
Abstract
Background:
Medically unexplained symptoms affect between 4% and 20% of children and adolescents; 30–60% of these children also experience mental health difficulties. Trials and reviews have focussed on physical gains in this population, often overlooking mental health outcomes.
Objectives:
To use a systematic review methodology guided by the PRISMA checklist to (1) investigate the effectiveness of psychological interventions for mental health difficulties in children and adolescents with medically unexplained symptoms and (2) identify aspects of interventions associated with their success.
Methods:
Randomised controlled studies investigating the impact of psychological interventions on mental health in children and adolescents with medically unexplained symptoms were included. Systematic searches of PsycINFO, MEDLINE and CINAHL were undertaken from inception to January 2018. Studies were appraised using the quality appraisal checklist. A qualitative synthesis of studies was completed.
Results:
In all, 18 studies were identified. Interventions targeting parental responses to illness and family communication appeared to have the best outcomes.
Conclusions:
Psychological interventions may be effective in improving mental health outcomes within this population; however, evidence for the efficacy of these interventions is limited due to a high risk of bias within the majority of reviewed studies. Future research using rigorous methodology and non–cognitive behavioural therapy interventions is recommended.
Introduction
There is a historical and current lack of clarity around the definition of medically unexplained physical symptoms, which is acknowledged within the research community (Lieb, Pfister, Mastaler, & Wittchen, 2000) and within clinical practice, with different interpretations of symptoms between medical specialities (Hinton & Kirk, 2016). The term medically unexplained symptoms, which will be used in the current review, applies to physical symptoms that cannot be accounted for by a disease-specific pathology.
According to the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5), if a collection of significantly debilitating symptoms is experienced over a long period of time and accompanied by disproportionate thoughts, emotions or behaviours, these symptoms may be categorised as somatic symptom disorder (American Psychiatric Association (APA), 2013). Physical symptoms can therefore be medically explained or unexplained and still fall under the somatic symptom disorder category if thoughts, emotions or behaviours relating to the illness are deemed excessive (APA, 2013).
Brown (2007) suggests that medically unexplained symptoms are experienced on a spectrum, ranging from solitary fleeting and mild to multiple and chronic. He also proposes that individual experiences of symptoms are reported in different ways. For children, developmental stage impacts how symptoms are expressed and communicated, and therefore, execution of robust epidemiological studies indicating accurate child prevalence has proven highly challenging (Hinton & Kirk, 2016).
Several longitudinal and cross-sectional studies have estimated numbers of children experiencing medically unexplained symptoms to be between 4% and 20%, with a higher prevalence in younger children (Domènech-Llaberia et al., 2004; Eminson, Benjamin, Shortall, Woods, & Faragher, 1996). In a longitudinal study of children followed from the age of 9 to 13 years in the United States, headaches were found to be the most common medically unexplained symptoms, followed by abdominal pain and musculoskeletal pain, although co-occurrence of symptoms was frequently described (Egger, Costello, Erkanli, & Angold, 1999). Medically unexplained symptoms are reported more often and to a higher degree in females throughout childhood and adolescence (Berntsson, Kohler, & Gustafsson, 2001).
Between 30% and 60% of children and adolescents reporting medically unexplained symptoms are thought to also be experiencing mental health difficulties meeting criteria for psychiatric diagnosis, such as anxiety and depression (Lieb et al., 2000). Although their aetiology remains unclear, several psychological theories describe causes and maintenance of medically unexplained symptoms linking physical symptoms with emotional distress (Husain, Browne, & Chalder, 2007).
Rationale for review
There have been several recent systematic reviews and meta-analyses of the evidence for psychological interventions in children with medically unexplained symptoms (e.g. Bonvanie et al., 2017; Fisher et al., 2014). Generally, these reviews have illustrated benefits of psychological therapies in terms of improvements of physical symptoms including reduction of pain, fatigue and irritable bowel syndrome (IBS) symptoms and functional outcome including improvements in school attendance and daily activities. However, review and synthesis of mental health outcomes have been scarce and largely unclear (Fisher et al., 2014). Trials and reviews have generally prioritised physical and practical gains, and where mental health results are included, they have mainly been measured as secondary outcomes. In a systematic review of psychological interventions for pain in children, Fisher et al. (2014) found insufficient evidence to draw conclusions relating to mental health outcomes, including anxiety. Given the co-morbidity of mental ill-health and medically unexplained symptoms, more focus should be placed on understanding and synthesising the evidence for reducing distress including depression and anxiety in these populations.
Objectives
The aims of the current review are as follows:
To investigate the efficacy of psychological interventions for mental health difficulties in children and adolescents with medically unexplained symptoms.
To identify significant aspects of interventions associated with their success, for example, presence/absence of parents and mode of delivery.
A systematic review methodology was used in order that the review could be repeated as the evidence base in relation to mental health symptoms and medically unexplained symptoms in children and adolescents increases.
Methodology
Search methods
Systematic review methods were carried out using Cochrane guidelines (Higgins & Green, 2008, See Supplementary File 2 for Data Extraction Checklist). The review was registered with PROSPERO (registration number: CRD42016035817). Electronic, reference list and citation searches were carried out in PsycINFO, MEDLINE and CINAHL databases from inception to January 2018 (See Supplementary File 1 for search terms by database). The search terms were largely categorised into three main areas: (1) medically unexplained symptoms, (2) mental health difficulties and (3) psychological intervention. To be inclusive, a wide range of search terms were applied. These were taken from various sources including adult functional symptoms by speciality (Wessely, Nimnuan, & Sharpe, 1999), the child somatisation inventory (Walker, Garber, & Greene, 1991) and the somatic symptom checklist adapted for adolescents (Eminson et al., 1996). Reference and citation lists of identified studies were examined for additional studies.
Inclusion criteria
Types of studies
Only randomised controlled trials published in a peer-reviewed journal in the English language were examined.
Types of participants
Study participants were children and adolescents up to the age of 18 years with medically unexplained symptoms. These were defined as any physical symptom causing distress or impeding function which was not accounted for through medical explanation. This definition was used in the absence of an agreed upon description that is consistently used by researchers and clinicians with regard to children and adolescents.
Types of interventions
Psychological interventions were included in the review. Psychological interventions were defined as any interventions which are specifically designed to alter psychological processes thought to underlie or significantly contribute to distress and suffering (Fisher et al., 2014). Examples include cognitive therapy, behavioural therapy, psychodynamic therapy, systemic family therapy, parent therapy designed to modify child behaviour and biofeedback (See Supplementary File 4 for a Table of treatment and outcomes of included studies).
Comparator
Comparators included any established psychological interventions, waiting list, treatment as usual, or attention control (See Supplementary File 3 for a description of control groups of included studies).
Outcome measures
Diagnostic interviews and child mental health measures relating to common mental health problems including depression, anxiety and child behaviour were included. Parent reports of child mental health (but not parent mental health) were included (See Supplementary File 3 for a description of the outcomes of included studies).
Exclusion criteria
Studies not reporting a mental health outcome measure, including studies using quality-of-life measures as opposed to measuring mental health outcomes, were excluded. Grey literature and unpublished dissertations were also excluded.
Data collection and analysis
Study selection
Studies were selected based on the above criteria. Abstracts were read and full-text articles were accessed by the first author to examine articles for eligibility where necessary.
Data extraction
Data extraction was carried out using the Cochrane data extraction checklist (Higgins & Green, 2008).
Methodological quality assessment
The review employed the quality appraisal checklist for quantitative evaluative studies (National Institute for Health and Clinical Excellence (NICE), 2012). This tool was chosen for its ability to appraise controlled intervention studies of varying quality within the area of public health research. Both internal and external validity are rated as strong (++), adequate (+) or weak (−) using predefined criteria from within the following domains: population and sampling, allocation, blinding, outcome measurement, treatment delivery, attrition and analysis. Strong external and internal validity are indicative of a low risk of bias, while adequate or weak validity is indicative of a moderate or high risk of bias. Assessor blindness was included in the review; however, the blinding of participants and investigators in relation to treatment was excluded as this is rarely applicable to delivery or receipt of psychological treatments (Fisher et al., 2014). Study quality was assessed independently by a reviewer and a second rater who reviewed a random 20% sample of the included studies. The Kappa statistic indicated very good inter-rater agreement, Kappa = 0.8 (p < .01).
Results
The initial search identified 2441 articles, following removal of duplicates. A total of 18 studies, and 1 follow-up study, were eligible for inclusion. Figure 1 shows the study selection process using the PRISMA flow diagram (Liberati et al., 2009).

PRISMA flow diagram of study selection process (Liberati et al., 2009).
Description of included studies
Design and participants
All 18 studies reviewed were randomised controlled trials; 15 studies employed two arms, while 3 used three arms. A total of 1396 participants took part in the studies (see Table 1 for characteristics of included studies). Participants were largely female, with 15 studies reporting at least 15% more females than males. This is representative of the wider population, with prevalence rates of medically unexplained symptoms reported to be generally higher in females (Nijhof et al., 2011). Importantly for the present review, several studies employed stringent criteria which excluded participants based on their diagnostic status in relation to common mental health conditions (Chalder et al., 2010; Hickman, Jacobson, & Melnyk, 2015; Kashikar-Zuck et al., 2012; Kashikar-Zuck, Swain, Jones, & Graham, 2005; McGrath et al., 1992; Warner et al., 2011).
Characteristics of included studies.
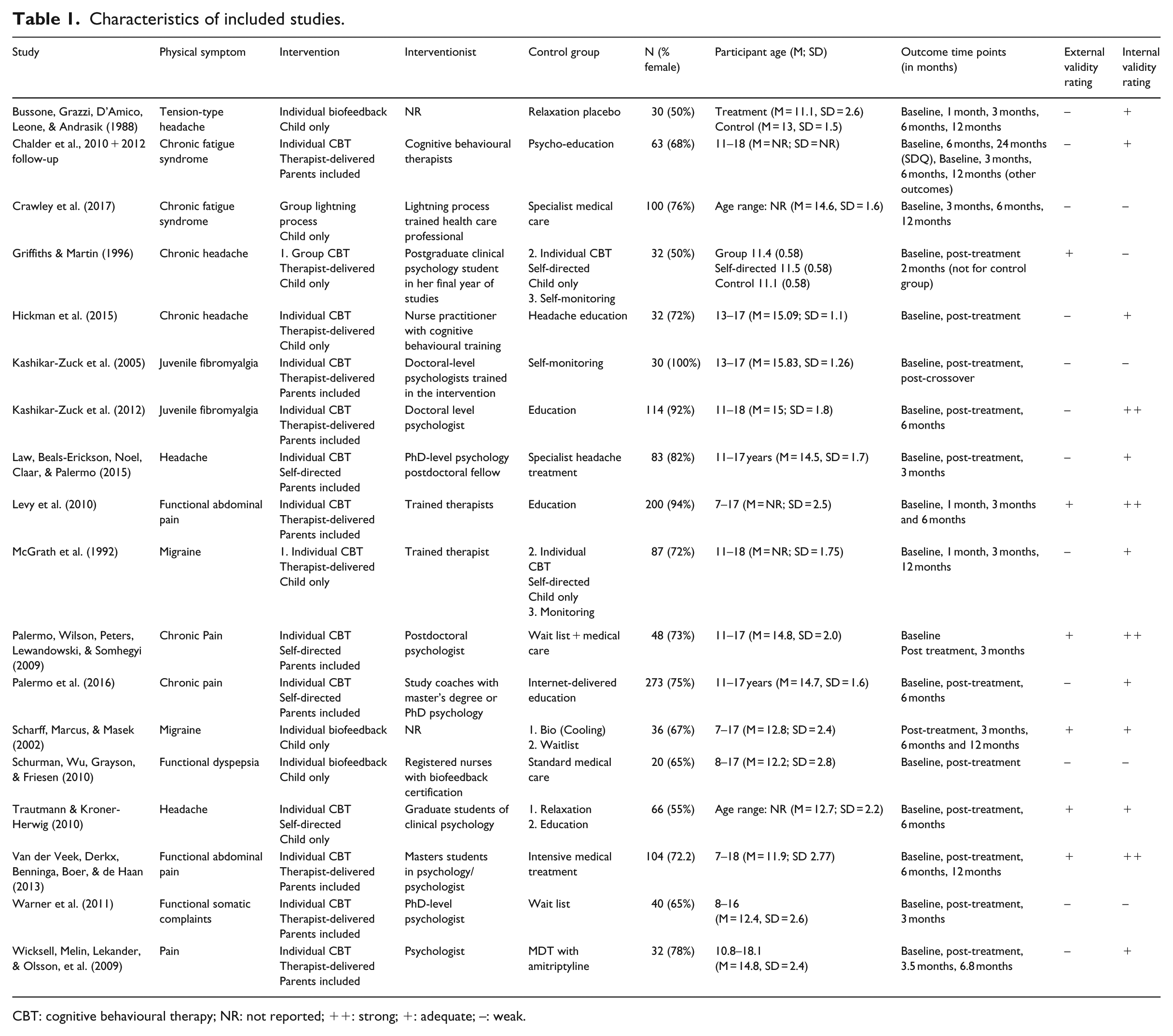
CBT: cognitive behavioural therapy; NR: not reported; ++: strong; +: adequate; −: weak.
Intervention
Interventions included face-to-face individual and group cognitive behavioural therapy (CBT), self-directed CBT, the ‘Lightning Process’ group therapy (developed from osteopathy, life-coaching and neurolinguistics) and biofeedback. Some of the CBT studies included parents, while others were child only. Where CBT studies included parents, nine reported using behaviour therapy directed at the parent (adapting parent responses to illness behaviours; Kashikar-Zuck et al., 2005, 2012; Law et al., 2015; Levy et al., 2010; Palermo et al., 2009, 2016; Van der Veek et al., 2013; Warner et al., 2011; Wicksell et al., 2009) and four involved strategies aimed at increasing parent–child communication (Chalder et al., 2010; Law et al., 2015; Palermo et al., 2009, 2016). See Table 1 for intervention type by study.
Outcome measures
In total, 36 outcome measures were used to examine outcomes across various domains including physical health, functional disability and mental health. All studies assessed self-report mental health with 16 measuring mood and 14 assessing anxiety. One study assessed anxiety through diagnostic interview (Warner et al., 2011). All trials measured self-report physical health experience, while three included objectively measured physical health status (tender point examination and electromyography (EMG); Bussone et al., 1998; Kashikar-Zuck et al., 2005, 2012). Eleven studies assessed functional disability (Chalder et al., 2010; Crawley et al., 2017; Hickman et al., 2015; Kashikar-Zuck et al., 2005, 2012; Law et al., 2015; Levy et al., 2010; Palermo et al., 2009, 2016; Van der Veek et al., 2013; Wicksell et al., 2009). See Supplementary File 3 for a description of the outcome measures of included studies.
Internal validity
Study design was generally simple, involving one or two treatment groups evaluated against a waiting list, treatment as usual or placebo control group. Randomisation procedures were generally acceptable; however, blindness in relation to measurement of outcome was usually unclear, with just two studies making reference to the manner in which self-report measures were administered by investigators at baseline and outcome (Law et al., 2015).
Investigators and participants were not blind to intervention delivery for any study due to the psychological nature of treatments. It is therefore imperative that careful attention is paid to condition equivalence in the design of psychological treatment studies to ensure control condition credibility is maximised and active treatment components can be identified (Fisher et al., 2014). For the studies included in the current review, condition equivalence within trials was poor, with just half of the trials employing control groups controlling for participant time or therapist time spent with participant and six trials (Crawley et al., 2017; Kashikar-Zuck et al., 2005; Palermo et al., 2009; Schurman et al., 2010; Warner et al., 2011; Wicksell et al., 2009) failing to control for participant attention altogether. Furthermore, treatment and control condition credibility, allocation of therapist to control or treatment group and supervision of therapists were cited infrequently. In addition to this, although manualisation of treatment was high, adherence to manuals was assessed by an independent evaluator in only three trials (Kashikar-Zuck et al., 2012; Levy et al., 2010; Wicksell et al., 2009).
Most studies accounted for group differences at baseline and through analyses and attrition was acceptably low for most trials. However, attrition bias was generally unclear, with studies rarely referring to differences between groups’ attrition rates or differences between completers and non-completers. Power within trials was largely weak, with less than half of studies reporting adequate power (⩾80%) to detect between groups differences for mental and physical health outcomes (Chalder et al., 2010; Crawley et al., 2017; Kashikar-Zuck et al., 2012; Law et al., 2015; Levy et al., 2010; Palermo et al., 2009, 2016; Van der Veek et al., 2013) increasing the possibility of Type II errors in the remainder of studies. In addition, intention-to-treat analysis was not carried out for the majority of studies, and adjustment of alpha level to correct for multiple statistical tests was rarely conducted or mentioned, increasing the likelihood of a Type I error. Furthermore, results from analyses conducted were not fully reported for several of the studies, suggesting a high degree of reporting bias and undermining the usefulness of pooling information about the effectiveness of these interventions.
Outcome measures employed were generally adequate. All studies were deemed to have employed relevant, reliable and valid outcomes, although five studies did not specifically measure anxiety, measuring either emotional symptoms or mood only (Chalder et al., 2010; Kashikar-Zuck et al., 2005, 2012; McGrath et al., 1992; Palermo et al., 2009). In addition, three studies did not measure mood, measuring either anxiety only or emotional symptoms (Bussone et al., 1998; Chalder et al., 2010; Warner et al., 2011). See Supplementary File 5 for a summary of the quality appraisal and see Supplementary File 6 for a risk of bias table based on the categories of the Quality Appraisal Checklist (NICE 2012).
External validity
Studies generally had weak external validity due to poor description and comparison of source population characteristics with study participants, high numbers of recruitment from specialist centres, such as pain management services and poor sampling methods. In addition to the strict inclusion/exclusion criteria previously described, these concerns limit the generalisability of the studies included in the current review. See Supplementary File 5 for a summary of the quality appraisal and see Supplementary File 6 for a risk of bias table based on the categories of the Quality Appraisal Checklist (NICE 2012).
See Table 1 for a summary of the results of the quality appraisal pertaining to the categories of the NICE (2012) quality appraisal checklist.
Effects of interventions
Generally, studies demonstrated mixed findings relating to treatment and control group differences on mental health, as well as physical health outcomes.
CBT: child-only therapist delivered
Two studies evaluated the effect of individual (child-only) therapist–delivered face-to-face CBT approaches on headache and mental health outcomes (Hickman et al., 2015; McGrath et al., 1992). Both studies used education control groups, and McGrath et al. (1992) also included a guided self-help group. Neither study reported a significant difference between the treatment group and control groups on mental health measures. Similarly, Hickman et al. reported no significant difference between treatment and control groups on headache scores. McGrath et al. reported a significantly greater reduction on headache scores in their guided self-help control group, compared with their education control group and their clinic-based CBT group. For each of these studies, significant within-group improvements from pre- to post-treatment were observed on headache scores and on at least one mental health outcome (depression or anxiety) for both treatment and control groups. McGrath did not report anxiety outcomes, reporting on depression outcomes only in relation to mental health.
Similarly, for the group-based therapist-delivered (child-only) CBT programme (Griffiths & Martin, 1996), significant differences between the treatment and control (self-directed CBT and waitlist) groups were not observed on mental health outcomes, including self-report depression and anxiety measures. Conversely, there was a significantly greater reduction in headache scores for the group-based therapist-delivered CBT and the self-directed individual CBT compared with the waitlist group. A significant within-group improvement in anxiety scores (but not depression scores) from pre- to post-treatment was observed for the group-based therapist-delivered CBT intervention, but not for the self-directed CBT or the waitlist. Similar to the above-mentioned face-to-face individual CBT interventions, this group-based intervention did not report inclusion of parents.
CBT: child and parent therapist delivered
Significant between-group differences on mental health outcomes are reported for six of the seven studies employing therapist-delivered CBT involving parents (Chalder et al., 2010; Kashikar-Zuck et al., 2012; Levy et al., 2010; Van der Veek et al., 2013; Warner et al., 2011; Wicksell et al., 2009). Parents were included in techniques that aimed to adapt parent responses to illness behaviours and increase parent–child communication. The number of sessions including parents varied between studies from parental involvement in one session to parental involvement in all sessions. Four of these studies measured child anxiety using self- and parent-report outcome measures (Levy et al., 2010; Van der Veek et al., 2013; Wicksell et al., 2009) and clinician report (Warner et al., 2011). All four reported significantly greater improvements post treatment in the treatment group compared to the control groups, which included education (Levy et al., 2010), intensive medical care (Van der Veek et al., 2013; Wicksell et al., 2009) and waitlist control (Warner et al., 2011). Although treatment gains in the intervention groups tended to be maintained at follow-up, between-group differences were no longer significant for two of the studies at follow-up due to the control group also improving (Van der Veek et al., 2013) or because follow-up data were not collected due to the control group receiving the treatment (Warner et al., 2011).
A similar pattern was seen for depression, which was measured through self-report instruments, with three out of the five studies which measured child depression reporting a significantly greater improvement at post-intervention in the treatment groups compared with the control groups which included education (Kashikar-Zuck et al., 2012; Levy et al., 2010) and intensive medical treatment (Van der Veek et al., 2013). While treatment improvements were upheld, between-group differences were observed for only one of these three studies at follow-up (Van der Veek et al., 2013), as control groups had also improved (Kashikar-Zuck et al., 2012; Levy et al., 2010). Kashikar-Zuck et al. (2005) reported within-group improvements in depression scores from pre- to post-treatments for both groups; however, differences between the treatment and waitlist control groups were not observed.
Chalder et al. (2010) measured children’s emotional and behavioural functioning using parent- and self-report questionnaires and found significantly greater improvement in the treatment group compared with the education control group from pre-treatment to 24-month follow-up, but not from pre-treatment to 12-month follow-up, when the control group had also shown improvement (Chalder et al., 2010; Lloyd, Chalder, & Rimes, 2012).
Regarding physical health outcomes, Chalder et al. (2010) and Van der Veek et al. (2013) reported no significant differences between groups from pre- to post-treatment or at follow-up on self-report fatigue and pain scores. However, Kashikar-Zuck et al. (2005, 2012), Levy et al. (2010), Warner et al. (2011) and Wicksell et al. (2009) reported significant improvements in treatment groups compared with control groups on physical symptoms including pain and functional somatic complaints from pre- to post-intervention and at follow-up.
CBT: self-directed
With regard to self-directed CBT with therapeutic contact via email or phone, the findings were inconclusive. One of these studies (Trautmann & Kröner-Herwig, 2010) involved individual (child-only) content and had an education control group, while three also included content for parents and employed specialist medical care (Law et al., 2015) waitlist (Palermo et al., 2009) and education (Palermo et al., 2016) control groups. Palermo et al. (2009) reported self- and parent-reported depression scores only, while the other three studies reported both anxiety and depression outcomes. No significant differences between treatment and control groups were reported on mental health outcomes for three out of four of these trials (Law et al., 2015; Palermo et al., 2009; Trautmann & Kröner-Herwig, 2010). Significant differences in pain intensity were observed between treatment and control groups from pre- to post-treatment for Palermo et al. (2009), but not for Law et al. (2015) or Trautmann and Kröner-Herwig (2010).
In one self-directed CBT trial, Palermo et al. (2016) reported a significantly greater improvement in the treatment group compared to the control group from pre- to post-intervention on depression and pain-related anxiety, but not on general anxiety scores. This difference was not observed at follow-up (6 months), as the control group had also improved. This study did not report between-group differences from pre- to post-intervention for the primary physical outcome measure, pain intensity; however, a significantly greater improvement was seen in the treatment group compared with the control group for activity levels.
Where self-directed CBT studies failed to illustrate between-groups effects, all showed significant within-group effects on the intervention group on at least one mental health outcome measure on at least one time-point (Trautmann & Kröner-Herwig (2010): pain catastrophising, a measure of anxiety, at post-treatment and 6 months; Palermo (2009): depression at 3-month follow-up; Law et al. (2015): depression at 3-month follow-up). Control groups also showed these improvements at these times points, although for Palermo (2009), the control group was not followed up as they had received the treatment.
Lightning Process
On the ‘Lightning Process’ trial, a significantly greater improvement in the treatment (Lightning Process plus specialist medical care) compared with the control group (specialist medical care alone) was observed from pre- to post-intervention on self-reported depression and anxiety scores, as well as physical function and fatigue scores. These differences remained significant at 6- and 12-month follow-up for anxiety, physical function and fatigue and at 12-month follow-up for depression.
Biofeedback
For the three biofeedback studies, one measured the effect of an intervention on self-reported anxiety (Bussone et al., 1998) and the others on self-reported depression and anxiety (Scharff et al., 2002; Schurman et al., 2010). Bussone et al. (1998) reported a significant difference from pre-intervention to follow-up between the treatment and relaxation control group on trait anxiety; however, once baseline levels were adjusted for, these effects disappeared. The other biofeedback studies, which employed relaxation and standard medical care control groups found no significant effects on mental health outcomes (Scharff et al., 2002; Schurman et al., 2010). However, all three biofeedback studies demonstrated significantly greater improvements in the treatment group compared to control groups on physical outcome measures including pain and headache.
Meta-analysis
As the current data did not meet recommendations for meta-analyses outlined in the Cochrane guidelines, including a low risk of bias within studies and homogeneity across studies, it was concluded that a meta-analysis of these data would not be meaningful (Higgins & Green, 2008). The studies comprise a clinically diverse population (headache, gastroenterological complaints, pain and chronic fatigue syndrome (CFS)), diverse treatment delivery (family, individual and self-directed CBT, Lightning Process and biofeedback) and diverse mental health outcome measures. Furthermore, the presence of bias was noted in the majority of the studies with 10 studies judged to have low internal or external validity and four studies judged to have low internal and external validity. According to the Cochrane guidelines, if bias is present in all or a percentage of the individual studies, meta-analysis is likely to compound biases and yield a misleading result (Higgins & Green, 2008). Furthermore, several studies failed to report treatment effect sizes necessary for collation of data. Taking each of these factors into account, it was decided that a meta-analysis would not currently add useful information to the evidence base.
Discussion
A total of 18 trials met inclusion criteria for the current review. The main findings in relation to the two study aims were as follows:
Evidence for the efficacy of psychological interventions for common mental health difficulties in children and adolescents with medically unexplained symptoms is limited due to a high or unclear risk of bias within the majority of these studies. Inferences should be considered within this context.
Treatments which include parents and which are delivered by a therapist (as opposed to self-directed modules) appear to yield better mental health outcomes compared to control groups, including education, self-monitoring, waitlist and intensive medical or MDT care.
Trials of face-to-face CBT, which involved parents, demonstrated promising outcomes in mental health, with these trials consistently showing significant differences between treatment and control groups. In addition, treatment gains were generally maintained in this group. In particular, those therapist-delivered interventions including components addressing parental responses to child illness behaviours consistently illustrated significant improvements in child anxiety (Levy et al., 2010; Van der Veek et al., 2013; Warner et al., 2011; Wicksell et al., 2009) and also showed reductions in child depression (Kashikar-Zuck et al., 2012; Levy et al., 2010; Van der Veek et al., 2013) when compared with control groups. Interventions including elements aimed at encouraging family communication about illness also demonstrated effectiveness in relation to child mental health when compared to a control group (Chalder et al., 2010; Lloyd et al., 2012). This is consistent with research linking parental modelling of illness behaviour and parental solicitousness of child illness behaviour with higher rates of child catastrophisation of symptoms, anxiety, depression and medically unexplained symptoms (e.g. Levy et al., 2004). Significant results were seen in studies that consisted solely of joint parent–child sessions and in those that included parents for a proportion of the sessions. Significant results were seen across the age range, with younger and older children showing improvements in mental health outcomes.
The results of delivery of individual and group CBT by a therapist in person or over the phone as well as results for self-directed CBT were inconclusive. Differences in mental health outcomes between groups were not generally observed for these studies; however, significant within-group improvements on mental health outcomes were observed from pre- to post-intervention for both treatment and control groups in the majority of these studies. It is possible, therefore, that the lack of power due to small sample sizes may have impacted results for these studies.
The ‘Lightning Process’ trial (Crawley et al., 2017) showed differences between treatment and control groups on anxiety and depression scores at several time points. These are promising results. However, since the ‘Lightning Process’ is a relatively new treatment and this is the only known randomised controlled trial (RCT) testing this method in young people, further research is necessary to establish consistent treatment effectiveness, particularly given the risk of bias found within this study.
The biofeedback trials (Bussone et al., 1998; Scharff et al., 2002; Schurman et al., 2010) did not demonstrate significant within- or between-group gains on any measure of mental health where baseline levels were controlled for. This indicates that there is currently no evidence to suggest biofeedback is a suitable treatment for mental health difficulties associated with medically unexplained symptoms.
Considering all of the studies in this review, improvement in mental health symptoms did not appear to be related to improvement in physical health symptoms at the post-treatment phase. Several studies illustrated reduction in medically unexplained symptoms, but not improvement in depression or anxiety (e.g. Bussone et al., 1998; Griffiths & Martin, 1996; McGrath et al., 1992). Other studies showed the reverse pattern (e.g. Chalder et al., 2010; Lloyd et al., 2012; Van der Veek et al., 2013).
However, given the strong relationship between mental health symptoms and medically unexplained symptoms, it is possible that mental and physical health symptoms interact and impact one another following treatment. Indeed, although there is good evidence for the effectiveness of psychological treatments for physical health outcomes for children with chronic pain, there is an overwhelming lack of evidence for lasting effectiveness on physical outcomes at follow-up (Fisher et al., 2014). This suggests that other factors may prevent maintenance of physical health gains. According to cognitive–behavioural models of medically unexplained symptoms, psychological processes can maintain physical symptoms. Indeed, in a review on psychological risk factors of unexplained pain, Keefe, Rumble, Scipio, Giordano and Perri (2004) found associations between persistent pain, pain catastrophisation and other anxiety-related beliefs, indicating that maintenance of physical symptom improvement following therapy may be impacted by mental health.
Research implications
The current review highlights several areas for further research. There was a lack of power to detect statistically significant differences between groups, particularly for studies measuring effectiveness of individual and self-directed CBT, and condition equivalence was poor. Furthermore, several studies employed stringent criteria which excluded participants based on their diagnostic status in relation to mental health conditions including depression and anxiety. This unfortunately limits participant numbers and generalisability of the studies particularly as previous studies have demonstrated that between 30% and 60% of the young people experiencing medically unexplained symptoms also meet criteria for these disorders (e.g. Lieb et al., 2000).
Research using large-scale RCTs controlling for participant time and attention and employing appropriate exclusion criteria are necessary to gauge the effectiveness of interventions in relation to mental health outcomes in children with medically unexplained symptoms.
For medically unexplained symptoms, physical health gains are prioritised and mental health outcomes are often viewed as an afterthought. This is reflected in the reviewed studies, where mental health measures were usually secondary outcomes and sometimes not fully reported. It is also reflected in numerous large-scale randomised controlled trials of psychological interventions for this population, where mental health outcomes have not been included (e.g. Levy et al., 2013). Trials are often deemed successful by authors if physical health outcomes improved, regardless of effectiveness in relation to mental health. Despite the widely recognised usefulness of the biopsychosocial model of health, the concept of the mind–body split (dualism) proposed by Descartes in the 17th century continues to direct Western language, health care and research. Future trials should assess the interaction between physical and mental health outcomes at various follow-up time points to examine the impact of these outcomes on each other over time. Data on this are currently sparse and could inform clinical intervention and explanatory theories of medically unexplained symptoms.
In addition, the majority of trials reviewed in the current review evaluated the effectiveness of CBT. Research using the RCT methodology has traditionally focussed on CBT, despite other types of intervention, including systemic and psychodynamic psychotherapies demonstrating promise within this population (e.g. Griffin & Christie, 2008; Söllner & Schüssler, 2001). This may be due to the nature of RCTs, which tend to require manualised interventions and categorisation of symptoms and outcomes (Shean, 2014). It may be useful for future research to investigate other intervention approaches within this population using rigorous research methodologies.
Clinical implications
Identifying key aspects leading to positive treatment outcomes is challenging for a number of reasons. According to Fisher et al. (2014), components of interventions are intended to interact and combine with one another to produce an effect, meaning that removing certain aspects of interventions or separating elements may not be useful. For the current review, while interventions were manualised, study protocols and available treatment manuals did not contain sufficient detail to thoroughly examine specific elements of treatment, for example, how much of the intervention focusses on which aspects, whether this differs across therapists and participants and whether therapist skill, therapeutic alliance or extra-therapeutic factors have also influenced results. Therefore, it is not possible to conclude based on these data whether one aspect of treatment is active, while another is not.
However, several studies within this review showed the benefits of including parents’ responses to illness behaviour or communication about illness within sessions. While further randomised controlled trials of sound quality with clear a priori hypotheses are necessary to support the significance of this treatment component, these findings may be clinically valuable. They illustrate the usefulness of including parents in sessions and are supported by theory (Bandura, 1977) and empirical evidence in the literature (Levy et al., 2004).
Conclusion
Psychological interventions may be effective in improving mental health outcomes for children and adolescents with medically unexplained symptoms. Interventions including aspects relating to parental responses to illness behaviour and family communication appeared to have the best outcomes. Biofeedback studies were not effective in reducing mental health symptoms, while further research is necessary to ascertain the effectiveness of individual and self-directed CBT, as well as the ‘Lightning Process’, for mental health outcomes in this population. Furthermore, given explanatory theories and research about the processes maintaining medically unexplained symptoms which emphasise the relationship of medically unexplained physical symptoms with psychological processes such as pain catastrophisation, researchers and clinicians should prioritise both physical and mental health outcomes. Related to this, while physical health gains did not appear to be associated with mental health improvement, further investigation should assess the interaction between physical and mental health outcomes at various time points to examine potential impacts of these outcomes on each other over time.
Supplemental Material
Supplementary_file_1 – Supplemental material for A systematic review of randomised controlled trials using psychological interventions for children and adolescents with medically unexplained symptoms: A focus on mental health outcomes
Supplemental material, Supplementary_file_1 for A systematic review of randomised controlled trials using psychological interventions for children and adolescents with medically unexplained symptoms: A focus on mental health outcomes by Christine O’Connell, Roz Shafran and Sophie Bennett in Clinical Child Psychology and Psychiatry
Supplemental Material
Supplementary_file_2 – Supplemental material for A systematic review of randomised controlled trials using psychological interventions for children and adolescents with medically unexplained symptoms: A focus on mental health outcomes
Supplemental material, Supplementary_file_2 for A systematic review of randomised controlled trials using psychological interventions for children and adolescents with medically unexplained symptoms: A focus on mental health outcomes by Christine O’Connell, Roz Shafran and Sophie Bennett in Clinical Child Psychology and Psychiatry
Supplemental Material
Supplementary_File_3 – Supplemental material for A systematic review of randomised controlled trials using psychological interventions for children and adolescents with medically unexplained symptoms: A focus on mental health outcomes
Supplemental material, Supplementary_File_3 for A systematic review of randomised controlled trials using psychological interventions for children and adolescents with medically unexplained symptoms: A focus on mental health outcomes by Christine O’Connell, Roz Shafran and Sophie Bennett in Clinical Child Psychology and Psychiatry
Supplemental Material
Supplementary_File_4 – Supplemental material for A systematic review of randomised controlled trials using psychological interventions for children and adolescents with medically unexplained symptoms: A focus on mental health outcomes
Supplemental material, Supplementary_File_4 for A systematic review of randomised controlled trials using psychological interventions for children and adolescents with medically unexplained symptoms: A focus on mental health outcomes by Christine O’Connell, Roz Shafran and Sophie Bennett in Clinical Child Psychology and Psychiatry
Supplemental Material
Supplementary_File_5 – Supplemental material for A systematic review of randomised controlled trials using psychological interventions for children and adolescents with medically unexplained symptoms: A focus on mental health outcomes
Supplemental material, Supplementary_File_5 for A systematic review of randomised controlled trials using psychological interventions for children and adolescents with medically unexplained symptoms: A focus on mental health outcomes by Christine O’Connell, Roz Shafran and Sophie Bennett in Clinical Child Psychology and Psychiatry
Supplemental Material
Supplementary_File_6 – Supplemental material for A systematic review of randomised controlled trials using psychological interventions for children and adolescents with medically unexplained symptoms: A focus on mental health outcomes
Supplemental material, Supplementary_File_6 for A systematic review of randomised controlled trials using psychological interventions for children and adolescents with medically unexplained symptoms: A focus on mental health outcomes by Christine O’Connell, Roz Shafran and Sophie Bennett in Clinical Child Psychology and Psychiatry
Footnotes
Review registration number: CRD42016035817
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by Canterbury Christ Church University, the National Institute for Health Research Biomedical Research Centre at Great Ormond Street Hospital for Children NHS Foundation Trust and University College London.
Supplemental material
Supplemental material for this article is available online.
Supplementary File 1: Search Terms by Database.
Supplementary File 2: Data Extraction Checklist (Higgins & Green, 2008).
Supplementary File 3: Description of Control Groups and Outcomes of Included Studies.
Supplementary File 4: Table of Treatment and Outcomes.
Supplementary File 5: Summary of Quality Appraisal Based on the Categories of the NICE (2012) Quality Appraisal Checklist.
Supplementary File 6: Risk of Bias Table Based on the Categories of the Quality Appraisal Checklist (NICE, 2012).
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.