
Abstract
Difficulties with emotion regulation have been identified as an underlying mechanism in mental health. This pilot study aimed at examining whether group skills training in emotion regulation for adolescents and parents as an add-on intervention was feasible in an outpatient child and adolescent psychiatric clinic. We also investigated if the treatment increased knowledge and awareness of emotions and their functions, increased emotion regulation skills and decreased self-reported symptoms of anxiety and depression. Six skills training groups were piloted with a total of 20 adolescents and 21 adults. The treatment consisted of five sessions dealing with psychoeducation about emotions and emotion regulation skills training. Paired-samples t test was used to compare differences between before-and-after measures for adolescents and parents separately. The primary outcome measure, Difficulties in Emotion Regulation Scale, showed significant improvement after treatment for both adolescents and parents. For adolescents, measures of alexithymia were significantly reduced. Also, emotional awareness was significantly increased. Measures of depression and anxiety did not change. In conclusion, group skills training as an add-on treatment can be feasible and effective but further studies are needed.
Introduction
Difficulties with emotion regulation have been identified as an underlying mechanism in mental health (Barlow et al., 2011; Payne, Ellard, Farchoine, Fairholme, & Barlow, 2014). Maladaptive strategies for emotion regulation, such as oppressing and avoiding emotions, tend to lead to vicious cycles of increased negative emotions that maintain psychiatric symptoms and suffering (Campbell-Sills, Ellard, & Barlow, 2014). Most definitions of emotion regulation emphasise strategies (in relationship to a specific goal) that humans use to influence the experience, intensity and expression of emotions (Barlow et al., 2011; Gross, 2014). Adaptive emotion regulation is a process that involves awareness and acceptance of emotions and the ability to modulate emotional responses, as well as controlling impulsive behaviours to act according to a long-term goal or value despite the presence of negative emotions (Gratz & Roemer, 2004).
Adolescence is a vulnerable time period with heightened emotional reactions which coincide with underdeveloped skills for emotion regulation. In fact, a recent study found a maladaptive shift in emotion regulation in adolescents aged 12–15 years, compared to both younger and older participants (Cracco, Goossens, & Braet, 2017). Difficulties with emotion regulation have been associated with both internalising problems, such as somatic complaints, anxiety and depression, and externalising problems, such as delinquent and aggressive behaviour (Garnefski, Kraaij, & van Etten, 2005; Neumann, van Lier, Gratz, & Koot, 2010), and psychiatric disorders, such as depression and anxiety, often have their onset during adolescence (Kessler et al., 2005). Taken together, these findings highlight the need for targeting emotion regulation skills in this age group.
Studies have shown that an increased capability to regulate emotions is advantageous in the treatment of several psychiatric diagnoses (Payne et al., 2014). Treatments that emphasise emotion regulation as a core component have been developed and shown to successfully reduce addiction, nonsuicidal self-injury, symptoms of posttraumatic stress disorder (PTSD), symptoms of borderline personality disorder (BPD) and depression and anxiety, to mention some examples (Barlow et al., 2011; Gratz & Tull, 2011; Linehan, 1993; Rathus & Miller, 2015). Emotion regulation treatments emphasise the need to acquire skills through practice. Dialectical behaviour therapy (DBT; Linehan, 1993) is one of the most disseminated treatments. One study, for example, showed that skills training on its own decreased participants’ symptoms of anxiety and emotion dysregulation (Neacsiu, Eberle, Kramer, Wiesmann, & Linehan, 2014). DBT has also showed promising results as a transdiagnostic treatment for depression and anxiety (Neacsiu et al., 2014; Neacsiu & Linehan, 2014), and has also been tested in a randomised control trial on adolescents (Mehlum et al., 2014). Another example is emotion regulation group therapy (ERGT; Gratz & Gunderson, 2006), which is based on DBT and acceptance and commitment therapy (ACT; Hayes, Strosahl, & Wilson, 2012), and was developed for BPD and self-harm. Good results have been observed in treatment studies (Gratz, Bardeen, Levy, Dixon-Gordon, & Tull, 2015; Gratz, Tull, & Levy, 2013), with increased emotion regulation skills and overall quality of life, and reduced self-harm, symptoms of BPD and depression (Bjureberg et al., 2016; Sahlin et al., 2017). Further examples are Barlow’s transdiagnostic treatment Unified Protocol (UP; Barlow et al., 2011), with promising effects on anxiety and depression for adults in both individual and group format (Bullis et al., 2014; Farchione et al., 2012; Gallagher et al., 2013).
The above-mentioned studies were all originally developed for adults, but have been modified for adolescents (Bjureberg et al., 2016; Coyne, Birtwell, McHugh, & Wilson, 2014; Ehrenreich-May, Queen, Bilek, Remmes, & Marciel, 2014; Rathus & Miller, 2015), and some also include parents in the treatment and skills training. Parents can potentially reinforce and maintain maladaptive strategies in adolescents, but they can also be suitable role models for more adaptive strategies (Trosper, Buzzella, Bennett, & Ehrenreich, 2009). Research has shown that when parents support the child’s emotional expression, for example, the child’s ability to regulate emotions improves (Trosper et al., 2009). There are thus advantages to be gained when adolescents and parents can learn and practice new skills together (Ginsburg & Schlossberg, 2002). Since emotion regulation difficulties seem to be an underlying mechanism for a wide range of psychiatric disorders, it would be interesting and meaningful to study emotion regulation treatment from a transdiagnostic perspective. The teaching of emotion regulation skills is not, however, used routinely in a systematic way in clinical practice, and to our knowledge, there are only a few studies (Bjureberg et al., 2016; Bjureberg et al., 2018) to date that examine the effects of emotion regulation interventions in adolescents in regular clinical settings. Difficulties in getting families to sign up for and complete extensive treatment programmes and a lack of competent therapists in these skills are other potential hindrances. Hence, many adolescents and their parents are not given the opportunity to increase their skills in emotional regulation.
The present study
This pilot study aimed at examining whether a short transdiagnostic add-on emotion regulation group skills training for adolescents and parents was feasible in an outpatient child and adolescent psychiatric clinical setting. Furthermore, it aimed at examining whether the treatment resulted in fewer difficulties with emotion regulation, increased emotional awareness and knowledge of emotions, and decreased levels of self-reported symptoms of anxiety and depression.
Method
Design and procedure
The present pilot study used an uncontrolled open trial design to examine the acceptability and utility of a transdiagnostic skills training in emotion regulation. Assessments were made at baseline (before treatment) and after treatment (five sessions). All patients were recruited from an outpatient child and adolescent psychiatric clinic during a period from September 2015 to February 2017. Six skills training groups completed the programme during the period from January 2016 to April 2017. No screening for suitability or motivation was done prior to group participation.
Participants
Participants were recruited from the outpatient unit of the child and adolescent psychiatric clinic in Linköping, Sweden. Before intake to the specialist clinic, every referral has been assessed by a child psychiatric specialist. Children and adolescents with a global functional level above 60 (as rated on the Children’s Global Assessment Scale (CGAS; Shaffer et al., 1983) are generally referred to primary care. Every adolescent who participated in the study had ongoing treatment for at least one psychiatric diagnosis and had moderate to severe functional impairment. Adolescent patients aged 14–17 years at the clinic were recruited through their ordinary therapists. In total, 41 participants were included in the study (see Figure 1 for flowchart of participants). The treatment was transdiagnostic and thus open to all patient groups and most diagnoses. Exclusion criteria were schizophrenia, ongoing psychosis or mania, drug or alcohol abuse, severe anorexia and/or known intellectual disability or autism. Participants with high-functioning autism and/or autistic traits were not excluded. All participating adults were either biological parents or foster parents of the included adolescents. Information about diagnoses, pharmacological treatment, length and frequency of treatment-as-usual (TAU) were gathered from patient charts (Table 1). There was an average of four adolescents in each group. After treatment, data from pre- and post-assessment were collected from 20 adolescents and 21 adults. Results are based on participants who completed the treatment, including those who only missed one session, and who filled in the before-and-after measures.

Flowchart of participants.
Adolescents’ demographics (n = 20).
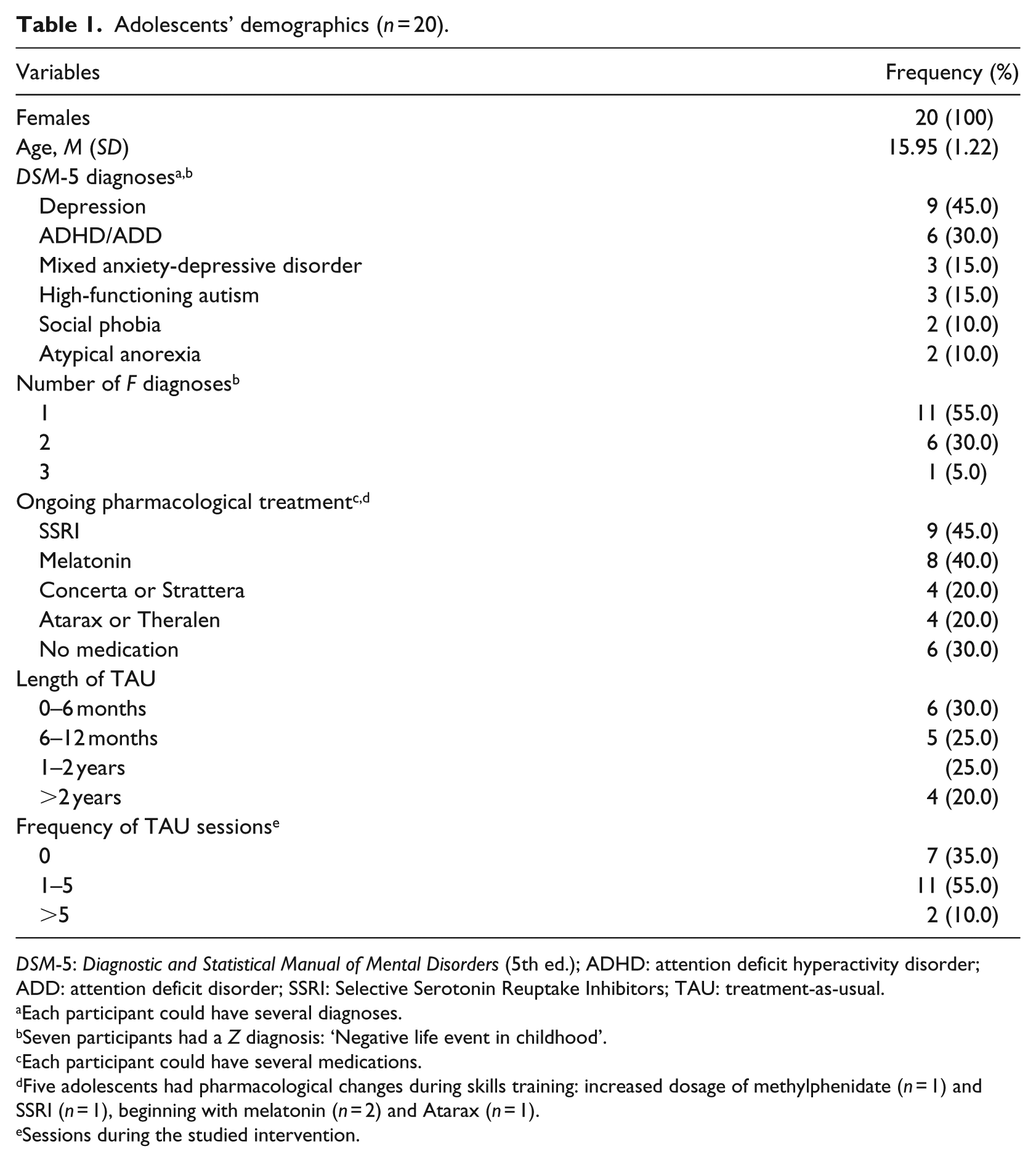
DSM-5: Diagnostic and Statistical Manual of Mental Disorders (5th ed.); ADHD: attention deficit hyperactivity disorder; ADD: attention deficit disorder; SSRI: Selective Serotonin Reuptake Inhibitors; TAU: treatment-as-usual.
Each participant could have several diagnoses.
Seven participants had a Z diagnosis: ‘Negative life event in childhood’.
Each participant could have several medications.
Five adolescents had pharmacological changes during skills training: increased dosage of methylphenidate (n = 1) and SSRI (n = 1), beginning with melatonin (n = 2) and Atarax (n = 1).
Sessions during the studied intervention.
Ethical considerations
The study was approved by the Regional Ethical Review Board of Linköping (Dnr, 2015/264-31). Participants received oral and written information about the study from their therapist, and also from the skills trainers during the introduction of the first session, after which adolescents and adults signed the informed consent form. Participants were informed that they could withdraw from the programme at any given moment without any consequences for their ongoing TAU.
Measures
Primary outcome measures
Difficulties in Emotion Regulation Scale
Difficulties in Emotion Regulation Scale (DERS; Gratz & Gunderson, 2006) measures difficulties in identifying and regulating negative emotions and using goal-directed behaviour while being under the influence of negative emotions. The questionnaire consists of 36 items rated on a 5-point Likert-type scale from ‘almost never’ to ‘almost always’. It has six subscales: difficulties in emotional acceptance (Acceptance), difficulties in goal-directed behaviour (Goals), difficulties in impulse control (Impulse), lack of emotional awareness (Consciousness), lacking emotion regulating strategies (Strategies) and lacking emotional clarity (Clarity). Higher scores indicate more difficulties with emotion regulation. The questionnaire has been used both clinically and in normative populations for adults and adolescents, and has shown to have high internal consistency, good test–retest reliability and adequate construct validity (Gratz & Roemer, 2004; Neumann et al., 2010; Weinberg & Klonsky, 2009). It has also shown good predictive validity (Ritschel, Tone, Schoemann, & Lim, 2015). Cronbach’s alpha for the adolescents’ total score in the present sample was α = .94, indicating excellent internal consistency.
Toronto Alexithymia Scale
Toronto Alexithymia Scale (TAS-20; Taylor & Doody, 1985) measures alexithymia and has 20 items, ranging from totally right to totally wrong on a 5-grade Likert-type scale. The questionnaire comprises three subscales: difficulties identifying emotions (Identifying), difficulties describing emotions (Describing) and difficulties externalising emotions (External focus). Higher score indicates higher levels of alexithymia. TAS-20 is one of the most used self-report scales for alexithymia (Leising, Grande, & Faber, 2009) and has shown good reliability and validity (Henry et al., 2006; Parker, Bagby, Taylor, Endler, & Schmitz, 1993). In the present adolescent sample, internal consistency for total TAS-20 was α = .81.
Levels of Emotional Awareness Scale for Children
Levels of Emotional Awareness Scale for Children (LEAS-C; Bajgar, Ciarrochi, Lane, & Deane, 2005) measures awareness of emotions, that is, the ability to identify and describe own and others’ emotions (Veirman, Brouwers, & Fontaine, 2011). The children’s version used in this study consists of 12 situations, in which the child is asked to describe which emotions he or she and another person would experience in a given situation. Answers are rated by an external rater on a 5-grade scale divided into the three subscales: Self, Other and Total. Cronbach’s alpha for LEAS-C in this study was α = .44 (Self), α = .88 (Other) and α = .51 (Total). In an earlier study by Bajgar and colleagues (2005) of LEAS-C, the internal consistency was α = .71 (self), α = .64 (Other) and α = .66 (Total). LEAS-C was coded and rated by an independent clinician who was blinded to participants’ identity and to their treatment status (before or after). The coder had extensive experience of coding LEAS-C. There was only one coder and no inter-rater reliability was reported.
Secondary outcome measures
The secondary outcome measures were only administered to the adolescents.
Becks Anxiety Inventory
Becks Anxiety Inventory (BAI; Beck, Epstein, Brown, & Steer, 1988) measures symptoms of anxiety with 21 items rated on a 4-grade scale where high scores indicate higher levels of anxiety. BAI is a commonly used instrument with good psychometric properties, and discriminates anxiety disorders from other diagnoses (Beck et al., 1988). Cronbach’s alpha for BAI in this study was α = .94, indicating high internal consistency.
Montgomery Åsberg Depression Rating Scale, Self-Report version
Montgomery Åsberg Depression Rating Scale, Self-Report version (MADRS-S; Montgomery & Asberg, 1979) measures symptoms of depression. Its main purpose is to monitor the development of symptoms during treatment. The scale consists of nine items, which are graded from 0 to 6. Higher scores indicate higher levels of depression symptoms. MADRS-S correlates well (r = .87) with Beck Depression Inventory (Svanborg & Åsberg, 2001). Internal consistency on MADRS-S in this study was α = .90.
Consumer satisfaction and impact on knowledge
A written consumer satisfaction measure created for this study was filled in anonymously after treatment. It contained questions about participants’ overall satisfaction of the skills training: if the skills training had helped the participants to deal with their problems in a better way, if participants would recommend the skills training to others and if the skills training had contributed to improve the family relations. Subjective levels of increased knowledge of emotions and their functions and adequate expression and response to emotions were also measured. Examples of items were as follows: I have learned more about emotions; I have learned to identify different emotions; I have learned more about the functions of emotions. The answers were rated on an ordinal scale from 1 to 5 where high scores indicated positive results. The questionnaire also left space for written comments from participants.
Intervention
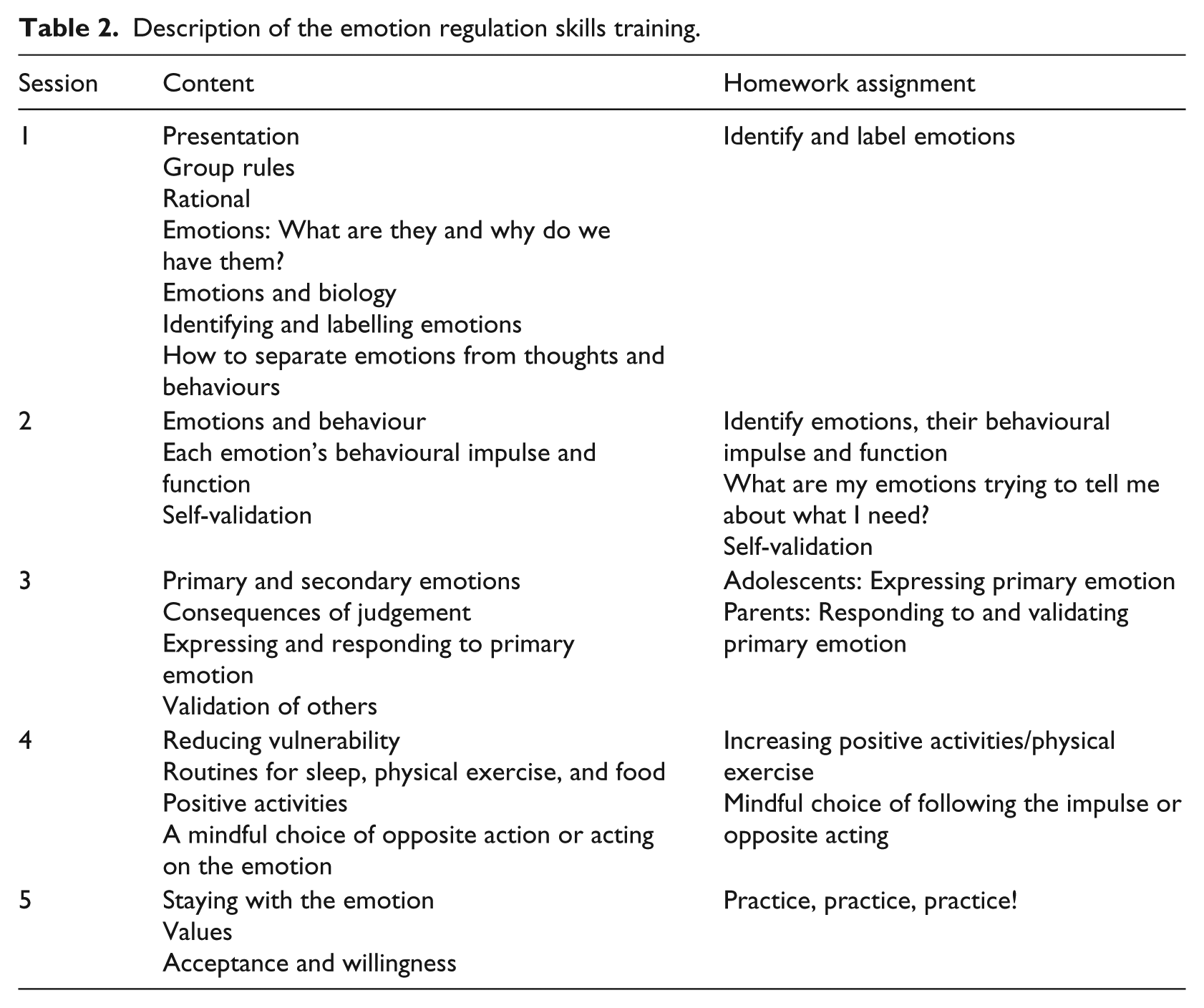
The treatment consisted of five 2-hour weekly sessions of emotion regulation skills training in groups with adolescents and parents together. The main purpose was to provide psychoeducation about the nature and function of emotions and, at the same time, to teach skills that can identify, label, express and regulate emotions. The treatment also consisted of teaching participants skills that can help to reduce judgement and vulnerability and increase positive activities and validation, both of self and others (Table 2). Parents or the adult care taker participated in the group sessions together with the adolescents. Each session included a rehearsal of the previous session’s content and a run-through of the homework assignments. The actual content of the session, introduced by psychoeducation and illustrated with role-play/video vignettes, was followed by a discussion. Each session ended with a summary and a homework assignment. The content was presented using PowerPoint slides and participants also received handouts. The intervention was based on treatment principals and ideas from ERGT, UP, DBT and ACT and developed by the first and last authors who also delivered the actual skills training in this pilot study.
Description of the emotion regulation skills training.
The skills trainers were experienced therapists and had high clinical expertise in child and adolescent psychiatry. They also had previous extensive experience of skills training and group treatments, for example, DBT with adolescents and parents.
Patients who were enrolled in the study also received both psychological and pharmacological TAU while participating in the skills training group.
Statistical analysis
Descriptive statistics were derived using mean values and standard deviations. Paired-samples t test was used to compare differences between before-and-after measures for adolescents and parents separately. In each group, within-group effect size was calculated using Cohen’s d. All statistical analyses were performed using the SPSS 23.0 software package.
Results
Feasibility
A majority of participants who came to the first session followed through the entire treatment (47 out of 54, 87.0%). For adolescents (n = 4), the reasons for dropping out during treatment were severe social phobia or other severe mental health problems that prevented them from completing the skills training or that the adolescents did not want to follow through without a participating parent. For parents (n = 3), reasons for dropping out were that the session dates were inconvenient or that they had insufficient knowledge of the Swedish language. The self-reported reason for declining participation (n = 12) before treatment had started or not showing up at the first session (n = 9) was mainly that dates and times of sessions did not suit the family’s schedule (see Figure 1).
Outcomes
Both adolescents and parents showed significantly reduced scores on the primary outcome measure DERS total scores, t(19) = 2.80, p = .01, Cohen’s d = 0.63, and t(20) = 2.17, p = .04, Cohen’s d = 0.47, respectively, indicating less self-reported difficulty with emotion regulation. Both adolescents and parents also reported a significant reduction in difficulties with goal-directed behaviour, t(19) = 2.35, p = .03, Cohen’s d = 0.52, and t(20) = 2.30, p = .03, Cohen’s d = 0.50. Furthermore, adolescent participants reported significantly fewer difficulties with strategies, t(19) = 3.45, p = .003, Cohen’s d = 0.77, and clarity, t(19) = 3.14, p = .005, Cohen’s d = 0.70, while parents showed a significant decrease in difficulties with impulse after treatment, t(20) = 2.24, p = .04, Cohen’s d = 0.49. The overall effect sizes were medium (Table 3).
Adolescents’ (n = 20) and parents’ (n = 21) self-reported difficulties with emotion regulation and alexithymia before and after treatment, means and standard deviations.
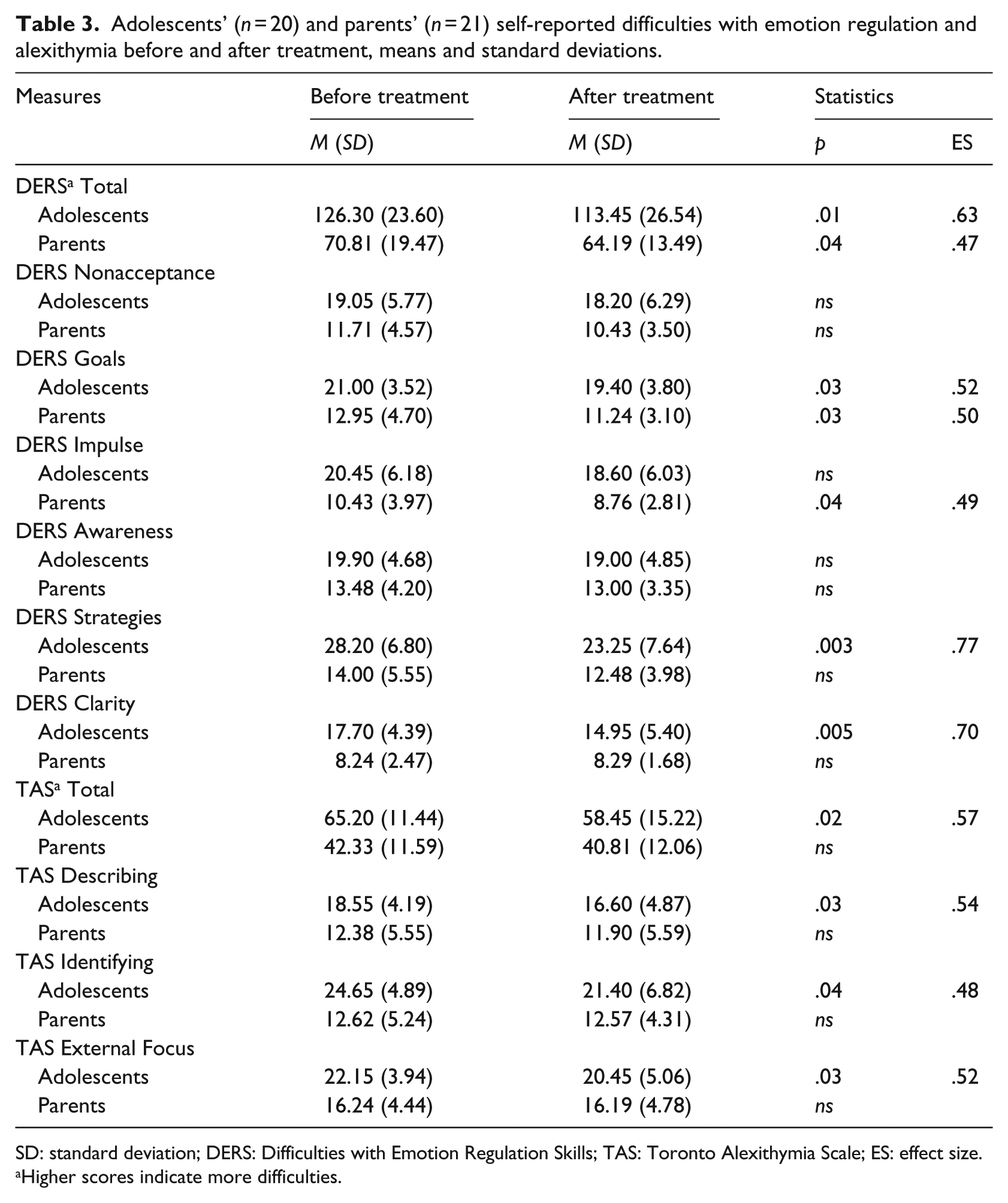
SD: standard deviation; DERS: Difficulties with Emotion Regulation Skills; TAS: Toronto Alexithymia Scale; ES: effect size.
Higher scores indicate more difficulties.
Self-reported levels of alexithymia were also significantly reduced following skills training for adolescents, but not for adults. TAS total scores were t(19) = 2.57, p = .02, Cohen’s d = 0.57, and the subscales Describing, t(19) = 2.44, p = .03, Cohen’s d = 0.54; Identifying, t(19) = 2.16, p = .04, Cohen’s d = 0.48; and External Focus, t(19) = 2.33, p = .03, Cohen’s d = 0.52, were all improved for adolescents and corresponded to a medium effect size (Table 3).
In addition to self-report measures, LEAS-C was used as a measure of adolescents’ levels of emotional awareness before and after treatment. Both total LEAS scores, t(19) = 2.45, p = .02, Cohen’s d = 0.55, and the subscales Self, t(19) = 3.05, p = .007, Cohen’s d = 0.68, and Other, t(19) = 3.55, p = .002, Cohen’s d = 0.79, increased significantly following skills training with medium effect size, indicating an improved awareness of emotions, that is, an ability to identify and describe both one’s own emotions and the emotions of others (Table 4).
Adolescents’ levels of emotional awareness before and after treatment, means and standard deviation (n = 20).
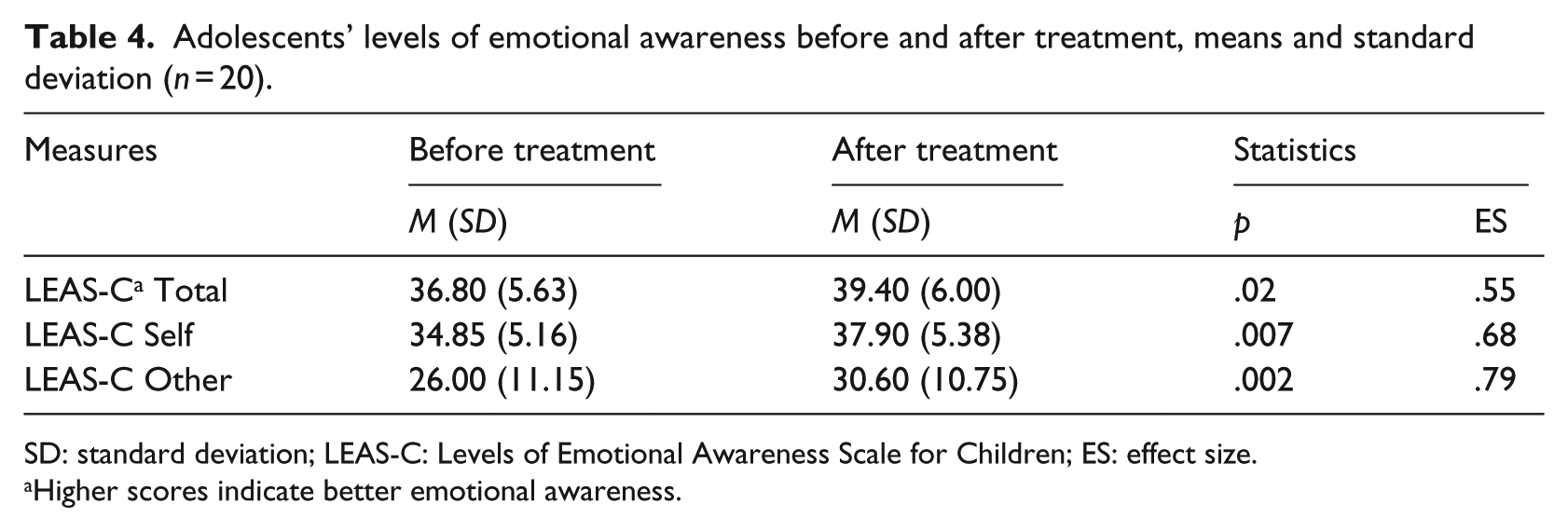
SD: standard deviation; LEAS-C: Levels of Emotional Awareness Scale for Children; ES: effect size.
Higher scores indicate better emotional awareness.
The adolescents in this study showed symptoms of clinical levels of depression and anxiety both before and after treatment, and there was no significant difference following skills training (Table 5).
Adolescents’ symptoms of depression and anxiety, means and standard deviations (n = 20).
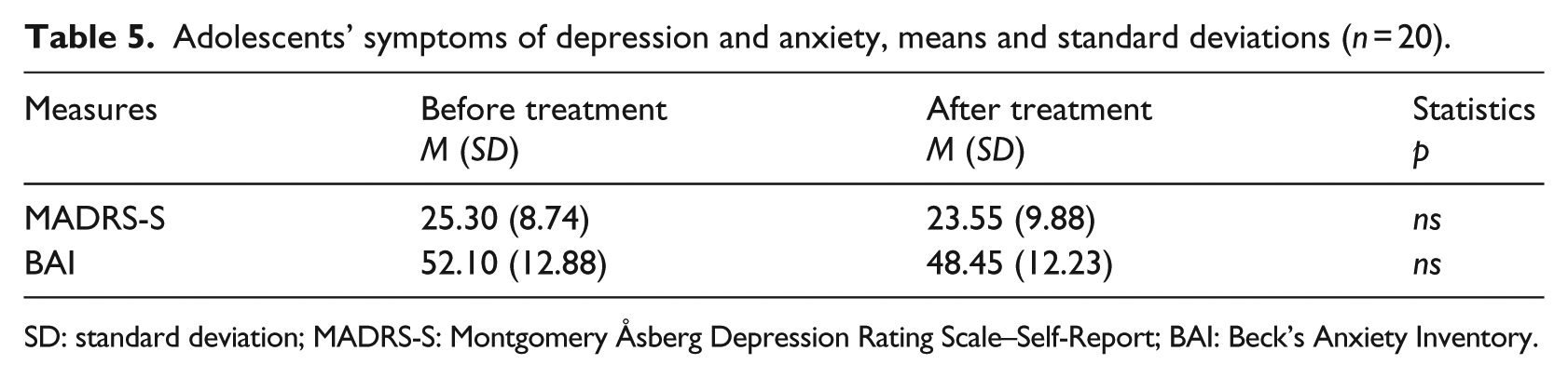
SD: standard deviation; MADRS-S: Montgomery Åsberg Depression Rating Scale–Self-Report; BAI: Beck’s Anxiety Inventory.
Increased knowledge
Participants generally rated the effect of the group skills training very positively with increased self-reported knowledge of emotions and their functions, as well as a perception of being better able to deal with life’s problems after the skills training. Parents generally rated subjective improvement somewhat higher than adolescents (Table 6). Overall, participants’ written evaluative comments were positive and emphasised the advantages of doing the skills training together with a family member. This had given them a mutual language for communicating about emotions and also brought family members closer to each other. Parents reported that they had gained a better understanding of their adolescent’s emotions. Participants were generally positive about homework and the chance to practice between sessions, and also appreciated the multi-model teaching method with films and YouTube clips to illustrate different emotions and emotional reactions and responses.
Participants’ evaluation after skills training, means and standard deviations.

Scale ranging from 1 ‘not at all’ to 5 ‘very much so’.
Discussion
This pilot study examined whether a short transdiagnostic group skills training in emotion regulation for adolescents and parents was feasible in an outpatient child and adolescent psychiatric clinic. Results on the primary outcome measure DERS showed a significant overall improvement after treatment for both adolescents and parents. For adolescents, measures of alexithymia also improved significantly, as did levels of emotional awareness.
Outcome measures
Adolescents pre-treatment scores (M = 126.30, SD = 23.60) on DERS at baseline were high, indicating that the participants had extensive difficulties with emotion regulation. A cutoff score of 96 has been proposed (Neacsiu et al., 2014). Weinberg & Klonsky (2009) found an average DERS score of 80.2 in their study of non-clinical adolescents. The DERS results in this pilot study were comparable to adult women with self-harm with BPD traits (Bjureberg et al., 2015; Gratz & Gundersen, 2006). Benchmarking comparisons between the pilot study and other skills training are difficult since other treatments usually continue for 14–16 weeks and are more extensive (e.g. Gratz & Gunderson, 2006; Neacsiu et al., 2014; Trosper et al., 2009). The DERS results in Gratz and Gunderson’s (2006) study of ERGT with adults had a pre-mean score of 127.92 and post-mean score of 79.75, compared to pre and post scores of 126.30 and 113.45 in this study. The DERS subscale Clarity was significantly improved for both adolescents and parents, which could be due to the fact that skills in identifying and labelling primary emotion and separating thoughts and emotions were practised throughout the treatment. Interestingly, not only adolescents’ but also parents’ total DERS scores were significantly reduced. Parents also improved their scores on DERS subscale Impulse. During skills training, the skill of reducing impulsive behaviours, taking a step back and then choosing a behavioural response was discussed frequently, which potentially resulted in this change for parents. In the oral feedback at the end of treatment, many parents emphasised that this was an important skill for them.
Self-reported alexithymia, measured by TAS-20, was significantly reduced for adolescents in the study. The participating adolescents had high scores on alexithymia before treatment (M = 65.20, SD = 11.44). Honkalampi et al. (2009) found an average score of 46.8 (9.9) on TAS-20 in an adolescent female non-clinical sample. Adolescents had lower results to start off with compared to adults, and thus had larger room for improvement. A short-term individual intervention which focused on emotion regulation for young adults diagnosed with anorexia nervosa (Adamson, Leppanen, Murin, & Tchanturia, 2018) had pre and post means of 56.64 and 53.30 on TAS-20. The improvement in our pilot study could potentially be an effect of repetition in practicing how to identify, label and describe emotions during skills training.
Interestingly, the skills training also resulted in improved scores on LEAS-C, which is not a self-report measure, but instead rated by the third author. LEAS-C has not, to our knowledge, previously been used to assess progress and improvement following treatment and is potentially a useful complement to self-report. Due to the limited use of LEAS-C as an outcome measure and limited psychometric properties, these results should be interpreted with caution. The results from this explorative pilot study of a brief intervention are potentially promising. Labelling emotions in exposure treatments has shown a positive effect on emotion regulation (Kircanski, Lieberman, & Craske, 2012). Labelling and describing emotions, that is, putting feelings into words, activates prefrontal regions of the brain and reduces responses in the amygdala, thereby helping to process and regulate intense emotions (Lieberman et al., 2007). There is also support for how the social environment can affect a child’s ability to regulate emotions (Thompson, 2014), which further strengthens the importance of parental participation in this context.
No significant changes were found when measuring symptoms of depression and anxiety before and after the skills training. The adolescents reported clinically high levels both before and after treatment. Symptoms of depression and anxiety were not directly targeted in the treatment. However, earlier studies have shown that an increased ability to regulate emotions affects symptoms of anxiety and depression (Barlow et al., 2011; Payne et al., 2014). There are several possible factors that could potentially explain the lack of effect on these symptoms in this pilot study, the first being that the after measures were administered at the last session, and that the effects on symptoms of depression and anxiety could potentially need a longer follow-up, after participants had had more time to practice skills. Another reason could be that the current skills training, with only five sessions, was too short an intervention to have an effect.
One of the main aims of this study was to examine the feasibility of this programme with clinical groups of families with multiple diagnoses in a natural clinical setting. The brief treatment made it relatively easy to motivate families to participate. One of the strengths of the skills training is that it is transdiagnostic, reaching many potential participants and targeting clinical families in a clinical setting. There was high participation throughout the skills training with relatively low dropout. There were high ratings generally on the participants’ consumer satisfaction.
Limitations
This was a preliminary open pilot study of the feasibility and effects of a brief transdiagnostic emotion regulation skills training, with potential promising effects. Due to the small sample and the pilot setting, there are several limitations that need to be addressed. The lack of control and randomisation undoubtedly make the study weaker. Spontaneous improvement or other treatment effects potentially attributed to TAU, which continued during the treatment, are some examples of alternative explanations of the findings. None of the ongoing TAU, however, directly targets emotion regulation skills. A longer follow-up period was also lacking. LEAS-C is not, to our knowledge, traditionally used as an outcome measure. The internal consistency of the items in this study, and in Bajgar and colleagues (2005), is questionable, and the results should be interpreted carefully. The last session covered themes such as values and acceptance, which are complex issues that need time to sink in and to practice. Results on the DERS subscale Acceptance could potentially be influenced by this. Participants were all girls, making generalisation difficult. Data on parents’ demographics were not collected and we do not know if differences in demographics potentially influenced the results. There was no random sampling of participants for inclusion. Instead, therapists chose suitable participants, potentially resulting in a selection bias. The study aimed at piloting a skills training with a heterogeneous group of patients in the complex context of clinical child psychiatry, without interfering with their other ongoing interventions. Changes in ongoing medication or therapy, together with other major life events, could certainly influence results. Two of the 20 participating adolescents had increased dosage of methylphenidate (n = 1) and Selective Serotonin Reuptake Inhibitors (SSRI) (n = 1) during the skills training, which could potentially influence difficulties with emotions regulation. There were some multiple statistical comparisons, and therefore, risk of type I error has to be taken into account when interpreting the results. Furthermore, the emotion regulation skills training also has to be delivered and investigated by others and then the creators.
Future studies
Future studies need to include more participants, as well as a randomised controlled trial (RCT) design with follow-up. Since five sessions were feasible without too high levels of dropout, the skills training could potentially include one or two additional sessions, to allow more time to consolidate and practice the content. This, however, must be balanced against difficulties in getting families to sign up for more extensive treatments.
Conclusion
Results from this pilot study showed that brief psychoeducation and skills training about emotions and emotion regulation administered to adolescents and parents jointly were feasible and appreciated by participants. The primary outcome measures showed promising preliminary results with decreased difficulties with emotional regulation, less alexithymia in adolescents and increased awareness of emotions. Parents also reported significantly fewer difficulties with emotion regulation following treatment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author biographies
![]()