
Abstract
Research on early intervention for young children (infants and toddlers) with fetal alcohol spectrum disorders (FASD), particularly children with comorbid maltreatment experiences, is limited. Existing research has primarily focused on structuring environments to be responsive to the needs experienced by children with FASD rather than improving their functioning. The purpose of this study is to present outcomes from an early psychosocial intervention with 10 adopted, maltreated young children diagnosed with FASD, aged 10–53 months (M = 35 months), and their adoptive parents. The potential for early, targeted interventions to improve developmental outcomes for children with prenatal alcohol exposure was examined, as well as improving the skills of and reducing stress experienced by their adoptive parents. Based on the outcomes of a neurodevelopmentally informed assessment protocol, the 10 children whose data are presented were recommended to receive a range of regulatory, somatosensory, relational, and cognitive enrichments. As part of their treatment, children and caregivers received Child–Parent Psychotherapy (CPP), and caregivers (here, adoptive parents) also received Mindful Parenting Education (MPE). Related-samples Wilcoxon signed-rank tests indicated that scores of several measures of child developmental functioning improved from pre- to post-intervention and that parents’ caregiving skills improved while their caregiving stress decreased. Reliable change analyses indicated that change observed from pre- to post-intervention was reliable. The promise of using neurodevelopmentally informed assessment strategies to sequence interventions for young children with diverse neurodevelopmental insults is discussed.
Keywords
Several terms have been used to define the diverse, deleterious, and cascading effects of in utero alcohol exposure, such as fetal alcohol syndrome (FAS; children on the more severe end of the spectrum), partial fetal alcohol syndrome (pFAS), alcohol-related birth defects (ARBD), and alcohol-related neurodevelopmental disorder (ARND) (Institute of Medicine, 1996). Currently, fetal alcohol spectrum disorders (FASD) is most commonly used to describe the range of the constellation of characteristics associated with prenatal alcohol exposure (Astley & Clarren, 2001), including damage to the central nervous system (Riley & McGee, 2005; Streissguth & O’Malley, 2000), facial dysmorphology (Warren & Foudin, 2001), and cognitive (Steinhausen, 1996), psychiatric (Paley & O’Connor, 2009), interpersonal, and psychosocial problems (Niccols, 2007; Roebuck-Spencer, Mattson, & Riley, 1999). May and colleagues (2014) estimated that up to 5% of US first graders have FASD, exhibiting physical, behavioral, or learning deficits, while Fuchs, Burnside, Marchenski, and Mudry (2010) cited studies rating FASD as high as 17% among children involved with child welfare.
The range, complexity, and severity of adverse outcomes of prenatal alcohol exposure (PAE) are well documented (Burd, Klug, Martsolf, & Kerbeshian, 2003). Research on the neurodevelopmental damages associated with FASD (Chasnoff, Wells, Telford, Schmidt, & Messer, 2010) has indicated structural damages to the corpus callosum, brainstem, cerebellum, hippocampus, basal ganglia (Roebuck-Spencer & Mattson, 2004; Sowell et al., 2001), and amygdala (Godel et al., 2000). Data also suggest impairment in basic regulatory functions such as heart rate, respiration, sleep, and sensory processing and integration (Geva & Feldman, 2008; Kodituwakku, 2007, 2009; Mayes, 2000; Stein & Barnes, 2002), which may place children with FASD at risk for later impairment in advanced developmental functions such as executive functioning (Niccols, 2007; Rasmussen, 2005) and social and emotional skills (Barkley, 2001). Unsurprisingly, over 90% of children with heavy PAE meet criteria for attention deficit hyperactivity disorder compared to 9% of intelligence quotient (IQ)-matched peers (Fryer, McGee, Matt, Riley, & Mattson, 2007), and 15–20% exhibit intellectual disabilities, 25% learning disorders, 30% speech and language disorders, 30% sensory impairment, 4% cerebral palsy, and 8–10% epilepsy (Burd et al., 2003).
The clinical picture of FASD is sometimes further complicated by the presence of other risk factors, such as child abuse and neglect. Children with developmental disabilities such as FASD are approximately three times more likely to be abused or neglected during early childhood than typically developing children (Kelley, 1992; Sullivan & Knutson, 2000), placing them at risk for attachment and psychosocial problems (Beeghly & Cicchetti, 1994). Reasons for this increased susceptibility for maltreatment may include their unpredictable emotional dysregulation (e.g. highly withdrawn, reactive to environmental stimuli; Bjorkquist, Fryer, Reiss, Mattson, & Riley, 2010; Jan et al., 2010) and a higher probability that mothers who abuse substances have limited positive parenting skills (Chronis, Chacko, Fabiano, Wymbs, & Pelham, 2004; Suchman, Pajulo, DeCoste, & Mayes, 2006). Many children with FASD have difficulties with interpersonal, psychosocial, and relational functioning, possibly due to altered neurodevelopment and impaired attachment experiences early in life (Jacobson & Jacobson, 2003).
The cost of FASD to society is vast and growing. In 1998, Harwood estimated the financial cost of FASD to be well over 4 billion dollars per year, and 2015 estimates reach 6 billion (Popova, Lange, Burd, & Rehma, 2015). The costs are potentially even greater if the child enters the child welfare system (Popova et al., 2015) and when accounting for debilitating comorbid concerns (Olson et al., 2009). The need for effective treatment for children with FASD, particularly with comorbid maltreatment histories, is imperative. Yet, the chronic, diverse, and cascading negative outcomes associated with FASD and maltreatment combined make it difficult to identify primary targets of treatment. As such, treatment for FASD has typically consisted of combining multiple treatment approaches to alleviate a diverse array of presenting problems (Paley & O’Connor, 2011; Pelech, Badry, & Daoust, 2013). Such treatments include behavioral therapy (Paley & O’Connor, 2011), psycho-pharmacological treatment (typically stimulant medication) for behavior problems and/or problems with sustained attention (Paley & O’Connor, 2011, social skills training (Brown & Bednar, 2004), and school-based interventions for learning problems (Streissguth & Kanter, 1997). Other treatments have focused on accommodating the child’s environment to meet their individualized needs (e.g. decreasing the number of transitions in the school day, decreasing the length of time spent in the regular classroom, or decreasing homework and chores) and providing psychoeducation to teachers and caregivers (Burd, 2007).
Although the aforementioned treatments often result in treatment gains (Paley & O’Connor, 2011; Zevenbergen & Ferraro, 2001), these gains may not hold up in environments with fewer accommodations or throughout development. Developmental transitions are often coupled with a resurgence of symptoms or even the onset of new symptoms in children with FASD (Autti-Rämö, 2002), requiring the child and/or family to remain in or return to treatment. Continued, significant functional impairment in many children with FASD despite their engagement in oftentimes long-term, time-consuming, and expensive treatments highlights the need to investigate interventions that have the promise of resulting in enduring, global change.
Early intervention for children with FASD that is focused on strengthening developmental functioning and repairing neurobiological deficits could possibly result in long-lasting treatment gains (Autti-Rämö, 2002). The first few years of life have been consistently documented as critical and sensitive periods for learning because during these years, children exhibit experience-induced brain plasticity (Shonkoff & Garner, 2012). Thus, these early years provide a window of opportunity for acquiring building blocks of developmental functions such as psychosocial skills (e.g. interpersonal relations, attachment to primary caregivers, and ability to interpret social cues) (Kaiser & Rasminsky, 2007), intellectual abilities, and language acquisition (Uylings, 2006). Research has begun demonstrating the utility of intervention with young children, such as the use of infant massage and sensory integration techniques in Occupational Therapy (Field, 1995), and psychomotor training for children with developmental delays (Klintsova et al., 2002).
Neurodevelopment is “use-dependent,” and all of the functions related to the neurotypical organization of the brain are influenced by the nature, pattern, and timing of early life experiences (Perry, 2002). The high malleability of these developing neural networks in the first years of life makes early intervention relatively more effective in shaping key functional capabilities (Lillas & Turnbull, 2009). Because children with FASD typically struggle with multiple developmental functions—including regulatory (self-soothing/self-regulation, sleep–awake pattern, and feeding; Premji, Serrett, Benzies, & Hayden, 2004); somatosensory (sensory integration and somatosensory processing; Morse, Miller, & Cermak, 1995); relational/psychosocial (attachment, peer, and adult relations; Frankel, Paley, Marquardt, & O’Connor, 2006); psychomotor (perceptual, vestibular, fine, and gross motor; Lillas & Turnbull, 2009); and cognitive (attention, memory, perception and concepts, problem solving, speech and language, and learning skills; Gibbard, Wass, & Clarke, 2003), that is, domains that begin to form during the first few years of life (Lillas & Turnbull, 2009)—early intervention is particularly important in this population. Unfortunately, little treatment outcome research has been conducted with children with FASD under the age of 5 years (Paley & O’Connor, 2011; Zevenbergen & Ferraro, 2001).
The Neurosequential Model of Therapeutics
The Neurosequential Model of Therapeutics (NMT) was chosen as an approach to clinical problem solving, in the hopes that through use of the NMT, children with FASD would receive intervention that could lead to broad developmental improvements. The NMT was designed to help providers make clinical decisions based on knowledge of a child’s current developmental functioning given their unique developmental insults. As part of this approach, a set of metrics is used to evaluate the client’s developmental history and current functioning. The NMT developmental history assessment examines the nature, timing, and intensity of developmental adversities (e.g. maltreatment and prenatal, perinatal, and postnatal history) and relational health factors (e.g. relational connection to caregiver, community supports). The NMT assessment of current functioning helps generate a “picture” of the developmental strengths and vulnerabilities of the client. This neurodevelopmental viewpoint, in turn, allows the clinical team to select and sequence a set of enrichment, educational, and therapeutic interventions to best match developmental needs in multiple domains of functioning.
The NMT was created to integrate biological, psychological, social, learning, and problem-solving aspects of a child’s development into one coordinated intervention plan and thus was expected to be a useful tool when planning interventions for young children with FASD. In this study, NMT is used as a data-organizing tool, providing recommendations for the clinicians using the NMT Metric scores obtained for the child through comprehensive assessment and evaluation processes (initial assessment, tests and measures, and historical data) on each of the four developmental domains: (a) regulatory system (self-soothing/self-regulation, sleep–awake pattern, and feeding); (b) somatosensory system (sensory functions, integration, and somatosensory processing); (c) relational system (attachment, psychosocial, interpersonal, peer, and adult relations); and (d) cognitive/cortical system (attention, memory, perception and concepts, problem solving, speech and language, and learning skills). As NMT is not an intervention, the assessment helps determine the selection and sequencing of intervention elements.
In this sample, some idiosyncratic intervention elements were employed given a child’s specific outcomes of their NMT assessment (e.g. infant massage 5–10 minutes three times a day, using soft or hard pressure as suitable for the individual child; rhythmic, patterned, and repetitive activities, such as gentle rocking or movements to rhythmic music; supported movements back and forth on a large exercise ball, blowing bubbles, or “smell the flower–blow the candle” to help with deep breathing; using balls made with soft material to play catch-throw or using wet/dry sand and other textured material during play time to address somatosensory challenges). Also, two evidence-informed interventions that contained elements that could address a vast amount of deficits across all of the children were delivered to each child. One approach was Child–Parent Psychotherapy (CPP; Lieberman, Van Horn, & Ghosh Ippen, 2005), which contains a range of specific parent–infant interactive elements that address relational and cognitive developmental domains in infants and toddlers (e.g. talking to the child, reading to the child, and reflective listening). The other was Mindful Parenting Education (MPE; Bögels, Lehtonen, & Restifo, 2010), which was selected to address parents’ regulatory challenges as it helps caregivers develop consistent and predictable patterns of responding to the needs of children with challenging behaviors (Pears, Kim, Healey, Yoerger, & Fisher, 2015).
CPP
CPP is an evidence-based, relationship-focused, reflective, and developmentally oriented model of psychotherapy. It is especially suitable for young children similar to the children in this study—with histories of trauma, maltreatment, and associated problems with attachment, behavior, self-regulation, and posttraumatic stress (Ghosh Ippen, Harris, Van Horn, & Lieberman, 2011; Lieberman & Van Horn, 2008; Lieberman et al., 2005, 2006). It was chosen over other similar approaches, such as Attachment and Biobehavioral Catch-Up (Dozier, Peloso, Lindhiem, Gordon, & Manni, 2006), given that it has been shown to improve the attachment relationship and symptoms of posttraumatic stress in young children (Lieberman & Van Horn, 2008; Lieberman et al., 2005, 2006).
CPP utilizes caregivers as the agents of change. Child–parent dyads/triads were seen together and received CPP-based intervention twice per week. CPP can be flexibly administered given the child’s age, trauma history, and caregivers’ functioning. It has been shown to improve outcomes in several domains through five randomized controlled trials, including attachment security, behavior problems, and posttraumatic stress (Lieberman, Silverman, & Pawl, 2000). In this study, it was hoped that CPP could particularly ameliorate relational and cognitive deficits through helping improve the caregiver–child attachment relationship.
MPE
Consistent and predictable parenting is associated with improved regulatory skills in young children (Pears et al., 2015). Thus, aspects of MPE (Bögels et al., 2010; Duncan & Bardacke, 2010) were used to supplement CPP and somatosensory interventions. A reflective, interpersonal model for psychoeducation and parenting, the MPE model was chosen for its emphasis on promoting caregiver self-reflection and intentional mindfulness of their own and their child’s experience while maintaining a sense of compassion and empathy toward the child (Bögels & Restifo, 2014; Siegel, 2003, 2007; Siegel & Hartzell, 2003). This approach was chosen over other efficacious parenting approaches (such as the Positive Parenting Program; Sanders, 2003) and added to CPP, which already confers parenting skills, given this specific emphasis on mindfulness. The hope was that mindfulness strategies would promote caregiver self-regulation and help caregivers model self-regulatory skills to children.
When faced with the daily challenges of parenting a young child with FASD, many parents may feel emotionally overwhelmed and physically exhausted. Caregiver education sessions were conducted once per week throughout the intervention period. During these sessions, caregivers’ concerns and questions related to parenting their children were addressed and components of MPE were delivered. Parents received psychoeducation regarding FASD and their child’s self-regulation; sensory, social, relational, emotional, and cognitive development and behavioral issues; and guidance on how to work through their own feelings and emotions while dealing with them. The MPE sessions were to improve caregivers’ understanding of the regulatory challenges of their adopted children with FASD while reducing stress through promoting caregiver attainment of self-regulation, parenting skills, and their sense of parental self-efficacy.
Current study
The goal of this study is to describe the NMT-directed selection of an early intervention protocol for young children with FASD with comorbid experiences of maltreatment or loss and to present the developmental outcomes of these children after 6 months of intervention. It was hypothesized that using an assessment and intervention planning process aimed toward identifying the broad neurodevelopmentally mediated problems experienced by young, maltreated children with FASD would help to identify interventions that would improve developmental outcomes in children.
Method
Participants
Participants were recruited from treatment referrals received from various referral sources in 2012 to an outpatient community mental health program in Southern California, including but not limited to pediatricians, family physicians, or other outpatient mental health providers. To meet criteria, children (a) need to be 5 years of age or younger, (b) need to be in the care of their adopted families for 6 months, (c) have been given a diagnosis of FASD by a medical provider, (d) have a history of maltreatment or loss, (e) should not be taking psychotropic medications, (f) should not have an additional genetic syndrome, (g) should not have active grand-mal epileptic seizures, (h) should not have a history of serious head injury, (i) should not meet criteria for profound intellectual disability, and (j) have adoptive caregiver(s) who could fully engage in the intervention process during the study time period and who could complete measures in English.
From a total set of 38 young children and their adoptive families who were referred and agreed to participate in the study, only 15 met inclusionary criteria. Ten of these 15 children completed six consecutive months of treatment intervention, some of whom completed a 1-year treatment period. Due to the smaller sample size at the end of the year, data from the first 6 months were used for this pilot study.
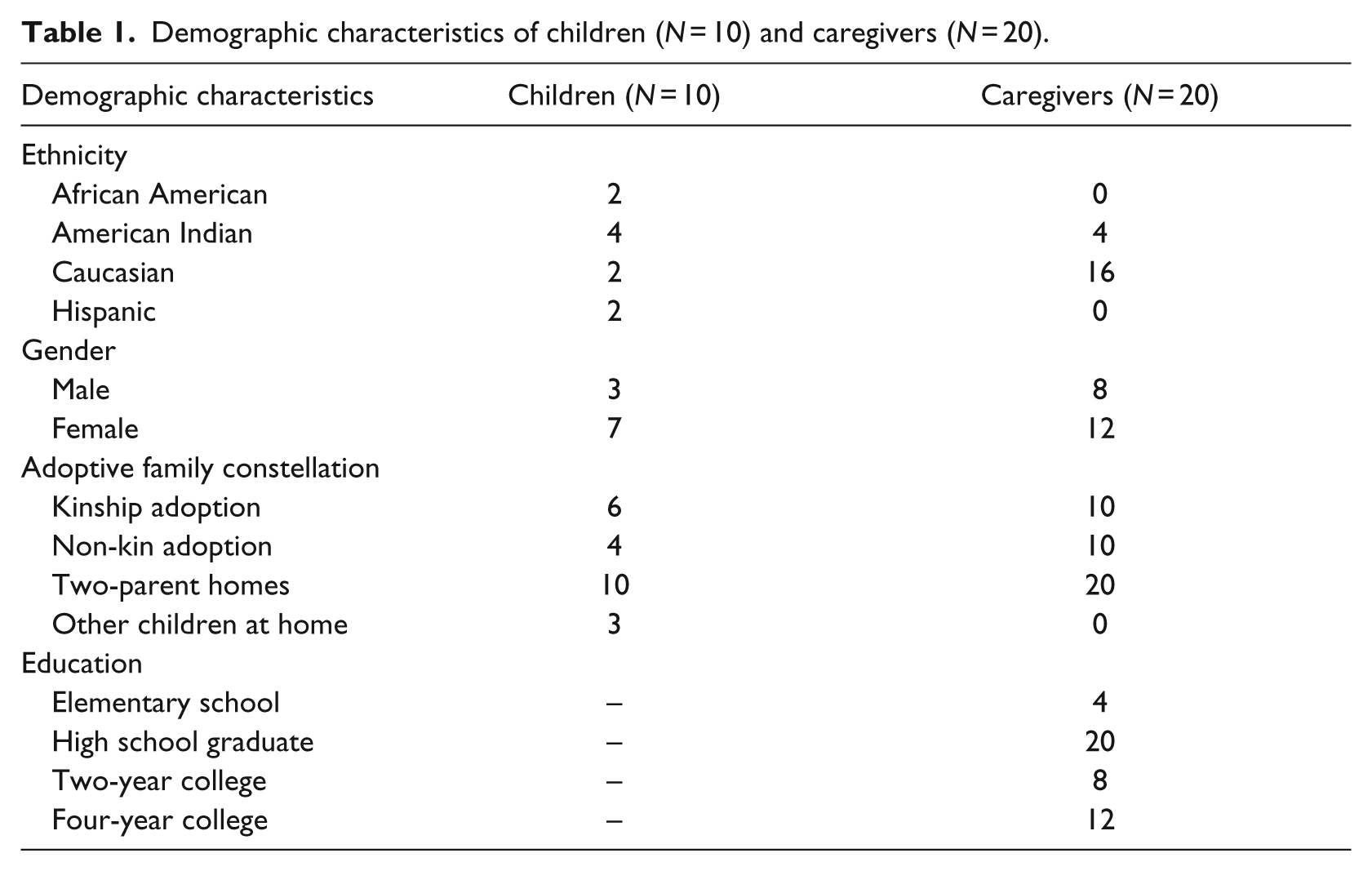
All adoptive families in the study were two-parent, English-speaking families. Half of the adopting caregivers were blood relatives of the children they adopted, and the majority of the adoptive caregivers were Caucasian (N = 16; 80%). All caregivers denied history of illicit drug use or serious medical and/or psychiatric problems. Caregivers’ ages were between 32 and 58 years, and all had been in a steady relationship with a partner/spouse for a minimum of 5 years. Children’s ages ranged from 10 to 53 months. Comprehensive demographic characteristics of children and their adoptive parents are provided in Table 1.
Demographic characteristics of children (N = 10) and caregivers (N = 20).
Therapists
Three licensed PhD and master’s level clinicians with general training in early childhood mental health and specific training in CPP, MPE, and NMT delivered the interventions under the supervision of a licensed pediatric psychologist (the primary investigator). The primary investigator was trained by Lieberman and Van Horn (2008) and Lieberman, Chu, Van Horn, and Harris (2011) on CPP; Siegel (2003, 2007) on Mindful Parenting; and Perry (2006, 2008) on NMT. In order to use the NMT Metrics, there is a manualized NMT Certification Process (90 hours of didactic, multimedia, and case-based training to ensure exposure to core concepts of traumatology, developmental psychology, neurobiology, and related areas relevant to a developmentally sensitive and trauma-informed approach). There is a maintenance training component and a bi-annual NMT Fidelity exercise to determine and maintain acceptable and high inter-rater reliability on the NMT Metrics. The primary investigator has completed all certification processes and conducts NMT training and mentoring to mental health, education, child welfare, and the juvenile court system professionals. The primary investigator ensured therapists’ fidelity to the interventions by didactic training, case conferencing, and individual and group mentoring of those involved in the intervention process.
Measures
Battelle Developmental Inventory, Second Edition
The Battelle Developmental Inventory, Second Edition (BDI-2) was completed by clinicians based on information obtained from the BDI-2’s structured, observational, and interview tasks (Newborg, 2005). The BDI-2 takes 60–90 minutes to complete. It assesses developmental skills in children aged birth to 8 years within five domains: Personal/Social, Adaptive, Motor, Communication, and Cognitive. The BDI-2 was standardized on a normative sample of 2500 children, and the strong psychometrics of the tool have been established (e.g. Internal consistencies ranging from .98 to .99; Newborg, 2005). A total BDI-2 score (comprising all five domains) evidenced a Cronbach’s α of .96 in this study.
Parenting Stress Index, Short Form
The Parenting Stress Index, Short Form (PSI-SF) is a 36-item parent-report measure of parenting stress (Abidin, 1990). It has been used to assess stress in diverse and high-risk parent populations, including foster mothers of prenatally drug-exposed children (Kelley, 1992). This scale provides a total score of parenting stress and three subscales: Difficult Child, Parent Distress, and Parent–Child Interaction. Internal consistencies have been cited as ranging from .88 to .95 (Reitman, Currier, & Stickle, 2002). The PSI Total evidenced a Cronbach’s α of .96 in this study.
NMT measures (NMT Metrics)
The NMT Metrics provide estimates of a child’s functional capacity in four domains: sensory integration, self-regulation, relational and cognitive, as well as an estimate of executive functioning, the Cortical Modulation Ratio (CMR) (Perry, 2006). The CMR provides a crude indication of the “strength” of cognitive regulatory capacity relative to the “dysregulation” (i.e. disorganization, under-development, and impairment) of lower networks in the brain; in essence, it is an estimate of how hard it is for an individual to use cortical (top-down, executive functioning) mechanisms to self-regulate. This factor is related to the executive function and “self-control” indicators (Moffitt et al., 2010; Piquero, Jennings, & Farrington, 2010) known to be predictive of positive outcomes in high-risk children. The higher the CMR value, the “stronger” the cortical mechanisms of self-control.
The NMT Metrics provide information that helps the clinical team select and sequence therapeutic, educational, and enrichment activities that are developmentally appropriate. Thus, the NMT is not a specific therapeutic technique or intervention, but serves to help clinicians select the right interventions, for the right child, at the right time given that child’s neurodevelopmental strengths and weaknesses. Importantly, there is a focus on sequencing interventions that first address functional impairments associated with a child’s deficits originating lower in the brain, such as with self-regulation or self-soothing, prior to having the child engage in interventions that address deficits related to dysfunction in higher areas of the brain, such as cognitive processing (Perry, 2014).
Procedures
The legal guardian(s)/adoptive parents of each child whose family accepted the invitation to join the study completed comprehensive informed consent and assent forms during the initial contact session. A local Institutional Review Board approved the methods of this study (blinded for review). Potential participants were informed that they would receive the same type of intervention whether or not they participated in the research study. The primary clinician assigned to each family obtained pre- and post-intervention data through multiple means, including direct interview with adoptive parents, biological parent(s)/kin, and other collaborators such as each child’s pediatrician following obtaining written consent from each child’s legal guardian (in this case, each child’s adoptive parents). Additionally, the child’s primary caregiver completed standardized measures before and at the end of the 6-month intervention interval. See Figure 1 (Consort Diagram) for more information on study procedures.
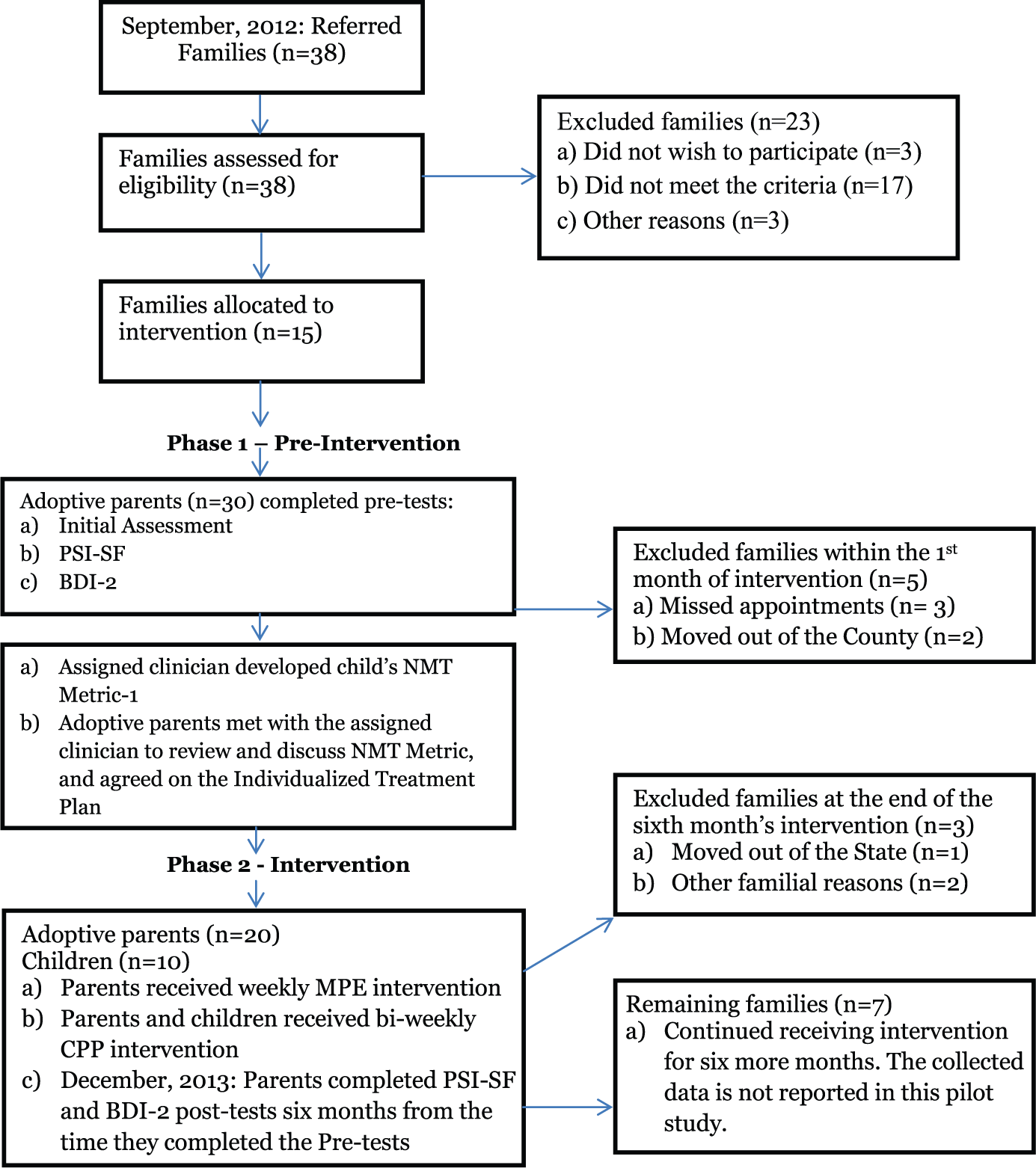
CONSORT flow diagram of the participants’ progress during the course of the study.
Results
Design and analysis
A window of 6 months was chosen for follow-up so that at least 10 children could be assessed at the same time point—prior to a significant amount of families attriting from or completing treatment. First, descriptive statistics were obtained. Then, whether or not changes observed from pre- to post-intervention were reliable was assessed using the Reliable Change Index (RCI; Jacobson & Truax, 1991). Finally, a series of related-samples Wilcoxon signed-rank tests were conducted in IBM SPSS Version 23 to detect changes from pre-intervention to post-6 months of intervention on the BDI-2, PSI-SF, and NMT metrics. At the end of the 6 months, the intervention process for all children and adoptive caregiver(s) still in treatment continued. Data for the children and adoptive caregiver(s) who could not continue their treatment before the end of 6-month period were excluded, as it was not expected that there could be measurable changes in children’s developmental functioning in a timeframe shorter than 6 months. The data for the rest of the families, who continued receiving treatment intervention beyond the 6-month time period, are not included either due to the shrinking sample size.
In the 6-month time interval, caregivers completed a “parent satisfaction survey questionnaire” which was created for this study to informally assess satisfaction. Eighteen out of twenty caregivers reported “yes,” that is, they had improved in their parenting capacities as compared to baseline on each of the following prompts: (a) identifying the needs of these young children in their care (reading their cues), (b) understanding the reasons behind children’s behaviors, (c) identifying their own feelings and emotions triggered by children’s behavior, (d) becoming more aware of their verbal and nonverbal actions and the impacts they may have on calming or exacerbating children’s “misbehavior,” (e) expressing compassion and empathy toward these children whom they used to call “difficult-to-manage” children just 6 months before, and (f) have learned a “new way of being” in the world. Caregivers were also given the opportunity to comment on improvements that could be made. The highest rated request (17/20 = 85%) was to have more frequent collateral contacts than once a week with the therapists to have increased chances for learning and problem solving.
Descriptive statistics
At baseline, each of the 10 children who completed this study had NMT metric scores that indicated clinically significant deficits in all four functional domains (Sensory Integration, Self-Regulation, Relational-Psychosocial, and Cognitive) and the CMR. In addition, all parents had PSI-SF scores indicating clinically significant parenting stress. Mean values, standard deviations, and ranges of the NMT Metrics, BDI-2, and PSI-SF at pre- and post-intervention are given in Table 2.
Descriptive statistics of measures.

M: mean; SD: standard deviation; BDI: Battelle Developmental Inventory, Second Edition (BDI-2 Total Score comprises Interpersonal/Social, Adaptive, Motor, Communication, and Cognitive subscales); PSI-SF: Parenting Stress Inventory, Short Form (PSI-SF comprises Difficult Child, Parent Distress, and Parent–Child Interaction subscales); NMT: Neurosequential Model of Therapeutics (NMT Total Score comprises Sensory Integration, Self- Regulation, Relational, and Cognitive subscales).
All data are in percentages.
Tests of reliable change from pre- to post-intervention
To assess for reliable change in participants’ scores from pre- to post-intervention, an RCI was conducted for each participant (Jacobson & Truax, 1991) on the NMT Total Score, the BDI-2 Total Score, and the PSI-SF. Results suggest that for each participant, change from pre- to post-intervention was reliable on each scale (Figure 2), as evidenced by an RCI score of over 1.96 (meaning that it is unlikely that the change observed was due to fluctuations as a result of the use of imprecise measurements).
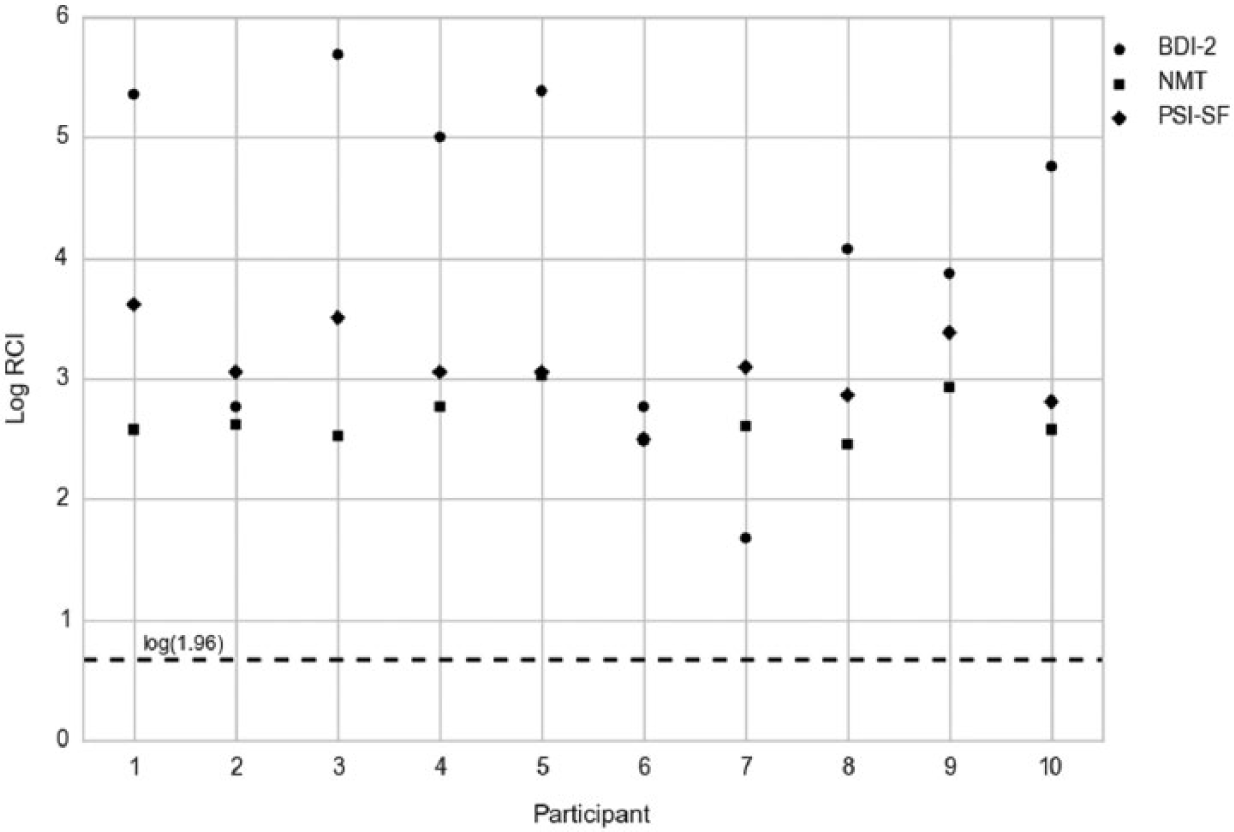
Reliable change of participant scores from pre- to post-intervention.
Tests of significant changes in mean scores from pre- to post-intervention
To assess whether the changes in mean scores on each measure across all participants were significant from pre- to post-intervention, a series of related-samples Wilcoxon signed-rank tests were conducted (Table 3). Wilcoxon signed-rank tests were conducted instead of traditional analysis of variance tests to manage the non-normal distributions of scores across the 10 participants in this pilot study. Results indicated improvements from pre- to post-intervention on the BDI-2 Total score, PSI-SF Total score, the NMT Total score, and the NMT CMR. All effect sizes were large.
Pre- and post-intervention related-samples Wilcoxon signed-rank tests (N = 10).
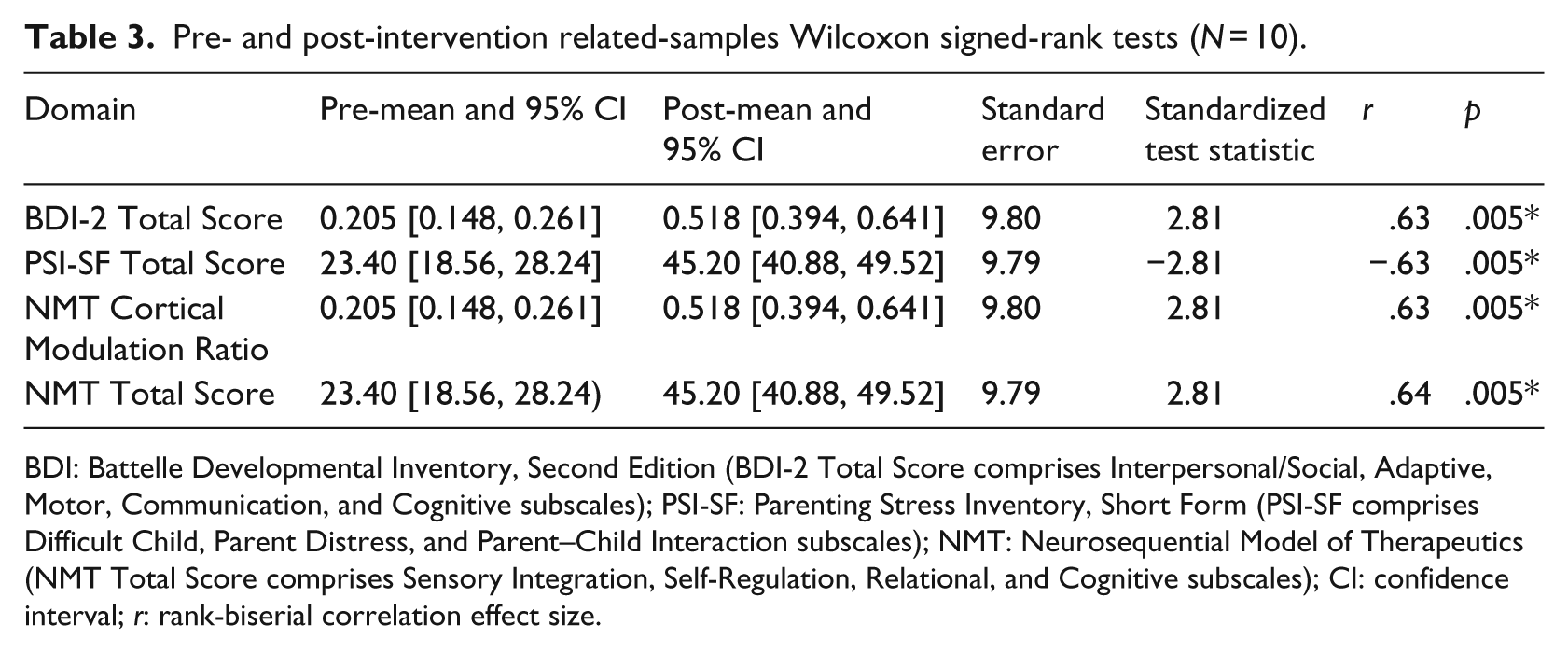
BDI: Battelle Developmental Inventory, Second Edition (BDI-2 Total Score comprises Interpersonal/Social, Adaptive, Motor, Communication, and Cognitive subscales); PSI-SF: Parenting Stress Inventory, Short Form (PSI-SF comprises Difficult Child, Parent Distress, and Parent–Child Interaction subscales); NMT: Neurosequential Model of Therapeutics (NMT Total Score comprises Sensory Integration, Self-Regulation, Relational, and Cognitive subscales); CI: confidence interval; r: rank-biserial correlation effect size.
Discussion
The goal of this study was to determine the potential utility of neurodevelopmentally informed intervention in a real-world setting with young children with FASD. The 10 children in this study entered treatment with a broad range of developmental deficits, similar to those observed in other children with FASD and histories of maltreatment (Burd et al., 2003). Statistically, children’s functioning significantly improved from pre- to post-intervention in several developmental domains, suggesting that early intervention that is tailored to children’s neuropsychological strengths and deficits may hold promise for promoting global improvements that could lead to lasting change. For example, improvement was observed on the BDI-2, indicating that children’s adaptive, motor, communication, and cognitive skills may have improved in a short amount of time. Improvement was also observed in caregivers’ self-reports of parenting stress reduction on the PSI-SF, indicating that parents’ general distress and their distress regarding the parent–child interaction decreased. Finally, although research has yet to validate the psychometric properties of the NMT Metrics, similar outcomes were seen with these metrics, indicating that children improved in cognitive, relational, sensory integration, and self-regulation domains, as well as in their abilities to modulate reactions to internal stimuli using more advanced top-down processing skills. Notably, these observed changes were reliable and not only an artifact of the use of imprecise measures. It should also be noted that improvements were observed in measures from multiple reporters (both clinician and parent report).
Although there are limitations to the generalizability of these findings, the findings are promising for several reasons. First, there has heretofore been a paucity of research on early intervention with children with FASD. Second, these interventions were focused on improving children’s developmental skills through improving their attachment relationships and caregivers’ skills instead of modifying children’s environments to meet their needs (Paley & O’Connor, 2011; Zevenbergen & Ferraro, 2001)—suggesting that more than one intervention method may be useful with this population. Third, these data were collected in a real-world setting, where there are significant challenges to engaging children and families in interventions. Children with FASD, like children with other disabilities, are at high risk of abuse, neglect, and repeated child welfare involvement. One major positive outcome of the treatment intervention applied in this pilot study appears to be improved child–caregiver relationships among children and their adoptive parents—potentially making them less at risk for future child welfare involvement.
One highly interesting finding was that children’s cognitive abilities, as measured by the BDI-2 and NMT Metrics, appeared to improve. This is surprising as previous researchers have speculated whether neurocognitive deficits due to alcohol exposure can be improved upon (e.g. Kodituwakku, 2009). We would suggest that some of the improvements in cognitive functioning seen over the 6 months were related to improved self-regulation. Both cognitive development and cognitive functioning are significantly influenced by internal state; anxiety, hunger, fear, and other “states” of dysregulation will impair cognitive functioning. With improved regulation, then, comes improved cognition. With the small numbers of children and the relatively brief period of intervention observed, it is difficult to determine whether the improved cognitive functioning was reflective of a shift in state or a true improvement in cognitive capabilities (Perry, Pollard, Blakley, Baker, & Vigilante, 1995).
Moreover, the extent to which findings from this study, with a small sample size, a short outcome evaluation window, and no control group, would generalize to the population of young children with FASD is unknown. The small sample size precluded analysis of covariates, such as age or severity of pre-intervention developmental problems. The short evaluation window precluded analysis of long-term impact. And, without a control group, it is difficult to infer that results were due to actual change beyond simple regression toward the mean or change attributable to the intervention, not just spending 6 months in a stable adoptive home.
However, research regarding the frequency with which children with FASD change adoptive and foster placements due to their difficult temperaments (Pelech et al., 2013) would suggest that without intervention, even remaining in a stable environment is a rare occurrence for children with such profound developmental challenges. In addition, this sample was homogeneous—a sample of 10 children 1–5 years old with FASD and histories of maltreatment who were currently living in adoptive homes. Finally, the change from pre to post was judged to be reliable, and the effect sizes of pre-post analyses were large. This suggests that once very young children with FASD have entered a stable caregiving environment, early, relationally based, neurodevelopmentally focused, comprehensive intervention that involves improving the attachment relationship and caregivers’ skills might be a promising mechanism for improving a broad range of skills even in this high-risk, difficult-to-treat population.
Future directions
Despite the noted limitations, the positive outcomes of this pilot study suggest the need for more research on neurodevelopmentally informed early intervention for children with FASD, potentially as guided by use of the NMT. Longitudinal studies of children who receive early intervention as part of a controlled trial would be most beneficial as they would confirm whether or not early, neurodevelopmentally informed intervention can truly strengthen and repair neurobiological systems that are associated with the chronic and cascading difficulties associated with FASD throughout the lifespan (Autti-Rämö, 2002). In addition, there is a need for larger samples so that children who receive different intervention plans that are neurodevelopmentally informed can be evaluated. Moreover, larger samples would help clarify whether gains in this study were due to the use of CPP and MPE alone or whether they can also be attributed to the use of a neurodevelopmental intervention planning framework. Young children with FASD are a vulnerable, costly population that typically experiences a low quality of life. The current findings provide support for the promise of neurodevelopmentally informed intervention as a mechanism of promoting developmental improvements for young children.
Footnotes
Acknowledgements
Authors thank all families whose valuable participation made this pilot study possible. We also thank the clinicians at the Child Health Integrated, including Parissa Ahmadi, PhD, Debbie Espinoza, MSW, Parvin Osanloo, MSW, and Paula Santos, PhD, for their valuable contributions, without which this study would not have been completed.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. We also would like to thank Dr. Alicia Lieberman, PhD, for her support and guidance.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: All the expenses for services provided for the families included in this study were provided through fee-for-service process in place at the community mental health clinic where this pilot study was conducted. Dr Hambrick (not the clinical work or research project) was supported by T32MH015442 during the preparation of this report.