
Abstract
Research into the effectiveness of therapeutic interventions for older children who have experienced multiple forms of trauma within the context of their early development is scant. This article explores the effectiveness of Neuro-Physiological Psychotherapy (NPP): a wrap-around multi-disciplinary, neuro-sequential, attachment-focussed intervention for children and families who present with multiple, clinically significant, emotional and behavioural difficulties. In total, 31 young people and their adoptive parents took part in the study. Baseline measures were repeated and parents and children interviewed. An assessment of the parent/child relationship and child attachment was undertaken but not analysed for this article. Analysis of the repeated measures received statistically significant changes in behavioural regulation, metacognitive executive functioning and externalising and internalising difficulties, alongside an improvement in thought and social problems. An analysis of the parent interviews provided positive results in terms of the children’s engagement in education, an absence of further mental health diagnosis or involvement in the criminal justice system. Further hypotheses are posited regarding the impact of the treatment and further research into the effectiveness of the model outlined.
Introduction
Two recent studies have provided invaluable data regarding the plethora of difficulties that many children in care or who are adopted from care can endure. Brown and Ward (2013) carried out an extensive review of the literature on the impact of maltreatment on child development and outcomes as part of their review for the Department for Education regarding decision making in child welfare. This review highlights the extent of developmental, social, emotional and attachment difficulties that many children who have experienced maltreatment present with throughout their life-span and the implications for intergenerational transmission of these patterns. Selwyn, Wijedasa, and Meakings (2014) conducted a study into adoption disruption in the United Kingdom and reported on experiences of family members when the adoption placement was in difficulty or disrupted. In this study, one-quarter of the adopted parents taking part reported major hardship in caring for children with multiple and overlapping difficulties. The study also found that this group of children had presented with ‘extraordinarily high’ 1 levels of social, emotional and behavioural difficulties across two screening tools which are predictive of later mental health difficulties. Also evident from the study was that older placed children experienced a higher level of difficulties and higher level of disruption rates. There was also a significant impact on the mental health of parents caring for this group of children, with higher levels of depression and post-traumatic stress disorder reported.
For this population of children, there is sparse evidence regarding treatment efficacy. There also appears to be little consensus among professionals working across the field as to what the most suitable treatment modality should be. Research into the effectiveness of therapeutic programmes for maltreated children who are in alternative care provision has proven to be mixed. Evidence shows that children who are looked after are at significant risk of later mental health difficulties (Brown & Ward, 2013; Meltzer, Gatward, Corbin, Goodman, & Ford, 2003). Brand and Brinich (1999) found that children adopted from care were more likely to have mental health difficulties than non-adopted children, with a small proportion of the group of adopted children accounting for the difference and therefore exhibiting clinically high levels of difficulty and later placed children exhibiting significantly greater difficulties in adolescence than non-adopted. In a time when clinicians are called upon to engage in evidence-based practice, little actually exists in terms of evidence for these children. An overview of research into interventions for this population of children is required before proceeding with the subject of this exploratory study.
While parent training programmes based on Social Learning Theory have yielded positive results when delivered to birth parents, there is limited evidence to support their effectiveness in reducing the complex emotional and behavioural difficulties presented by many children who have suffered neglect, abuse and the effects of multiple foster placement breakdowns. Although foster carers and adoptive parents report a positive experience of such programmes, no significant improvement in the children’s behaviours has been found (Hill-Tout, Pithouse, & Lowe, 2003; Minnis & Devine, 2001; Pallett, Scott, Blackeby, Yule, & Weissman, 2002; Rushton, Monck, Leese, McCrone, & Sharac, 2010).
The Multidimensional Treatment Foster Care programme in the United States (Chamberlain, 2003) and England (Roberts, 2007) is targeted at adolescents who have serious behaviour difficulties. Three randomised controls have taken place, and although these studies found an improvement in challenging behaviour for adolescents who completed the programme, they do not provide evidence for a change in emotional or mental health difficulties (Chamberlain, Leve, & DeGarmo, 2007; Chamberlain & Moore, 1998; Chamberlain & Reid, 1991; Eddy & Chamberlain, 2000; Eddy, Whaley, & Chamberlain, 2004; Leve & Chamberlain, 2005, 2007; Leve, Chamberlain, & Reid, 2005).
Golding and Picken (2004) have developed a model for working with parents based on neurodevelopmental and attachment theory. Studies which examine the effectiveness of this approach, while having small samples (less than 15), do show some change. Golding and Picken (2004) and Gurney-Smith, Randle, and Fletcher (2010) reported improvement in carer’s satisfaction in parenting their children and understanding their children’s needs. Similarly, some significant improvements were documented in the children’s behaviours and emotional functioning. A 3-month follow-up found such changes were sustained (Gurney-Smith et al., 2010). While other studies evaluating an application of the same approach reported improvement in carer’s stress, they found no significant improvements in the child’s behaviours, emotional functioning or the child–parent relationship (Laybourne, Andersen, & Sands, 2008). The authors suggest that for families with greater level of difficulties and need, such a group is only a starting point and further therapeutic work is needed if change is to be achieved.
The effectiveness of dialectic behaviour therapy (DBT) with adolescents in the looked-after care system was also explored and obtained mixed results (James, Winmill, Anderson, & Alfoadari, 2011). Again, it is important to note the small sample size (20). In the treatment group, 35% failed to engage, but despite this, an ‘intention-to-treat’ analysis found that of the outcomes measured, DBT significantly improved emotional functioning in terms of level of depression, sense of hopelessness, frequency of self-harm and global functioning. However, no significant changes in attachment style, negative automatic thoughts or quality of life scores were reported. An intervention for young people leaving care which integrates Dyadic Developmental Psychotherapy (DDP) and DBT has been developed (Andrew, Williams, & Waters, 2014). Although formal analyses of the efficacy of the intervention are yet to be published, initial exploration indicated positive effects with self-reported reductions in self-harm, suicidal ideation, relationship difficulties and drug use.
Positive evidence for trauma-focussed cognitive behavioural therapy (TF-CBT) of children exists only for those who have experienced single incident trauma (Cary & McMillen, 2012; Cohen & Mannarino, 2008, 2010), and studies generally do not include children in alternate care provision. Cohen, Mannarino, Kliethermes, and Murray (2012) have begun to discuss the need to adapt TF-CBT for children who are in alternative care provision and who have experienced complex trauma.
Moving towards family interventions, DDP (Hughes, 2006, 2007) is an attachment-based family therapy developed for children who are adopted or fostered and aims to strengthen the child–parent relationship. The model is discussed in greater depth in the companion paper in this publication (Vaughan, McCullough, & Burnell, this issue). Currently there are three studies where aspects of DDP are integrated with other interventions in the treatment of children with complex trauma to produce positive results (Aideuis, 2007; Andrew et al., 2014; Friend, 2012). There are two small studies of Becker-Weidman (2006, 2008) that are rightfully questioned on methodological grounds but might be considered initial pilot studies of DDP to encourage further research. A large empirical approach across is currently in process.
The Attachment, Regulation, Competency (ARC) model (Kinniburgh, Blaustein, Spinazzola, & van der Kolk, 2005) addresses three core domains: attachment, self-regulation and developmental competencies. The model is flexible and involves the child, the family and the system around the family. Arvidson et al. (2011) found that the ARC model significantly improves children’s behaviour and emotional functioning.
While some positive practice is indicated, limitations and sparse number of studies in this literature review highlight the need for further research for this population of children. It also emphasises the lack of research into the effectiveness of a multi-component treatment model addressing the many areas of difficulty which manifest following complex trauma during early development.
Family Futures is a Voluntary Adoption Agency and community interest company that specialises in Adoption Support. Its therapeutic treatment approach to recovery of children who have experienced sustained trauma in the context of their birth family environment has been influenced by pioneering and leading research and practice in the field. Neuro-Physiological Psychotherapy (NPP) is a wrap-around multi-disciplinary, neuro-sequential, attachment-focussed intervention for children and families who present with multiple, clinically significant, emotional and behavioural difficulties. The model is described in the companion paper (Vaughan et al., this issue), and a summary of the main components is shown in Figure 1.
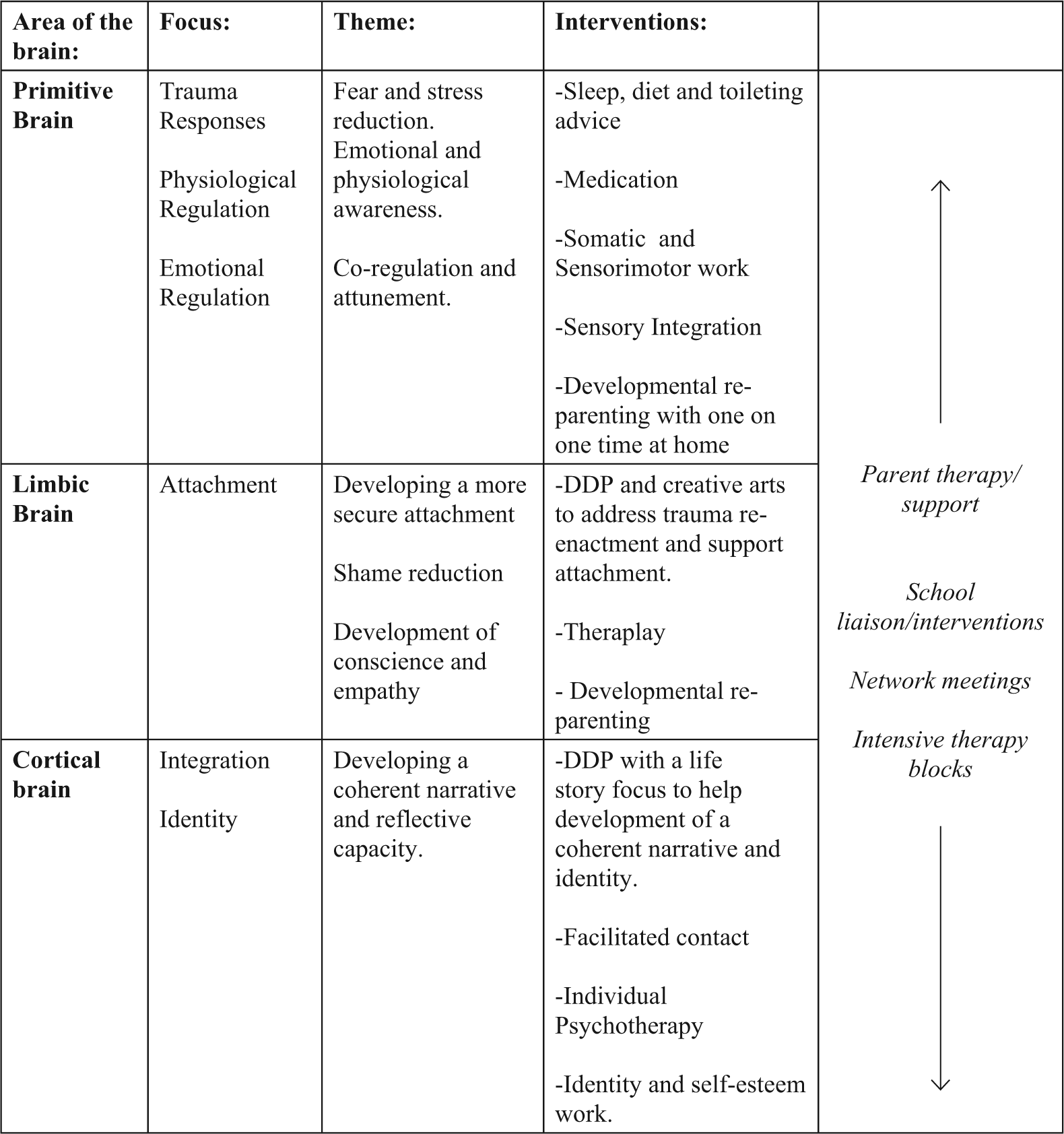
The Neuro-Physiological Psychotherapy model.
Aims of this study
This pilot study aims to evaluate the NPP model. While there is little empirical evidence currently in existence for the component parts of the model, there is good theoretical justification for the integration of its core modalities (Vaughan et al., this issue), and an evaluation of clinical outcomes provides an opportunity to explore the changes witnessed in practice. This study set out to explore changes in behavioural, emotional and executive functioning difficulties in young people who have completed the NPP programme.
Ethics
This study is an internal third sector agency, post-treatment service evaluation, and therefore, ethics committee approval was not required on this occasion. Appropriate external consultation on matters pertaining to ethics was sought throughout.
Method
Participants
Participants consisted of young people and their adoptive parents who had either completed their treatment programme at the organisation or who had completed all the recommendations made at assessment and were in a ‘maintenance’ phase of treatment. All the young people involved had a history of exposure to multiple traumatic experiences in their birth families and were living in alternative care provision. Only young people who had received treatment at all three levels of the model, and were still in placement with the primary caregivers who originally presented in treatment with them, were included in the study. 2 Young people whose agreed treatment package planned for elements at all three levels of the model but who had not yet received this were excluded. Young people with a diagnosed moderate or severe learning disability, birth children in the adoptive families and those whose placement had disrupted 3 were excluded. In addition, those who were assessed using different assessment tools to those used currently were also excluded. Figure 2 shows the procedure by which the final sample was reached.
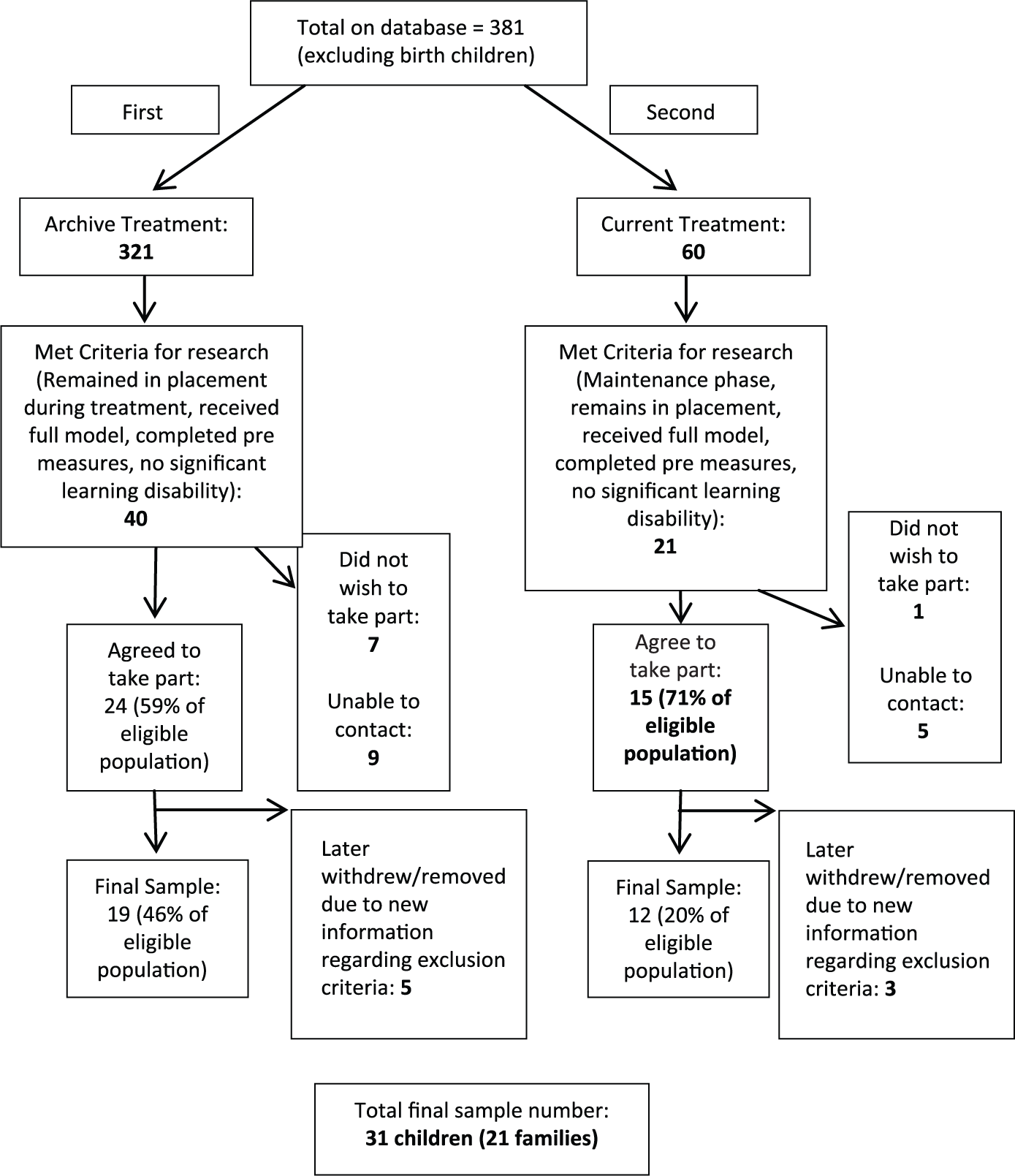
The research sample.
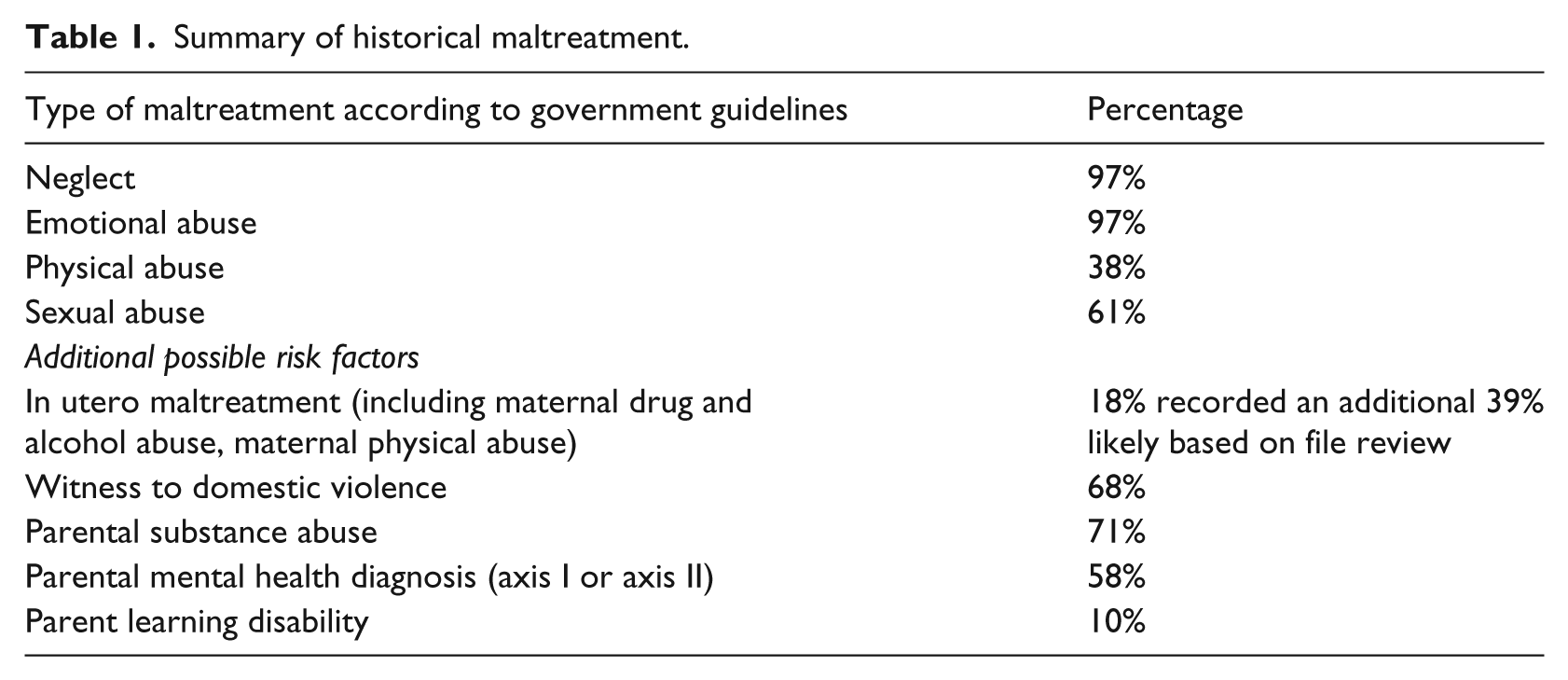
The final group consisted of 31 young people with a mean age of 14.68 years (standard deviation (SD) = 3.14). In all, 45% were male and 55% were female. Details regarding the history of the children and young people participating are summarised in Table 1. The average age at which children had been placed with their adoptive parents was 3.69 years. The average age at which children came into treatment was 9.74 years .
Summary of historical maltreatment.
The mean time in treatment was 56.36 months (SD = 34.29). For those who had completed treatment, the mean time between treatment and participation in this research was 20.6 months (SD = 17.60). The group consisted of 7 sibling groups of 2, 2 sibling groups of 3 and 13 individual young people. The number of sets of parents involved was 22.
The degree to which the families wished to be involved varied. For example, some parents agreed to complete questionnaires but did not consent to school participation. In addition, the questionnaires completed at the assessment stage varied.
Representativeness
The research participants were compared to those who had been identified as eligible but who did not respond to attempts to contact them or declined to participate in the research in order to investigate whether the research group was representative of all those eligible. Chi squared tests or Fisher’s tests where the expected count was lower than 5 were used to investigate the differences regarding history of abuse type and number of children presenting with internalising and externalising problems as measured by the Child Behaviour Checklist 6–18 (CBCL) and executive functioning difficulties as measured by the parent Behaviour Rating Inventory of Executive Function (BRIEF). Fisher’s tests revealed there were no differences between the two groups in terms of frequency of children who had histories of emotional, physical and sexual abuse and neglect; presence of domestic violence in the birth families; and birth parents with drug or alcohol abuse (all ps > .05). There were also no differences between the groups regarding the number of children presenting at assessment with CBCL Total scores, Internalising Problem scores and Externalising Problems scores in the Clinical or Borderline range as demonstrated by chi squared tests (all ps > .05). Finally, chi squared tests also revealed no differences between the two groups regarding the number of children with BRIEF Global Executive Composite, Behavioural Regulation Index and Metacognition Index scores in the Elevated range at assessment stage (all ps > .05).
Measures
CBCL
The CBCL is a paper questionnaire completed by parents or primary caregivers of children aged 6–18 years (Achenbach & Rescorla, 2001). The first section evaluates the child’s social and academic competencies. The second section consists of 118 items evaluating behavioural and emotional problems in the last 6 months. The response is on a 3-point Likert scale: not true, somewhat or sometimes true, or very true or often true. The items load onto eight syndrome scales: Anxious/Depressed, Withdrawn/Depressed, Somatic Complaints, Social Problems, Thought Problems, Attention Problems, Rule-Breaking Behaviour and Aggressive Behaviour. Anxious/Depressed, Withdrawn/Depressed and Somatic Complaints are grouped together to form the broader scale Externalising Problems. Rule-Breaking Behaviour and Aggressive Behaviour are grouped together to form an Internalising Problems scale. There is also a Total Clinical Problems scale. Diagnostic and Statistical Manual of Mental Disorders (DSM)-oriented scales and Competence scales are also produced but were not used in this study. The CBCL is widely used and has been shown to have good reliability and validity (Achenbach & Rescorla, 2001).
Teacher Report Form
The Teacher Report Form (TRF) is a teacher-completed version of the CBCL and reflects the child’s functioning in school (Achenbach & Rescorla, 2001). It consists of an evaluation of their adaptive functioning, and as with the CBCL also consists of a 118-item section on a 3-point Likert scale evaluating behavioural and emotional problems which load on to the same empirically based scales as the CBCL. Teachers are asked to consider the last 2 months rather than 6 months as in the CBCL. Good validity and reliability have also been found for the TRF (Achenbach & Rescorla, 2001).
BRIEF
The BRIEF is a paper questionnaire completed by parents and teachers of children aged 5–18 years and is a measure of children’s executive functioning and regulation (Gioia, Isquith, Guy, & Kenworthy, 2000). It consists of 86 items which are answered on a 3-point Likert scale to indicate the frequency of particular behaviours: never, sometimes or often. The items load on to eight scales measuring different aspects of executive functioning: Inhibit, Shift, Emotional Control, Initiate, Working Memory, Plan/Organise, Organisation of Materials and Monitor. The Global Executive Composite is an overall score and two indexes Behavioural Regulation and Metacognition are also produced. The BRIEF has been shown to have appropriate reliability and validity (Gioia et al., 2000).
Assessment Checklist for Children
The Assessment Checklist for Children (ACC) is a questionnaire designed specifically for children in care, adopted from care and maltreated children (Tarren-Sweeney, 2007). It consists of 120 items completed by the child’s caregiver on a 3-point Likert scale. The first 81 items have a Likert scale with the responses: not true, partly true or mostly true. The remaining items are answered using the following responses: did not occur, occurred once or occurred more than once. The clinical scales produced are Total Clinical score, Sexual Behaviour, Pseudomature, Non-reciprocal Behaviour, Indiscriminate Behaviour, Insecure, Anxious–Distrustful, Abnormal Pain Response, Food Maintenance, Self-injury and Suicide Discourse. A composite self-esteem score and scales for Negative Self-Image and Low Confidence are also produced. The ACC has high internal consistency and good construct and content validity.
Parent interview
This was a semi-structured interview conducted with parents and covered the family’s experiences of the treatment programme, their child’s presentation currently, their child’s relationships, their child’s education and any involvement their child may have had in the criminal justice system. For the two-parent families, where possible dyadic interviews with both parents were carried out and where this was not possible, the interview was conducted with just the available parent.
Additional measures
The Parent Stress Index (Abidin, 1983), Sensory Processing Measure (Parham, Ecker, Miller-Kuhaneck, Henry, & Glennon, 2007), semi-structured child interviews, Marschak Interaction Method (MIM) assessment (Marschak, 1960) and Child Attachment Interview (Target, Fonagy, & Shmueli-Goetz, 2003) or Story Stem Assessment Profile (Hodges, Hillman, & Steele, 2007) dependent on child age were also completed by parents or children to be reported on at a later date.
Procedure
Informed consent was sought from parents and children prior to completing the interviews or questionnaires. Families were offered theatre or supermarket vouchers to thank them for their participation. Questionnaire scores from assessment were obtained from client files and compiled in a database. Parents were asked to complete the questionnaires that they had originally completed at the assessment stage. If the young people were currently in school, teachers were also asked to complete school questionnaires that were also completed at the assessment stage. Given the use of the ACC is a relatively recent addition to the organisation’s assessment tools, the data for ACC completed at assessment were very limited. Therefore, retrospectively, it was decided that scores for ACCs completed during treatment would be included as pre-measures provided they were from a reasonable amount of time prior to finishing treatment. Parents then completed the semi-structured interview with a researcher in their own homes. Where they agreed, children also completed a brief version of this interview.
During the research visit to the home, parents and their children also completed a Theraplay MIM assessment of the parent–child relationship. The young people also completed either the CAI or the Story Stem Assessment dependent on their age. If the participants consented, the MIM, CAI and Story Stem Assessments were filmed. These will be analysed and compared to those completed at assessment at a later date.
Results
Data for each measure were analysed in two ways: in the first instance, all raw scores obtained were included in the analysis. In the second instance, only scores identified by the user manual as being elevated/borderline/clinical assessment stage were included in the analysis (the equivalent post-treatment score was also excluded) to explore the efficacy of the target.
Due to the small sample sizes, the Shapiro–Wilk (S-W) test was used to determine whether the data were normally distributed. Where the sample was not found to significantly differ from a normal distribution, dependent t-tests were used to explore the difference between pre-treatment and post-treatment scores for CBCL, TRF, BRIEF (teacher and parent) and ACC scales. Where an S-W test indicated that the sample did vary significantly from a normal distribution, this violated the assumptions of a t-test, and therefore, the non-parametric Wilcoxon signed-rank test was used as an alternative.
Values of p < .05 were used to determine whether the null hypothesis of no change following treatment should be rejected. Exact p values are also reported in order for readers to see where change neared statistical significance and where this may be reached with larger sample sizes. Effect sizes using Cohen’s d are also reported. These were calculated using the formula d = (M1 − M2)/SDpooled.
Parent and teacher BRIEFs
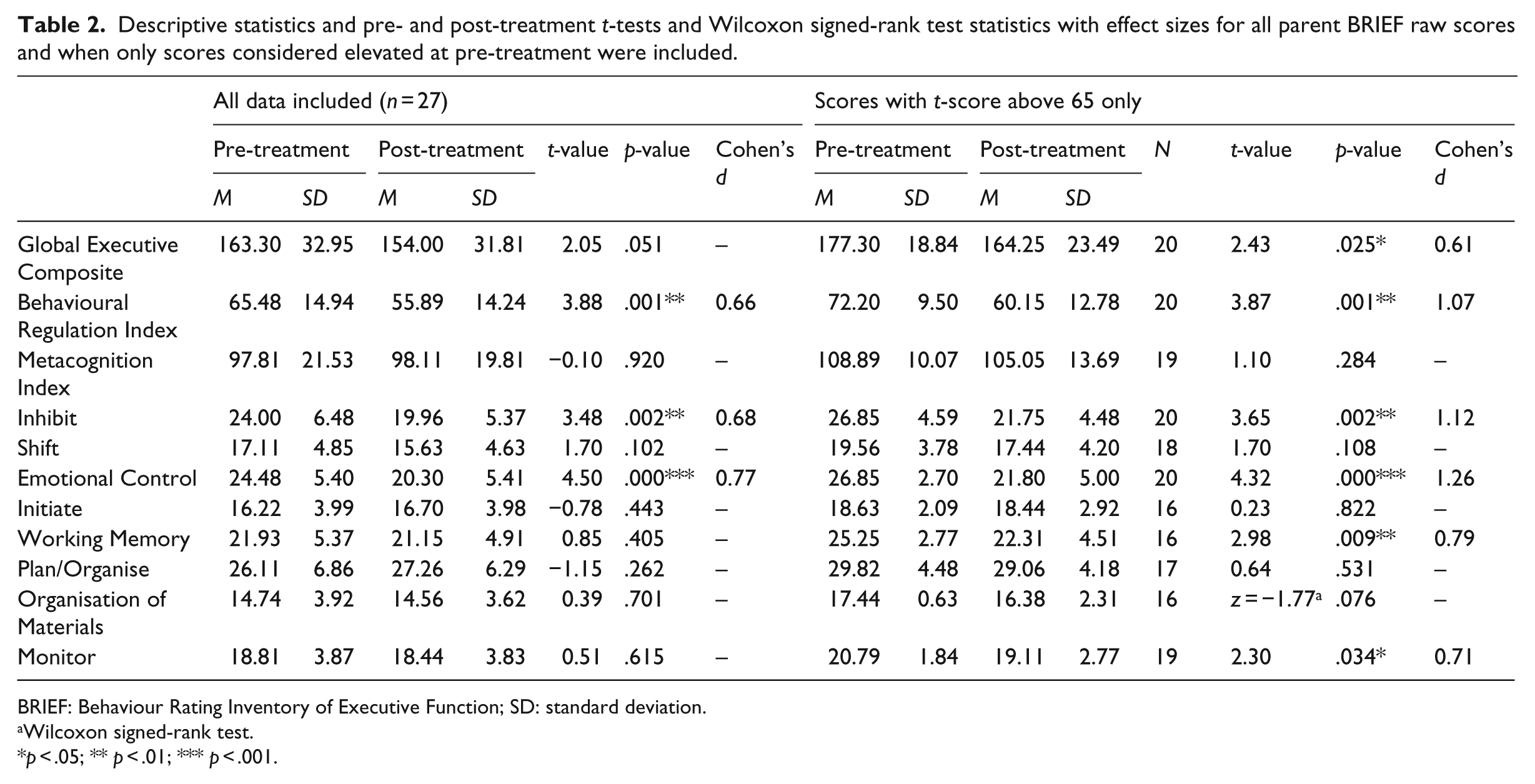
Descriptive statistics, T, Z, p and Cohen’s d values for parent and teacher BRIEF scales can be seen in Tables 2 and 3. Dependent t-tests revealed that for the parent-completed BRIEF scores for the Behavioural Regulation Index, Inhibit and Emotional Control scales decreased significantly from pre- to post-treatment (p < .05) with medium effect sizes when all scores were included. The decrease in the Global Executive Composite neared statistical significance. When scores in the ‘normal’ range pre-treatment were excluded from the analysis, scores for Global Executive Composite, Behavioural Regulation Index, Inhibit, Emotional Control, Working Memory and Monitor all significantly decreased with medium to large effect sizes.
Descriptive statistics and pre- and post-treatment t-tests and Wilcoxon signed-rank test statistics with effect sizes for all parent BRIEF raw scores and when only scores considered elevated at pre-treatment were included.
BRIEF: Behaviour Rating Inventory of Executive Function; SD: standard deviation.
Wilcoxon signed-rank test.
p < .05; ** p < .01; *** p < .001.
Descriptive statistics and pre- and post-treatment t-tests statistics with effect sizes for all teacher BRIEF raw scores and when only scores considered elevated at pre-treatment were included.

BRIEF: Behaviour Rating Inventory of Executive Function; SD: standard deviation.
p < .05; **p < .01; ***p < .001.
For the teacher-completed BRIEF scores for Global Executive Composite, Behavioural Regulation Index, Metacognition Index, Inhibit, Shift, Emotional Control, Initiate, Working Memory and Planning scales were significantly lower post-treatment compared to pre-treatment (p < .05), with medium to large effect sizes, when all scores were included in the analysis. When only pre-treatment ‘Elevated’ scales were analysed, effect sizes became large and decreases in scores for Organisation of Materials and Planning were also significant; however, decreases in Working Memory and Metacognition Index scores were no longer statistically significant.
ACC
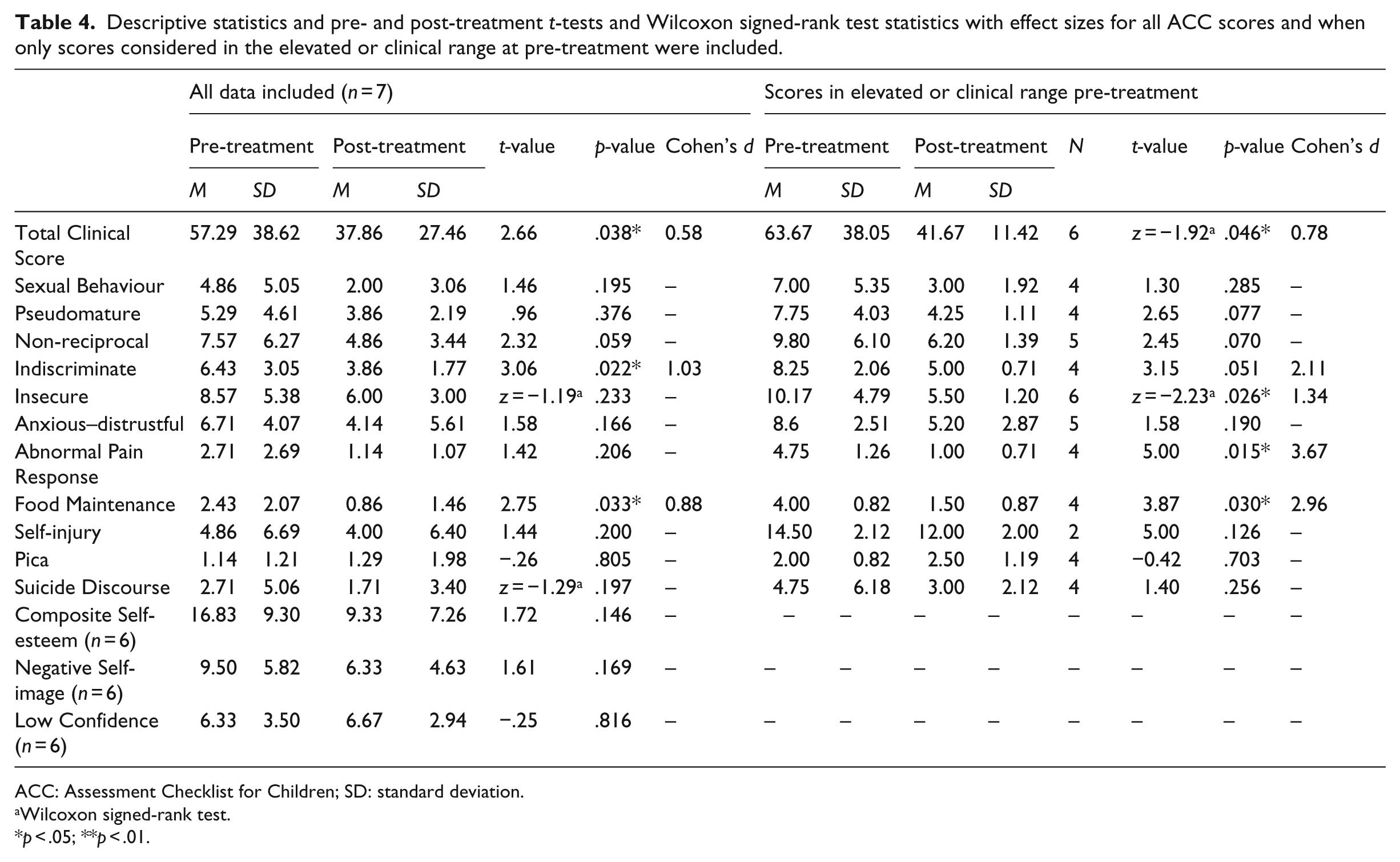
Descriptive statistics, T, Z, p and Cohen’s d values for the ACC scores can be seen in Table 4. When all scores were included in the analysis, Total Clinical Score, Indiscriminate and Food Maintenance scores decreased significantly pre- to post-treatment (p < .05). When only scores which were in the elevated or clinical ranges pre-treatment were included in the analysis, scores for the Insecure and Abnormal Pain Response also decreased significantly and effect sizes increased. The decrease in the score for Indiscriminate moved just out of this significance level.
Descriptive statistics and pre- and post-treatment t-tests and Wilcoxon signed-rank test statistics with effect sizes for all ACC scores and when only scores considered in the elevated or clinical range at pre-treatment were included.
ACC: Assessment Checklist for Children; SD: standard deviation.
Wilcoxon signed-rank test.
p < .05; **p < .01.
CBCL and TRF
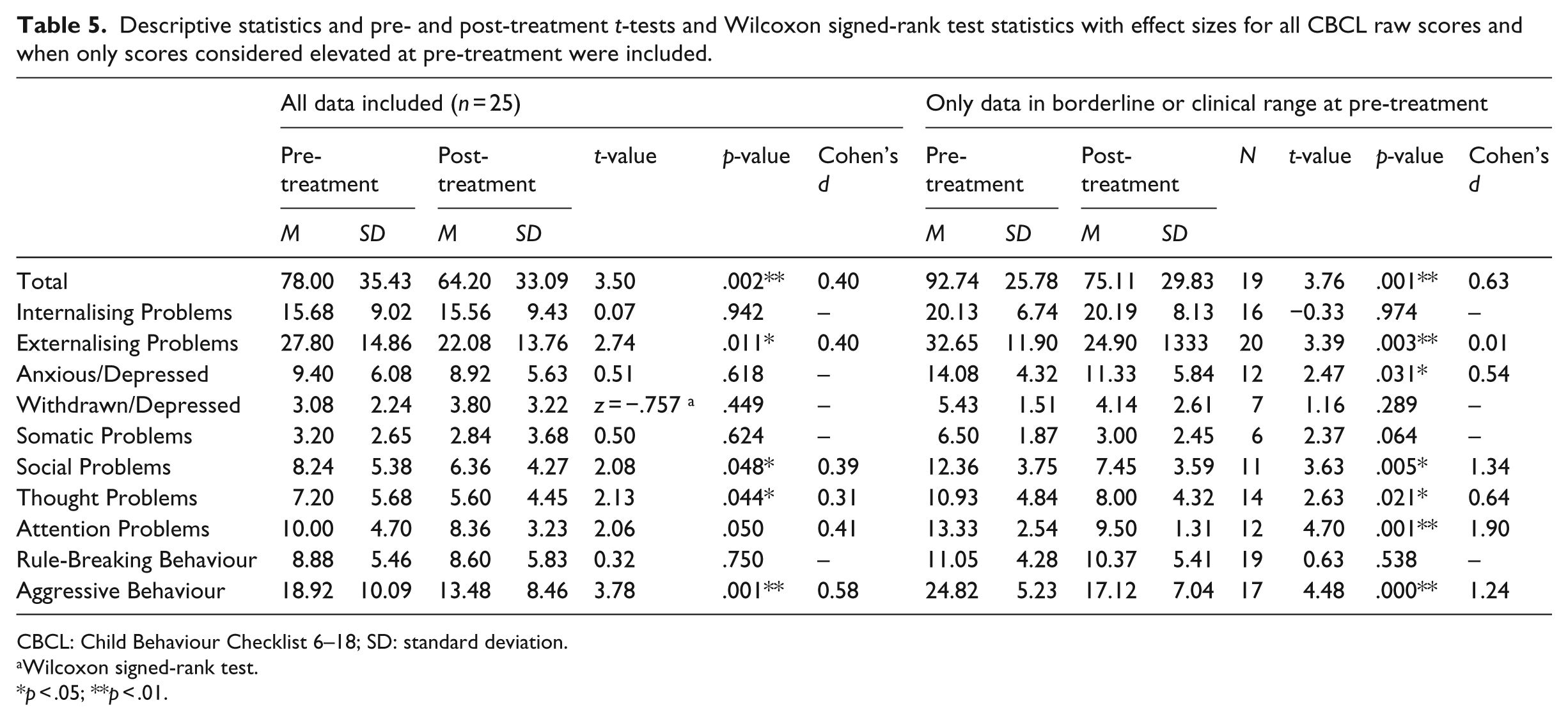
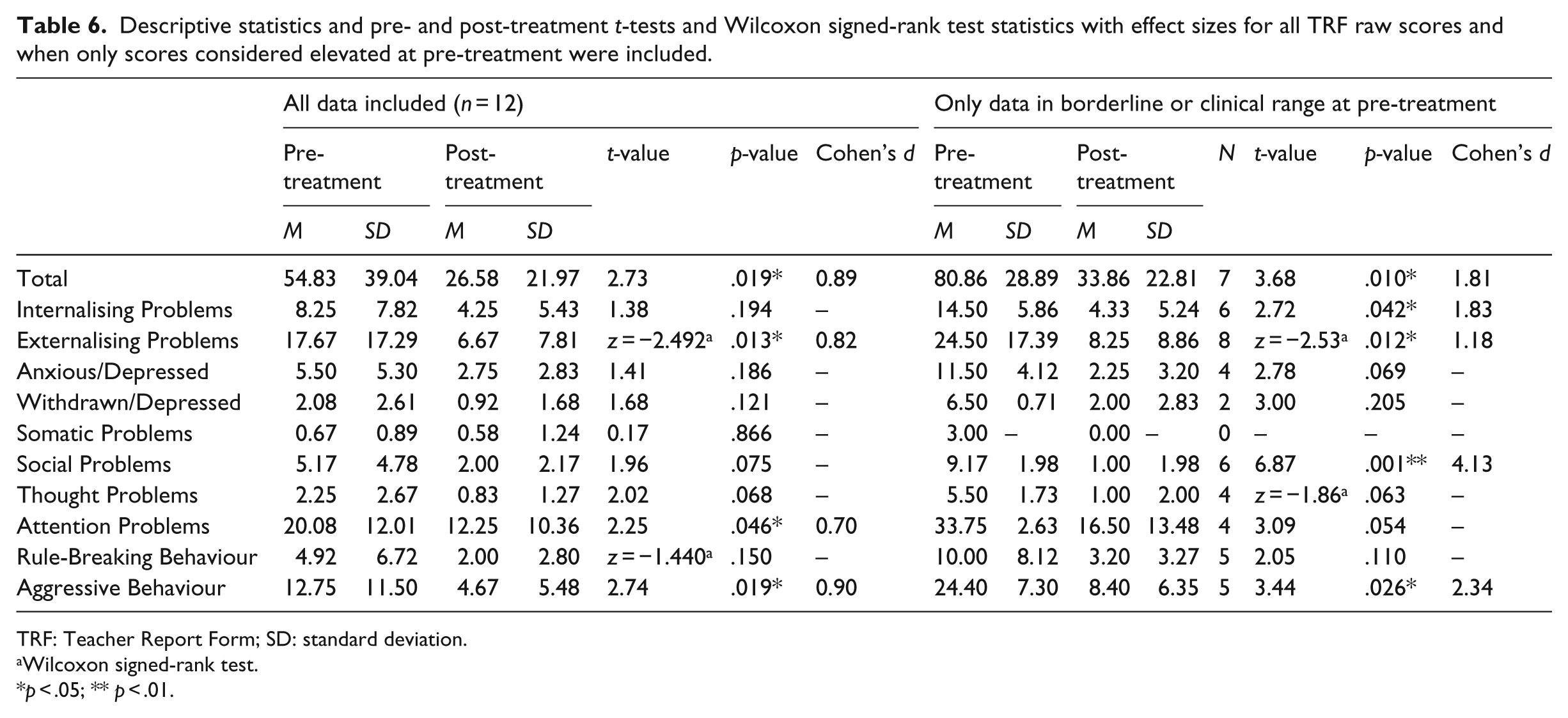
Descriptive statistics, t, Z, p and Cohen’s d values for CBCL and TRF scores can be seen in Tables 5 and 6. When all scores were included in the analysis of the CBCL (parent-completed forms), Total Problems, Externalising Problems, Social Problems, Thought Problems and Aggressive Behaviour reduced significantly (p < .05). When ‘normal’ scores at assessment were excluded from the analysis, decreases in scores for Anxious/Depressed and Attention Problems scales also moved into significance.
Descriptive statistics and pre- and post-treatment t-tests and Wilcoxon signed-rank test statistics with effect sizes for all CBCL raw scores and when only scores considered elevated at pre-treatment were included.
CBCL: Child Behaviour Checklist 6–18; SD: standard deviation.
Wilcoxon signed-rank test.
p < .05; **p < .01.
Descriptive statistics and pre- and post-treatment t-tests and Wilcoxon signed-rank test statistics with effect sizes for all TRF raw scores and when only scores considered elevated at pre-treatment were included.
TRF: Teacher Report Form; SD: standard deviation.
Wilcoxon signed-rank test.
p < .05; ** p < .01.
For the TRF (teacher-completed forms), scores for Total Problems, Externalising Problems, Attention Problems and Aggressive Behaviour significantly decreased after treatment (p < .05). When ‘normal’ scores at the pre-treatment phase were excluded from the analysis, the Externalising Problems and Social Problem scores also decreased significantly (p < .05). The decrease in Attention Problems score neared this significance level.
Semi-structured interview data
Table 7 provides a summary of data from the semi-structured interviews. This provides evidence on the majority report of improved parent/child and child/sibling relationships. In all, 10% of the cohort received further mental health diagnosis with 35% receiving further intervention post-treatment. This took the form of a variety of interventions to infrequent therapy sessions, parent support sessions, family therapy and one-off life story work. Given the breadth of the types of these interventions and the lack of an evidence base for their efficacy, the effect size of these interventions on the outcome is not considered to be great or meaningful. A total of 77% of the cohort remained in mainstream education (including private provision) with 23% in special educational facilities and a total of 55% receiving educational support with 41% having been in receipt of a statement of special educational needs at some point. In all, 77% remained in education without exclusions. While two of the children had been arrested, no formal charges were received, and so 100% of the cohort were without any criminal conviction.
Semi-structured interview data.

CAMHS: Child and Adolescent Mental Health Services; EBD: educational and behavioural difficulties.
Discussion
This study evaluates a family-based integrative neuro-sequential approach to reducing complex emotional, behavioural and executive functioning difficulties in children and young people in adoptive families. The participating children had all experienced significant early life trauma and presented at the time of referral with a range of clinically concerning emotional and behavioural problems as reported by parents and teachers. Significant relationship difficulties were also reported. This study set out to explore where change lay for the children and families at follow-up.
At the time of follow-up, children and young people demonstrated significant change in areas of executive functioning, attachment strategies and emotional and behavioural presentation as reported by parents and teachers.
Analysis of the BRIEF demonstrated significant changes, as reported by parents and teachers, in Global Executive Functioning and Behavioural Regulation (Tables 2 and 3). In the first instance, the children’s increased capacity to engage in behavioural regulation, namely, to inhibit, to shift and to engage in emotional control, is encouraging. Due to the absence of a control group, we cannot attribute pre–post reductions in symptoms as evidence of treatment effectiveness; however, the emphasis of the model on the development of regulation strategies particularly in the early stages of treatment suggests that this may be a possible factor contributing to such significant change. The model integrates sensory, somatic body work and regulation techniques that focus on enabling the child or young person to become aware of their own physiological state, particularly hyperarousal, and teaches them strategies for reducing this. Parents are also encouraged to become detectives of their own and their children’s nervous systems and to act as co-regulators. Further to this, significant change across metacognitive executive functioning based on both teacher and parent report is promising and possibly supportive of a hypothesis that change in a capacity to regulate is necessary as a precursor to other changes. That significant change in the children’s metacognition based on their teacher’s observations of their performance in a school environment which places demand on executive functioning is noteworthy. It may be that, alongside other therapeutic aspects of the programme, the high level of structure and additional-focused support that many of the children receive within school as a consequence of the treatment intervention aid their performance in these areas.
Early results using the ACC, while based on very small sample sizes, are positive and indicate an overall reduction in the total clinical score (see Table 4). As scores on this measure are predictive of mental health difficulties in the population of children and young people in alternative care (Tarren-Sweeney, 2014), this information is extremely promising and could suggest that the intervention may also contribute to change across a range of domains that are common to this population. For this small sample, significant statistical change was found for insecure behaviours and strategies for managing distress (food maintenance), with non-reciprocal and indiscriminate behaviour moving towards statistical significance. This suggests that the children and young people in this sample displayed a reduction in insecure strategies as a way of coping and may have developed alternative, more secure strategies which involved accessing their parents. This claim cannot be substantiated yet but may be borne out by the thematic analysis of the qualitative attachment data at a later date. However, the evidence so far possibly suggests that the underpinning of the tri-part brain-based intervention by attachment-focussed, dyadic therapy may consequently influence the attachment relationship. There is good evidence that early placed children with attachment difficulties develop alternative, more secure representations of their (adoptive) caregivers over time (Hodges, Steele, Hillman, Henderson, & Kaniuk, 2003, 2005). It would make sense that a focus on this area of difficulty in treatment would enhance the child’s ability to internalise the parent as available to them and develop more secure strategies for accessing the parent when under stress.
Outcomes using the CBCL showed a significant reduction in Total Difficulties as reported by both parents and teachers (Tables 5 and 6). Parents and teachers also report significant reductions in externalising difficulties at follow-up and significant reductions in aggressive behaviour.
Teachers report a statistically significant reduction in Total Internalising scores (Table 6). While parent report on Total Internalising Difficulties was not significant, a significant reduction in anxious/depressed symptoms was found (Table 5). An analysis of the children whose internalising difficulties, based on parent report, did not improve did not reveal a pattern to allow for hypothesis formation regarding the lack of significant change found in parent reports of internalising behaviours. Larger study numbers are required.
Parents and teachers also report a significant decrease in children and young people’s social problems and parents report a significant decrease in attention difficulties and thought problems (Table 5 and 6). The reduction in thought problems is of interest particularly to the model of intervention as it is thought that attachment-based strategies used in childhood can lead to more entrenched ways of seeing and organising one’s thinking about others in the world (Tarren-Sweeney, 2013). While, again, this reduction cannot be directly attributed to the therapeutic intervention, the approach posits that through a focus on emotional and physiological regulation and the building of the attachment relationship, the child develops new ways of managing their trauma-related fears and develops alternative templates for relationships, including alternative perceptions of others. While the numbers are currently small, this study lends support to this hypothesis and requires further exploration. However, a reduction in these difficulties is a positive indicator in terms of parent–child relationship and in terms of the child’s ability to engage in learning and more positively in society.
Qualitative evidence from the interviews also lends support to both positive outcomes for the children and parents’ relationships post-treatment. Parents’ high degree of satisfaction with the treatment, particularly the support they received, and their report of improvements in their relationship with their children since engaging in the treatment offer positive support for the model. That a majority of children remained in education, did not access mental health services and were not involved with the criminal justice system is encouraging and may be indicative of the long-term economic benefits of employing such an integrative wrap-around service for children who are adopted or placed for adoption and who present as having a high level of complex needs as a consequence of their early experiences of complex trauma.
This evaluation is particularly encouraging given the high percentage of children who had experienced numerous risk factors for later mental health difficulties and that the average age at which these children presented for treatment was into middle childhood. It also begs the question, ‘What would the outcomes be for children who had similar risk factors if they were offered such a service at time of placement?’ The answer is one that should be considered by all those responsible for the allocation of services to this vulnerable population and those who take on responsibility for their care.
Limitations of the study
While this preliminary evaluation presents data that show significant changes in many areas of cognitive, emotional and behavioural functioning for children post-intervention, the absence of a comparison control group means that we cannot attribute pre–post reductions in symptoms as evidence of treatment effectiveness. This is due to the difficulty of confidently interpreting data in the absence of a control group due to possible systematic respondent bias, regression towards the mean (families are referred to family futures when problems are particularly acute) and the possibility of natural recovery. However, some of the large effect sizes are unlikely to be accounted for by regression to the mean. Only families who received the full treatment model and whose placement did not disrupt were included in the analysis. While only one family who received the full treatment model had a placement disruption, their exclusion from the follow-up may have impacted the findings in a small way had they been included in the analysis.
Further research
This evaluation offers further information about a wrap-around service that provides specialist trauma and attachment-informed interventions to children in alternate care. This is the first evaluation of its kind for this service, and while the numbers are small, they are encouraging. Ongoing follow-up of current families will hopefully lend further weight to this analysis.
Given the positive findings of this exploratory research, a cost-effectiveness analysis could help identify the long-term savings from early investment in this wrap-around service.
Further studies into the effectiveness of the model which would allow attributions regarding treatment effectiveness to be made would involve recruiting a comparison group. For example, it may be possible to recruit families who were assessed by the organisation but who were not funded for a treatment programme. However, considerable ethical constraints may apply, and it is likely that there may be many confounding factors. A randomised controlled trial would ultimately be the most robust form of analysis and would require external funding and inter-agency support. Several theoretical and clinical hypotheses have been raised as a consequence of this practice-based research and discussed in section ‘Discussion’. Further research is required to explore these hypotheses in more detail.
Further research will include analysis of changes in the attachment strategies utilised by children pre and post treatment. This may add further information about the mechanism of change for these children.
Footnotes
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.