
Abstract
Background:
With the number of children being placed in the care of local authorities increasing, the need to recruit and retain foster carers is essential. Compassion fatigue is recognised as a negative effect for professionals working with adults and children who have experienced trauma. This study aims to confirm the proof of concept within foster carers and to explore the potential risks associated with intent to continue fostering, overall job satisfaction and psychological factors (avoidant coping) that could be targets for interventions.
Methods:
In total, 131 foster carers completed an online survey including self-report measures of compassion fatigue and associated risk factors.
Results:
Results confirm the existence of compassion fatigue among foster carers with rates in line with previous studies on other professionals working with children. High compassion fatigue was associated with lower intent to continue fostering and lower job satisfaction. Avoidant cognitive styles of psychological inflexibility and thought suppression were associated with compassion fatigue.
Conclusion:
The confirmation of compassion fatigue among foster carers and the potential risks to job retention are important findings for social care. The associations with avoidant cognitive styles have clinical implications for potential interventions. Recommendations for further research and the limitations of this study are also discussed.
According to the Department for Education (2016) in the United Kingdom, 69,540 children were in the care of local authorities on 31 March 2015, with 75% (52,050) of these children living with foster carers. With numbers of children being taken into care increasing, and social care being faced with a growing shortage of foster carers (Harber, Oakley, & Exchange, 2012; Rodger, Cummings, & Leschied, 2006), the need to recruit and retain foster carers is essential. Research shows that foster carers report high levels of stress related to their role (Murray, Tarren-Sweeney, & France, 2011; Vanschoonlandt & Vanderfaeillie, 2013; Whenan, Oxlad, & Lushington, 2009). The typical stressors faced by foster carers include placement disruptions, allegations, difficulties with social services and contact with birth families (Wilson, Sinclair, & Gibbs, 2000). High levels of strain are associated with a foster carers’ overall job satisfaction and intention to quit (Farmer, Lipscombe, & Moyers, 2005). In addition, a recent review highlights the impact of carer-well-being on overall placement stability (Rock, Michelson, Thomson, & Day, 2015). Limited training, feeling unsupported and low self-efficacy also appear to contribute to a foster carer’s likelihood of leaving the profession (Denby, Rindfleisch, & Bean, 1999; Rhodes, Orme, & Buehler, 2001; Sinclair, Gibbs, & Wilson, 2004). While placement stability is a priority for social care, research exploring the overall well-being of foster carers remains extremely limited.
The reasons children are placed in the care of a local authority are often related to potentially traumatising experiences of abuse and neglect (Department of Children, Schools and Families, 2009). Given the adverse circumstances usually associated with a child being taken into care, looked after children often present with high rates of behavioural difficulties and emotional distress (Cook et al., 2005; Greeson, Briggs, & Kisiel, 2011; Oswold, Fegert, & Goldbeck, 2010). It is well established that looked after children in the care of a local authority experience higher rates of psychiatric disorders (Ford, Vostanis, Meltzer, & Goodman, 2007; McAuley & Davis, 2009; Meltzer, Gatward, Corbin, Goodman, & Ford, 2003; Richardson & Joughin, 2000) and increased rates of behavioural difficulties than children living with their biological parents (Burns et al., 2004; Clausen, Landsverk, Ganger, Chadwick, & Litrownik, 1998; Halfon, Mendonca, & Berkowitz, 1995; Sawyer, Carbone, Searle, & Robinson, 2007). With this in mind, the impact of caring for children presenting with a history of complex trauma, as well as behavioural and emotional difficulties understandably puts a strain on the foster carers with whom they are placed.
Psychological impact of working with traumatised individuals
A number of terms have been used to describe the psychological impact of working with traumatised individuals, including burnout (Maslach, 1982; Maslach, Schaufeli, & Leiter, 2001), secondary trauma (Figley, 1995) and compassion fatigue (Bride, Radey, & Figley, 2007; Stamm, 2005).
Compassion Fatigue is considered to be an overarching term used to describe the emotional impact of working with traumatised individuals including secondary trauma and burnout (Figley, 2002, 2013; Stamm, 2010).
Secondary Trauma is characterised by tension and preoccupation with the suffering of others as a result of working in trauma-related contexts. Secondary trauma symptoms are similar to symptoms of posttraumatic stress disorder (PTSD) and include heightened states of arousal, intrusive thoughts or images, and avoidance of thoughts or reminders of the person’s traumatic experiences (Figley, 1995).
Burnout is the response that occurs as a result of prolonged exposure to demanding interpersonal situations and is characterised by emotional and physical exhaustion, depersonalisation and reduced personal accomplishment (Maslach et al., 2001). The symptoms of burnout tend to develop gradually over time but if ignored can progressively worsen (Figley, 1995).
Compassion Satisfaction is described as the positive emotional response that results from helping others, including positive feelings about colleagues, contributions to the work setting and doing something good for society (Phelps, Lloyd, Creamer, & Forbes, 2009; Stamm, 2002). Compassion satisfaction has been found to mitigate the effects of burnout and secondary trauma (Ray, Wong, White, & Heaslip, 2013; Wee & Myers, 2003).
The presence of compassion fatigue has been widely reported in various professionals working with traumatised individuals including nurses (Beck, 2011; Burtson & Stichler, 2010; Hooper, Craig, Janvrin, Wetsel, & Reimels, 2010), trauma counsellors (Carmel & Friedlander, 2009; Ghahramanlou & Brodbeck, 2000), domestic violence staff (Baird & Jenkins, 2003) and social workers of adult trauma victims (Boscarino, Figley, & Adams, 2004). There have been fewer studies investigating the impact of working with traumatised children; however, there are indications of similar experiences of compassion fatigue in child protection workers (Conrad & Kellar-Guenther, 2006; Cornille & Meyers, 1999; Sprang, Craig, & Clark, 2011), forensic interviewers of abused children (Perron & Hiltz, 2006) and paediatric health care providers (Meadors, Lamson, Swanson, White, & Sire, 2010). The emotional impact of working with children may occur directly as a result of the challenges of managing behavioural difficulties or indirectly through hearing about a child’s traumatic history (Meyers & Cornille, 2002).
Avoidance of trauma
Avoidance of trauma-related thoughts and memories is central to the definition of compassion fatigue and specifically secondary trauma (Figley, 1995). More broadly, avoidant coping has been found to be common in a range of psychological problems, including depression and anxiety disorders (Holahan, Moos, Holahan, Brennan, & Schutte, 2005; Thompson & Waltz, 2010; Tull, Gratz, Salters, & Roemer, 2004). As such, this exploratory study aims to investigate the relationship of avoidant coping with compassion fatigue. Two cognitive processes that have been described as highly related to avoidance are psychological inflexibility and thought suppression. Psychological flexibility is described as ‘the ability to fully contact the present moment and the thoughts and feelings it contains without needless defence’ (Hayes, Luoma, Bond, Masuda, & Lillis, 2006, p. 7). Thought suppression is the conscious attempt to stop thinking about a particular thought (Wegner, Schneider, Carter, & White, 1987). Research indicates a paradoxical effect of thought suppression and avoidance of unwanted internal experiences with continued avoidance over time actually causing maintenance or increased frequency of the unwanted experiences (Hayes & Wilson, 1996; Kumpula, Orcutt, Bardeen, & Varkovitzky, 2011; Marx & Sloan, 2005; Wegner et al., 1987).
The present study
This is a proof of concept study that aims to examine whether the model of compassion fatigue, described in other professionals, applies to this population. The study draws similarities from previous unpublished work by McLain (2008) and a recent study by Ottaway and Selwyn (2016), who investigated compassion fatigue in foster carers. This study expands on previous work by also considering the potential relationship with job retention and satisfaction as well as underlying avoidant mechanisms. The study examined the association between secondary trauma, burnout and compassion satisfaction on intent to continue fostering and overall job satisfaction, two outcomes that will have significant practical implications. Finally, the study explored the association of compassion fatigue with two cognitive processes, psychological inflexibility and thought suppression, which are known to be related to symptoms of avoidance in trauma.
Method
Participants
Participants were 131 local authority foster carers, foster carers from the independent sector and kinship carers approved as foster carers working in the United Kingdom. Inclusion criteria for participation in this study were that the foster carers were (a) registered foster carer for at least 6 months and (b) currently looking after at least one child placed by the Local Authority, or had done so within the last 6 months. An a priori power analysis was carried out to determine the minimum sample size required to detect a statistically significant relationship between compassion fatigue and job satisfaction and intent to continue fostering. Based on the results of previous studies investigating compassion fatigue, with an effect size of r = .33 (Perron & Hiltz, 2006), a sample size of at least 102 was required with an alpha level set at .01 and power of .80. There is currently no comprehensive data on the demographic profile of foster carers in the United Kingdom; however, limited data suggest that the current sample is of a similar age, gender and marital status (McDermid, Holmes, Kirton, & Signoretta, 2012), although more ethnically diverse, which may be a reflection of the urban recruitment in the current sample.
Measures
Professional Quality of Life Questionnaire
The Professional Quality of Life (ProQoL; Stamm, 2005) questionnaire is a 30-item, 6-point Likert-type scale based on experiences in the last 30 days measuring three components: compassion satisfaction, burnout and compassion fatigue, with each score measuring distinct theoretical concepts. This measure has good psychometric properties from a range of populations including social work and nurses (Adams, Boscarino, & Figley, 2006; Potter et al., 2010). The ProQoL was scored using the method outlined in the ProQoL Manual (Stamm, 2010), which includes cut-offs for high (75%) and low (25%) scores based on a databank of 1289 cases created from multiple studies across various helping professions. For this study, Cronbach’s alpha indicates good internal reliability for all subtests: secondary trauma (.75), burnout (.80) and compassion satisfaction (.87).
Secondary Trauma Stress Scale
The Secondary Trauma Stress Scale (STSS; Bride, Robinson, Yegidis, & Figley, 2004) is a 17-item, 5-point Likert-type scale designed to assess the frequency of intrusion, avoidance and arousal symptoms over the past 7 days. A score of 38 or higher indicates secondary trauma. The STSS has demonstrated good validity and reliability in studies of social workers (Bride et al., 2004; Ting, Jacobson, Sanders, Bride, & Harrington, 2005). In relation to this study, the total STSS score showed good internal reliability (.94) as did the subtests of intrusions (.80), avoidance (.87) and arousal (.84).
Intent to continue and job satisfaction were measured using two items from a previous study investigating foster carer satisfaction and intent to continue (Denby et al., 1999). The first item, ‘all in all, how satisfied are you as a foster parent?’ consisted of a 4-point scale. Binary categories were created by combining ‘not at all satisfied’ with ‘somewhat dissatisfied’ and ‘somewhat satisfied’ with ‘very satisfied’ to represent low and high satisfaction. The second item, ‘how likely is it that a year from now you will still be working as a foster carer?’ consisted of a three-level scale of ‘not at all likely’, ‘somewhat likely’ or ‘very likely’. The latter two scores were combined to create a high intent to continue score.
Acceptance and Action Questionnaire–II
The Acceptance and Action Questionnaire–II (AAQ-II; Bond et al., 2011) consists of seven items on a 7-point Likert-type scale. The scale reflects the single domain of psychological inflexibility with higher scores indicating greater psychological inflexibility. The psychometric properties of this measure are well documented in non-clinical samples (Bond et al., 2011). In this study, internal reliability for this scale was high (.93).
The White Bear Suppression Inventory
The White Bear Suppression Inventory (WBSI; Wegner & Zanakos, 1994) is a 15-item measure on a 5-point Likert-type scale measuring a person’s tendency to suppress thoughts. This measure has been found to have good reliability and validity (Luciano et al., 2006), and the internal consistency in this study was high (.96).
Procedure
Foster carers were contacted via local authorities in and around London as well as The Adolescent and Children’s Trust, the United Kingdom’s largest Fostering and Adoption charity. Following consent from gatekeepers, foster carers were sent an email invitation to participate in the study containing the information sheet and a link to the online survey. Consent was implied by participants completing the survey. Once the survey had been completed, participants were given an opportunity to contact the researcher via email to claim a £5 voucher. Participants were able to remain anonymous and not claim the voucher should they wish.
Both the information sheet and the exit page of the survey contained information for accessing further support for participants who experienced any anxiety or distress as a result of completing the survey. The research was approved by King’s College London Research Ethics Committee, and consent forms and information sheets were available via the online survey. Data collection was conducted between October 2015 and January 2016.
Data analysis plan
The data from the survey were exported from the Bristol Online Survey into IBM SPSS Statistics 22 where it was then coded and analysed. Due to data not being normally distributed, the bootstrap function (5000 samples) was used to generate more accurate standard errors, confidence intervals (CIs) and p values (Good, 2005). The bootstrap function on independent-sample t-tests does not use the t-distribution and degrees of freedom to derive the p value and CIs, and so these are not provided. Effect sizes for t-tests were defined as weak (.2), moderate (.5) or large (.8) as recommended by Cohen (1992). For bivariate analyses, correlations were defined as weak (r = .1), moderate (r = .3) or strong (r ≥ .5) based on recommendations by Cohen (1992).
Results
Descriptive statistics
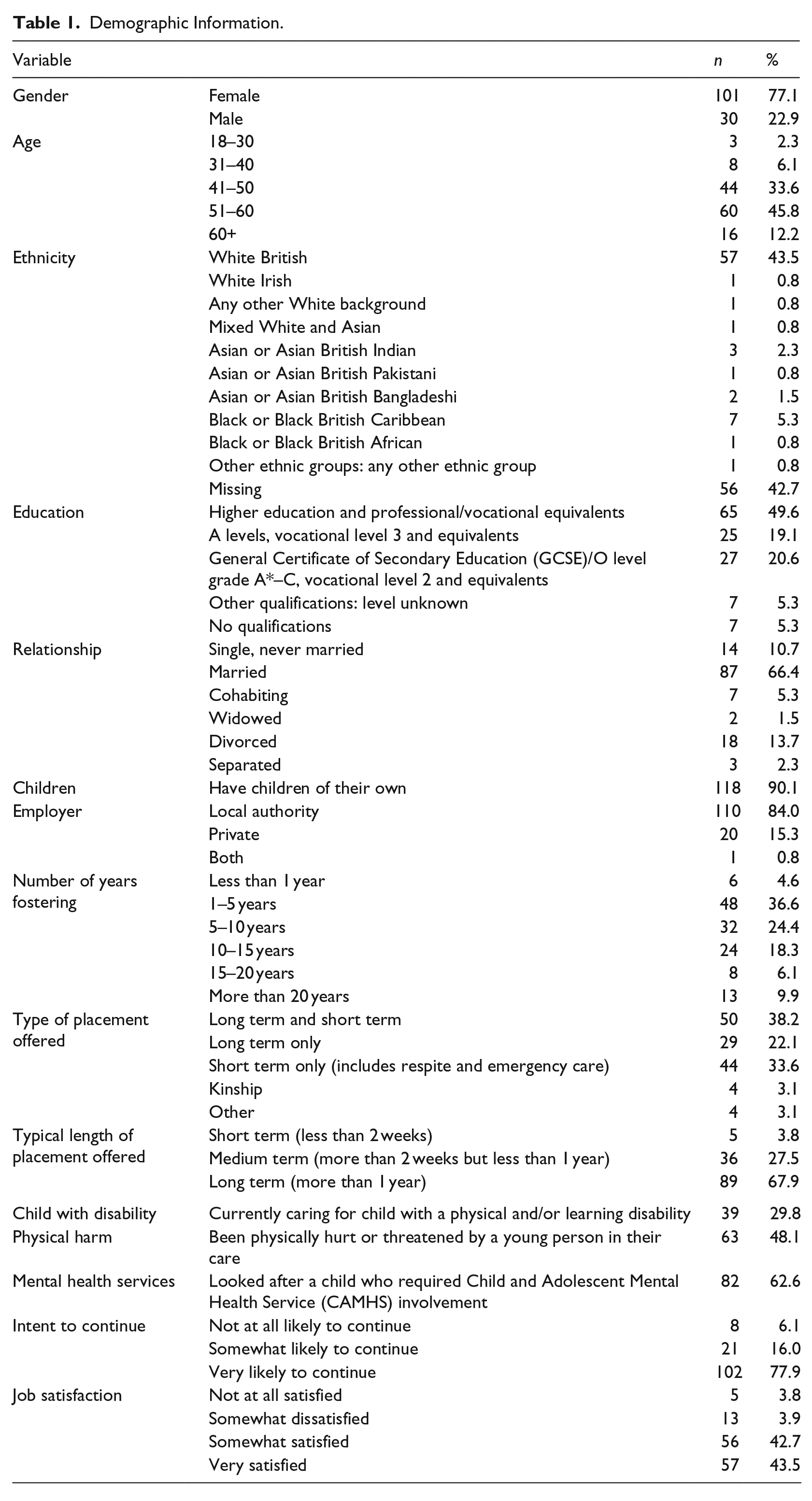
The majority of participants were females (77.1%), over 40 years old (91.6%), married (66.4%) and had their own children (90.1%); 43.5% of the sample were White British and 49.6% had obtained higher education or professional qualifications. The majority of participants reported they were very likely to continue fostering (77.9%) and either somewhat (42.7%) or very (43.5%) satisfied in their jobs (see Table 1 for demographic information).
Demographic Information.
Overall, 25.2% (n = 33) of participants reported high levels of secondary trauma and 30.5% (n = 40) reported high levels of burnout; 18.3% (n = 24) of participants rated themselves as high for compassion satisfaction (see Table 2).
Rates of secondary trauma, burnout and compassion satisfaction from the ProQoL.
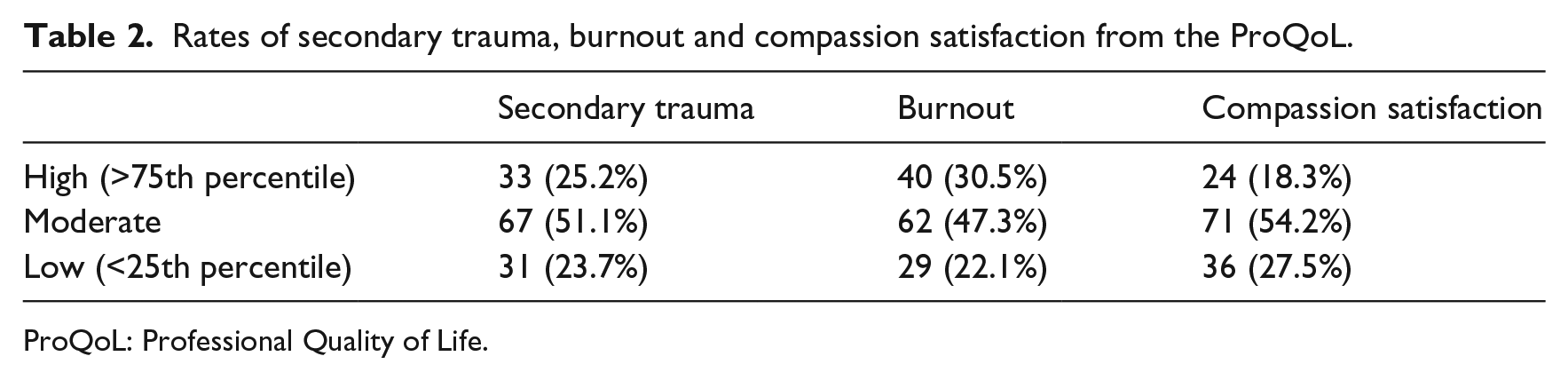
ProQoL: Professional Quality of Life.
The mean scores and standard deviations for the STSS can be found in Table 3. The STSS provides a specific clinical cut-off of 38 and this study found that 19.8% (n = 26) of participants were above the clinical cut-off for secondary trauma.
Mean scores and SDs from STSS.
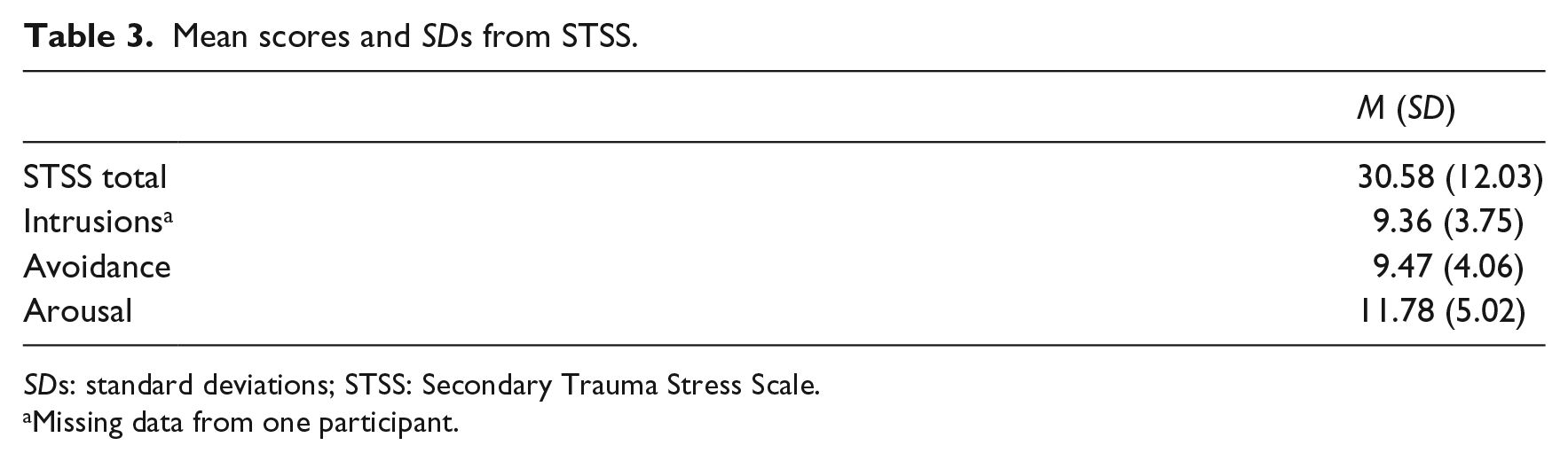
SDs: standard deviations; STSS: Secondary Trauma Stress Scale.
Missing data from one participant.
In line with the hypothesis, there was evidence supporting the presence of secondary trauma and burnout in foster carers. Further analysis indicated significant correlations between the two measures of secondary trauma (see Table 4). Furthermore, and in line with previous findings, compassion satisfaction was negatively associated with secondary trauma and burnout scales.
Bivariate correlation of ProQoL and STSS measures.
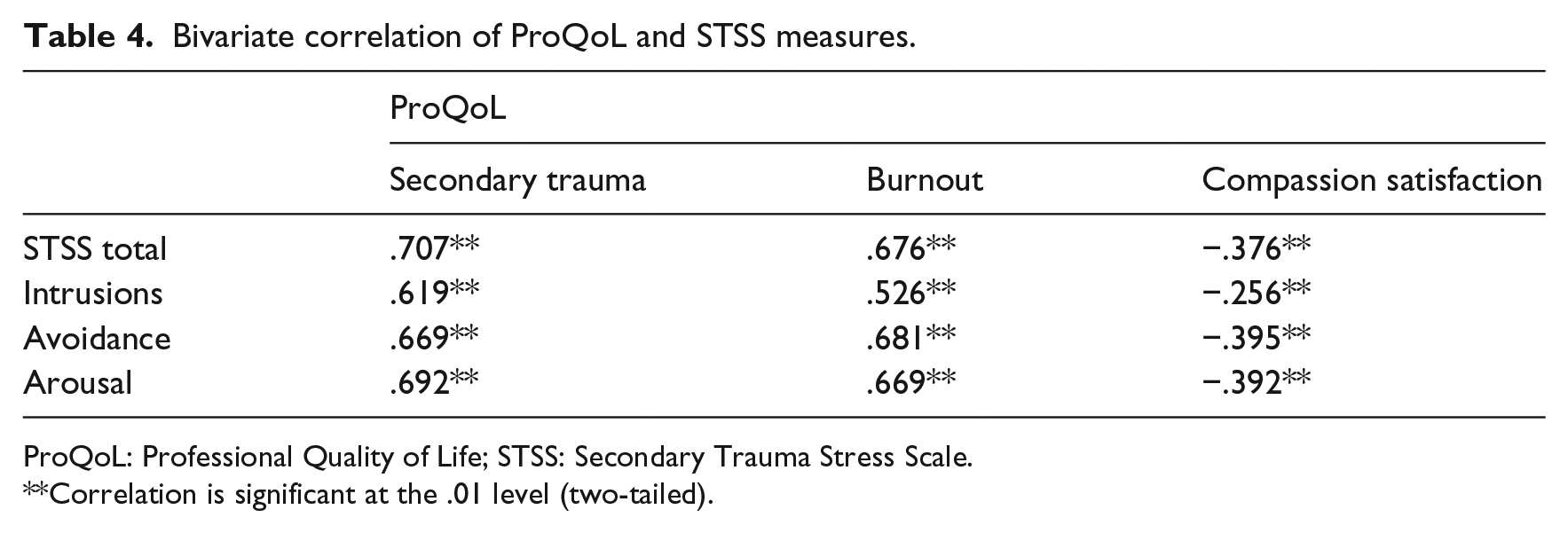
ProQoL: Professional Quality of Life; STSS: Secondary Trauma Stress Scale.
Correlation is significant at the .01 level (two-tailed).
Intent to continue fostering was significantly associated with secondary trauma (95% CI = [4.07, 15.90], p = .006, d = .70), burnout (95% CI = [2.85, 7.70], p < .001, d = .88) and compassion satisfaction (95% CI = [−6.39, −0.68], p = .036, d = −.54). Participants with low intent to continue fostering had significantly higher secondary trauma and burnout scores and significant lower compassion fatigue scores than those with high intent to continue fostering (see Figure 1).

Mean scores and standard errors for low and high intent to continue fostering.
Low job satisfaction was significantly associated with secondary trauma (95% CI = [−17.92, −2.57], p = .035, d = .73), burnout (95% CI = [−9.34, −1.88], p = .009, d = .82) and compassion satisfaction (95% CI = [1.26, 9.43], p = .023, d = .77). Participants with low job satisfaction had significantly higher secondary trauma and burnout scores, and significantly lower compassion satisfaction scores (see Figure 2).

Mean scores and standard errors for low and high job satisfaction.
Results indicate that psychological inflexibility was significantly and positively correlated to secondary trauma (r = .349, p < .001) and burnout (r = .520, p < .001). Thought suppression, as measured by the WBSI, was also positively associated with secondary trauma (r = .597, p < .001) as well as burnout (r = .437, p < .001). As predicted, higher levels of psychological inflexibility and increased thought suppression are related to higher secondary trauma and burnout scores (see Table 5).
Bivariate correlations of secondary trauma, intrusions, avoidance and arousal (from STSS), and burnout (from ProQoL) with psychological inflexibility (AAQ-II) and thought suppression (WBSI).

STSS: Secondary Trauma Stress Scale; ProQoL: Professional Quality of Life; AAQ-II: Acceptance and Action Questionnaire–II; WBSI: White Bear Suppression Inventory.
Correlation is significant at the .01 level (two-tailed).
Discussion
This study investigated the experiences of compassion fatigue in foster carers working in the United Kingdom. A sample of 131 foster carers completed an online survey to measure compassion fatigue and several related variables. The primary aim of the study was to establish whether the concept of compassion fatigue, the overarching term to describe the effects of secondary trauma and burnout, occurs within this population. This study also examined the impact of compassion fatigue on risk factors related to intent to continue fostering and job satisfaction. This study also examined the associations between compassion fatigue and avoidant cognitive styles of psychological inflexibility and thought suppression.
Results indicate that 19.8% of participants were above the clinical cut-off for secondary trauma based on the STSS, and 25.2% presented as high risk for secondary trauma and 30.5% for burnout on the ProQoL. While STSS scores appear somewhat lower than previous studies on nurses (38%, Quinal, Harford, & Rutledge, 2009; 33%, Dominguez-Gomez & Rutledge, 2009), the results remain concerning. In addition, results from the ProQoL appear to be consistent with previous work with foster carers (Ottaway & Selwyn, 2016) as well as other professionals working with trauma victims (Bride et al., 2007; Stamm, 2005; Van Hook & Rothenberg, 2009). Compassion satisfaction was found to be negatively associated with compassion fatigue, in line with Stamm’s (2010) model, supporting the idea that is potential for mitigating effects of compassion satisfaction on compassion fatigue. While similarities can be drawn from studies examining other caring professions, it should be noted here that fostering vulnerable children is unique and complex work unlike any other profession and requires incredible emotional commitment. As such, all references to fostering as a job do not intend to simplify this important and at times complicated role. With this in mind, this study focuses primarily on compassion fatigue but acknowledges there are range of stressors related to this role that have not been measured in this study (e.g. interactions with the local authority, issues around intimacy and decision making or personal stressors) which may also impact a carers’ job satisfaction and intent to continue fostering.
Local authorities are currently facing a significant challenge in recruiting and retaining sufficient numbers of foster carers to take on the growing numbers of looked after children in the United Kingdom. The high rates of mental health difficulties and behavioural challenges in looked after children are well documented, and these are known to contribute to the success of a placement. However, the experience of the foster carer themselves is underresearched and this study aimed to explore the relationship between compassion fatigue with job satisfaction and foster carer’s intent to continue fostering. Foster carers with lower job satisfaction and intent to continue had significantly higher compassion fatigue scores and this could be a target for intervention as discussed below. In addition, compassion satisfaction scores were higher for foster carers with higher intent to continue and job satisfaction. The report of physical harm at 48% appears high and may well contribute to the level of secondary trauma in this sample. However, the data were collected as a single item as part of the demographic data and as such we would not claim that it is necessarily a precise representation.
Bivariate analyses found strong correlations between compassion fatigue and psychological inflexibility and thought suppression. Given the paradoxical effect of avoidant cognitive styles, foster carers with higher psychological inflexibility and a tendency to suppress thoughts may be at increased risk for compassion fatigue. Similarly, the negative emotional impact of their work may be exacerbated by a predisposition to engage in avoidant styles, that is, be bidirectional (see below).
This is an initial study to establish proof of concept and the relation to some key variables. As such, the sample is relatively small and diverse in terms of the type of foster placement and recruitment centring in and around one major urban region, all of which may impact the representativeness. One potential limitation is that the content of the survey may have influenced the type of respondent and affected the return rate. One possibility is that those experiencing higher strain and possibly at greater risk of compassion fatigue did not feel able to take the time to complete the survey and the current results underestimate the overall levels of compassion fatigue among foster carers. On the other hand, the survey content may have appealed to those experiencing high levels of strain as a means of reflecting experiences. Qualitative studies may be more able to investigate the potential influences driving participation and responses.
As a cross-sectional study, we are unable to describe the direction of effects. Further research should be conducted to examine the direct effect that compassion fatigue may have on intention to leave. In addition, the outcomes for job retention and satisfaction were measured as binaries, derived from ordinal scales, and although this has been done in other studies (e.g. Denby et al., 1999), the relationships between satisfaction and retention are likely to be more nuanced than captured in these binary constructs. Future studies would benefit from more in-depth investigation of these constructs, especially, if there was an aim to predict risk of leaving the profession based on current satisfaction. Conducting a longitudinal study, with repeated measures of compassion fatigue, may be particularly valuable in assessing the trajectory of foster carers’ job retention in relation to their compassion fatigue levels. In terms of the risk factors investigated in this study, the relationship between compassion fatigue and other variables may well be bidirectional.
Clinical implications
The current study provides important evidence of the presence of compassion fatigue in foster carers, which is relevant to those managing and supporting the foster carers in their work. The association between compassion fatigue and job satisfaction and intent to continue provides further support for increased awareness and support for foster carers as symptoms may have negative implications to placement stability and overall retention. Formal training on compassion fatigue and related risk factors, as well as encouraging services to screen for symptoms may be beneficial. This study has shown that ProQoL and STSS are two reliable measures that could be used for screening symptoms of compassion fatigue.
In addition, the associations between avoidant cognitive styles and compassion fatigue have implications on further interventions that aim to reduce thought suppression and increase psychological flexibility, as a way to target possible mechanisms underlying compassion fatigue. Acceptance and commitment therapy (ACT; Hayes, Strosahl, & Wilson, 1999) is a psychological therapy that promotes a non-judgemental willingness to experience aversive events while moving towards valued life goals, and an intervention incorporating an ACT framework could be useful for foster carers. Interventions incorporating mindfulness (which may address avoidant coping styles; Shapiro, Carlson, Astin, & Freedman, 2006) may also be worth consideration, although further research is required to explore their efficacy in relation to compassion fatigue.
Conclusion
This study is the first to describe rates of compassion fatigue in foster carers with approximately one quarter of participants reporting high levels of secondary trauma and burnout. This study also replicates previous findings of the association between compassion satisfaction and compassion fatigue. Higher levels of compassion fatigue were also associated with lower job satisfaction and lower intent to continue fostering. To promote placement stability and foster carer retention, services should pay attention to the well-being of foster carers particularly regarding recognition of compassion fatigue. Findings confirm an association between avoidant cognitive styles and compassion fatigue. Possible ways to target this could be to consider interventions based on increased psychological flexibility such as ACT. Clinical implications are discussed in terms of direct support for foster carers through reflective practice and clinical interventions targeting cognitive styles such as ACT or mindfulness to promote foster carer well-being. Further research is required to explore the efficacy of these interventions and the well-being of foster carers generally.
Footnotes
Acknowledgements
The authors would like to thank all of the local authorities who assisted with recruitment and to all of the foster carers who took the time to participate in the study. They also thank Dr Wendy Geraghty for her contributions to the project.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author biographies
![]() ]. He has a particular interest in the assessment and treatment of complex presentations of adopted children or children from the care system, especially with regard to disentangling the effects of biological and neurodevelopmental factors from attachment, trauma and behavioural issues.
]. He has a particular interest in the assessment and treatment of complex presentations of adopted children or children from the care system, especially with regard to disentangling the effects of biological and neurodevelopmental factors from attachment, trauma and behavioural issues.