
Abstract
Background
Social Anxiety Disorder (SAD) is one of the most common disorders of adolescence and results in marked impairments in social and academic/occupational activities that likely to persist into adulthood. Multiple etiological factors contribute to the development of social anxiety disorder. Two critical factors in presenting with a primary diagnosis of SAD might be adverse childhood experiences (ACEs) and attachment styles. The current study examined how ACEs and attachment styles may be related to SAD in adolescents.
Methods
60 participants with ages ranging from 11 to 18 (M = 14.6; female = 36), who have a primary diagnosis of SAD and 60 control group adolescents (M = 14.6; female = 30) were included in the study. Both groups completed the Liebowitz Social Anxiety Scale (LSAS), the Childhood Trauma Questionnaire (CTQ), and the Adolescent Relationship Scales Questionnaire (A-RSQ).
Results
After controlling adolescent gender and parental education levels, childhood emotional neglect and income significantly predicted an increased risk for adolescents’ SAD diagnosis. Attachment styles did not significantly contribute to predicting adolescents’ SAD diagnosis after controlling childhood emotional neglect.
Conclusion
The high predictive value of emotional neglect in childhood emphasizes its importance as a risk factor of SAD in adolescence.
Introduction
Social Anxiety Disorder (SAD), also referred to as social phobia, is one of the most frequent anxiety disorders, affecting about 1% to 10% of adolescents (Burstein et al., 2011; Merikangas et al., 2010). The Diagnostic and Statistical Manual of Mental Disorders, 5th ed. (DSM-V), describes SAD as an intense, irrational, and persistent fear of being scrutinized or negatively evaluated by others. People with SAD feared social or performance situations that typically provoke an immediate anxious reaction as well as avoidance of such situations. To meet the diagnostic criteria for this disorder, the symptoms must be severe enough to cause marked distress or disability with daily life or work, and that a minimum duration of 6 months (American Psychiatric Association, 2013). SAD can be reliably diagnosed in children and adolescents using the same diagnostic criteria to identify cases across various age groups (Heimberg et al., 2014).
This excessive fear of negative evaluation by others and generalized avoidance and distress in social situations are often associated with substantial impairments in important facets of life, such as school and academic life or relationships with family and friends, which play a substantial role in adolescent development and have significant implications in adult life (Stein & Kean, 2000). Since the age-of-onset is typically in adolescence and often follows a chronic and recurrent course (Krumpal, 2013; Stein et al., 2017), it is vital to understand factors in youths that may serve to either exacerbate or reduce SAD symptoms. Although anxiety has a genetic component (Thomason et al., 2017), social anxiety may also result from experiences during early childhood. There has been growing recognition of the potential links between an insecure attachment style, traumatic life events, especially early childhood adversities (ACEs), and the development, maintenance, and progression of mental health problems in general (Chen et al., 2010; Scott et al., 2008).
Adverse Childhood Experiences (ACEs), also called childhood trauma, refer to various types of maltreatment and stress sources that occur to children under 18 years of age (Felitti et al., 1998). It includes all kinds of physical and/or emotional ill-treatment, sexual abuse, neglect, or other adverse circumstances within the household, which results in actual or potential harm to the child’s health and development (Felitti et al., 1998). Broad categories in types of events that are classified as ACEs vary greatly. There may be differences in the characteristics of events that are specifically important for SAD outcomes.
Abuse is a mistreatment of children and can come in many forms including physical, sexual, verbal or emotional maltreatment. Neglect is a failure to provide consistent care and ignoring or not meeting child’s necessary needs whether physical or emotional. Both abuse and neglect can carry on in a child’s life with many long-term effects, including both physical and mental health problems (Miller et al., 2018). A few studies show that different types of childhood adverse life events such as unfavorable parenting behaviors (Bandelow et al., 2004; Erwin et al., 2006), childhood physical and sexual abuse (Chartier et al., 2001), and emotional maltreatment (Taillieu et al., 2016) are associated with SAD. Still, there remains a paucity of evidence on specific kinds of ACEs that may particularly predict SAD in adolescence.
Quality of early attachment between children and parents is another factor that has been linked to the development of the condition in some studies (Brumariu & Kerns, 2008; Vertue, 2003). Attachment theory posits that a secure attachment with the primary caregiver is critical for development (Bowlby, 1969), and it tends to influence an individual’s perceptions of self and others throughout the lifespan (Ainsworth, 1979). If the caregivers provide warm, close, and consistent care, the child’s attachment is likely to be secure, but if the caregivers are inconsistent, neglectful, less responsive, and sensitive, then the child’s attachment is likely to be insecure (Ainsworth, 1979). This early experience with the primary caregiver has the critical features influencing how an individual experiences and processes later interpersonal relationships (Brumariu & Kerns, 2008). In particular, there may be parallels between the early experiences of exclusion or rejection from the attachment figure and later fear of social exclusion or social rejection (Vertue, 2003). Insecure attachment influences maladaptive interpersonal behaviors and dysfunctional emotion regulation strategies, which subsequently contribute to SAD development in adults (Bifulco et al., 2006; Eng et al., 2001). Although studies have recognized the insecure attachment style as a risk factor for developing SAD, the relationship between specific attachment patterns and SAD in adolescents has not been dealt with in-depth.
Given that childhood ACEs and attachment styles appear to be particularly important in predicting SAD (Bandelow et al., 2004; Brumariu & Kerns, 2008), increasing knowledge about these key indicators is vital to developing and improving interventions aimed at its prevention and treatment. To our knowledge, no study examined the different facets of ACEs and attachment styles in the same study and compared these with a clinical sample of adolescents with SAD. Therefore, the purpose of the current study is to expand on previous findings by investigating the relation between SAD, ACEs, and attachment styles, using a well-evaluated patient group in comparison to age and gender-matched comparison group.
Methods
Participants
Our sample included 60 adolescent cases with Social Anxiety Disorder (SAD), and 60 healthy controls. Eighty-five patients who were diagnosed with SAD and admitted to receive treatment from the Child and Adolescent Psychiatry outpatient clinic of the Istanbul University Faculty of Medicine were given information about the study and were asked to participate in the study. Patients were eligible for the study if aged 11 to 18 years and met DSM-5 criteria for a primary diagnosis of SAD. 60 patients who agreed to participate were interviewed in person by the primary investigator. The diagnosis of the SAD was confirmed by the PI, who is a child psychiatrist based on the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) SAD criteria. A SAD diagnosis was ascertained by administration of a structured DSM-5 symptom checklist. In DSM-5, the criterion is tied to the clinician’s judgment that socially anxious individuals overestimate the likelihood of negative outcomes in social situations and underestimate their likeability, social, and behavioral performance (Heimberg et al., 2014).
Exclusion criteria were severe current medical illness or present (or a history of) other mental disorders, including major depression, bipolar disorder, obsessive-compulsive disorder, posttraumatic stress disorder, substance abuse, or personality disorder. Participants with a comorbid disorder diagnosis were excluded to reduce the potential confounding influence of comorbid disorders in the group of SAD. The healthy controls were recruited predominantly through different departments of the same primary medical care facility from fliers and advertisements and using the snowball method in which already recruited controls were asked to invite participants who may be interested in the study. Within 6 months of recruitment flyers, this process continued until a sex and age control was recruited for each case. 83 phone inquiries were received by the PI, and 60 of those adolescents met our inclusion criteria. Those who agree gave signed consent and were interviewed. Healthy controls with no history of mental health diagnosis completed the same interview and questionnaires. Protocol for this research project was approved by the ethics committee of the Child and Adolescent Psychiatry of the Istanbul University Faculty of Medicine (IRB Protocol 2016/997). Study participation was voluntary and written informed consents were obtained from SAD and healthy controls prior to study participation.
Measures
Liebowitz social anxiety scale
The LSAS (Liebowitz, 1987) was used to establish that participants are still experiencing SAD. LSAS is a commonly used self-report measure of social anxiety symptom severity and comprises 24 social situations that are each rated for level of fear (0 = none to 3 = severe) and avoidance (0 = none to 3 = usually) for the past week. The Turkish version of LSAS has well-documented psychometric properties (Soykan et al., 2003). In the present study, the scale showed good internal consistency (Chronbach’s α= 0.92).
Adolescent relationship scales questionnaire
The A-RSQ (Scharfe et al., 2002) is the revised version of the Relationship Scales Questionnaire (RSQ; Bartholomew and Horowitz, 1991; Griffin & Bartholomew, 1994). The RSQ is a self-report questionnaire used to assess underlying attachment dimensions in close relationships and can be used to categorize participants into one of four prototypical attachment patterns: secure, fearful, preoccupied, and dismissing. The A-RSQ has a 5-point Likert scale (1 = not at all to 7 = very much), and participants rate the extent to which each statement best describes their characteristic style in close relationships. For each subscale, the items’ mean score was calculated by adding the scores on the individual items and dividing the summation by the number of items. Thus, each participant had four mean scores, one for each subscale. There is no research investigating the psychometric properties of the adolescent version, but there has been some research on the psychometric properties of the adult versions of the scale in the Turkish population (Sumer & Gungor, 1999), and it has been used in studies using Turkish adolescent sample (Erkan et al., 2015; Gençoğlan et al., 2016).
Childhood trauma questionnaire
Adolescents' recall of childhood trauma was measured using the Childhood Trauma Questionnaire (CTQ; Bernstein et al., 1994), a 28-item screening questionnaire intended to quantify self-reported childhood trauma history in the home. The CTQ measures childhood trauma using five subscales: emotional abuse, physical abuse, sexual abuse, emotional neglect, and physical neglect. Responses are measured on a 5-point Likert scale (1 = never true to 5 = very often true). Each subscale is represented by five questions with a score range from 5 to 25. The Turkish version of CTQ has well-documented psychometric properties (Sar et al., 2012). The Cronbach’s α within individual subscales ranged from 0.52 to 0.86 for this study.
Demographic form
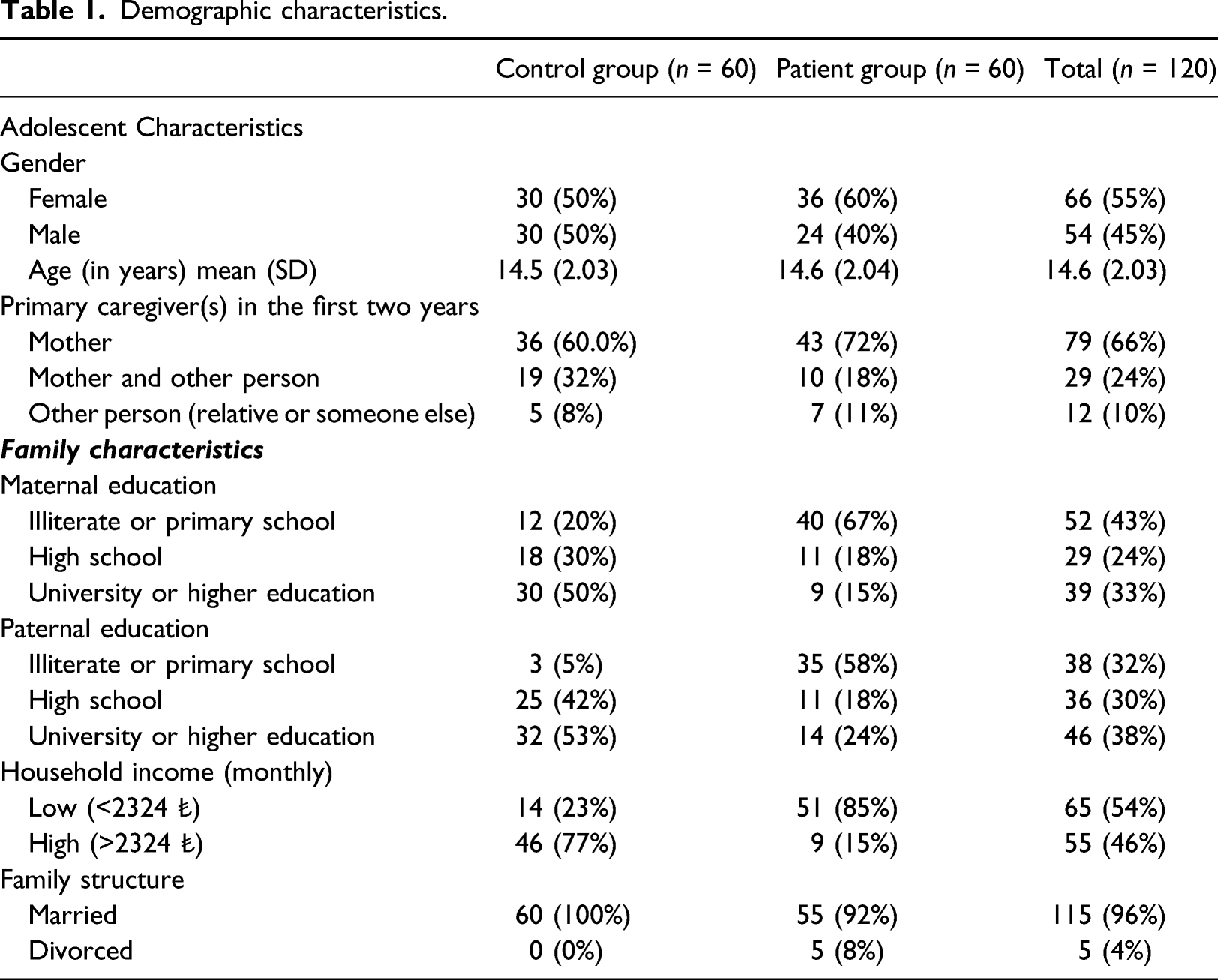
Demographic characteristics.
Analysis plan
Data analysis took place in two steps. First, differences between groups were tested using t-tests for continuous variables and chi-squared tests for categorical data. The variable that is significantly associated with the outcome is parental education levels, and family income was also considered in the analysis in order to control for potential confounding. Second, binary logistic regression analysis was used to generate odds ratios of patients to controls to develop a model for predicting adolescents’ SAD from their attachment styles and their self-report of childhood adverse experiences.
Results
Sociodemographic characteristics
Participants were 120 adolescents (M = 14.6 years, SD = 2.03), ranging in age from 11 to 18 and 55% (N = 66) were female. Eligible adolescents in this study were either diagnosed with a Social Anxiety Disorder (SAD; N = 60, M = 14.6 years, SD = 2.04) or in the control group (N = 60, M = 14.6 years, SD = 2.04). There were no significant differences between the two groups with respect to gender, χ2(1) = 0.84, p = 0.35, or age, t(118) = −0.13, p = 0.89. Differences regarding maternal education level, t(117) = 5.83, p < 0.001, paternal education level, t(106) = 6.26, p < 0.001, and household income level, χ 2 (1) = 43.5, p < 0.001, were observed.
Controls generally had mothers (50%; N = 30) and fathers (53%; N = 32) who graduated from university at a significantly higher rate than mothers (15%; N = 9) and fathers (23%; N = 14) of participants with SAD. 85% (N = 51) of SAD patients had incomes lower than minimum wage, in contrast to 23% of controls (N = 14). Our data showed that the LSAS scores ranged from 54 to 186 in the total sample and patients with SAD (M = 134.2, SD = 23.5) had a significantly higher mean value in LSAS than controls (M = 90.1, SD = 21.8), t(117) = −10.61, p < .001.
Adverse childhood experiences
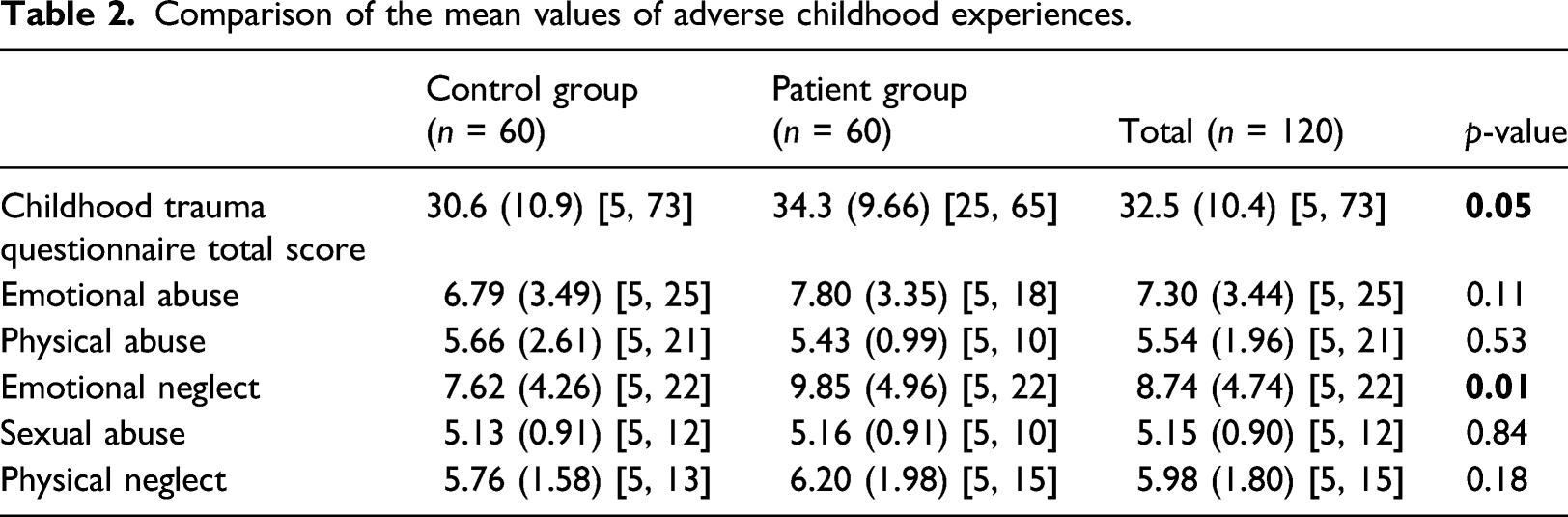
Comparison of the mean values of adverse childhood experiences.
Attachment styles
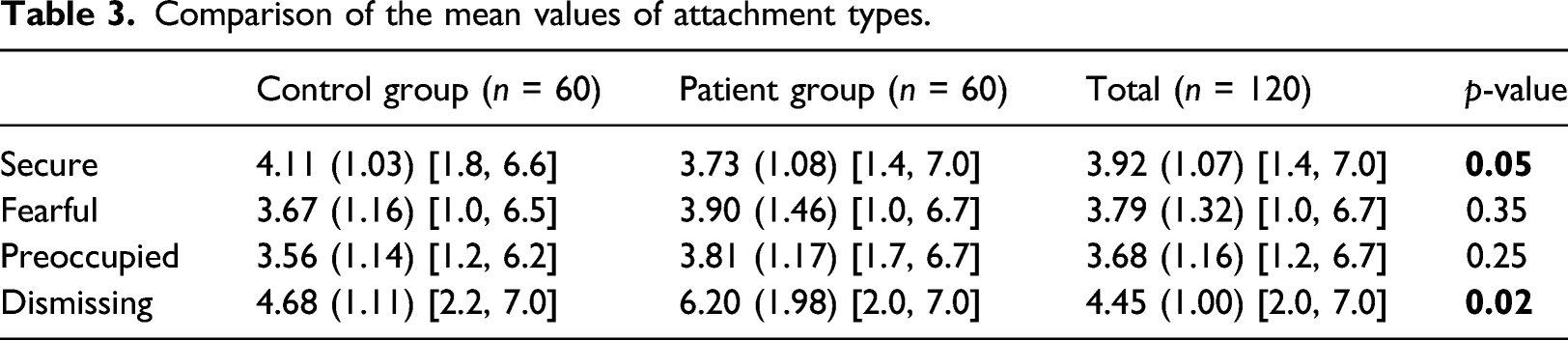
Comparison of the mean values of attachment types.
Binary logistic regression analysis
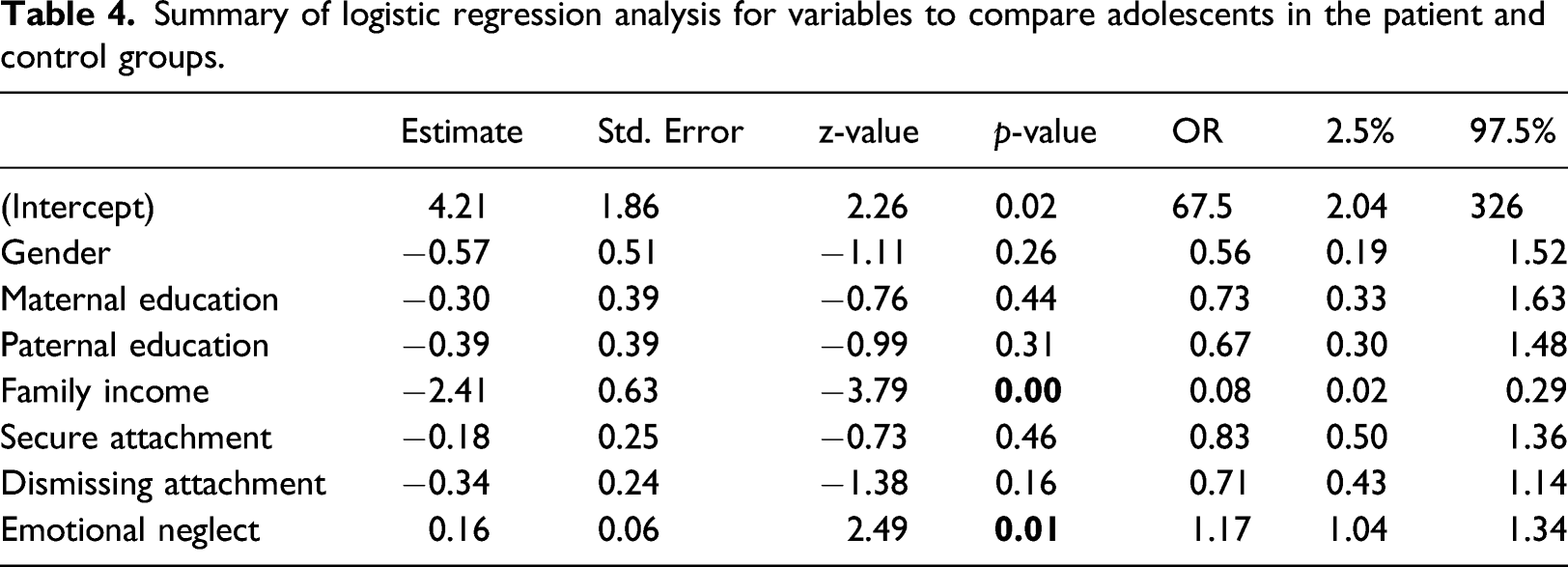
Analyses were conducted using adolescent SAD diagnosis as the dependent variable. Gender, maternal education, paternal education, and household income were controlled in the analyses. Emotional neglect and attachment styles were examined in the same model. We included secure and dismissing attachment styles separately to further inform the relationship.
Summary of logistic regression analysis for variables to compare adolescents in the patient and control groups.
Discussion
This study examined various types of adverse childhood experiences (ACEs) and attachment styles as psychosocial risk factors for developing Social Anxiety Disorder (SAD) in adolescents, using a clinical sample compared to the control group. Building on prior studies suggesting that insecure attachment styles and ACEs play critical roles in the development, maintenance, and progression of mental health problems (Chen et al., 2010; Scott et al., 2008), we pursued a rigorous approach to test which kinds of ACEs and attachment styles that may particularly predict SAD in adolescence.
Patients with SAD reported a higher number of total childhood adversities than control group adolescents, regardless of the type of the event. However, surprisingly, patients with SAD did not differ in subtypes of childhood adversities such as emotional, physical, or sexual abuse or physical neglect, compared to control group adolescents. However, patients with SAD reported childhood emotional neglect significantly more frequently than control group adolescents. Notably, the SAD-related difference in emotional neglect remained significant when we controlled for parental education, household income as well as attachment styles. Therefore, early childhood neglect was revealed as a risk factor associated with an increased probability of developing SAD in adolescence. Hence, our results emphasize the type of an adverse life event as a predictor of SAD.
This result supports evidence from previous research (i.e., Zhang et al., 2012; Johnson et al., 2000; Taillieu et al., 2016) that indicate emotional neglect is particularly predictive of psychopathologies characterized by avoidance of strangers and novelty, shyness, heightened sensitivity, and anxiety reactivity (Alden et al., 2002; Cox et al., 2005; Meyer et al., 2005), which is also implicated in the development of SAD and in the propensity for the development of various problems pursuant to SAD. Although childhood trauma and parental maltreatment are well recognized as being risk factors for numerous psychopathologies in general (Hernandez et al., 2012; Yen et al., 2002), the contribution of childhood neglect has received little attention (Carr et al., 2013; Hovens et al., 2010). This study shows the specific consequences of the types of maltreatment that the child may suffer and the unique contribution of emotional neglect to adolescent SAD, which corroborates these earlier findings linking neglect to increased risk for several mental health diagnoses in adults (Johnson et al., 1999, 2000; Sareen et al., 2005) including SAD (Taillieu et al., 2016).
It is important to consider which mechanisms might account for this relation. As stated earlier, emotional neglect is generally defined as caretakers’ failure to meet the child’s basic emotional and psychological needs, such as love, attention, motivation, encouragement, and emotional support, intentionally or not (Bernstein et al., 1994). Undoubtedly, a continuous frustrating and discouraging home climate with less parental positive attention, demonstration of love, and pride in the child could be harmful experiences. When caregivers are highly ambivalent about their children’s needs, especially when their children are hurt, crying, or looking for emotional support, a child might think she or he is not worthy of love and care. From a child’s perspective, the constant early childhood experience of emotional neglect might be perceived as invisible to others, which may affect the child’s perceptions of others as safe sources of comfort, support, and reassurance, a perception that might be the source of further social anxiety (Eikenaes et al., 2015).
Besides this, studies showed that emotional neglect is more strongly associated with problems in social behaviors than other types of maltreatment (Ometto et al., 2016; Paradis & Boucher, 2010). Severe neglect in childhood may affect emotion regulation development, and thereby children experience difficulties in emotional understanding (Kim & Cicchetti, 2010). Moreover, for neglected children, social situations may evoke negative self-views, lack of interpersonal trust as well as negative interpretations of others’ behaviors (Eikenaes et al., 2015). Such experiences could substantially impact the child’s future experience of social situations through the way they perceive and behave in future social situations. Therefore, it is reasonable to think that early maladaptive social experiences related to emotional neglect might lead to social dysfunctioning, which in turn predispose maltreated children to developing SAD.
This study’s results provide evidence of specificity regarding the associations between attachment styles and SAD in adolescents. Analysis of the type of attachment styles showed that the dismissive style was highly represented as an insecure attachment type in the patient group, and the secure style was found significantly higher in the comparison group. In accordance with the present results, previous studies have demonstrated that lower attachment security is related to higher social anxiety (Brumariu & Kerns, 2008; Bohlin et al., 2000), and dismissive attachment style is mainly associated with anxiety symptoms in general (Bifulco et al., 2006). There might be several explanations for the relationship between attachment styles and SAD in adolescents. Secure adolescents with a history of available, responsive, and sensitive relationships with the primary caregiver may experience positive aspects of social interaction such as positive affect, prosocial behaviors, and social initiative (Bohlin et al., 2000), therefore less likely to have SAD symptoms in adolescence.
Contrary to our results, a few studies indicated that dismissive attachment style is associated with less rather than more reported SAD symptoms (Bohlin et al., 2000; Brumariu & Kerns, 2008). Growing up with frustrating attachment experiences with the primary caregiver might result in dismissive avoidance from social relationships by hiding and suppressing feelings to avoid future potential rejection or disregard for interpersonal closeness during adolescence (Shumaker et al., 2009). It has been argued that individuals with the dismissive attachment style avoid intimacy in social situations; therefore, they are less likely to develop anxiety (Brumariu & Kerns, 2008). However, adolescents who rate their parents as a less significant source of attachment support may want less closeness with people in the future, but this may contribute to negative moods, more distress, and impairments when they encounter social situations.
Moreover, dismissive adolescents are emotionally distant and have difficulty making and keeping close friendships (Shumaker et al., 2009). As they experience the inability to form close interpersonal relationships, they may have limited opportunity to discover the peer relationships and achieve necessary social and emotional skills to know others better and become closer emotionally (Brumariu & Kerns, 2008). Therefore, limited social experiences and the inability to perceive others’ emotional states to manage interpersonal relationships thereby may contribute to higher social anxiety during adolescence, such as greater distress about and efforts to counteract interpersonal rejection in social situations than the nonclinical control sample.
On the other hand, the relationship between either dismissive attachment style or secure attachment style and SAD diagnosis in adolescents was not statistically significant after controlling for the experience of childhood emotional neglect. However, it is possible that emotionally neglectful parental behaviors might play a mediating role with regard to the pathway through which insecure attachment styles may lead to later impairments in social functioning. A parent’s poor attachment with his/her child can result in dysfunctional parenting, including low levels of affection and neglect, and these experiences may lead children to feel greater anxiety in future social and interpersonal relationships (Eng et al., 2001; Read et al., 2018). Even with the main predictors utilized in the study (attachment styles and adverse childhood experiences), more complex effects could be fit. This is an area for future research to further explain this relationship and identify additional mechanisms. The results of the current study suggest that childhood emotional neglect is the most potent risk factor of SAD diagnosis in adolescents and has an independent influence beyond what is predicted by attachment styles.
Although our results indicated no sex differences regarding SAD symptoms in adolescents and these findings differ from earlier studies (i.e., Inderbitzen et al., 1997; La Greca & Lopez, 1998), they are consistent with those of showing no sex differences regarding some forms of SAD symptoms (i.e., Brumariu & Kerns, 2008; Ranta et al., 2012). A possible explanation for this might be that there may be cultural variations in the sex differences of the Turkish sample of adolescents report for their symptoms of SAD compared to western cultures (Ranta et al., 2012). For example, sex may impact underreporting especially amongst male participants. Although sex was not the primary focus of the present study, these findings should be addressed in future research.
The significant role of household income in developing SAD symptoms during adolescence observed in the present sample is consistent with results reported in the literature (Stein et al., 2017). A possible explanation for this might be that poverty might put children at risk for experiencing emotional neglect as it causes increases in stress levels for parents. When parents become overwhelmed under that pressure, they may fail to respond adequately to their child’s emotional needs, and as such, it may be an indirect precipitating factor in the occurrence of SAD symptoms (Slack et al., 2004; Taillieu et al., 2016). These findings illustrate the importance of assessing the roles of household income, early ACEs, and psychopathologies simultaneously in future studies that seek to understand the links between income, emotional neglect, and SAD.
Overall, this study is useful in establishing childhood emotional neglect as a vulnerability factor for SAD symptoms in adolescents. Being able to accurately determine the extent of an early adverse childhood experience on SAD symptoms is an essential task as this can provide the basis for the development of potential screening instruments for preventative and therapeutic interventions. Thus, it may be possible to undertake preventative work with individuals who report high emotional neglect during childhood in order to prevent future relapse.
On the other hand, the results also have limitations. First, the primary limitation of cross-sectional studies is that it establishes associations, but cannot determine causality. Additionally, early childhood adversities were measured retrospectively, which may be affected by the current emotional state, and therefore may have caused overestimation or underestimation compared to prospective measures of experiences. Therefore, future research with a contemporaneous recording of childhood emotional neglect would enable prospective examination of these results.
The current study had many strengths including a suitable sample size, measured adolescent ACEs and attachment styles, and the ability to control for a broad number of important demographic covariates, such as income and maternal and paternal education levels, yet some weaknesses need to be acknowledged. All data were self-reported by the adolescent, and reliance on self-report methods raises the possibility of correlated error and social desirability bias (Krumpal, 2013). In addition, the study’s focus on social anxiety may amplify validity concerns if adolescents with SAD symptoms are more likely to report a particular attachment type. It is unclear, however, whether increased SAD symptoms would lead to over-reporting or underreporting of these attachment types and behaviors. Furthermore, participants with a comorbid disorder diagnosis including major depressive disorder were excluded to reduce the potential confounding influence of depressive disorder in the group of SAD. However, because measures of concurrent depressive symptoms were not collected, the results do not preclude the possibility that low/mild depressive symptoms may influence the aspects of the SAD.
Moreover, we had no exact information about the severity and the duration of early childhood adversities, which may have a differential effect on the risk of developing SAD. Furthermore, our patients reported more frequently emotional neglect by their parents than other types of early maltreatment, and this is consistent with what is reported as the most commonly reported form of early childhood maltreatment (Dubowitz et al., 2004). However, it is also possible that patients’ reporting of emotional neglect in their own childhood may be easier than other types of maltreatment due to social attitudes and beliefs toward sexual or physical abuse in society. Finally, there remains an absence of evidence of the Adolescent Relationship Scales Questionnaire’s psychometric properties among Turkish youth. Although there has been research that established its validity in the Turkish adult population (Sumer & Gungor, 1999), future research is needed to confirm its intended use among youth.
Conclusion
Assessing the type of childhood adversity and attachment styles are critical in understanding psychopathology outcomes in adolescence. The present study extends the previous literature in two ways. First, we examined which types of adverse childhood experiences are uniquely and consistently related to adolescents’ Social Anxiety Disorder. Second, we examined the relationship between different attachment dimensions and Social Anxiety Disorder in adolescents. The main finding of the present study was that social anxiety in adolescence was associated with more self-reported childhood neglect compared to control group. The results suggest that childhood emotional neglect has a unique association with social anxiety symptoms in adolescents beyond what is predicted by attachment styles.
Footnotes
Acknowledgements
We thank the Department of Child and Adolescent Psychiatry of the Istanbul University Faculty of Medicine for their support in the recruitment of patients for the study. We also thank all patients and volunteers for their participation in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclosure
Case group in this study consisted of the subjects included in a graduate thesis entitled “The Relation Between Social Phobia, Adolescent Attachment Styles and Mother’s Attachment Styles”.