of LAC who likely experienced multiple trauma histories. Becker-Weidman (2009) was one of few authors to acknowledge the current literature on complex trauma, suggesting that subscales of the Vineland-II map onto some domains of the complex trauma diagnosis (Cook et al., 2005). Becker-Weidman’s sample met the diagnostic criteria for both reactive attachment disorder and complex trauma and thus may be most representative of children and young people with a history of developmental trauma.
Reliability and validity
The majority of measures evidenced good reliability in the form of alpha coefficient ratings for the entire scale and the within-scale factors (Table 2); however, there were a notable number of validity and utility limitations in all studies.
Many studies utilised the CBCL (Achenbach, 1991) to assess discriminant validity. At times this failed to provide adequate evidence of validity where positive associations were not identified (e.g. SFRS; Kruczek & Ægisdóttir, 2005). The low or absent correlations between the CBCL (parent report) and the SFRS (self-report) may have been confounded by the low correlation sometimes reported between parent and adolescent reports of behaviour and emotional distress (Seiffge-Krenke & Kollmar, 1998). The SFRS seemingly has poor face validity, for example, the Social Engagement factor included uniquely loading items such as ‘Sleep OK’ (Item 3) and ‘Stand up for myself’ (Item 5). These are not social engagement behaviours and did not correlate with Self Care and Interpersonal Assertion, respectively, as one would expect. Neither measures of the CYRM were examined for discriminant validity during development (Liebenberg et al., 2013; Liebenberg et al., 2012), and the Vineland-II study (Becker-Weidman, 2009) was limited by being purely descriptive (only mean values and standard deviations were reported).
Other studies lacked sensitivity, for example, Murray et al.’s (2013) MMPI-A model made more accurate classifications for the no-trauma history cases than trauma history cases. The CBCL (Achenbach, 1991) was unable to identify 41% of children who met the criteria for problematic sexual behaviours according to the CSBI (Baker et al., 2008). Meanwhile, the BYI-S showed promise for identifying levels of self-esteem among adolescents with a history of sexual abuse (Runyon et al., 2009). Out of the 90% of participants who scored below average self-esteem, 53 had scores classified as ‘lower than average’ and 37 had scores classified as ‘much lower than average’. This suggests that the BYI-S is sensitive enough to discriminate qualitative differences in self-esteem among a sample with primarily below average scores.
The factor structure of the ACSBI has been questioned after studies reported differing results of either five- or three-factor structures (Friedrich et al., 2004; Wherry, Berres et al., 2009, respectively). Wherry, Berres et al. (2009) argued this was due to their sample not including participants referred for sexual abuse evaluations; however, both studies investigated the ACSBI with a mixed sample of adolescents with or without sexual abuse histories, all of whom were being treated for psychiatric difficulties. The actual reason for the variation in factor structure arguably remains unclear.
The AAI studies raised questions about the measure’s utility. Both studies reported that without probe questions, reports of abuse were low and thus prevented an assessment of ‘Unresolved status’ (Bailey et al., 2007; Madigan et al., 2012). The AAI reflects a move away from traditional diagnostic classification systems to broader concepts, such as attachment status, which may be more useful in future conceptualisations of developmental trauma.
Conclusion – general functioning and mental health
The majority of measures of general functioning provided inadequate demographic information in relation to participants’ experiences of adversity, thereby limiting the conclusions that can be drawn about their utility with a DTD population. The MMPI-A and Vineland-II studies made reference to complex trauma and the CSBI utilised a LAC sample; however, the studies were limited by factors such as the use of specific populations, simple descriptive data and restricted age ranges. The BYI-S appeared good at distinguishing between qualitative differences in low self-esteem but was marred by utilising a female-only sample about whom there was limited information about concurrent abuse experiences. As such these measures require further evaluation with greater demographic information before they can be recommended for use with the developmental trauma populations.
PTSD
Seven measures were identified for assessment based on PTSD diagnostic criteria (Tables 3 and 4). Of these measures, three were validated for use with children (two versions of the CBCL-PTSD subscale (Dehon & Scheeringa, 2006; Loeb, Stettler, Gavila, Stein, & Chinitz, 2011), and Child Dissociative Checklist (CDC; Wherry, Neil, & Taylor, 2009), one for use with adolescents (Adolescent Dissociative Experiences Scale (ADES; Keck Seeley, Perosa, & Perosa, 2004)) and three were developed or validated for use across the age range (a third version of the CBCL-PTSD (Rosner, Arnold, Groh, & Hagl, 2012; Sim et al., 2005), the University of Los Angeles–Post-Traumatic Stress Disorder–Reaction Index (UCLA-PTSD-RI; Elhai et al., 2013; Steinberg et al., 2013) and Child PTSD Symptom Checklist (CPSC; Milot et al., 2013)).
Demographic data for measures of post-traumatic stress disorder.
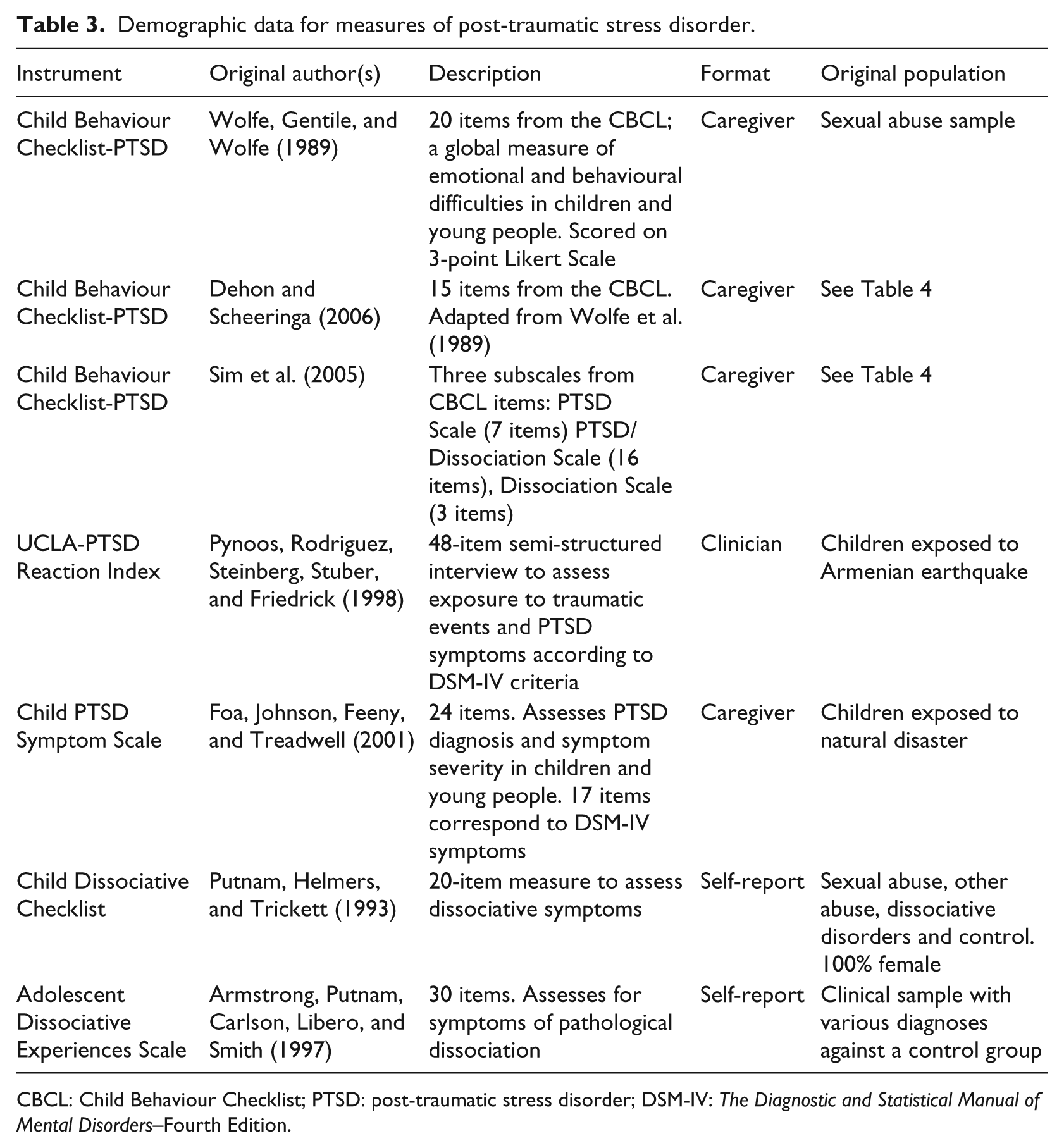
CBCL: Child Behaviour Checklist; PTSD: post-traumatic stress disorder; DSM-IV: The Diagnostic and Statistical Manual of Mental Disorders–Fourth Edition.
Quality information for measures of PTSD.
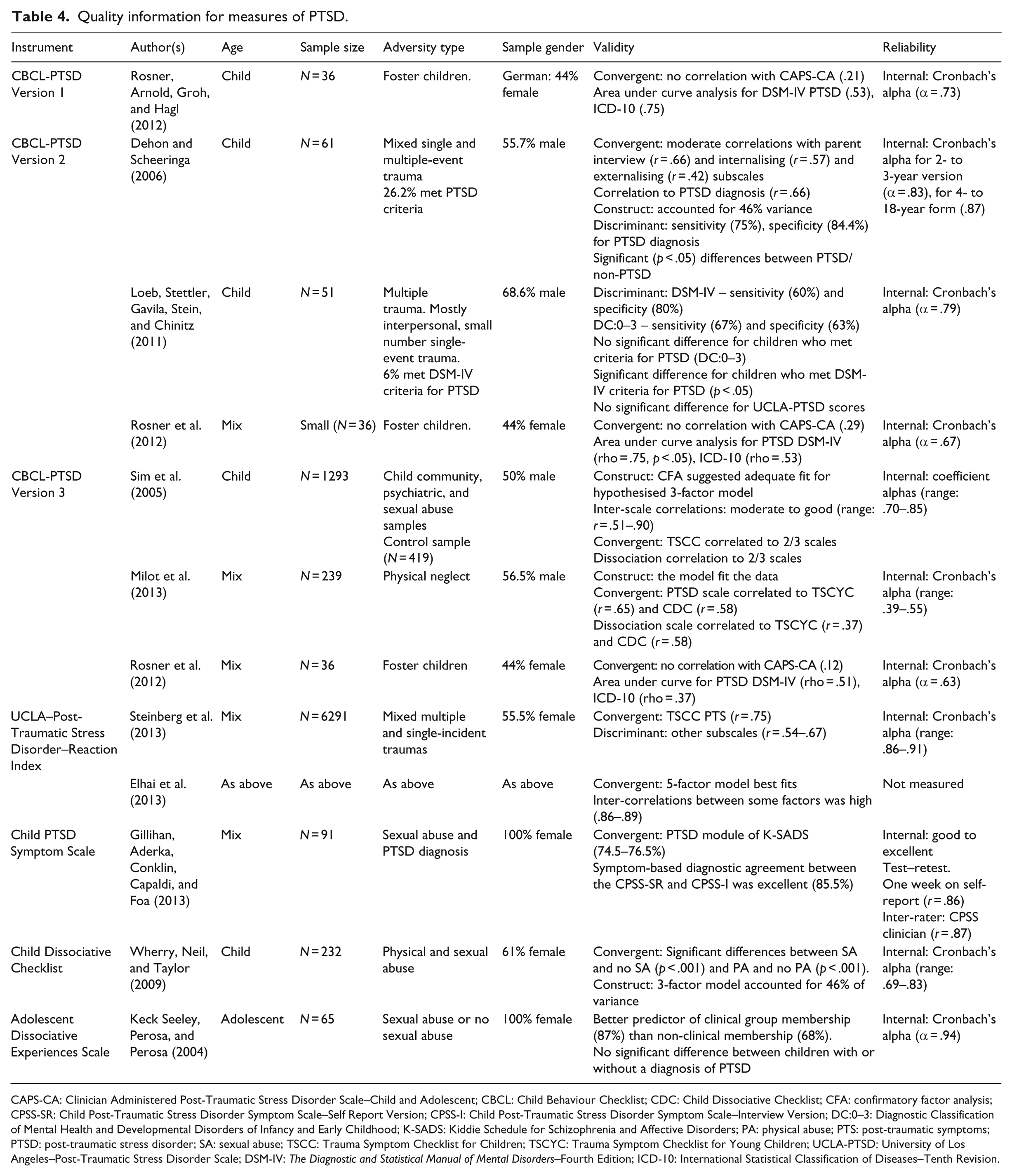
CAPS-CA: Clinician Administered Post-Traumatic Stress Disorder Scale–Child and Adolescent; CBCL: Child Behaviour Checklist; CDC: Child Dissociative Checklist; CFA: confirmatory factor analysis; CPSS-SR: Child Post-Traumatic Stress Disorder Symptom Scale–Self Report Version; CPSS-I: Child Post-Traumatic Stress Disorder Symptom Scale–Interview Version; DC:0–3: Diagnostic Classification of Mental Health and Developmental Disorders of Infancy and Early Childhood; K-SADS: Kiddie Schedule for Schizophrenia and Affective Disorders; PA: physical abuse; PTS: post-traumatic symptoms; PTSD: post-traumatic stress disorder; SA: sexual abuse; TSCC: Trauma Symptom Checklist for Children; TSCYC: Trauma Symptom Checklist for Young Children; UCLA-PTSD: University of Los Angeles–Post-Traumatic Stress Disorder Scale; DSM-IV: The Diagnostic and Statistical Manual of Mental Disorders–Fourth Edition; ICD-10: International Statistical Classification of Diseases–Tenth Revision.
Sample quality
Sample age
The majority of measures were validated against samples spanning a wide age range. In one case, participants’ ages ranged from 6 to 18 years (CPSC; Milot et al., 2013). Three instruments were validated in child-only populations in four studies (Table 4), while the ADES was the only measure validated within an adolescent population (11–18 years; Keck Seeley et al., 2004).
Trauma/adversity type
Across the majority of studies, demographic information regarding adversity type was sparse and samples were often contaminated through combinations of participants who had experienced multiple or single-event traumas (Dehon & Scheeringa, 2006; Elhai et al., 2013; Loeb et al., 2011; Steinberg et al., 2013). Of the studies which focused on interpersonal trauma, there were different adversities reported for each sample such as sexual abuse (Gillihan, Aderka, Conklin, Capaldi, & Foa, 2013; Keck Seeley et al., 2004), historical physical and sexual abuse (Wherry, Neil, & Taylor, 2009) and neglect (Milot et al., 2013). Often, although adversity type was labelled, the authors failed to document whether other forms of abuse had occurred in conjunction with those documented (e.g. Gillihan et al., 2013; Keck Seeley et al., 2004). Only one study considered the complex trauma debate and utilised a sample of fostered children who reported past experiences of one or more traumatic events. Although the authors elaborate on the type of events that were measured, children in out of home care who have experienced multiple traumatic events are highly likely to be reflective of a developmental trauma population (Rosner et al., 2012).
Reliability and validity
A range of reliability and validity evaluations were carried out in all studies in the PTSD category including assessments of convergent validity, sensitivity and factor structure. The majority of measures demonstrated good alpha coefficient ratings for the entire scale and within measure subscales (Table 4). However, although early validation studies of the CBCL-PTSD showed good internal reliability (Sim et al., 2005), further studies reported acceptable (Rosner et al., 2012) or poor internal reliability (Milot et al., 2013) suggesting it is not stable across different samples.
Most authors reported correlations with other trauma-focused measures such as the Trauma Symptom Checklist for Children (TSCC; Briere, 1996) as evidence of convergent validity (Sim et al., 2005; Steinberg et al., 2013), with high correlations reported for theoretically similar subscales. However, some instruments recorded poor correlation reports, such as the pre-school version of the CBCL-PTSD subscale (Dehon & Scheeringa, 2006) which demonstrated no significant correlation to the UCLA-PTSD-RI (Loeb et al., 2011), and the CBCL-PTSD subscales (Sim et al., 2005) which demonstrated poor correlations with a Clinical Administered PTSD measure despite significant correlations to DSM-IV criteria (Loeb et al., 2011; Rosner et al., 2012).
Some measures demonstrated a lack of sensitivity. For example, although the ADES was better at predicting clinical or non-clinical group membership, there was no significant difference in the average scores of clinical participants with or without a PTSD diagnosis (Keck Seeley et al., 2004). Similarly Sim et al.’s (2005) PTSD subscale showed two clinical groups as undistinguishable from each other, although the absence of trauma assessment may have skewed the results. Receiver operating characteristic (ROC) curve analyses of the CBCL-PTSD subscales revealed that only the pre-school CBCL-PTSD scale had the capacity to predict PTSD at a level significantly different from chance. However Dehon’s CBCL-PTSD scale was criticised for its maximum sensitivity which appeared to reflect generic rather than trauma-related distress (Loeb et al., 2011).
Some measures recorded weak factor structures, for example, the UCLA-PTSD-RI. Nonetheless, the measure showed high between-factor correlations even in the five-factor modification (Elhai et al., 2013). Similarly, support was reported for Sim et al.’s (2005) PTSD and Dissociation scales; however, investigation of the longer PTSD/Dissociation scale revealed a two-factor structure rather than the one-factor structure suggested by the author (Milot et al., 2013).
Conclusion – PTSD
The lack of appreciation for developmental difference in children and young people who have experienced symptoms of trauma is a significant limitation within this category as few measures were designed for children or adolescents alone. The results do not provide support for any of the CBCL-PTSD scales; however, the samples were small and specific, therefore replication with larger and more diverse samples is necessary. The UCLA-PTSD-RI study (Elhai et al., 2013; Steinberg et al., 2013) utilised the most robust sample size and statistical analysis; however, the poor distinction between single and multiple-incident traumas may limit its assessment utility. The UCLA-PTSD-RI focuses on PTSD diagnostic criteria and was not designed for a maltreated population; therefore, it would not be recommended as a stand-alone assessment tool.
Measures of trauma symptomatology outside PTSD criteria
A total of 11 measures were identified which assessed trauma symptomology outside, or in addition to, PTSD diagnostic criteria (Tables 5 and 6). Of these, nine were validated for children (Trauma Symptom Checklist for Young Children (TSCYC; Gilbert, 2004; Pollio, Glover-Orr, & Wherry, 2008; Wherry, Graves, & King, 2008), TSCYC - Short Form (TSCYC-SF; Wherry, Corson & Hunsaker, 2013), Assessment Checklist for Children (ACC; Tarren-Sweeney, 2007), Brief Assessment Checklist for Children (BAC-C; Tarren-Sweeney, 2013b), Trauma Assessment for Young Children (TAYC; Strickler, 2011), Child Paediatric Emotional Distress Scale (Saylor, Cupit, Reynolds & Taylor, 1999), Story Stem Assessment Profile (Hodges, Steele, Kaniuk, Hillman, and Asquith, 2009), Trauma Play Scale (Findling, Bratton & Henson, 2006; Myers, Bratton, Hagen, & Findling, 2011) and Dominic Interactive Assessment (de la Osa, Ezpeleta, Granero, Olaya, & Domenech, 2011)) and two for adolescents (Assessment Checklist for Adolescents (ACA; Tarren-Sweeney, 2013a) and Brief Assessment Checklist for Adolescents (BAC-A; Tarren-Sweeney, 2013b)). None were developed or validated for use across the age range.
Demographic information for measures of trauma not including PTSD.
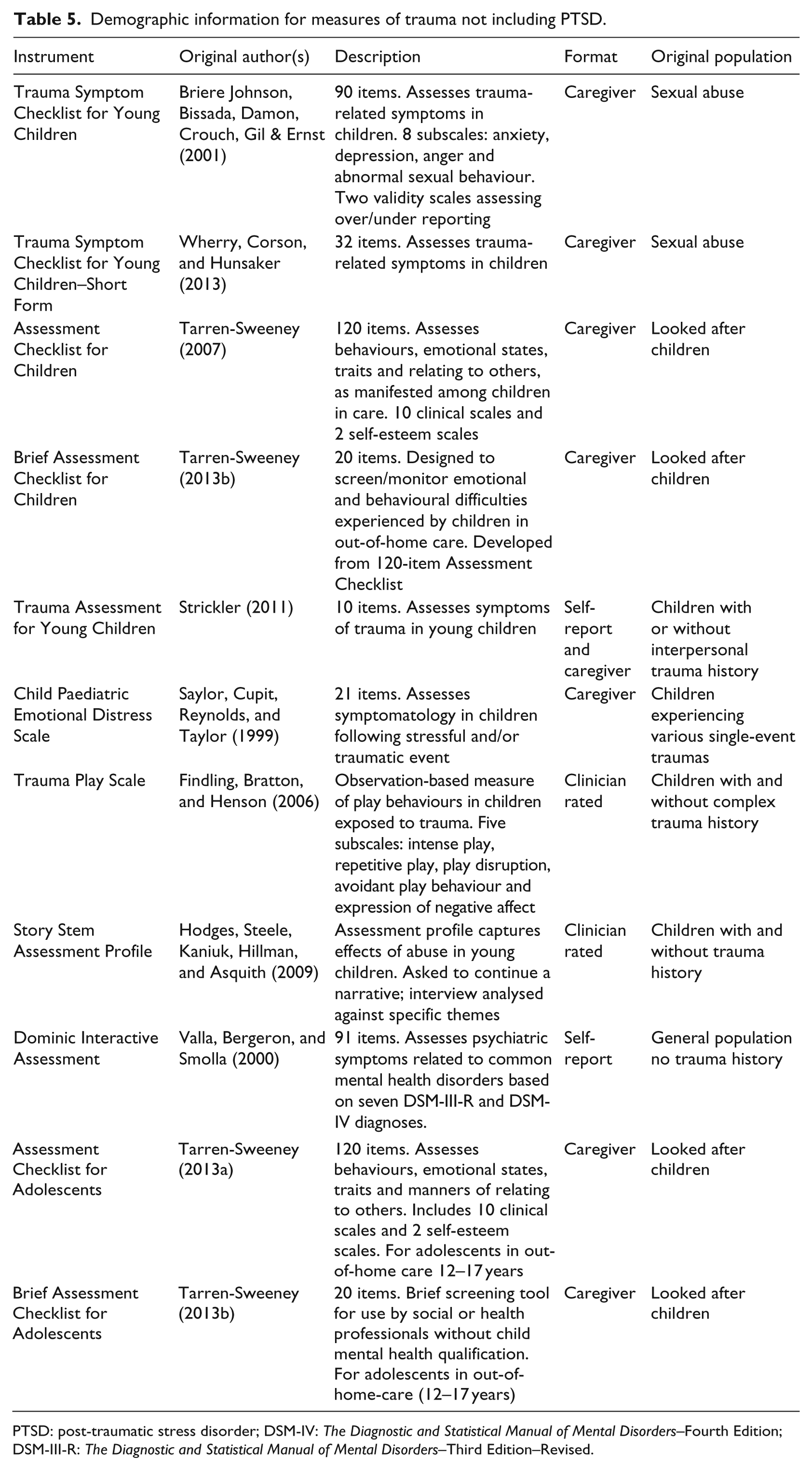
PTSD: post-traumatic stress disorder; DSM-IV: The Diagnostic and Statistical Manual of Mental Disorders–Fourth Edition; DSM-III-R: The Diagnostic and Statistical Manual of Mental Disorders–Third Edition–Revised.
Quality information for measures of trauma not PTSD.
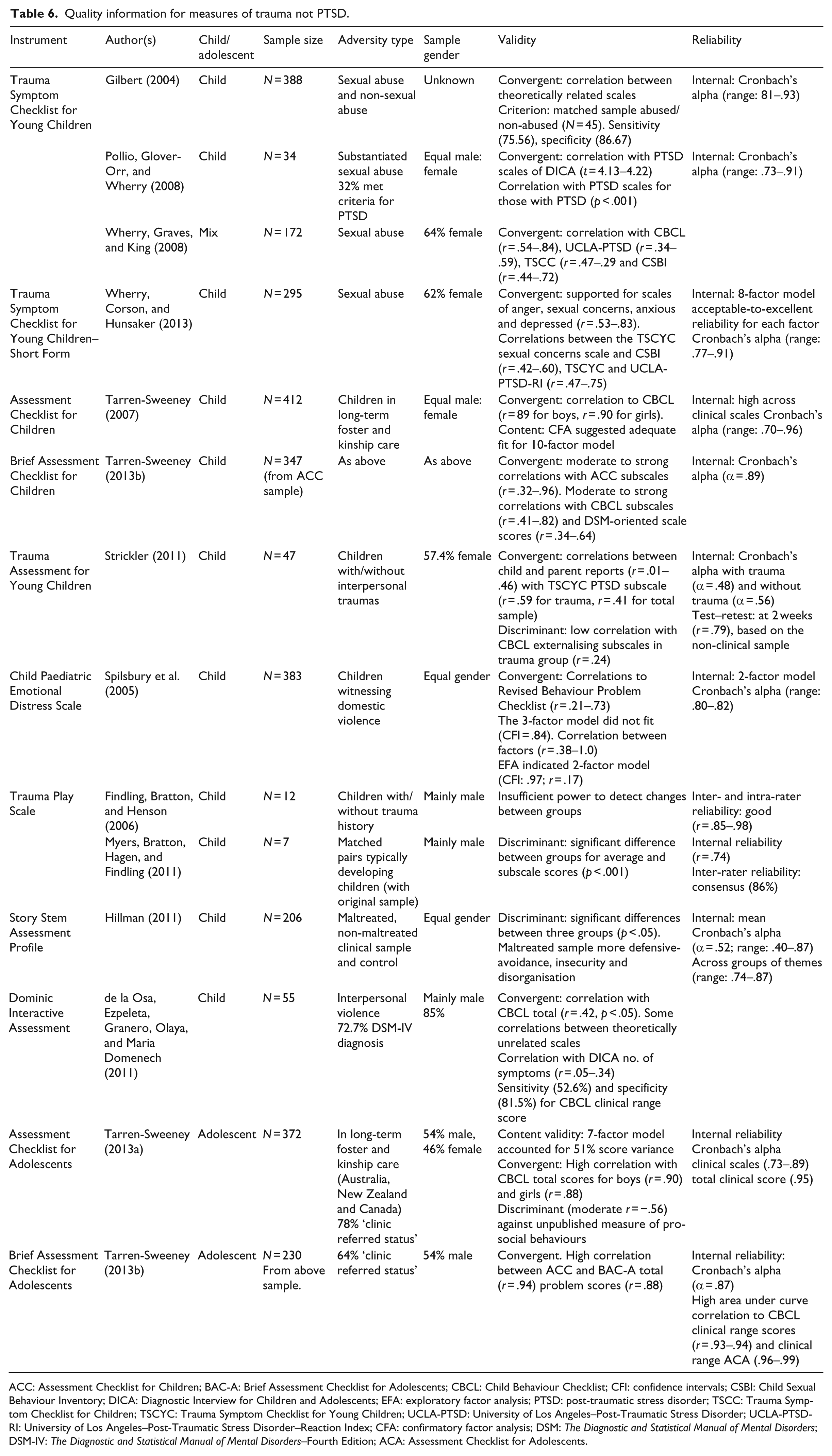
ACC: Assessment Checklist for Children; BAC-A: Brief Assessment Checklist for Adolescents; CBCL: Child Behaviour Checklist; CFI: confidence intervals; CSBI: Child Sexual Behaviour Inventory; DICA: Diagnostic Interview for Children and Adolescents; EFA: exploratory factor analysis; PTSD: post-traumatic stress disorder; TSCC: Trauma Symptom Checklist for Children; TSCYC: Trauma Symptom Checklist for Young Children; UCLA-PTSD: University of Los Angeles–Post-Traumatic Stress Disorder; UCLA-PTSD-RI: University of Los Angeles–Post-Traumatic Stress Disorder–Reaction Index; CFA: confirmatory factor analysis; DSM: The Diagnostic and Statistical Manual of Mental Disorders; DSM-IV: The Diagnostic and Statistical Manual of Mental Disorders–Fourth Edition; ACA: Assessment Checklist for Adolescents.
Sample quality
Sample age
The measures within this category were largely designed and validated within child populations (2–12 years). Only two measures, the ACA (Tarren-Sweeney, 2013a) and the BAC-A (Tarren-Sweeney, 2013b), were validated against an adolescent population (12–18 years).
Trauma/adversity type
Most commonly, measures were evaluated against samples of participants who had experienced one type of adversity, for example, all studies on the TSCYC, including those on the short-form of the measure, utilised participants who had been exposed to sexual abuse (Gilbert, 2004; Pollio et al., 2008; Wherry et al., 2013; Wherry et al., 2008). Failure to document the presence of other forms of adversity and/or whether trauma was single-event or ongoing was common across studies. Of note were the studies investigating the PEDS (Spilsbury et al., 2005) and DIA (de la Osa et al., 2011). These studies investigated samples of children, high proportions of whom rated themselves as having both exposure to violence and expectation of event re-occurrence. This suggests these samples were exposed to chronic and possibly ongoing trauma and would potentially meet the criteria for DTD.
A selection of studies included multiple trauma samples that would likely meet developmental trauma criteria. Strickler (2011) evaluated the TAYC on a sample of children with experience of ‘interpersonal trauma’ including domestic violence, sexual abuse, physical abuse and/or emotional abuse. Similarly, the ACC (Tarren-Sweeney, 2007), ACA (Tarren-Sweeney, 2013a), BAC, BAC-A (Tarren-Sweeney, 2013b) and the Story Stem Assessment Profile (Hillman, 2011) were evaluated against data from samples of LAC and young people who had experienced various social adversities and multiple forms of maltreatment in their lifetime.
Reliability and validity
The majority of measures demonstrated good reliability in the form of Cronbach’s alpha coefficient ratings (Table 6). One instrument demonstrated poor internal reliability for both children with and without traumatic histories (TAYC; Strickler, 2011]), although this was one of the few studies investigating a self-report measure. Spilsbury et al. (2005) demonstrated good internal reliability for the PEDS after adjustments were made to the model suggesting that the original was not appropriate within a complex trauma population.
Only two studies reported test–retest reliability for the measures (Myers et al. 2011; Strickler, 2011) with good results, although Strickler’s investigation of the TAYC was based solely on the non-clinical sample. Evidence of convergent validity was reported against other known PTSD measures such as the UCLA-PTSD-RI (Wherry et al., 2013; Wherry et al., 2008), or the PTSD Diagnostic Interview for Children and Adolescents Scale (DICA; Pollio et al., 2008). A measure of sexual behaviour (CSBI; Baker et al., 2008) was also used to establish the validity of the sexual behaviour subscale of the TSCYC (Wherry et al., 2008). A selection of studies made comparisons against general measures of emotional and behavioural functioning such as the Revised Problem Behaviour Checklist (Spilsbury et al., 2005) or the CBCL (Strickler, 2011). While several studies reported correlations to the CBCL measure as evidence of convergent validity (de la Osa et al., 2011; Tarren-Sweeney, 2007, 2013a, 2013b; Wherry et al., 2013; Wherry et al., 2008), one study argued that a low correlation to the externalising scale of the CBCL demonstrated evidence of discriminant validity in their measure (TAYC; Strickler, 2011).
Discriminant validity was also reported in significant differences between groups of children with and without a history of trauma. This was found to be true for the Trauma Play Scale (Myers et al., 2011), Story Stem Assessment profile (Hillman, 2011) and the TSCYC (Pollio et al., 2008). Some also measured sensitivity by ROC under the curve analysis to assess the ability of the measure to detect PTSD diagnosis (Pollio et al., 2008) or CBCL clinical range scores (de la Osa et al., 2011).
Conclusion – trauma symptomology outside PTSD criteria
A greater number of studies evaluating measures of trauma symptomatology outside PTSD criteria utilised looked after child samples who had been exposed to multiple traumas and were most likely to meet criteria for DTD. Other studies restricted their investigations to samples with experience of one type of adversity and at times, details about the type, severity, and chronicity were absent. The TSCYC (Gilbert, 2004; Pollio et al., 2008; Wherry et al., 2013; Wherry et al., 2008) demonstrated psychometric strengths but has largely been studied within a sexual abuse population. The TAYC (Strickler, 2011) benefits from a self-report format and the authors’ consideration of complex trauma and age-appropriate cognitive and social skills in its development. The Assessment Checklists (Tarren-Sweeney, 2007, 2013a, 2013b) had the most robust sample size and statistical analysis and demonstrated utility for trauma-related psychopathology within a clinically relevant population. However, there is no self-report component, and the authors warned that the brief versions of the Assessment Checklist’s (Tarren-Sweeney, 2013b) should not replace comprehensive, multi-informant assessment. Nonetheless, they show promise as an assessment tool (both brief and fuller versions) for a developmental trauma population.
Discussion
The field of trauma assessment has grown over the last decade, with 42 papers evaluating assessment instruments identified since Strand et al.’s (2005) review. The current review identified that few assessment measures have been robustly investigated to generate confidence in their use with children and adolescents who have suffered developmental trauma. The majority of studies utilised samples that were demographically ill-defined, too small or too specific (e.g. participants who reported only one form of abuse). The focus on sexual abuse has meant that there are a number of assessment measures that could be recommended for use with children and/or adolescents with a history of sexual abuse (TSCYC (Briere et al., 2001), CSBI (Baker et al., 2008), SFRS (Kruczek & Ægisdóttir, 2005) BYI-S (Runyon et al., 2009), CPSC (Milot et al., 2013) and ADES (Keck Seeley et al., 2004)). However, studies failed to highlight whether victims were subject to single or multiple-event sexual trauma; therefore, caution should be exercised in their use. The lack of attention to demographic information suggests that researchers have not engaged sufficiently with the evidence that abuse rarely occurs in isolation from other adversities (Dong et al., 2004).
A definition of trauma in research
The challenge for researchers is to remain focused on the unique impact of cumulative trauma (Briere, Kaltman, & Green, 2008) and the research suggesting multiple- and single-trauma experiences result in different trauma symptomatology profiles (Green et al., 2000; Jonkman, Verlinden, Bolle, Boer, & Lindauer, 2013). Despite qualitatively distinct outcomes for children who experience interpersonal trauma and abuse versus road traffic accidents and natural disasters (Cook et al., 2005), this review suggests that researchers continue to group participants together under an all-encompassing ‘trauma’ label, with little consideration of the type, frequency or developmental context within which the experience occurred. Future studies need to provide detailed demographic data so that instruments’ validation population is clearly defined and subsequent generalisation to maltreatment populations is appropriate.
The assessment checklist tools
Even without adequate validation data, the review highlighted an overreliance on measures designed for existing clinical populations. Very few standardised measures were designed for use with a developmental trauma population, a weakness that has previously been highlighted by other authors (DeJong, 2010; Tarren-Sweeney, 2013a). The Assessment Checklist tools developed by Tarren-Sweeney (2007, 2013a, 2013b) were the only measures designed to encapsulate the pervasive effects of developmental trauma experiences that have been observed and documented by clinicians and researchers in the field (Cook et al., 2005; DeJong, 2010; Octoman, McLean, & Sleep, 2014; van der Kolk, 2005). Children and young adolescents in out-of-home placements are likely to represent the extremity of the maltreatment spectrum (DeJong, 2010) as they are highly likely to have experienced multiple forms of abuse, abandonment and general maltreatment (Browne & Lynch, 1999) which mirror the multiple chronic traumas argued to precede DTD (van der Kolk, 2005). One of the major strengths of the Assessment Checklists was the design of age-specific versions developed for children and adolescents.
A developmental context
The need for a developmentally appropriate conceptualisation of the impact of maltreatment has long been discussed (Cichetti & Toth, 1995). There is strong consensus of a statistically significant risk between childhood maltreatment and developmental deficits (Thornberry, Ireland, & Smith, 2001). However, measurement of such emotional and behavioural delays must be given appropriate developmental consideration (Downs, 1993). The timing of abuse experiences has been associated with discrete symptom profiles among children and adolescents (Keiley, Howe, Dodge, Bates, & Petit, 2001; Thornberry et al., 2001) as well as in later adulthood (Thornberry, Henry, Ireland, & Smith, 2010). Advances in the field of neuropsychology support this with identification of volumic changes to specific regions of the brain dependant on abuse timing (Andersen et al., 2008; DeBellis et al., 1999). Maltreatment occurring in multiple developmental periods increases the risk of developing internalising and externalising problems and lower IQ compared with incidence in one developmental period (Jaffee & Maikovich-Fong, 2010). Therefore, when assessing the impact of developmental trauma on children and adolescents, utilising measures developed and validated for specific developmental periods is prudent.
This review identified a significant divide in developmentally appropriate measures of trauma for children and adolescents. Interestingly, the majority of tools developed solely for adolescents examined general functioning and mental health factors, whereas those designed for solely children often focused on trauma-related symptomatology outside of DSM diagnostic criteria. In the assessment of PTSD, adolescents were predominantly grouped with children as young as 7 years old (Blake et al., 2007; Elhai et al., 2013; Steinberg et al., 2013). This replicates Strand et al.’s (2005) conclusion that there is a lack of adolescent measures of trauma symptoms beyond PTSD. Tarren-Sweeney (2013a) highlighted that expression of behavioural and emotional difficulties within the maltreated population varies by developmental level and without a developmental framework, age-appropriate behaviours could be inappropriately pathologised. Many studies identified in this review included samples of children and adolescents in restricted age groups (e.g. 10–12 or 14–18 years), or those which crossed over developmental periods (e.g. up to 22 years; Liebenberg et al., 2013) suggesting the impact of developmental stage was not considered. This may also be due to the lack of age-specific assessment tools currently available to researchers in the field since many of the tools included in this review were validated for a wide age range spanning from early childhood into early adulthood.
The developmental trauma debate
A challenge presented within the reviewed papers is the lack of consistency in the theoretical understanding of these children and adolescents’ difficulties. There has been an emphasis on trying to conform to a diagnostic classification system, for example, DSM-IV PTSD, but failure to recognise the complexity of presenting difficulties, leading to multiple co-morbid diagnoses. The majority of authors failed to engage with the developmental trauma debate; however, studies including LAC largely acknowledged the need for broader conceptualisation of maltreatment experiences. Moreover, there appeared to be an emerging recognition of the need to examine other psychological and behavioural constructs (e.g. self-esteem, dissociation, attachment and sexual behaviour) beyond PTSD criteria.
The dilemmas of seeking to diagnose children and adolescents with histories of developmental trauma against the current classification system are well-documented (Spinazzola et al., 2005). Although the DTD debate attempted to address these challenges, the proposal was not accepted into the new edition of the DSM (DSM-V; APA, 2013). Critics have suggested its inclusion would weaken the authority of current classification systems by failing to clearly distinguish between DTD symptoms and syndromes already widely accepted, such as Borderline Personality Disorder (for a review of the debate, see Schmid, Petermann, & Fegert, 2013). Researchers have highlighted the limitations of overreliance on diagnostic constructs with developmentally traumatised populations due to their narrow constraints and the often atypical presentations observed in these children (DeJong, 2010). However, with access to Child and Adolescent Mental Health Services (CAMHS) being largely diagnosis-led, many children are failing to receive adequate mental health care provision (Minnis & Del Priore, 2001), often resulting in carers managing high levels of complexity and risk alone (Sturgess & Selwyn, 2007). Clinicians and researchers have called for a multi-strand approach when working with developmentally traumatised populations including the use of psychological formulation and multi-agency working (Golding, 2010). Incorporating these principles into assessment protocols could limit an overreliance on narrow assessment tools while accounting for the wide range of contextual factors these young people present with (Callaghan, Young, Pace, & Vostanis, 2004). Ongoing research into the clinical utility of DTD and associated tools is required to determine how a developmental perspective on trauma can be incorporated into current diagnostic systems.
Conclusion
Given that childhood adversity has profound implications on a child’s development, leads to difficulties across multiple domains of functioning and is likely to minimise the chances of realising their potential, trauma-informed assessment is fundamental. Despite some methodological shortfalls, there are a growing variety of assessment tools available such as the TSCYC (Briere et al., 2001), TAYC (Strickler, 2011) and ACC/BAC-C (Tarren-Sweeney, 2007, 2013b) for children and the ACA/BAC-A (Tarren-Sweeney, 2013a, 2013b) for adolescents. Future research needs to validate the measures with well-defined samples, as well as inductively developing new measures or tools to assess the range of pervasive difficulties that are sensitive to the child’s cognitive and social developmental stage. For clinicians seeking to assess these children, the incorporation of multiple methods of assessment, including psychological formulation and developmentally appropriate tools, is recommended.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.