
Abstract
In 2018, approximately 20,000 unaccompanied children and young people applied for asylum in a European Union country. Unaccompanied asylum-seeking children present with significant emotional and physical health needs. These needs are likely the result of the situation that led them to leave their home, the difficult journeys they make to reach safety and their living circumstances after arriving at their destination. Maintaining engagement with both screening and therapeutic health services is challenging. A stepwise approach to delivery of services is recommended so as not to overwhelm them. Case studies and personal practical experience are used to highlight key learning points.
Keywords
Unaccompanied minors – definitions
In recent years, the World has seen a significant increase in the number of children migrating alone. The United Nations High Commissioner for Refugees (UNHCR) defines an unaccompanied child as any person under the age of 18 who is ‘separated from both parents and is not being cared for by an adult who by law or custom has responsibility to do so’ (Office of the UNHCR, 1997). An unaccompanied asylum-seeking child (UASC) is an unaccompanied child who is seeking legal refugee status having ‘been forced to flee his or her country because of persecution, war or violence’ (UNHCR Agency, 2020).
In 2015–2016, at least 300,000 unaccompanied and separated children moved across international borders – a fivefold increase from 2010–2011 (United Nations Children’s Fund [UNICEF], 2017). In 2018 19,700 unaccompanied minors applied for asylum in Europe (Eurostat, 2019). Lone children seeking asylum in the United Kingdom are typically aged between 14 and 17 years (UK Refugee Council, 2019).
For the purposes of consistency in this article, we have used the term UASC to describe all children/young people with whom we have worked who are displaced from their home country and seeking safety and refuge in a foreign country. Their individual legal statuses varied at the time of our work with them.
Health and lone migration as a child
Multiple factors combine to place UASC at high risk of physical and mental health difficulties. Most UASC originate from the world’s poorest countries where health care provision may be extremely limited. Trauma (both physical and mental) is a common ‘push’ factor for lone migration and UASC often undertake prolonged and physically gruelling journeys when seeking asylum (Thomas et al., 2004).
In a survey of displaced refugees living in northern France, many of whom were children, 52% of respondents reported a health need. Of those, 21.2% reported a mental rather than physical health problem. Many respondents blamed lack of sleep and their hopeless situation as the main factors in making them feel mentally unwell. (Refugee Rights Europe, 2018).
For those arriving in the UK, 75% had specific health issues including active and latent tuberculosis (TB), hepatitis B and schistosomiasis. Other skin conditions, sleep issues and non-specific pain were also reported. More than half of these children reported mental health symptoms and over a third were referred to specialist mental health services. A quarter were referred to sexual abuse services (Battersby et al., 2019; Williams et al., 2019).
Our working environments
A.W. and S.P. work in contrasting environments. S.P. is a Consultant Clinical Psychologist who volunteers for the Refugee Resilience Collective, a UK-based charitable collective of systemic and narrative therapists who have a presence in Calais once a week (Burck & Hughes, 2018). Between April 2016 and 2017, SP met with UASC in Northern France while they were residing in an unofficial temporary refugee camp known as ‘The Jungle’ or in an ‘official camp’ in Dunkirk. All these young people were still on the move. A.W. is a Consultant Community Paediatrician employed by an inner-London NHS Foundation Trust. She has worked for 5 years in a weekly outpatient clinic providing statutory initial health assessments to UASC who have recently been placed in the care of the local authority.
We came together to share our experiences of working with unaccompanied children at differing stages of their asylum journey. This article aims to use the stories of two UASC to highlight the complex overlap of their physical and psychological health needs and make the case for developing more integrated mind–body approaches to addressing their needs.
Case study 1
Abreham 1
Abreham, a 14-year-old boy, lived at home with his mother and younger sister in Keren, Eritrea, an East African country. His father and older brother had been conscripted into the military service (UK Home Office, 2015). His father left 5 years ago and nothing had been heard from him for 2 years. Abreham presumed he was dead. His older brother had been away for more than 18 months (the official length of military service). Abreham told his mother he wanted to leave Eritrea before he was old enough to be conscripted. Friends had told him that ‘you have a 50% chance of surviving military service and returning home and a 50% chance of surviving the journey to Europe’. He wanted to try to get to England where his aunt lived. His mother was worried that she may never see him again but she agreed to support him. She gave him money and explained that she could transfer money to him during his journey.
The first part of his journey was to Sudan to visit his older sister who lived in Khartoum. Here he collected contact details of reputable smugglers who could facilitate his journey across the Sahara and arrange a boat across the Mediterranean Sea. He learnt where to hide his money and which clothes, food and medicine to carry. He left Khartoum in a minibus with 25 other refugees. In the Sahara desert, the minibus was stopped by men, claiming to be military. They beat Abreham and robbed him of his few possessions. They stole the vehicle. Abreham and his fellow travellers were left with no transport, very little food and water for several days. One day a car stopped and offered to take Abreham and two other young adolescent Eritrean males to Libya.
In Libya, Abreham and his two companions were handed over to people traffickers. They were forced to work for the traffickers until they had earned their ‘fee’ for transport across the Mediterranean Sea, which took 9 months. The living conditions were appalling and he described eating rancid meat. He was regularly beaten across the head and torso by the traffickers.
After a precarious journey across the Mediterranean Sea in an overcrowded boat, Abreham was rescued by a humanitarian organisation on the coast of Italy. Abreham remembers the kindness of his rescuers. Abreham was physically unwell and treated for dehydration in hospital. Once recovered, he travelled by various modes of transport to Ventimiglia in Italy, where he stayed for a month in a church.
Abreham eventually managed to hide on a train and cross into France where he made his way to Calais. From here he knew he would have the best chance of getting to the United Kingdom and his aunt.
Abreham spent from November to February 2017 in the camp in Calais known as the ‘Jungle’ sleeping in makeshift temporary accommodation with other refugees from Eritrea. He met a lawyer there who explained that he was eligible to come to the United Kingdom under the Dublin III Regulation (UK Home Office, 2020). Dublin III is a European Union regulation that allows young people who are in other European Union (EU) countries to be brought to the United Kingdom to be reunited with family members who are already resident in the United Kingdom. One cold evening Abreham was given wood by volunteers to make a fire and his temporary accommodation caught fire. Abreham suffered significant burns while trying to save his few possessions. He received treatment in hospital but was nervous that he would be transferred to a French reception centre so he discharged himself. He tried unsuccessfully to reconnect with the lawyer. After 4 months in ‘the Jungle’, he was frustrated by the delays in arranging his legal journey to the United Kingdom.
On many nights, Abreham tried to get into the back of lorries bound for the United Kingdom. One night he was successful. By the time he arrived in the United Kingdom and presented himself to the British Transport Police. Abreham was 16 years old. His asylum journey had taken 2 years and he had travelled 8,000 km alone. He was placed in the care of local government authority while they tried to find his aunt.
Abreham’s social worker arranged for him to undergo a statutory comprehensive health assessment by a specifically trained doctor (UK Department for Education., & UK Department of Health, 2019). A face-to-face Tigrinya interpreter was present for the assessment. The following physical health issues were identified and treated:
Itchy skin secondary to scabies (a parasitic skin infection) requiring treatment with an insecticide.
Multiple healed skin scars consistent with his history of being beaten with implements in Libya and burnt in France. Abreham described aches and pains in these body areas, especially at night, that did not settle with painkillers.
Upper abdominal discomfort secondary to a bacterial stomach infection with Helicobacter pylori. H pylori infection is common among newly arrived refugees (Abdul Rahim et al., 2017).
Latent TB (a potentially serious bacterial infection), schistosomiasis (a parasitic infection in the urinary tract) and a gut tapeworm.
A hearing test revealed a moderate to severe hearing impairment in his right ear. The causes of deafness in refugee populations are multiple (Reilly, 2010) but in Abreham’s case could be attributed to the repeated significant head trauma in Libya.
A heart murmur secondary to rheumatic heart disease, as a consequence of a streptococcal infection in earlier childhood
Abreham was asked about his emotional health at his first health assessment in the United Kingdom. He replied that he was simply happy and relieved to have arrived in the United Kingdom safely.
After 2 months, Abreham was reunited with his aunt. Four months later, Abreham’s aunt took him to the general practitioner (GP) to report that he was still suffering sleep difficulties as well as frequent headaches and body pains which did not respond to painkillers. He felt permanently tired and presented as very irritable and uninterested in even playing football that he loved. He worried frequently about his family in Eritrea. The GP was unable to identify a medical cause for his physical symptoms and referred him to a local CAMHS (Child and Adolescent Mental Health Service).
Abreham’s presentation and account of his experiences are typical.
Case study 2
Linh 1
Linh grew up in Vietnam with a maternal aunt. Both her parents, whom she described as political activists, died in her early childhood. At 13 years, Linh became interested in Buddhism and started attending meetings with other young teenagers. In Vietnam, practicing religious beliefs is not allowed and one evening Linh was arrested during a meeting (UK Home Office, 2018). Linh spent 4 weeks in prison, where she described being tortured daily. Her hands were beaten with a metal stick and she was forced to kneel for long periods of time.
Upon release from prison Linh’s aunt arranged for a family acquaintance to take her to the United Kingdom. Linh, now 14 years of age, took two flights and several lorry journeys with other Vietnamese refugees. Upon arrival in the United Kingdom, Linh travelled to the North of England where she lived for 4 weeks in a house with other Vietnamese people. She was then put on a coach to London, where she lived in another Vietnamese household for 2 weeks. Linh met a Vietnamese woman in a café who encouraged her to present herself to Social Services to get help with food, clothing and accommodation. Linh went to a local council office to ask for help. Aged 14, Linh became looked after by the local authority and was placed with a local foster carer.
Linh’s social worker arranged for her to have a comprehensive health assessment with a specialist paediatrician. Being female, Linh is part of a significant minority in the UK UASC population as almost 90% of unaccompanied minors applying for asylum in the United Kingdom are male (UK Refugee Council, 2019). At her health assessment, Linh was notably quiet and withdrawn. The assessing paediatrician found it very difficult to gather a detailed history of her journey despite the presence of a face-to-face Vietnamese interpreter.
Linh was identified as having the following physical health needs:
Pain and difficulties passing stool – clinical examination revealed damage to the skin around the anus and chronic constipation.
Chronic Hepatitis B infection. The remainder of her infection screening tests were negative.
Linh could not provide a menstrual history. A urine pregnancy test was positive. Linh consistently denied that she had ever been in a sexual relationship.
Linh described finding it hard to fall asleep at night preferring to sleep during the day.
Following her initial assessment, Linh struggled to settle in her foster placement. Over the next 2 months, she missed several hospital appointments related to her pregnancy. She was often reported missing from her foster carer’s home. When she returned she was quiet and withdrawn. The local network became increasingly concerned that Linh was the victim of human trafficking.
Now 4-month pregnant Linh was moved to a foster placement over 100 miles outside London. Linh started attending a new school. She cautiously formed a good relationship with her foster carer and after 4 months, with the delivery of her baby imminent, Linh disclosed a history of sexual abuse by numerous adult males upon arrival in the United Kingdom. Linh was referred by her social worker to a local multi-disciplinary service for children and young people who have experienced sexual abuse. When Linh was almost 15 years of age, she delivered a healthy baby girl who, with Linh’s consent, was placed in foster care.
Trafficking, modern slavery and the UASC population
Few children can be considered more vulnerable than those who have been forcibly trafficked across or within international borders for work in the sex, drug or domestic service industries. In 2018, almost 7000 individuals were referred to the UK National Referral Mechanism as possible victims of human trafficking or modern slavery (UK National Crime Agency, 2019). About 45% of these were minors and of these 45% were reported to be Vietnamese.
Some trafficked children continue to be exploited even after they have entered local authority care. The possibility of human trafficking must be considered for all unaccompanied minors. Victim disclosure of trafficking is rare at health consultations, as trafficking victims are prevented from disclosing their status to health care providers by fear, shame, language barriers and limited interaction with medical personnel (Baldwin et al., 2011).
The relationship Linh forged with her foster carer eventually allowed her to disclose her history of human trafficking. The physical health needs identified at Linh’s initial health assessment were consistent with the sexual abuse she experienced.
Linh’s presentation and account of her experiences are typical.
Responding to the health needs of UASC
UASC on the move
UASC who have not arrived at their destination of choice are unlikely to stay in one place for long. They may present to health services only for emergency care as they are concerned that once medical staff have a formal record of them that they will only be able to claim asylum in that country. It is important for health professionals to address their immediate concerns promptly and appreciate that UASC may feel extremely vulnerable at this initial consultation.
UASC on arrival at their destination
UASC present with multiple areas of health need at their initial health assessments in the United Kingdom. Health assessments take time and should be completed by practitioners with experience working at the interface of physical and emotional health. Practitioners must be aware that a UASC may not be in the position to immediately co-operate with treatment.
Contextualising with Maslow’s hierarchy of needs
When A.W. first began working with UASC in the United Kingdom, the uptake of offered health services was poor. After the initial comprehensive health assessment, there were very high levels of non-attendance at appointments for both physical and mental health services. UASC reported being ‘overwhelmed’ by the number and frequency of health, education and immigration appointments.
Maslow’s Hierarchy is a five-tier model of human needs (Figure 1). Maslow suggested that needs lower down the model need to be satisfied before individuals can attend to higher needs (Maslow, 1943). It is a useful way of understanding how UASC respond to their health needs.
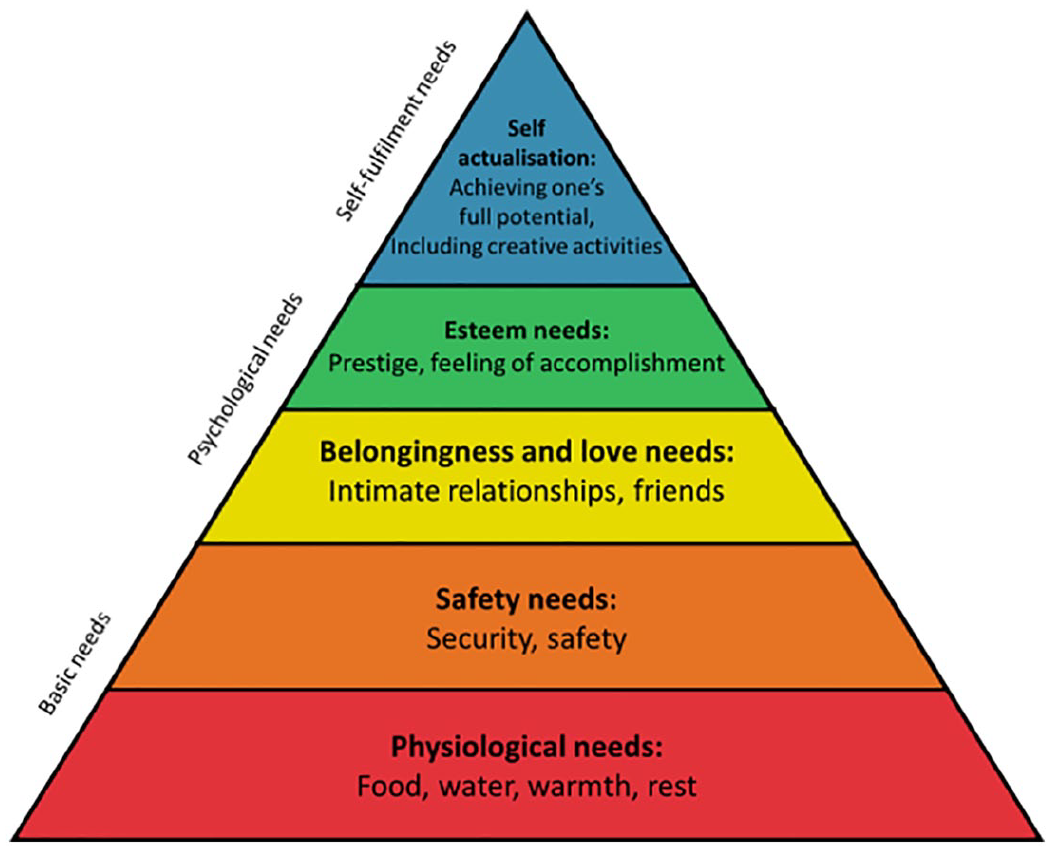
Maslow’s Pyramid after Maslow’s Hierarchy of Need (Maslow & Lewis, 1987).
Level one of need: physiological survival
For UASC that have recently arrived in the UK priorities will include securing somewhere safe to sleep, physical protection from the elements and access to food and water. In our experience, this phase lasts days to weeks. Unaccompanied minors by law should be seen for their comprehensive health assessment within 20 working days (UK Department for Education & UK Department of Health, 2019). It is sensible to assume that UASC attending their first health assessment may be preoccupied with their basic physiological needs and not able to consider higher levels of need.
Level two of need: safety and physical discomfort
At this level, UASC may begin to describe physical health symptoms such as abdominal or dental pain, body or headaches and sleep disturbance. UASC should be asked direct questions about their physical symptoms rather than being relied upon to volunteer this information. Relevant medical investigations should be completed, but if no physical cause can be identified then health practitioners should not forget that these symptoms may be indicative of emotional distress that a UASC is not yet able to articulate.
Levels three, four and five of need: emotions, esteem and actualisation
It is perhaps only once UASC feel consistently safe and physically comfortable that they may begin to consider and communicate their higher levels of need. This may include discussions about their anxiety for the safety of relatives who remain in their home country, their feelings of social isolation in a foreign country and their guilt at having ‘escaped’ persecution when those they love have not. These higher levels may also be experienced when they access education enabling them to have a rewarding career as an adult. The rate at which a young person may reach this level of expression is hugely variable. Many UASC who initially present, as did Abreham, with a reluctance or inability to discuss their emotional health often return to professionals after several months requesting assistance for emotional difficulties.
Non-linear passage through Maslow’s hierarchy of need
Maslow’s theory could be seen as an overly simplistic tool because it ignores the numerous external factors that may also impact on a UASC’s readiness to access health services, such as the stability of their care environment, their legal status and their situation at school. It must also be emphasised that UASC can present with clear symptoms of emotional distress even when they remain on tier 1 in the hierarchy. However, an understanding of the theory has proved useful – particularly for professionals working with UASC without a clear background of psychological training. It can also be useful in helping professionals understand how the needs of UASC change over time and how interventions need to be adjusted accordingly.
Even when settled in their new country UASC may move back and forth between the different levels of need on Maslow’s Hierarchy. Placement changes and official decisions on immigration status in particular seem to place UASC at risk of a backward step and they may show symptoms such as irritability, self-harm and sleep disturbances (The Children’s Society 2018; Hodes et al., 2008). UASC who cannot be returned to their country of origin are often granted a specific form of leave to remain in the United Kingdom called ‘UASC leave’. This is temporary and each UASC must apply for confirmed asylum-seeker status as they approach their 18th birthday. This may coincide with changes in educational placement as well as care placement. About 85% referrals to the Child and Family Refugee Service for unaccompanied young people are for those approaching this crisis point (Hughes & Rees, 2016). This is a particularly stressful moment with some young people even becoming suicidal (The Guardian, 2019). In 2018, the refusal rate for asylum was 60% (UK Refugee Council, 2019).
Experiences of providing psychological support for UASC
UASC show more traumatic stress reactions than young people who arrive with their family (The Children’s Society, 2018). This is not surprising because they are likely to have experienced trauma from the reasons that prompted fleeing their home of origin, their migration journey itself and the immigration process once they have arrived. The most common symptoms are disordered sleep, lethargy, lack of motivation, being withdrawn, headaches, stomach aches or other body pains. They also exhibit intrusive thoughts, irritability or anger and disruptive behaviour (The Children’s Society, 2018).
When working with people who have experienced trauma, it is important to spend time on the initial stages of contact. UASC are marginalised, no country makes them feel wanted, and it is difficult for them to get their voices heard. They can feel like they do not matter so it is important to make sure they know that they do (Madsen, 2019). It is essential, where possible, to use face-to-face interpreters. It is easy to make assumptions and believe that you have understood. It is important to check your understanding as well as checking that you are talking about what is important to them. Being aware that most of these young people have spent so much time feeling unsafe with people in authority, it is important to create ‘islands of safety’ for them (Lee, 2013). Get to know them first before talking about why they have come to this meeting. Asking questions about their interests, their skills and abilities and who is important to them makes people realise that they do matter and that they are more than the sum of their problems (Madsen, 2019).
Enabling the young person to feel they have control over the meeting will help place them on an “island of safety’. One way of giving them that control is by offering a red card and explaining that if you ask any questions they would prefer not to answer, they can hold up the red card and you will move on (Vermeire, 2017).
Being transparent and clear with young people about how you can help and what is beyond your remit is important to gain trust. It is also a form of intelligent kindness (Campling, 2015) which builds therapeutic relationships.
There is a western notion of Catharsis that it is important for a person who has experienced trauma to tell their story. There is an alternative idea that it can be re-traumatising to just tell and re-tell this difficult story (White, 2004). Reliving trauma reactivates the brain’s alarm systems and makes it more likely that an individual will relive the past rather than resolve it (Van der Kolk, 2014). If a young person does start to talk about their ‘difficult’ story it is useful to try and slow down the telling. The experience of trauma can leave an individual feeling like they have very little control over their lives. They can be robbed of their ‘personal agency’ so asking questions about what happened as well as how they responded to these challenges is essential (White, 2004). These stories are often not talked about. It may be that an individual stayed quiet in the hope that their attacker would be gentler with them or screamed out in the hope that someone would come to their rescue. They may have held on to certain thoughts while being attacked to protect themselves. By encouraging a young person to tell these stories of response as well as the stories of the trauma, it can give them back a sense of personal agency.
About 92% of UASC in the care of local authorities in England in 2017 were male (Association of Directors of Children’s Services [ADCS], 2016). UASC are likely to come from communities where mental health means psychosis and where shame may be attached to mental health problems. There may be added stigma around men asking for support so significant under-reporting of symptoms is likely. It is important, therefore, to remove stigma as far as possible by talking about some of the symptoms that other young unaccompanied young people have reported and ask if they are experiencing anything similar. The session notes contain the young person’s stories. Offering the young person a copy of the notes can increase trust.
Including the young person in the co-management of their physical and emotional health needs can offer them a different experience to the immigration process. Joint assessments and open lines of inter-professional communication can help reduce the number of appointments and help these marginalised young people feel like they matter.
Learning from our experiences to improve health services for UASC
Our work with UASC, both overseas and in the UK, has helped us to acknowledge the challenges in providing health services to UASC. It has also allowed us to identify key areas of good practice.
Routinely offer a comprehensive and holistic health assessment to UASC with trained health professionals
This represents not only an ideal opportunity to identify any immediate risks to health as a result of physical or emotional health disorder, but also to initiate systems to detect and manage additional health needs that may present themselves as a UASC continues along their asylum journey. Practitioners must be mindful that many illnesses appear to be asymptomatic in UASC (Battersby et al., 2019; Williams et al., 2019)
Work together whenever you can
The paediatric team performing initial health care assessments (IHAs) for UASC soon noted that they were identifying significant mental health difficulties alongside their complex profile of physical health needs. This generated a high volume of urgent CAMHS referrals but subsequent uptake of offered appointments with CAMHS was poor. In response to this, it was agreed that a clinical psychologist from the local CAMHS refugee service would be present at the majority of IHAs for UASC. This recommendation forms part of a locally agreed multi-professional guideline (Social workers are not routinely present at IHAs in this borough).
The clinical psychologist joins the medical assessment and can quietly observe the UASC while a comprehensive medical, social and developmental history is taken.
Next the clinical psychologist conducts a screening interview with the UASC. This interview screens for symptoms of mood disorders such as post-traumatic stress disorder, anxiety and depression as well as current risk of self-harm and suicide. The psychologist will also be alert to indicators of psychotic experiences and substance dependence. Both the young person and their carer (if in attendance) complete the ‘Strengths and Difficulties questionnaire’ (Goodman, 2001).
Following a brief professional discussion, the paediatrician and clinical psychologist feedback to the UASC a summary of their jointly identified physical and emotional health needs. This provides an important opportunity for discussion and exploration of the often-overlapping mind–body nature of some common health issues – such as experiences of pain and sleep disturbance. Many UASC originate from cultures where there is no Cartesian split in the concepts of illness; therefore, we as professionals mirror this by assessing health holistically.
A care plan for addressing these overlapping health needs is formulated collaboratively, taking into consideration each UASC’s individual needs and readiness to engage in the various offered physical and emotional health services. Psychological coping strategies are explored in brief. Where indicated and with consent from a UASC a referral is made for a more in-depth multi-disciplinary CAMHS assessment.
The joint assessment usually takes approximately 2 hours and a detailed joint report is shared with the young person and their social worker highlighting the priority with which each health task should be addressed.
The benefits of the joint assessment are multiple – and include rapid access to a clinical psychologist for mental health screening and initiation of appropriate support, provision of health recommendations that respond to the overlapping mind–body needs of UASC and reduction in unnecessary duplication of appointments.
Education, support and health care promotion for all staff working with UASC
Not all health needs will be evident at the IHA. All staff working with UASC including social workers, care workers, those in the education and voluntary sectors, should receive education regarding the varying presenting physical and emotional health needs of UASC. As new concerns around physical and emotional health arise, advice should be sought from appropriate health professionals and safety measures put in place.
The gold standard aim – involve UASC themselves in delivering and improving UASC health services
It must be acknowledged that in our work so far we have not yet managed to robustly collect feedback from UASC themselves about what is important to them regarding their physical and emotional health. This is our next goal. It will provide UASC the opportunity to ‘give back’ and perhaps an opportunity to meet the highest level of need on Maslow’s hierarchy.
Conclusion
Children and young people fleeing persecution and seeking refuge in a foreign country present to professionals – both during their journey and upon arrival at their ultimate destination – with a wide-range of health needs. Physical and psychological health needs – as well as external factors such as their legal status and the stability of their care environment – overlap and cannot be considered in isolation.
A comprehensive health assessment should be offered to all UASC with consideration of both symptomatic and asymptomatic patterns of illness common in this group. The possibility that a UASC is the victim of historical or ongoing human trafficking should be considered. Joint working between physical and mental health practitioners can promote better understanding of mixed mind–body health needs.
Professionals working with UASC should appreciate the potentially non-linear presentation of health needs in UASC – and in particular be alert to emerging psychological difficulties as a UASC approaches 18 years of age.
In the future, service development work should involve UASC directly.
Footnotes
Acknowledgements
The authors thank Zoe Given-Wilson (Lead Clinical Psychologist, LAC/Refugee CAMHS, Tavistock and Portman NHS Foundation Trust) for her insight into the clinical psychologist role at joint health assessments for UASC.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.