
Abstract
Maudsley Family-Based Treatment (FBT) is currently the best supported treatment for adolescents with anorexia nervosa (AN); however, little is known about whether it achieves its stated aim in the final phases of promoting the patient’s return to an expected developmental trajectory. This study aimed to explore the perspectives of young people and their parents regarding the developmental impact of AN, and the role of FBT in addressing developmental challenges. Young people (N = 12) who ceased FBT a minimum 1 year prior, and their parents (N = 12), completed face-to-face semi-structured interviews, and data were analysed using a narrative inquiry method. All the participants described AN as highly disruptive to adolescent development, with phase one of FBT accentuating this experience. In phases two and three, FBT helped facilitate adolescent development in three key ways: Supporting return to adolescent pursuits, facilitating autonomy and providing freedom to develop post-FBT. This study offers preliminary insights into the variety of developmental challenges and needs experienced by families, as well as approaches clinicians can take to supporting development in phases two and three of FBT.
Adolescence is a period of rapid physical and psychosocial development. Particularly crucial is the expansion of social relationships beyond the family, increased independence, increased self-regulation, formation of academic and vocational plans, development of a sexual identity and formation of a stable sense of self (Fornari & Dancyger, 2003). Anorexia nervosa (AN) has peak onset in adolescence (Le Grange, 2005), and during this period, causes disruption to physical, social and psychosexual development (Hatch et al., 2010; Herpertz-Dahlmann et al., 2001; Ruuska, Koivisto, Rantanen, & Kaltiala-Heino, 2007), including independence from family of origin (Ratnasuriya, Eisler, Szmukler, & Russell, 1991).
Given the significance of development during this period, the disruption caused by adolescent-onset AN often persists long-term (Råstam, Gillberg, & Wentz, 2003; Ruuska et al., 2007). Individuals experience difficulties with employment and social isolation, even in the context of recovery from eating disorder symptoms (Råstam et al., 2003; Ruuska et al., 2007; Wentz, Gillberg, Gillberg, & Råstam, 2001), and long-term interpersonal difficulties and dependence on family are common (Ratnasuriya et al., 1991). Given this pervasive impact, the need for research exploring how treatment can better facilitate recovery from AN beyond weight gain and abatement of eating disorder cognitions and behaviours has become increasingly apparent (Dawson, Rhodes, & Touyz, 2014b; Jarman & Walsh, 1999; Keski-Rahkonen & Tozzi, 2005). Furthermore, while quantitative investigations have provided some indication of the nature and extent of this impact, little is known about patients’ and their families’ experiences of this developmental disruption, and thus where their priorities for addressing developmental issues in treatment may lie.
Available treatments for adolescents with AN have varying levels of developmental focus. Adolescent focused therapy (AFT) takes development as its primary focus. A formulation is developed regarding how AN may function as a strategy to cope with developmental challenges; attention is given to adolescent issues such as self-efficacy, autonomy and assertiveness, and the young person is assisted to develop ways of managing common stressors that occur during this developmental period (Fitzpatrick, Moye, Hoste, Lock, & Le Grange, 2010). Sessions together with parents, generally primarily occurring in the early stages of treatment, seek to assist parents to support their child in taking on adolescent challenges and making self-directed changes (Fitzpatrick et al., 2010). Enhanced cognitive behavioural therapy (CBT-E), when adapted for adolescents, also focuses on promoting healthy development, and includes enhancement of autonomy and addressing difficulties with peer relationships from early on in treatment(Fairburn, 2008). The treatment with the highest level of empirical support for adolescents below 18 years with a short duration of illness is Family-Based Treatment (FBT; Couturier, Kimber, & Szatmari, 2013). FBT is a behaviourally focused outpatient treatment that seeks to utilise the adolescent’s family as a resource to aid re-feeding and recovery (Lock & Le Grange, 2013). Therapy is conducted in three phases. In the first, adolescent developmental tasks are deferred to focus on achieving weight gain through transfer of responsibility for the young person’s weight-related behaviours to their parents. In the second phase, responsibility is gradually returned to the young person, and attention is given to issues of adolescent development as they relate to AN, as well as beginning to addressing psychiatric comorbidities (Lock & Le Grange, 2013). Phase three focuses on facilitating a developmentally appropriate relationship between parents and the young person, as well as exploring issues such as independence and sexuality (Lock & Le Grange, 2013). However, the actual developmental issues addressed depend upon the needs of each young person/family.
While a key aim of phases two and three is thus to assist the adolescent’s return to a healthy developmental trajectory (Lock & Le Grange, 2013), little is known about whether, or how, this is achieved. Proponents of individual approaches, such as AFT, have argued that the transfer of responsibility for eating to parents may be disruptive to the development of autonomy (Lock & Le Grange, 2005). Attention to development in phases two and three may serve to offset potential disruption in phase one, however, little is known about this aspect of the treatment model.
The aim of this study was thus to explore the perspectives of young people and their parents regarding the developmental impact of AN, and any role of FBT in facilitating a return to healthy adolescent development.
Method
Participants
Participants were young people and one of their parents. Parents as well as young people were included to achieve data source triangulation (Carter, Bryant-Lukosius, DiCenso, Blythe, & Neville, 2014; Flick, 2004), in particular taking into account the potential effect of the cognitive impairment of AN on patients’ recall. Young people were eligible if they had ceased FBT at least 12 months prior, and had completed at least four sessions of phases two and three – the minimum possible number of sessions indicated in the treatment manual (Lock & Le Grange, 2013). Participants were required to be weight restored (defined as body mass index (BMI) ⩾ 18.5; World Health Organisation, 2011), to ensure their participation was not affected by the cognitive and/or psychological effects of malnutrition. Participants were excluded if they had an intellectual disability or did not have fluent or near-fluent English.
A total of 42 families were approached via both letter and phone call. One participant was excluded due to cognitive impairment, and another three due to being currently physically unwell with AN, while 23 young people and/or their parents declined participation. The reasons given for declining were anticipated distress (N = 7), a negative experience of treatment (N = 2), current other mental health difficulties (N = 2) and practical barriers (N = 8). A further three families were excluded as, subsequent to the parent completing the interview, the young person withdrew from the study.
A total of 12 young people and 12 parents were thus included. Participants were aged between 16 and 24, with a mean age of 19.67 (SD = 2.14), and 11 were female. Of the 12 parents who participated, 83.3% were mothers (n = 10). At commencement of FBT, young people had a mean percentage Expected Body Weight (%EBW) of 91.9 (SD = 10.8), with most participants having been hospitalised for weight restoration prior to commencing FBT, having been medically unstable on admission. Mean BMI at the time of recruitment was 22.76 (SD = 2.99). The mean age of onset was 14.17 (SD = 1.11), and participants had ceased FBT on average 4 years and 5 months prior to participation. The participant demographics are displayed in Table 1.
Participant demographics.
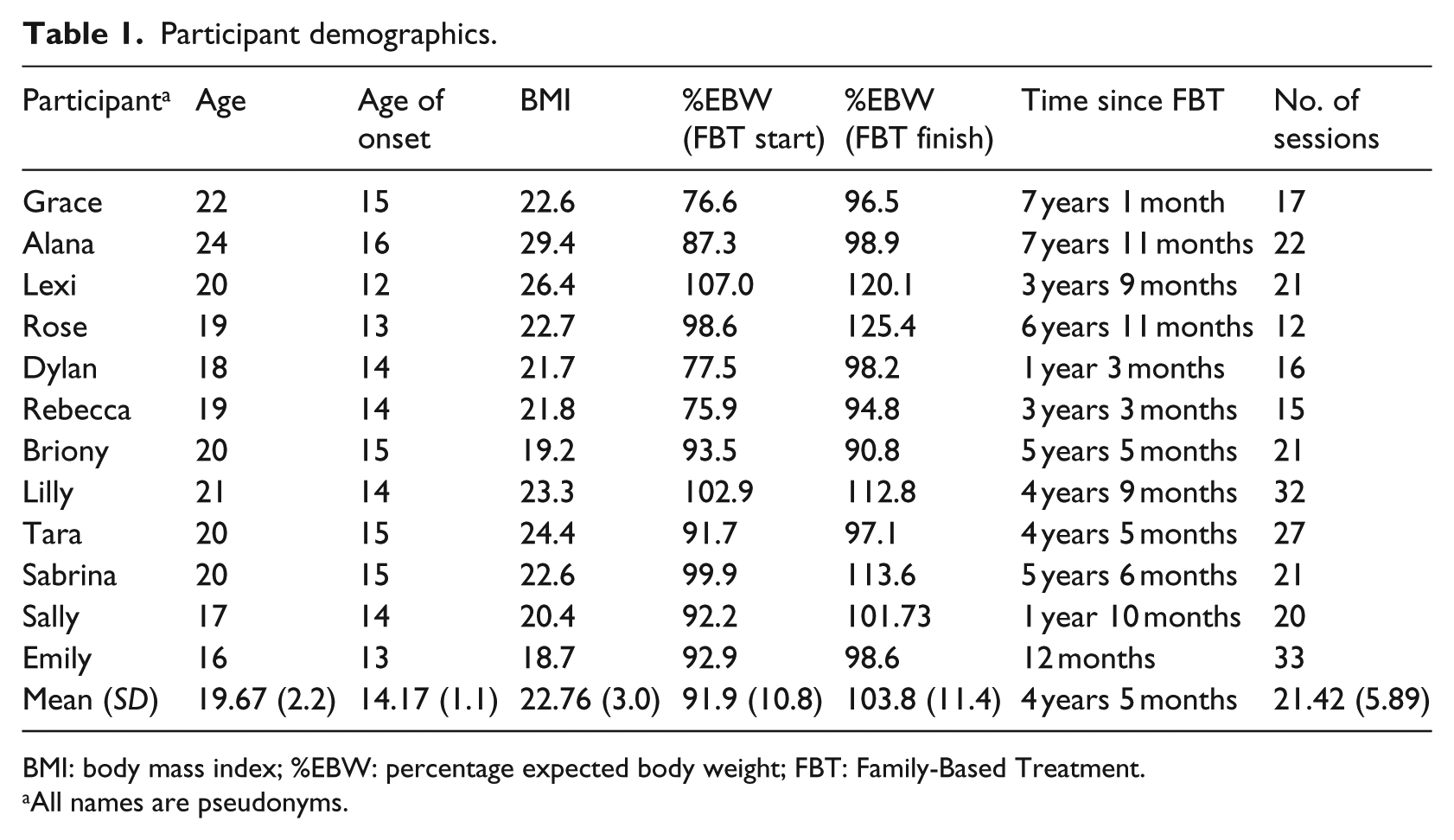
BMI: body mass index; %EBW: percentage expected body weight; FBT: Family-Based Treatment.
All names are pseudonyms.
Ethics approval
This study was approved by the Sydney Children’s Hospital Network Human Research Ethics Committee (Ref. 14/SCHN/145).
Design
The method of data collection and analysis was narrative inquiry (Clandinin & Connelly, 2000). This is a qualitative research method that seeks to understand individuals’ stories and associated processes of meaning making (Clandinin & Connelly, 2000). Participants’ experiences are organised temporally, with attention given to plot, scenes and character, and commonalities between narratives may be explored to identify narrative types (Frank, 2013; Howie, 2010). Since this method is particularly useful in understanding the temporal dimensions of an individual’s experience, it is ideally suited to the aims of this study (Howie, 2010). Qualitative methodology was selected to be able to explore the areas of development of significance to patients/parents themselves, and to gain a depth of understanding regarding families’ experiences of how FBT functions with respect to patients’ developmental needs. In addition, quantitative measures were administered to characterise the sample in terms of current eating disorder concerns. Given AN has a particularly significant impact on family and peer relationships (Cunha, Relvas, & Soares, 2009; Whitney & Eisler, 2005), a measure of attachment to parents and peers was also included.
Procedure
Recruitment
Participants were identified from records of families who had received outpatient FBT at the Eating Disorder Service at the Children’s Hospital at Westmead, NSW, Australia. Participants’ files were used to verify their completion of an adequate number of sessions of phases two and three. Eligible families were sent an invitation letter from the Eating Disorder Service coordinator, followed by a phone call inviting them to participate. Families that declined were asked to give a brief reason, if they wished.
Interviews
Young people and parents completed separate semi-structured face-to-face interviews, which were approximately 1 hour in duration. Interviews were audio-recorded. Participants were prompted to tell their story from when they first noticed symptoms of AN, through their period of being unwell, receiving FBT and the period since FBT. Parents were prompted to narrate their observations of their child’s experiences, as well as their own. Participants were asked open-ended questions, in particular regarding the impact of AN on various areas of development and their trajectory of development throughout FBT.
Following the interview, young people completed quantitative measures (see below), and their height and weight were measured by the first author to verify that they were weight-restored.
Measures
Eating Disorders Examination Questionnaire
The Eating Disorders Examination Questionnaire (EDE-Q; Fairburn & Beglin, 1994) is a 28-item self-report measure of eating disorder psychopathology, derived from the ‘gold standard’ Eating Disorders Examination, assessing key cognitive and behavioural features of eating disorders (Fairburn, Wilson, & Schleimer, 1993). The EDE-Q has been validated in both clinical and community samples and has demonstrated robust psychometric properties (Berg, Peterson, Frazier, & Crow, 2012).
Inventory of Parent and Peer Attachment
The Inventory of Parent and Peer Attachment (IPPA; Armsden & Greenberg, 1987) examines attachment to each parent and to peers, and has strong reliability and validity (Armsden & Greenberg, 1987). A shortened, 45-item version of the scale was used as this has been shown to have similarly strong psychometric properties as the original, longer form (Wilkinson & Goh, 2014). The scale was developed for use with adolescents, but has also been validated in young adult samples (Fass & Tubman, 2002; Ryan, Solberg, & Brown, 1996).
Data analysis
Interviews were transcribed verbatim. Following the narrative inquiry methodology, data were organised temporally using the periods ‘pre-anorexia nervosa’, ‘anorexia nervosa’, ‘phase one FBT’, ‘phase two/three FBT’ and ‘Post-FBT’, and were then rewritten into third-person narratives (Howie, 2010; Polkinghorne, 1995). Narratives were sent to participants via email for member checking to ensure fidelity to his or her story (Clandinin & Connelly, 2000; Krefting, 1991).
Participants’ names were replaced by pseudonyms (used below) and other identifying details removed prior to further analysis. Line-by-line coding of each narrative was conducted and themes and subthemes were identified (Howie, 2010). A second researcher (P.R.) independently coded three sets of narratives to ensure validity of the coding process, and differences were discussed and resolved before proceeding. Sometimes described as investigator triangulation, this enhances rigour by providing a variety in perspectives on the data (Flick, 2004). Parents’ and young people’s narratives were analysed separately. Comparison across narratives was conducted, including identification of any key points of difference between the narratives of each young person and their parent, to identify narrative threads, or higher order themes present across individuals (Howie, 2010). Cross-coding by two authors (M.M. and P.R.) was again conducted for three sets of narratives to ensure validity of the higher order themes. Narrative threads were checked against participant characteristics, including age of onset and age at which treatment ceased, %EBW at commencement of treatment and scores on quantitative measures.
Results
Quantitative measures
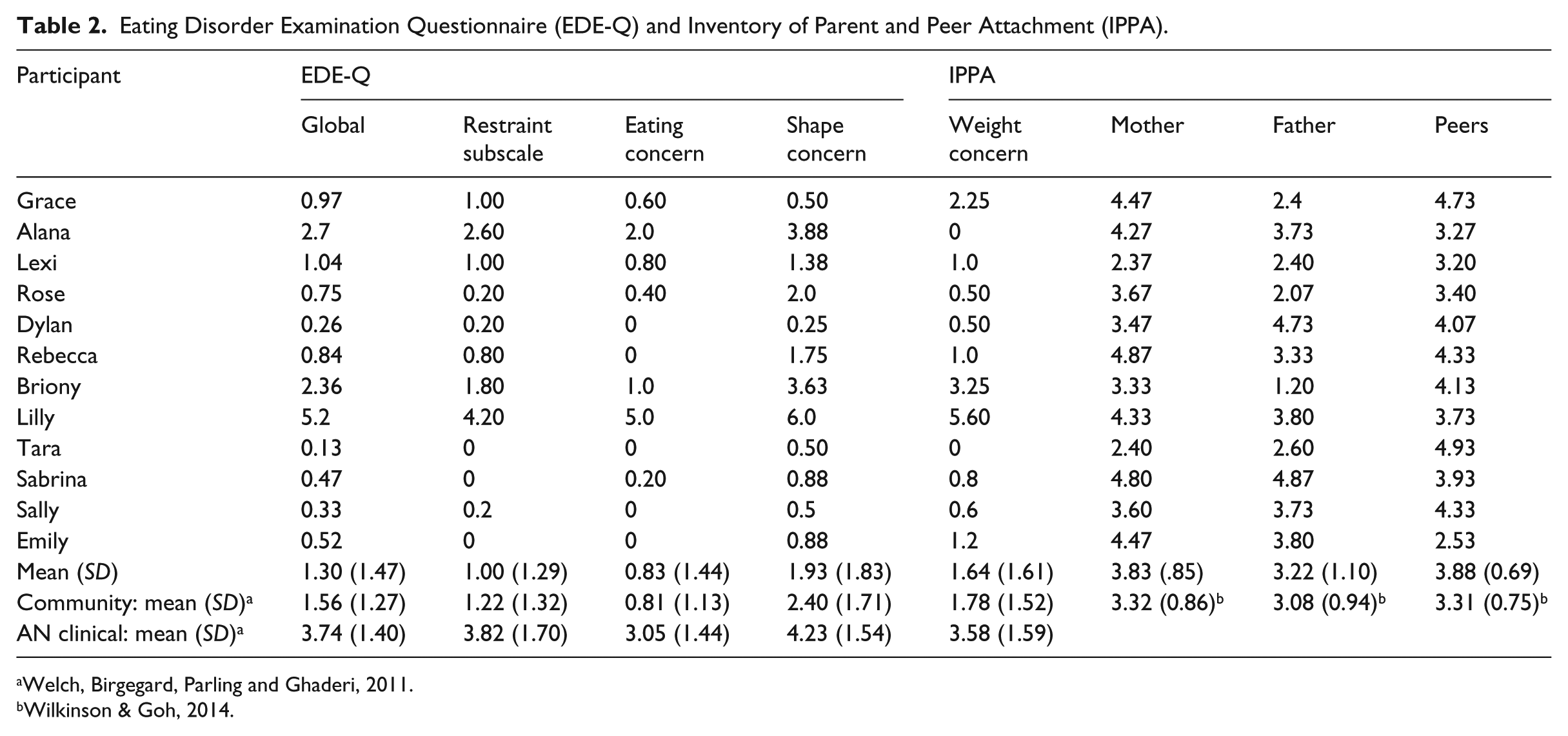
Results from the quantitative measures are presented in Table 2. All but one participant scored within one standard deviation (SD) of community norms on the EDE-Q, which is regarded as indicating absence of significant eating disorder psychopathology (Bardone-Cone et al., 2010; Welch, Birgegård, Parling, & Ghaderi, 2011). On the IPPA, two participants scored more than one SD below community norms with respect to maternal attachment, and one participant with respect to paternal attachment (Wilkinson & Goh, 2014). All participants scored within one SD of community norms on peer attachment. Compared with participants who described FBT supporting return to adolescent pursuits (see below), those who referred to treatment facilitating autonomy and providing freedom to develop post-FBT had higher EDE-Q scores, suggesting the former participants may have tended to have reached a greater degree of recovery in terms of eating disorder psychopathology. Participants following the third trajectory tended to have lower parent attachment scores. Some differences in the nature of developmental disruption depending on age of onset were observed (reported below). There was a tendency for young people with a longer time period since ceasing FBT to belong to the first trajectory. No other differences based on quantitative data were observed.
Eating Disorder Examination Questionnaire (EDE-Q) and Inventory of Parent and Peer Attachment (IPPA).
Qualitative results
Narratives of parents and young people were analysed separately, however, due to a high degree of similarity in the themes and subthemes emerging from each, these perspectives are reported together below. A schematic representation of the qualitative results is shown in Figure 1.

Schematic representation of qualitative results.
There was a high degree of commonality across participants in their description of the developmental impact of AN, and experience of phase one. Descriptions of treatment beyond phase one, however, were more heterogeneous and suggested three trajectories towards developmental recovery, with FBT playing a different role in each: (1) Supporting return to adolescent pursuits, (2) facilitating autonomy and (3) providing freedom to develop post-FBT. For some participants, more than one of these was relevant, with two participants describing both supporting return to adolescent pursuits and facilitating autonomy.
Before FBT: Developmental function and impact of AN
Most participants described experiencing developmental difficulties prior to AN. For some, this involved difficulties with mood and emotion regulation since early childhood. A number of young people had pre-existing social difficulties, including lack of social confidence, difficulty acquiring social skills or frequent bullying. These became more prominent as the young person reached adolescence and relationships outside the family became more important. For some, social difficulties were observed to make individuation from their primary caregiver more difficult. A number of participants described AN as an attempt to gain social acceptance.
Participants described pervasive developmental disruption upon becoming unwell, particularly in terms of relationships with peers. Pre-existing social difficulties were exacerbated. Sabrina and Rebecca described increased bullying, and recalled friends beginning to avoid them upon noticing changes in their appearance and behaviour. Briony and Alana both described beginning to avoid previously enjoyed social interactions because they involved eating, while Emily described losing her connection with friends: ‘I still sat with them at lunch at school, but it was almost like no relationship there . . . I was just a zombie’. She described how her development of independence was stalled by AN, and this meant she was not at the same stage as her peers, interfering with her ability to relate to them: ‘They continued to develop and I was still kind of stuck’.
Parents observed that their child’s development was limited by reduced interest in experimentation: they shied away from joining peers in ‘pushing the boundaries’ with respect to, for example, intimate relationships, alcohol or minor risk-taking behaviours. Some young people were described as having missed a period of development of critical skills. Sabrina’s mother described her daughter’s lack of development of assertiveness skills: ‘She missed those couple of years of development on herself. It was all about eating, rather than about liking herself or how to say no to somebody or stick up for yourself in an argument’.
Phase one of FBT: Further regression
Once participants commenced FBT, development was initially further disrupted. The nature of developmental disruption in phase one varied depending on the age of the adolescent, with disruption to the development of adolescent friendships more prominent for those with younger age of onset, and disruption to romantic relationships and plans for the future more prominent among those who developed AN, and received FBT, at an older age. Continuous supervision from parents or teachers resulted in young people feeling they lacked developmentally appropriate freedom and had an unwanted level of intensity in their relationship with their primary caregiver. Emily described how difficulty forming her own identity was exacerbated in phase one: ‘I had to focus on getting better physically . . . I think it was a really important time, thirteen, fourteen, to start being your own person, and I didn’t really get that opportunity’. The developmental impact of treatment in phase one appeared to be strongest socially. Ceasing sport, which for many participants was previously central to their social life, increased isolation.
Participants experienced their parents’ control of their eating in phase one as returning them to an earlier point in development. Rebecca described feeling like a she had been ‘thrown straight back to when I was 10 years old and reliant on my parents telling me what I can and can’t do’. Parents recognised this disrupted the adolescent’s development of their own life and identity separate from the family. Young people reported understanding that addressing issues such as social and body image difficulties was not the priority in this stage of treatment, and thus often refrained from raising these.
Beyond phase one: Three trajectories of adolescent development
Supporting return to adolescent pursuits
Five participants found phases two and three facilitated developmental recovery chiefly by using particular ‘milestones’ to inspire the young person to begin to take responsibility for their own eating and recovery. Young people described that the more they ‘re-entered life’, the stronger their motivation to leave the eating disorder behind, and observed that they found developmentally typical activities inherently motivating. Some had been relatively on track developmentally prior to the onset of AN, and thus were eager to return to certain aspects of their life. For others, the fact that they had not yet experienced certain events or milestones was motivating. Grace described that: I had never kissed a boy. I’d never gone to a party . . . I’m quite lucky that it [AN] happened in that time of my life because you can’t have a boyfriend if you don’t eat . . . You’re not going to get invited to parties . . . Whereas I think if I had gone through that now where I have all this freedom and have had those experiences, there’d be less motivation to seem normal and get normal.
Participants observed that FBT facilitated a cycle whereby normalisation of their eating allowed gradual increases in freedom and independence, and this motivated further normalisation of their eating. Tara described that: As I had more control, I felt like I was more free and more able to enjoy my social life or my schooling life or I was able to work . . . The more I got, the more beneficial it was for me because I was like, well this is great . . . How could I throw it away and go back to something like that?
Parents found that the use of developmental motivators made the process of handing back control more manageable for them, and appreciated being able to work with the therapist to identify appropriate developmental ‘rewards’. Participants described their desire to ‘fit in’ socially contributing to motivation to recover. Some participants described attempting to ‘make up for lost time’. When speaking about dating, Sabrina said: ‘Once I was at a healthy weight and out of hospital, I just went nuts . . . I wanted to explore everything that I’d missed’.
Young people were engaged with therapy in phases two and three, and some developmental issues were able to be discussed. For example, Rebecca described working with both the therapist and her parents to problem solve social difficulties. Nonetheless, a number of participants identified issues they would have liked to be addressed further at this stage, including body image difficulties, self-esteem and identity issues.
Facilitating autonomy
Four participants described significant difficulties with appropriate independence prior to phases 2–3, and gradual development of autonomy from family, aided by FBT. Increased autonomy included increased formation of relationships outside the family, engaging in activities such as getting a part-time job independently, engaging in behaviours or developing ideas that were different from those of the young person’s parents, and managing stressors with reduced parental assistance. Compared with participants for whom FBT supported return to adolescent pursuits, these participants described more significant psychosocial difficulties prior to the onset of AN, particularly difficulties with anxiety and separating from parents. Whereas the former participants were motivated to return to adolescent activities, and this could be used to encourage normalisation of eating behaviours, these participants required direct assistance with developing the motivation and skills to develop social and practical independence.
Lilly described extreme shyness and difficulty separating from her mother as a child, which continued to affect her ability to form relationships outside the family as she developed. Sabrina and Alana were similarly described by their parents as anxious to separate, and had difficulty forming their own identity as they approached adolescence. Sabrina’s mother described that Sabrina was her ‘little shadow’ who, as she got older, ‘wanted to copy everything I did’. Emily described being very close with her parents prior to adolescence; upon reaching adolescence and developing AN, this became a problematic inability to create relationships outside the family, stalling her development: ‘Independence, things like boyfriends, going to parties, new relationships. I couldn’t connect with that at all, it kind of scared me . . . If it was outside of family, I would get really nervous and scared’. In phase one, FBT was noted to increase overdependence on parents. However, in phases two and three, a key role of the therapist was to guide parents to allow a developmentally appropriate level of freedom. For some parents, this helped to address overprotectiveness that had been present prior. Lilly’s mother explained that later in treatment, Lilly ‘learnt to be independent herself and I had to let her go as a mum’. For these participants, individual therapy after FBT was noted to be particularly helpful in allowing the young person the independence of addressing intra-psychic issues with someone outside the family. This was able to be done only once the young person had, with the assistance of FBT, regained responsibility for their own eating and gained sufficient independence to be able to begin addressing difficulties alone with a therapist.
Both Briony and Lilly’s mothers described a continuing developmentally atypical level of reliance on them for assistance in regulating emotions; Lilly’s mother noted that ‘She still does call me a lot when she’s having a bad day . . . does rely on me to manage her emotions’. Emily observed that she believed increased dependence in phase one had had a lasting effect, although it had been necessary for her physical recovery. She noted a great deal of difficulty transitioning to phase two, and current ongoing difficulties with autonomy, both in terms of eating and more broadly, including difficulty sustaining independent relationships: ‘I was kind of attached to my parents because I had relied on them for so long . . . I think later on it [phase one] might have contributed to not being able to do things on my own’. She noted remaining somewhat behind her peers in terms of independence from family, but feeling she was steadily progressing: ‘I feel like I’m behind but I’ll get there . . . It’s almost like I have to do it manually; they [peers] did it automatically’.
Providing freedom to develop post-FBT
Five participants described disengagement from FBT throughout all phases, and only achieving broader recovery post-FBT. These participants tended to describe a greater degree of developmental difficulty prior to the onset of AN. Disengagement included lack of active participation in therapy and lack of contribution in sessions, resistance to therapeutic efforts throughout the phases of treatment and reluctance to share information with the therapist. Young people’s attitudes remained ambivalent regarding weight gain and change in eating behaviours, and their relationship with the therapist remained somewhat stagnant, with little shift towards greater cooperation. They reflected that phase one had successfully facilitated weight gain purely by working with their parents, and this had been necessary for their later steps towards broader recovery. Gradual transfer of control back to the young person was difficult, and in some instances the patient felt it would have been more helpful for them to gain control in other areas of their life before attempting to let go of rigid control with respect to eating. These participants particularly emphasised the importance of reaching a point of making their own decision to work towards recovery, independent of the influence of parents or the therapist.
Compared with other participants, these young people described poorer relationships with parents and more pronounced family conflict and stress during the time they were unwell. This included lack of understanding from family, violence towards parents, and high expressed emotion in and outside the therapy room. Attempts by the therapist to address adolescent issues in phases two and three were largely unsuccessful, as the young person remained disengaged. Barriers to engagement cited included the above-mentioned family difficulties, lack of a positive therapeutic relationship, and strong negative feelings about weight gain and how this had been achieved. Changes in some participants’ lives external to therapy precipitated recovery by bringing about increased self-confidence and an expanded identity. Others described becoming worn out by the disorder and treatment, leading them to work towards leaving FBT and re-engaging with development on their own. Sally explained: ‘Therapy helped, but not in the way I thought it would . . . It helped me by annoying me until I wanted to avoid it . . . I just wanted to be living my life’. Briony described that she ceased FBT physically recovered but still psychologically unwell. Changes such as leaving school, choosing a career, getting a job and forming new friendships facilitated increased confidence and a greater sense of independence. As a result, eating disorder cognitions and behaviours gradually faded. Her mother observed: ‘She matured, that’s what got her through. Getting a bit of independence, got her licence and that sort of stuff, and left school . . . She went and did TAFE for six months . . . Those things were really important’.
Lexi explained that FBT was unable to assist beyond weight gain, due to previous abuse in the family that compromised her level of trust in her parents as a resource to assist recovery. However, the therapist was able to help with practical changes which facilitated independence, and she believed this was a catalyst for her broader recovery. Other psychosocial changes such as forming a long-term intimate relationship were also recalled to have been important. Similarly, Sally’s mother described key experiences post-FBT that appeared to bring about positive change in her confidence, including taking up a leadership position at school and commencing creative pursuits.
Discussion
The aim of this study was to explore the role that FBT plays in fostering adolescent development beyond the markers of weight and eating disorder symptomatology. We aimed to explore the lived experience of adolescent development, as defined, and told retrospectively, by both young people and their parents. At the time of recruitment, all participants in this study were within a healthy weight range, and most fell within the range of community norms in terms of eating disorder psychopathology, indicating they no longer met the diagnostic criteria for AN. The findings of this study suggest that AN is highly disruptive to social development, growth of autonomy and adolescent exploration. FBT played a varied role in addressing developmental issues, with three distinct routes towards maturity identified.
Findings support the view that phase one of FBT brings about a temporary increase in dependence on parents (Lock & Le Grange, 2013). Overall the results of this study indicate that this does not cause lasting developmental disruption for most young people, but caution may be needed where young people have pre-existing difficulties gaining independence from parents. Incorporating efforts to enhance the young person’s autonomy in non-eating-related areas during phase one may assist, so long as this does not interfere with weight restoration.
The first two developmental routes, supporting return to adolescent pursuits and facilitating autonomy, aligned most closely with the trajectory of treatment suggested in the manual (Lock & Le Grange, 2013). Participants reported that phase two shifted the locus of control to the young person. For many adolescents, the transition to phase two can be highly fraught. The young person may return to previous eating disorder behaviours, or increase resistance to treatment (Wagner, Diamond, Levy, Russon, & Litster, 2016). The results of this study offer insight into the mechanisms that may make this transition successful. For some young people, therapist guidance in re-engaging them in developmentally typical activities appears to be key in motivating change in eating disorder behaviours. This is a particularly helpful strategy for adolescents who were largely on-track developmentally prior to the onset of AN. It should be noted that participants who described FBT as assisting them in this way tended to have had a longer period since ceasing FBT from the time of interview, suggesting that temporal distance from their experience of treatment may have played a role in their reflections. Where excessive control or involvement of parents was a difficulty prior, it may be effective to utilise the process of handing back responsibility for eating to the young person to address this; for example, by challenging parents’ ideas regarding developmentally appropriate autonomy. Thus, while the chief focus of phase two is facilitating age-appropriate responsibility for eating, findings suggest this process also often involves reengaging the young person in adolescent activities and facilitating autonomy more broadly. For these young people, results suggest assisting the adolescent to resolve the developmental problem of forming relationships outside the family is key to recovery, although given the small sample this can only be suggested tentatively.
Results indicated that some young people, particularly those who were older, felt that social and psychosexual issues were best left for individual therapy post-FBT. However, consistent with the findings of previous qualitative research (Krautter & Lock, 2004), others expressed that they would have benefitted from more time in phase three to address psychosocial issues, particularly body image, self-esteem and social relationships. Results suggest an individual treatment such as AFT may be appropriate for some young people who felt that underlying difficulties such as coping with expectations associated with becoming an adult or difficulties with self-esteem were not adequately addressed within FBT (Fitzpatrick et al., 2010). Particularly for older patients, the ‘broad’ form of CBT-E, in which focus is given to broader maintenance factors such as low self-esteem, interpersonal issues and perfectionism, may be an appropriate way for underlying issues to be addressed (Fairburn, 2008). Findings suggest, however, that for some young people, individual support post-FBT that does not have an eating disorder focus is most appropriate.
The third developmental trajectory, providing freedom to develop post-FBT, was less consistent with the phases laid out in the manual, indicating that the sequence of manualised FBT may be less applicable for these families post phase one. FBT was unable to assist the young person to return to healthy development, beyond physical recovery. For participants describing this route, the importance of a motivational shift was emphasised. Previous qualitative research has identified factors that enhance self-determined steps towards recovery, including increased understanding from and connection to significant others (Dawson, Rhodes, & Touyz, 2014a). The experiences reported by these participants were consistent with the findings of previous qualitative research, suggesting that therapy is one of many contributors to recovery, and psychosocial changes, such as the development of meaningful relationships and activities, are key (Hay & Cho, 2013). Therapist involvement in bringing about significant psychosocial changes that enhance motivation for change may be helpful for these patients. FBT utilises the assumption that nutritional recovery is an essential first step, and may be the catalyst for broader recovery (Accurso, Ciao, Fitzsimmons-Craft, Lock, & Le Grange, 2014; Lock & Le Grange, 2013). For participants who experienced developmental recovery post-FBT, physical recovery in phase one appeared to be essential to broader change, which occurred despite lack of direct attention to developmental issues in treatment. The experiences of these participants suggest the value of persistence in FBT with young people who appear disengaged, since physical recovery and independent management of weight-related behaviours was experienced as a precursor to working towards broader recovery at a later stage. Quantitative data indicated only minor differences between developmental routes, indicating that these participants may not have fared more poorly than others in terms of eating disorder psychopathology and attachments. Further research is required to improve identification of for which young people direct attention to adolescent developmental issues is most likely to be helpful.
Some participants for whom FBT provided freedom to develop post-treatment emphasised the role of conflict and/or lack of close attachment with parents in limiting the effectiveness of phases two and three. Attachment quality, as indicated by IPPA scores, suggested some continuing difficulties in this regard. These young people may thus benefit from a strong focus on addressing relational issues before parental assistance is enlisted to aid development (Wagner et al., 2016).
Strengths, limitations and recommendations for future research
The key strengths of this study included the selection of a range of participants in terms of current age, age of onset and time elapsed since completion of FBT, and enhancement of methodological rigour through the use of member checking and multiple forms of triangulation. The findings contribute to our knowledge of the developmental focus of FBT, as well as the often-neglected view of the young person.
In terms of triangulation, the inclusion of both young people and their parents was particularly important. These data were combined in the analysis as there were no clear overall differences in the narratives of young people and parents. It appeared that the family therapy model increased communication between family members and resulted in a common ‘family narrative’ of their experiences. Reflection as a family since ceasing FBT may also have contributed to the development of a common narrative.
This study also had some limitations. The focus was the role of FBT in facilitating developmental recovery, and as such, only young people who had received a substantial portion of phase two/three treatment were included. This meant, however, that the experiences of those for whom FBT was not successful in facilitating weight gain were absent. Future qualitative research exploring the narratives of these young people would be valuable in allowing critique and improvement of the model. While participants’ files were used to verify their adequate completion of phases two and three, these phases were at times difficult to distinguish from patient records, and thus some participants who may not have completed sufficient sessions of phase three may have been included.
This study investigated retrospective experiences of treatment only. Some participants had limited recall, due to the time elapsed or possible cognitive compromise during the time they were unwell. While investigating retrospective perspectives had the advantage of allowing participants to tell a more complete story, this may have resulted in poorer accuracy and detail, and future investigations exploring young people’s perspectives while receiving FBT could offer rich and insightful data.
This study has identified some of the developmental areas that young people and their parents see as key to address in the latter phases of FBT. Future research could utilise quantitative measures to evaluate FBT in terms of developmental, as well as physical and psychological, outcomes.
Conclusion
The findings of this study suggest that developmental difficulties are both a risk factor for and a consequence of adolescent AN. Young people often view AN as an attempt to manage pre-existing developmental challenges, and phases two and three of FBT have an essential role in providing alternative ways to negotiate these difficulties. The nature of the role of FBT in assisting developmental recovery is varied. For some young people, FBT plays a key role in easing their return to activities that promote healthy development, or in adjusting their relationship with their family or origin to be more developmentally appropriate. For others, the role of FBT is largely limited to weight gain; however, this can allow young people to find their own path back to healthy development post-treatment. The results suggest that formulation in terms of developmental difficulties is essential in managing challenges that may arise in progressing through the phases of FBT, as well as determining the likely priorities for phases two and three.
Footnotes
Acknowledgements
We wish to acknowledge the generosity of the participants in this study in sharing their experiences, and the contribution of the family therapists and other clinicians at the Eating Disorder Service at the Children’s Hospital at Westmead.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: M.M. received an Australian Postgraduate Award which supported the research, authorship, and/or publication of this article.