
Abstract
Gender minority stress refers to social stressors such as discrimination and stigma that gender minorities are subject to. This study examines the relationship between gender minority stress and psychological well-being in trans and gender diverse young people (TGDYP). We used a cross-sectional design to investigate the relationship between gender minority stress and mental well-being in TGDYP aged 16–25. We measured anxiety, depression, general psychological well-being, gender dysphoria, gender minority stress (distal and proximal), resilience and heteronormative beliefs in cisgender (n = 135) and trans and gender diverse (TGD) (n = 106) participants. Hierarchical regression was used to analyse the data. TGD participants had significantly higher levels of anxiety and depression, and poorer general well-being, than cisgender participants. Although the direction of the relationship cannot be determined through our analysis, TGD participants who experienced more minority stress and were assigned female at birth had higher levels of depression and anxiety. TGD participants with higher resilience scores and were assigned male at birth had better well-being overall. Our findings suggest that we should pay attention to minority stress when thinking about how to reduce anxiety and depression in TGDYP. The responsibility for improving well-being lies not just with services but instead should be held by our whole society.
Keywords
Introduction
The term transgender refers to a range of gender identities which are underpinned by a conflict between someone’s sex assigned at birth (SAAB) and felt gender. It includes both binary gender identities (someone may identify as female when they were assigned male at birth, or vice versa) and ‘non-binary’ gender identities, which are often also referred to by other labels such as agender, pangender or gender fluid (Richards et al., 2016). In this study, the term ‘trans and gender diverse’ (TGD) will be used to refer to the spectrum of transgender identities (Johnston, 2016), while individuals who identify fully with their sex assigned at birth are referred to as ‘cisgender’ (Enke, 2013). Some transgender people experience gender dysphoria (GD), which is a diagnosis in the Diagnostic and Statistical Manual of Mental Disorders-Fifth Edition (DSM-V, APA, 2013), referring to psychological distress due to the mismatch between SAAB and felt gender.
A higher proportion of individuals within TGD communities experience psychological distress than in the general population, with some US-based studies reporting rates of anxiety and depression that are two to six times higher in TGD individuals (Bockting et al., 2013; Harvard Medical School, 2007). Trans and gender diverse adults are also significantly more likely to report depressive symptoms and suicide attempts than their LGB counterparts (Su et al., 2016). In addition, English population studies report that people assigned female at birth (AFAB) have higher rates of anxiety and depression than those assigned male at birth (AMAB; McManus et al., 2016).
Adolescence is a crucial time for many sexual and gender minorities in terms of ‘coming out’ and is also a time when many mental health (MH) difficulties emerge (Kessler et al., 2007; Office for National Statistics, 2017). Furthermore, when puberty starts creating bodily changes, this has the potential to increase the distress of TGD youth (Steensma et al., 2011). One UK-based study reported that between 21.7% and 47.8% of 16–25 year-old TGD participants were struggling with an MH condition, compared to 18.8% in the general population (Office for National Statistics, 2017; Rimes et al., 2019).
A model which attempts to explain the higher rates of MH problems in TGD people is the Gender Minority Stress Model (GMS Model; Hendricks & Testa, 2012). It is based on theories which consider conditions in the social environment to be sources of stress (Pearlin, 1989), and is an extension of the Minority Stress Model (Meyer, 2003). The GMS Model explains how members of gender minority groups are disproportionately affected by social stress due to their minority status in society. This experience includes both proximal stressors (which take place on a personal/individual level, such as internalised stigma) and distal stressors (which take place on a societal level, such as discrimination; Mongelli et al., 2019).
GMS theorises that the higher incidence of MH difficulties in TGD individuals is directly related to the stress that they experience due to being part of a marginalised group (Hendricks & Testa, 2012). Studies have linked higher rates of psychological distress in TGD 18–40 year-olds to higher levels of GMS (Staples et al., 2018). Distal minority stressors have been found to be a predictor of suicide attempts, and proximal minority stressors a predictor of depressive symptoms in American TGD adults (Brennan et al., 2017). GMS also applies to trans and gender diverse young people (TGDYP; Chavanduka et al., 2021), with a recent cross-sectional study finding that high levels of internalised transphobia (a proximal stressor) were associated with higher depression and anxiety in American TGDYP (Chodzen et al., 2019).
Heteronormative beliefs endorse heterosexuality as the only valid sexual orientation with the associated implications for male and female gender roles, resulting in ongoing discrimination against LGBT people (Habarth, 2014). They are a major contributor to GMS, as prejudice and discrimination are directed towards those who do not fit these approved norms (Habarth, 2014). Heteronormative beliefs impact on gender minorities both overtly, such as within healthcare settings when TGD individuals delay seeking treatment due to discrimination, and covertly, an example of which is the poor representation of TGD individuals in advertising (Jaffee et al., 2016; Nielsen et al., 2000). In TGDYP, heteronormativity is argued to contribute to psychological distress through increasing experiences of health inequalities, stigma, violence and discrimination (Zeeman et al., 2019).
The current research
While GD plays a role in the relationship between psychological distress and TGD identities, the GMS Model posits GMS as another contributor in this relationship. Existing research alludes to heteronormative beliefs and attitudes also contributing to GMS-related experiences. Much of the research in this area has been conducted with adult populations, yet the evidence base suggests that adolescence and young adulthood is a common and challenging time to be questioning one’s gender identity. The research question explored whether GMS and heteronormative beliefs contribute to the psychological distress experienced by TGD adolescents and YP when variance related to GD is controlled for.
Hypotheses
Anxiety and depression scores will be higher in TGD participants than in cisgender participants. Well-being scores will be lower in TGD participants than in cisgender participants.
For TGD participants: 3. Higher scores for distal stress and proximal stress will be positively associated with depression and anxiety scores, and negatively associated with well-being scores, when GD is controlled for. 4. Higher scores on the Heteronormative Attitudes and Beliefs Scale (HABS) will be positively associated with depression and anxiety scores, and negatively associated with well-being scores, when GD is controlled for. 5. Higher scores for resilience will be negatively associated with depression and anxiety scores, and positively associated with well-being scores, when GD is controlled for.
Methods
Participants
Participants were aged between 16 and 25 years-old and living in the UK at the time of participation. Participants were recruited through local education centres, social media pages, internal advertising within the hosting University and through LGBTQ+ organisations across the UK.
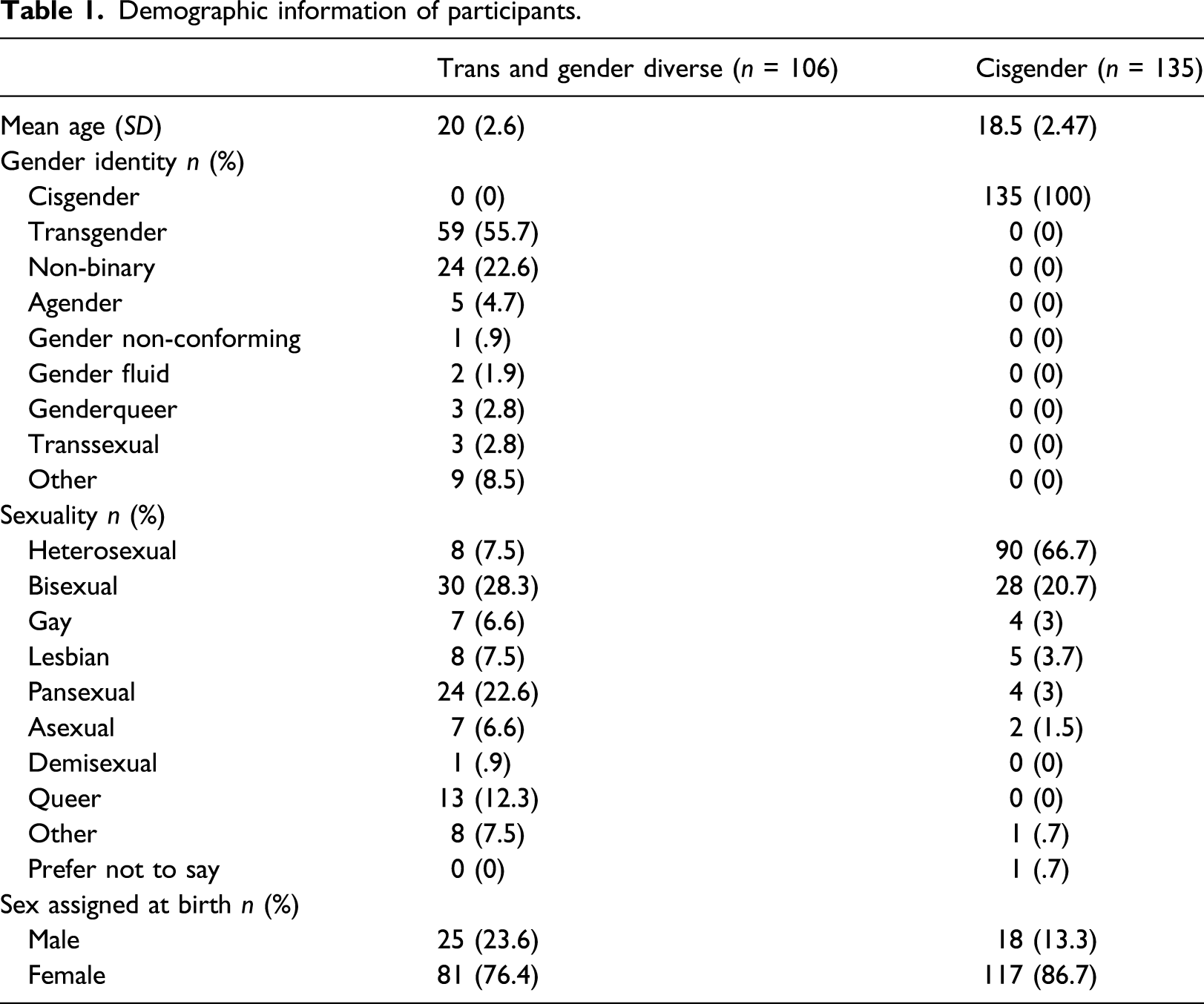
Demographic information of participants.
Design and procedure
We collected study data using an online survey. Ethical considerations included ensuring that the information given to participants and the measures that they completed did not trigger excess emotional distress, and that participants were aware of this being a risk before taking part. Ethical approval was granted by the hosting University's Psychology research ethics panel (ref 19-008). The study design was guided by input from a local LGBTQ+ youth group: the format and wording used on recruitment posters, information sheets and debriefs were changed according to this feedback.
Measures
Demographics
Participants answered questions describing their age, relationship status, ethnicity, nationality, educational level, sexuality and gender identity. Demographic information relating to sexuality and gender identity was collected using multiple-choice options (as listed in Table 1), but participants were also able to define these characteristics using free-text boxes under ‘other’.
Patient Health Questionnaire-9
The Patient Health Questionnaire-9 (PHQ-9; Spitzer et al., 1999) is a nine-item questionnaire designed to measure depressive symptoms which has been validated for use with adolescents (Richardson et al., 2010). Each item is scored on a four-point Likert scale (‘0 = not at all’ to ‘3 = nearly every day’) with higher scores indicating more severe depressive symptoms. It had good internal consistency (α = .91) in the current study.
Generalised Anxiety Disorder Assessment
The Generalised Anxiety Disorder Assessment (GAD-7; Spitzer et al., 2006) is a seven-item instrument measuring GAD symptoms validated for use with adolescents (12–17 years; Mossman et al., 2017). Each item is rated on a four-point Likert scale (‘0 = not at all’ to ‘3 = nearly every day’) with higher scores indicating more severe symptoms. It had high internal consistency (α = .89) in the current study.
Warwick–Edinburgh Mental Well-being Scale
The Warwick–Edinburgh Mental Well-being Scale (Tennant et al., 2007) is a 14-item instrument which measures general mental well-being, validated for use with adolescents (Clarke et al., 2010). There are five response categories (1 = ‘none of the time’ to 5 = ‘all of the time’). Lower scores indicate poorer mental well-being. It had good internal consistency (α = .92) in the current study.
The GenderIidentity/Gender Dysphoria Questionnaire for Adolescents and Adults
The Gender Identity/Gender Dysphoria Questionnaire for Adolescents and Adults (GIGDQ-AA; Deogracias et al., 2007) is a 27-item questionnaire developed as a dimensional measure of gender identity/GD in adolescents and adults. Each item is scored on a five-point Likert scale (‘1 = always’ to ‘5 = never), and the score is averaged to give a final score of between one and five. Lower scores are indicative of more gender identity difficulties. Scores of 3 or below are suggested as being indicative of GD. The GIGDQ-AA was adapted for this study, as it was identified in the planning stages that the language excluded non-binary individuals. It retained good internal reliability (α = .98) in the current study.
The Gender Minority Stress and Resilience Measure
The Gender Minority Stress and Resilience Measure (GMSR; Testa et al., 2015) measures nine constructs to assess minority stress and resilience factors in TGD people. Four of the subscales measure distal factors, three measure proximal factors, and two measure resilience factors, with five to nine items per subscale and a total of 58 items overall. The concepts of distal and proximal stressors refer to external sources of minority stress (e.g. violence and discrimination) and internal sources (e.g. negative expectations for the future and internalised transphobia), respectively.
Answers for items in the subscales looking at ‘gender-related discrimination/rejection/victimization’ are scored with a zero for ‘no’ and one for any other answer (‘yes, before age 18/after age 18/in the past year’). The remaining subscales (‘non-affirmation of gender identity’, ‘internalised transphobia’, ‘negative expectations’, ‘non-disclosure’, ‘community connectedness’ and ‘pride’) have five response categories ranging from 0 for ‘strongly disagree’ to 4 for ‘strongly agree’. Higher scores on the distal and proximal stressor scales indicate more minority stress while higher scores on the pride and community connectedness subscales indicate higher resilience. The subscales had good internal validity (between α = .73 and α = .97) in the current study. Due to researcher error, the GMSR scale was administered with a subscale missing from the proximal stress scale (non-disclosure). The internal reliability of this scale was found to be acceptable (α = .73) and was therefore included in the analysis.
Heteronormative Attitudes and Beliefs Scale
The Heteronormative Attitudes and Beliefs Scale (HABS; Habarth, 2014) is a 16-item measure consisting of two subscales (‘essential sex and gender beliefs’ and ‘normative behavioural attitudes’), designed to measure heteronormative attitudes and beliefs in respondents. It was initially validated with a group of participants aged 22 years and older so is not currently validated with a younger age group. Items are scored on a seven-point Likert scale (1 = ‘strongly disagree’ and 7 = ‘strongly agree’). Higher scores are indicative of stronger heteronormative beliefs/attitudes. Both subscales had good internal consistency (α = .8 - α = .89) in the current study.
Analysis plan
We completed assumption testing to confirm that our data met the assumptions of collinearity, independence of residuals, homogeneity of variance, and multicollinearity. We also checked the internal reliability of our measures. We dummy coded the variable for sex assigned at birth (0 = male and 1 = female) and sexuality (0 = heterosexual and 1 = all other sexualities) to allow us to incorporate these nominal variables into the regression analysis.
Correlation matrix of variables.
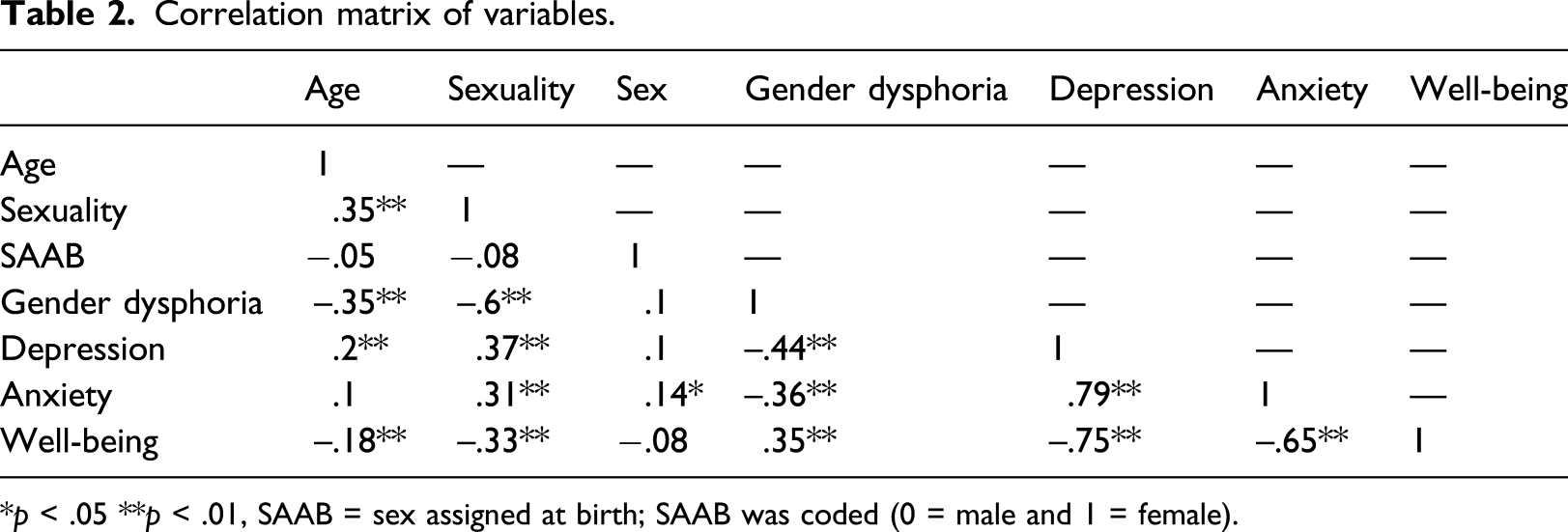
*p < .05 **p < .01, SAAB = sex assigned at birth; SAAB was coded (0 = male and 1 = female).
To test hypotheses 1 and 2, analyses of covariance were used, controlling for age, sexuality and SAAB, to test the difference in means between the two participant groups (cisgender and TGD) on the three DVs. For hypotheses 3–5, hierarchical regression analyses were used to identify the association between DV scores and independent variables (IVs; distal/proximal stress scores, resilience scores and heteronormative beliefs and attitudes) for TGD participants only, controlling for age, sexuality, SAAB and GD. A separate regression analysis was run for each of the three DVs.
Results
Analyses of covariance
Depression, anxiety and psychological well-being
Means and SDs by participant group.
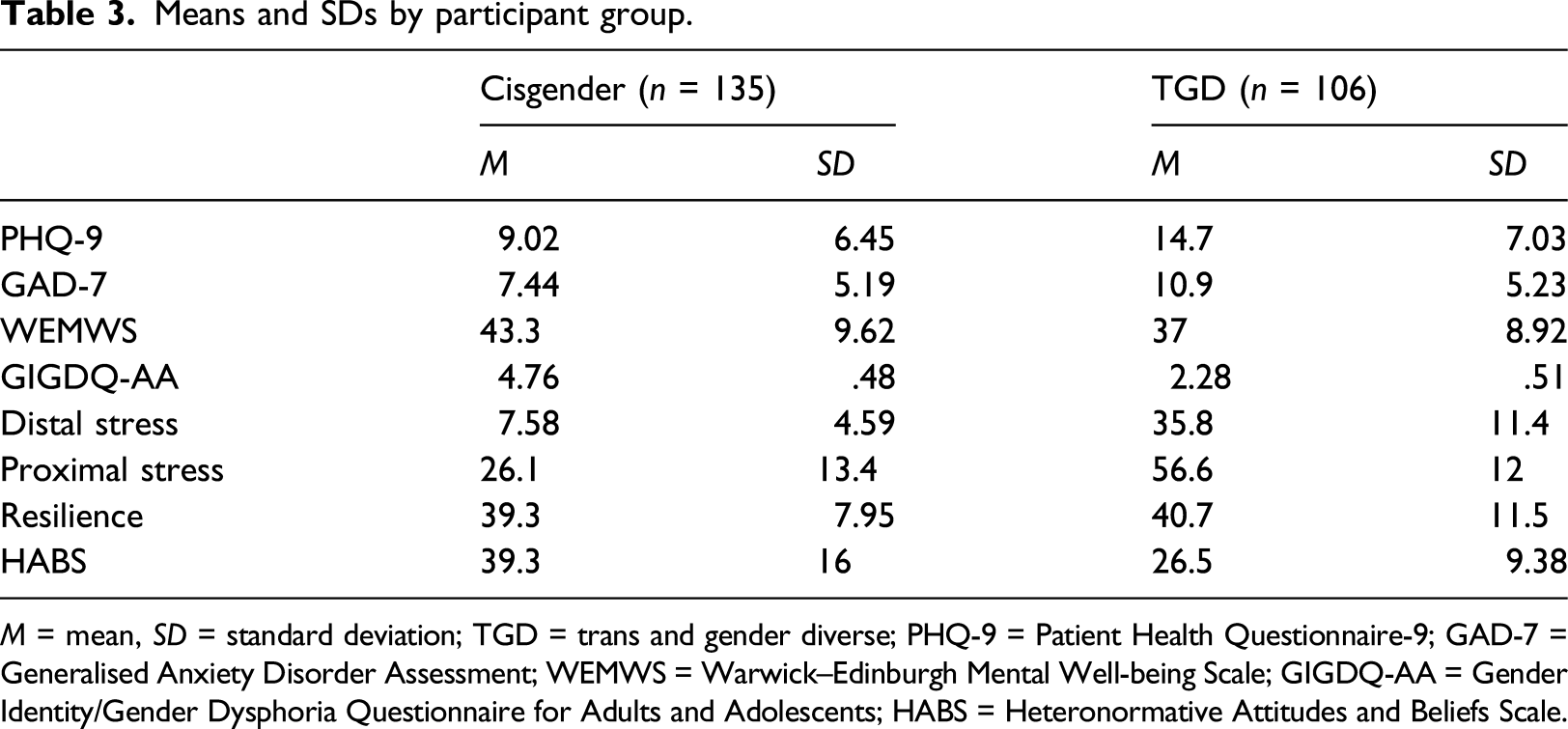
M = mean, SD = standard deviation; TGD = trans and gender diverse; PHQ-9 = Patient Health Questionnaire-9; GAD-7 = Generalised Anxiety Disorder Assessment; WEMWS = Warwick–Edinburgh Mental Well-being Scale; GIGDQ-AA = Gender Identity/Gender Dysphoria Questionnaire for Adults and Adolescents; HABS = Heteronormative Attitudes and Beliefs Scale.
Hierarchical regression analyses
Four models were used for our hierarchical regression analyses predicting the outcome variables depression, anxiety and well-being. Model 1 included age, sexuality and GD, Model 2 added distal and proximal stress, Model 3 added heteronormative beliefs and Model 4 added resilience.
Depression
Hierarchical regression analysis for variables predicting depression scores in TGD Participants (n = 106).
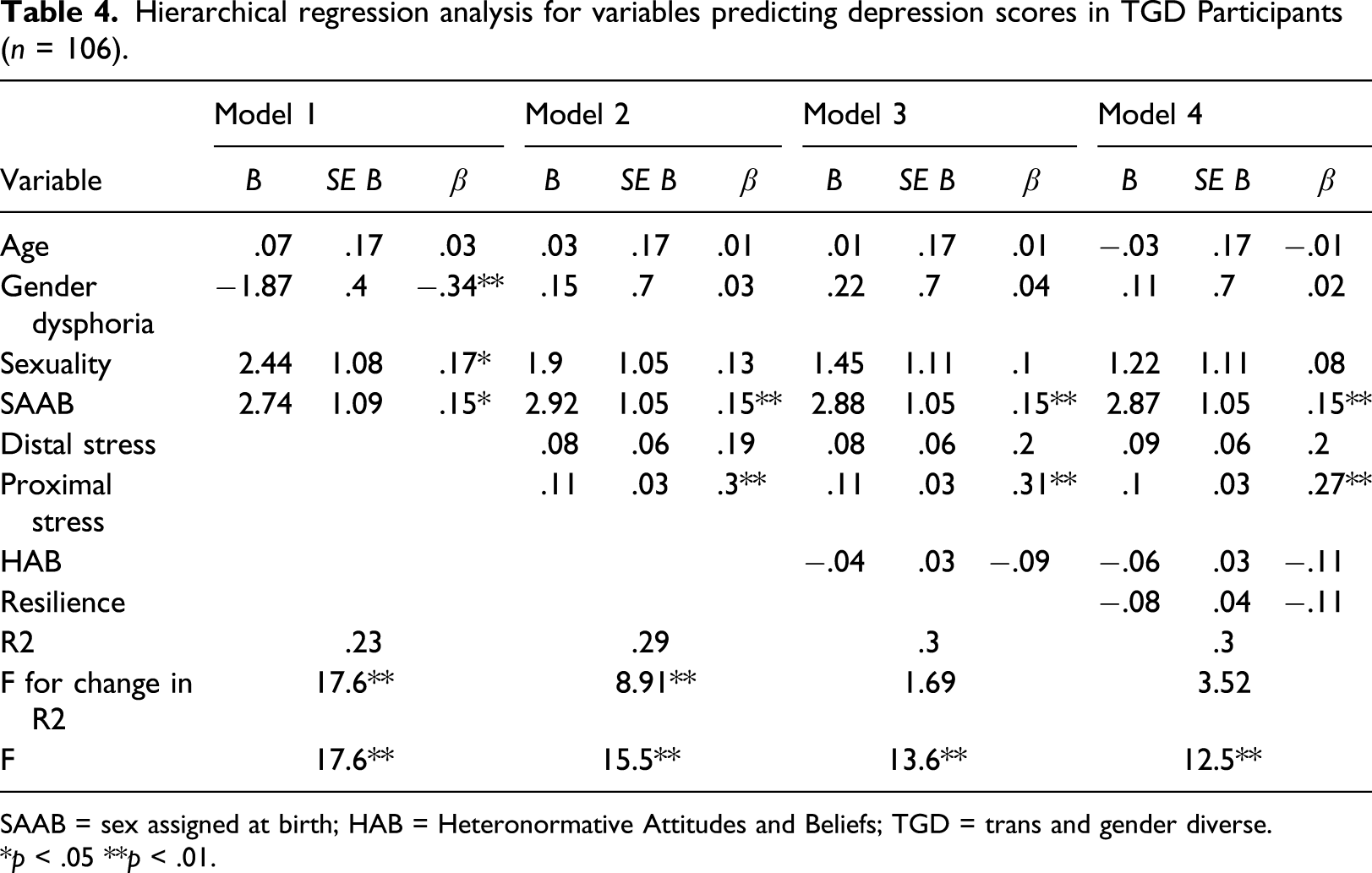
SAAB = sex assigned at birth; HAB = Heteronormative Attitudes and Beliefs; TGD = trans and gender diverse.
*p < .05 **p < .01.
Anxiety
Hierarchical regression analysis for variables predicting anxiety scores in TGD Participants (n = 106).
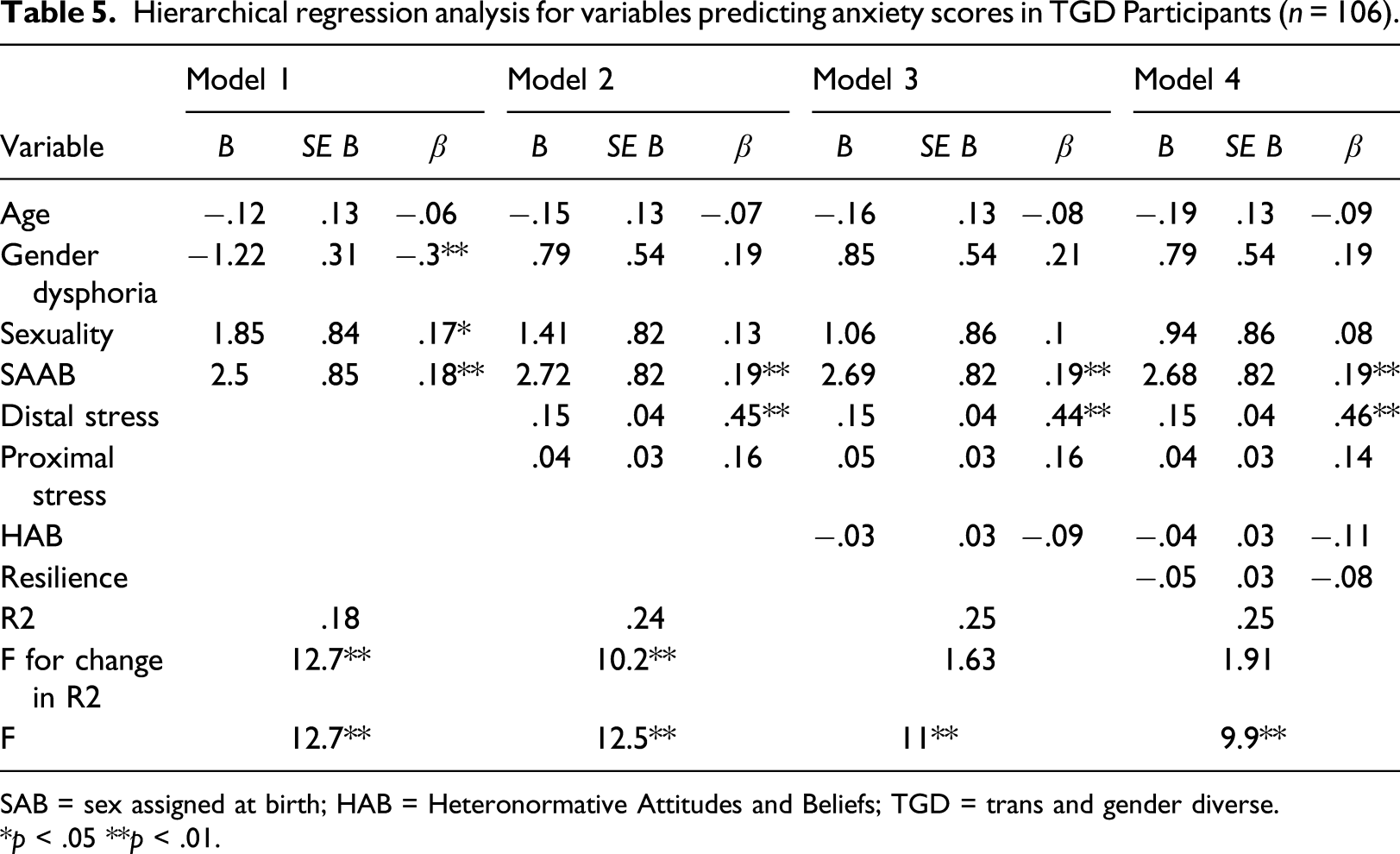
SAB = sex assigned at birth; HAB = Heteronormative Attitudes and Beliefs; TGD = trans and gender diverse.
*p < .05 **p < .01.
Well-being
Hierarchical regression analysis for variables predicting well-being scores in TGD participants (n = 106).
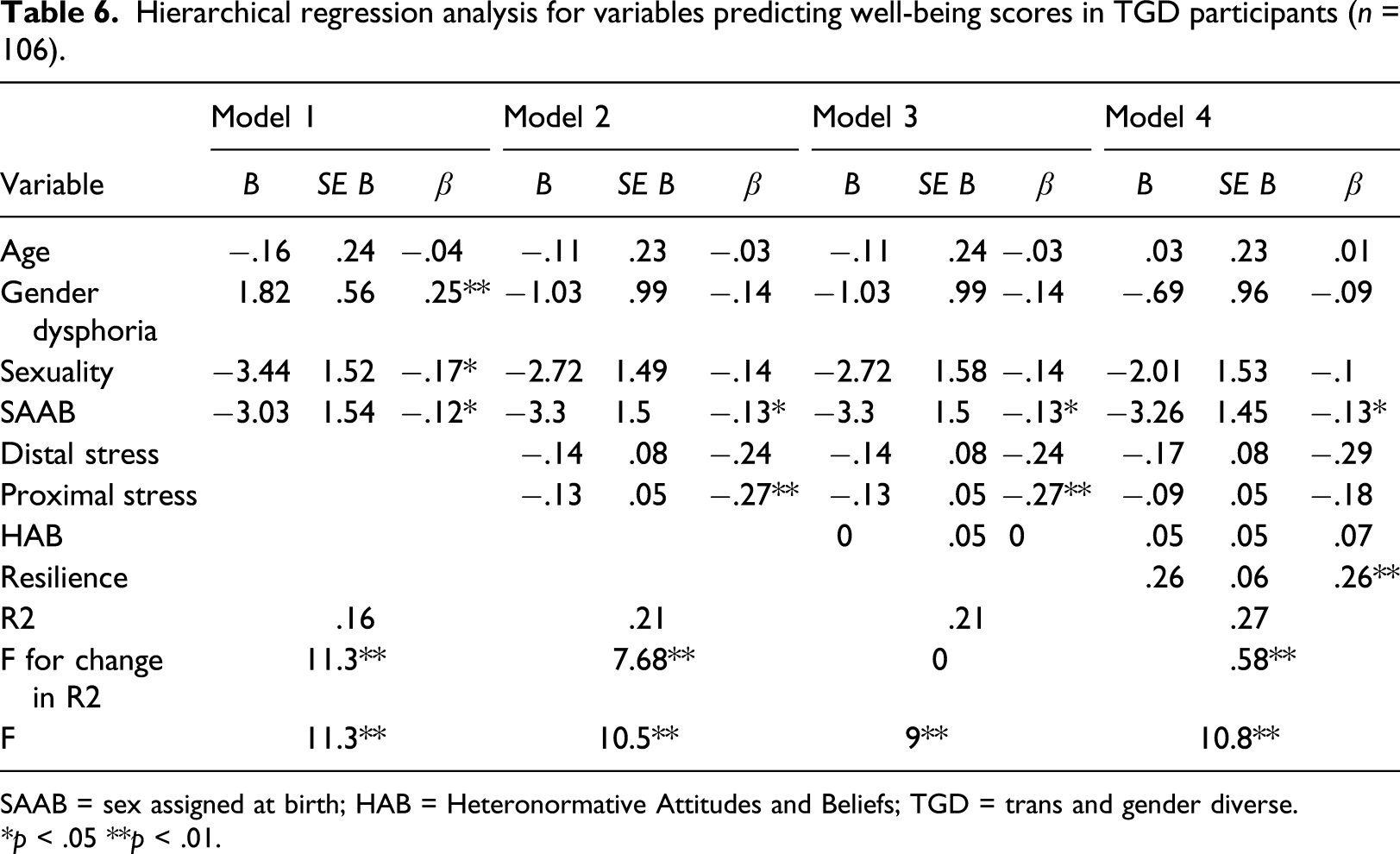
SAAB = sex assigned at birth; HAB = Heteronormative Attitudes and Beliefs; TGD = trans and gender diverse.
*p < .05 **p < .01.
Discussion
The aim of this study was to explore how participants’ experience of gender minority stress and their heteronormative attitudes and beliefs were associated with psychological distress. We found support for our hypothesis that there would be higher levels of anxiety and depression and poorer psychological well-being in TGD participants. There was support for the hypothesis that higher distal and proximal minority stress would be associated with greater anxiety and depression and poorer well-being in TGD participants, even after adjusting for GD. The hypothesis regarding heteronormative beliefs was partly supported, as lower heteronormative beliefs only predicted higher well-being before resilience was included in the regression model. There was partial evidence for our final hypothesis, as participants with higher resilience had better psychological well-being. However, we did not find a significant relationship between resilience and depression/anxiety scores.
The finding that levels of anxiety and depression were significantly higher and psychological well-being significantly lower in TGD participants is in keeping with the existing literature in this area (Rimes et al., 2019). In the TGD group, 88.7% of participants met the clinical cut-off for a diagnosis of GD. However, our findings suggest that GD is only part of the picture when it comes to explaining the relationship between being TGD and poor MH. GD was only a significant predictor of higher levels of depression and anxiety when minority stressors were not factored into the models. This highlights that GMS and resilience are associated with the variation in scores more so than GD alone.
Depression had a stronger relationship with proximal stressors and anxiety with distal stressors. This relationship is supported by the existing literature (Bockting et al., 2013). Although not all TGD individuals report feeling distressed about their gender identity, in general, they still experience more MH difficulties as a group than cisgender individuals. Our findings offer an explanation as to why this might be, supporting the argument that minority stress is a key factor in the relationship between higher levels of anxiety and depression and being a TGDYP (Hendricks & Testa, 2012).
It is unclear why heteronormative attitudes and beliefs were not associated with depression, whereas proximal stressors (including internalised transphobia) were. One possible explanation is that having more flexible beliefs about gender roles and normative behaviours acts as a protective factor against emotional distress but is not enough in itself to reduce distress. Alternatively, heteronormative attitudes and beliefs may be factors which moderate other aspects of GMS rather than directly impacting on emotional distress. However, there is not currently much research to explain this relationship in more detail.
Resilience (consisting of pride and community connectedness) was associated with higher well-being scores but not with lower anxiety or depression. Although their study looked at an adult TGD population, Bockting et al. (2013) found that family support, peer support and identity pride were negatively associated with psychological distress and were therefore felt to be protective factors. With our younger population, it is likely that these factors would be as protective, if not more so. Adolescents and young adults are more likely to be living with their family, so family and peer relationships are of particular importance (Johns et al., 2018).
Clinical implications of the findings
While supporting TGD adolescents and YP, focussing only on reducing difficult emotional experiences might improve negative symptoms, but may not necessarily improve general well-being. There appear to be different pathways and processes through which symptoms of mental ‘illness’ operate, in comparison to mental ‘well-being’ at the other end of the scale. This is in line with research which suggests that mental well-being exists relatively independently from symptoms of mental illness (Weich et al., 2011). To improve mental well-being as well as reduce emotional distress, our findings suggest that we need to consider building resilience as well as attending to GD and GMS.
Specialist services could draw on this research to educate other professionals about the role of GMS in the psychological well-being of TGD YP by asking questions about this in assessments and including this as a factor in formulations and interventions. On a societal level, our research suggests that gender minority stressors are having a detrimental impact on the MH and well-being of TGD youth. Services should consider how they can actively engage in shifting public attitudes towards TGD adolescents and YP by working with the wider community.
Limitations and directions for future research
A significant limitation of this research is the cross-sectional design of the study, which cannot tell us about the direction of the relationship between our variables. While it is possible that participants who experience more GMS may have higher levels of anxiety and depression as a result, the direction of the relationship may be the opposite. This would make sense in the context of cognitive biases, such as the attentional bias towards external negative cues associated with high levels of anxiety, and a bias towards interpreting ambiguous situations in a negative light in depressed individuals (Wisco & Nolen-Hoeksema, 2010).
Due to researcher error, the GMSR scale was administered without one of the nine subscales (non-disclosure). We checked the internal reliability of the subscale (proximal stress) and found that the reliability was acceptable (α = .73). Another limitation concerns the gender-related discrimination, victimization and rejection subscales (distal stress), which were not inclusive of participants aged under 18. There is now a measure which has been adapted for adolescents which we were unfortunately not able to use in this research (Hidalgo et al., 2019). Future research would benefit from using this adolescent-specific measure to explore GMS in this population.
Not more than 30% of the variance in scores can be accounted for by the models tested in this research, which is important when it comes to interpreting the meaning of our findings. There are likely to be a range of other factors involved in mediating this relationship, including childhood maltreatment/abuse, which has been found to be more common for TGD individuals (Bandini et al., 2011). It would be beneficial for future research to collect data from participants in relation to these factors to see if other models may account for a greater proportion of the variance in scores.
While the samples are matched in terms of SAAB being predominantly female in both groups, it is acknowledged that in the cisgender group this may limit the generalisability of the results, as in the general population the split between AFAB and AMAB is closer to 50% and 50%. The distribution of SAAB was not intentional and is likely a result of the opportunistic sampling method used.
We note that most of the existing research referred to within the discussion section has been conducted with adult populations. More research with TGD adolescents and young people is needed to confirm and replicate the outcomes of this study. It would also be helpful to look more closely at heteronormativity and the role this factor might play in mediating levels of anxiety, depression and general well-being in TGD adolescents and YP.
Conclusion
This study explored the relationship between GMS, resilience, heteronormative beliefs and the psychological well-being of TGD adolescents and young people. Our hypotheses were largely supported, although resilience and heteronormative beliefs did not have the predicted relationship with anxiety and depression. Our results support much of the existing literature, and we extend these findings by identifying that GMS plays more of a significant role in predicting psychological outcomes for this group of individuals than GD. This is somewhat contrary to other research and has not been explored in other existing studies.
Footnotes
Acknowledgements
The authors give thanks to members and facilitators of a local LGBTQ+ youth group, without whom we would have lost the richness and authenticity of this research. Their input in the planning stages was invaluable, and we would not have been able to make such a success of this without them.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Kate is funded by a National Institute for Health Research (NIHR) Clinical Doctoral Research Fellowship for this research project (ICA-CDRF-2018-04-ST2-047).