
Abstract
The process of communicating a diagnosis of an autism spectrum disorder (ASD) stands out as the first important factor when confronting parents with such a diagnosis for their child. The situation in which a child is diagnosed with ASD is viewed as certainly one of the most stressful moments for parents. Previous research has indicated several factors that affect the positivity of parents’ experiences. Therefore, the aim of the current study was to examine the experiences of parents in the Republic of Croatia concerning the process of communicating a diagnosis of ASD to them and to show the satisfaction level of parents with the characteristics of this procedure. The study involved 52 parents of children who were either suspected of having or diagnosed with ASD. For the purposes of the research, a questionnaire was constructed. The results showed a relatively high degree of parental satisfaction with the process of communicating a diagnosis of ASD. A significant correlation was found between parental satisfaction and the presence of positive characteristics in both the diagnostic process and communicating the diagnosis. However, the results also indicated that there is much room for improvement regarding the conditions and manner of expressing this unwanted news.
Introduction
Communicating a suspicion or diagnosis of autism spectrum disorder (ASD) is an important event that has a long-term impact on the lives of not only children and their parents but also their extended family (Midence & O’neill, 1999). Parents report feeling a wide range of emotions, such as not only shock, anger, guilt, sadness, and loss but also relief during this process (Fleischmann, 2004; Hutton & Caron, 2005). Although such news may have a negative emotional impact on parents in the short term, it is important to be aware that such news still needs to be communicated (Baile et al., 2000); furthermore, there is no dilemma regarding whether to break the news or not, only regarding how to do so (Buckman & Kason, 1992).
A review of the literature points to the importance of the characteristics of the diagnostic process itself as the first factor in the process of coping with such a diagnosis (Buckman & Kason, 1992; Nissenbaum et al., 2002). Although receiving a diagnosis of ASD reduces the level of stigma and allows parents to receive an appropriate level of support (Chamak & Bonniau, 2013), the “invisible” nature of ASD, or the lack of specific physical characteristics of children with ASD, also make it difficult for parents to accept such a diagnosis (Midence & O’neill, 1999).
Parents of children with ASD experience high levels of stress, anxiety, fear, and guilt (Gray, 1994), and communication with professionals is cited as something that further generates stress for these parents (Brogan & Knussen, 2003). A direct diagnosis that contains a sufficient explanation and level of support helps reduce the amount of stress in parents (Osborne & Reed, 2008) and thus may affect their ability to overcome their initial shock and begin to adapt to their child’s diagnosis (Grubić et al., 2013).
It is important to be aware of how the perception of professionals can differ significantly from the perception of parents. Experts often fail to notice that parents’ understanding of the information provided is reduced (Butow et al., 1995); thus, they may fail to anticipate the parents’ needs (Girgis & Sanson-Fisher, 1995). Experts tend to keep some information to themselves or else they do not convey it clearly and understandably enough; they also do not consider that some parents want to know more about the diagnosis itself and the course of the disorder compared to other parents.
The National Collaborating Centre for Mental Health (2011) provides guidance to experts on the process of communicating a diagnosis, such as sufficient time for the entire procedure, including time for questions to be asked, communicating conclusions in person in a mild and supportive but direct manner, pointing to a higher incidence of ASD in siblings, and providing related written material. The way in which information is presented needs to be adapted to parents’ capacity level and their level of understanding (Girgis & Sanson-Fisher, 1995), while using understandable and clear language consisting of as few technical expressions as possible (Baile et al., 2000). It is also recommended to ensure sufficient levels of privacy, reduce the number of distractions and have tissues and the attendance of loved ones available (Baile et al., 2000; Girgis & Sanson-Fisher, 1995). Furthermore, it is desirable that both parents be present at the interview to be able to support each other and to memorize as much information as possible.
The physical environment and a relaxed atmosphere also contribute to a better acceptance of such a diagnosis. Negative experiences of parents are associated with frequent interruptions during the diagnostic process, frequent checking of the clock (Nissenbaum et al., 2002) and the impression that the expert cannot obtain a realistic picture of the child in such a short timeframe (Kerrell, 2001). Additionally, experts often do not point out reasons for their hope and optimism but rather comment on the poor prognosis of a child with ASD (Nissenbaum et al., 2002).
Parents also report that the expert’s way of communicating a diagnosis of ASD affects their ability to cope with such a diagnosis (Chamak et al., 2010). Parents are more satisfied when they have more information about the difficulty itself (Hasnat & Graves, 2000); however, at the same time they may be confused or overwhelmed by the amount of new information they receive, which is why they emphasize the importance of reliable written material, as opposed to receiving unverified information from various sources (Osborne & Reed, 2008). They appreciate the opportunity and a sufficient amount of time to ask questions and the structured and direct approach of experts (Abbott et al., 2012) who communicate information in a way that is understandable and lacking the use of professional terms, as well as experts who respect their opinions and concerns (Brogan & Knussen, 2003). Another important item is that parents also mention the possibility of holding further conversations with the expert, either in person or by phone, to obtain additional information, answers to questions and help in choosing the appropriate support (Nissenbaum et al., 2002).
Parents are also dissatisfied with the long waiting period between the first suspicions of an ASD diagnosis and the final diagnosis (Abbott et al., 2012; Howlin & Moore, 1997); they are also dissatisfied with the fact that children with ASD are diagnosed at a later age compared to children with other developmental difficulties, i.e., mostly between the ages of four and five (Chamak et al., 2010; Goin-Kochel et al., 2006). Thus, they are often faced with long periods of insecurity (Nissenbaum et al., 2002). They state that, on average, they visit four to five different experts before a final diagnosis is made (Siklos & Kerns, 2007).
In conclusion, the relationship that is established between parents and professionals is an important factor in the process of communicating or accepting an ASD diagnosis (Abbott et al., 2012; Hutton & Caron, 2005). Emphasis is placed on a family-oriented approach in which “power” arises precisely from the cooperation of experts and parents. Although parents differ in their speed and degree of adjustment, both good communication and a collaborative relationship with professionals facilitate the adjustment process and reduce stress levels.
The aim of this study was to examine the experiences of parents in the Republic of Croatia in regard to the process of communicating a suspicion or diagnosis of ASD and to determine the level of parental satisfaction with the characteristics of the procedure of experts communicating their suspicion or diagnosis of ASD.
Methods
Participants
The study included 52 parents of children with suspected/diagnosed ASD who volunteered to complete the questionnaire. They were provided with written informed consent. The sample was selected based on two criteria: the chronological age of the child and the time when the child was suspected of having or diagnosed with ASD. Parents of children aged 0–7 years were included in the study, which is a somewhat specific criterion compared to that of other studies that included a wider range of ages (Brogan & Knussen, 2003; Goin-Kochel et al., 2006; Hutton & Caron, 2005). The sample was limited to parents of children who were suspected of having/diagnosed with ASD in the last 18 months, which we believe contributed to the reliability of the parental experience reports. The questionnaire was completed mainly by mothers (96%) and less often by fathers (4%), with an average age of 37.3 years and either a university degree (53.8%) or a secondary education (42.3%).
Measuring instrument
A questionnaire on the experience of parents in the process of communicating an ASD diagnosis was constructed (hereafter called “the questionnaire”), which consisted of the following two parts: (1) Fifteen items that provided general information on the circumstances surrounding the procedure of expressing the suspicion/diagnosis of ASD (for example, the age of the child when the diagnosis of ASD was established); and (2) Twenty-seven items/statements that provided information on the characteristics of the situation, which were divided into the following three areas: (a) spatial and temporal determinants of the procedure; (b) characteristics of the behaviour of experts; and (c) characteristics of the information obtained. The items included in the questionnaire were formed based on an extensive review of the literature in which all important factors that have been shown to influence the parental experience of the diagnostic process and the communication of the diagnosis were highlighted. Participants rated their level of (dis)agreement with the statements on a Likert scale (1 = strongly disagree to 5 = strongly agree).
Finally, on a scale of 1 to 10, parents rated their general satisfaction with the overall procedure (from 1 = extremely dissatisfied to 10 = extremely satisfied) and were given the opportunity to describe their impression after the diagnostic procedure.
Procedure
Parents completed the questionnaire electronically by accessing it on a website. The research was approved by the Ethics Committee of the Faculty of Education and Rehabilitation Sciences, University of Zagreb. Data were collected over a period of 2 months, i.e., from July to September 2020.
The data were collected through an online questionnaire that was developed in Google Forms and then coded and processed using the statistical program IBM SPSS Statistics 25.
Results
General information on the circumstances of the ASD suspicion/diagnosis procedure
The age of the child when the specialist first suspected the child of having/diagnosed with ASD.

M = mean (expressed in months); SD = standard deviation.
The suspicion or diagnosis of ASD was most often communicated to parents by psychologists (28.8%) and educational rehabilitators/special educator teachers (25%) and much less often communicated to parents by speech and language pathologists (13.5%), paediatricians (13.4%) or psychiatrists (7.7%). No more than 6 months (53.4%) or 1 year (76.2%) elapsed between the expression of concern to the expert and the communication of suspicion/diagnosis of ASD to the parents.
Characteristics of the situation in which suspicion/diagnosis of ASD is made.
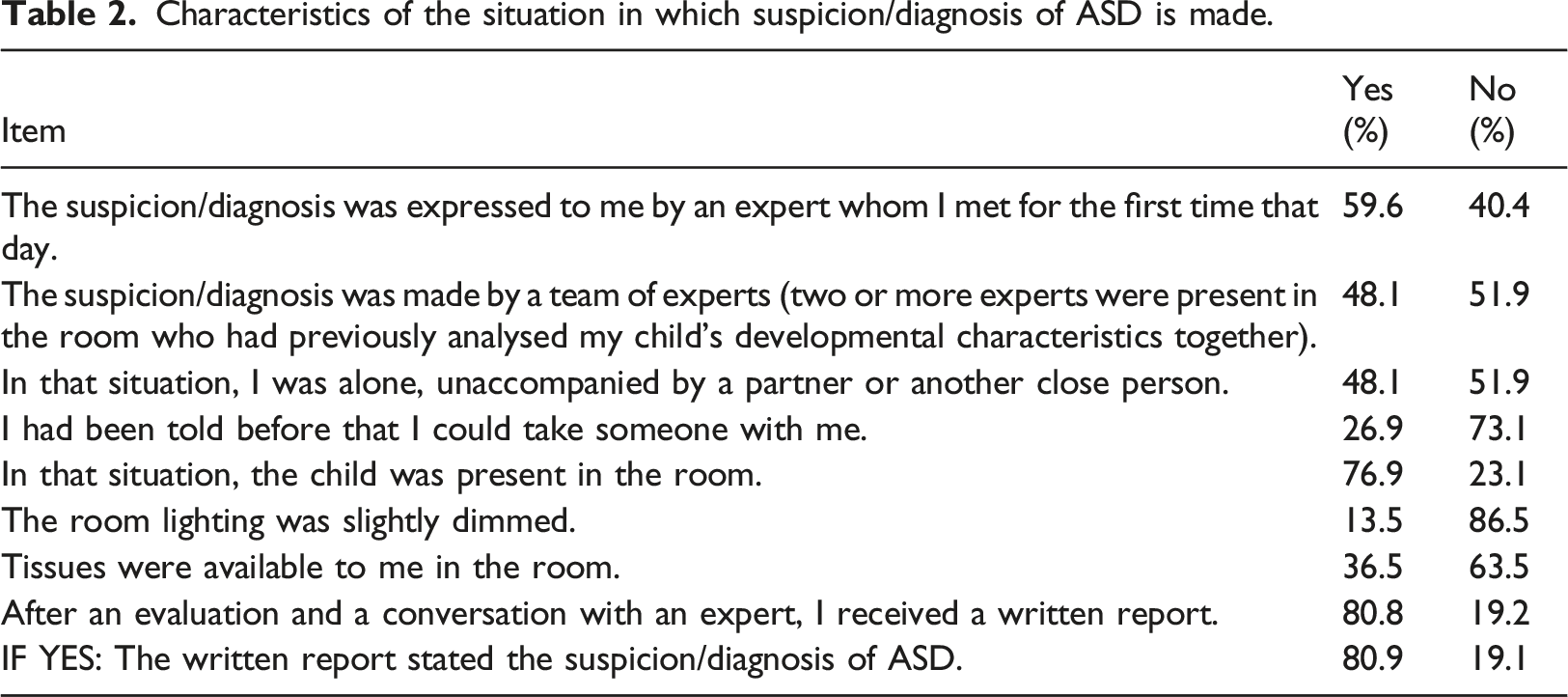
The situation of an ASD diagnosis was mostly described by the parents as a conversation with an expert (not a team of experts) whom they met for the first time that day, as a situation in which they were unaccompanied by a partner (mostly due to not being told they could take someone with them), with a child present in the room at the time of diagnosis, and in a room where tissues were not available nor was the room slightly darkened. Following the assessment, the parents were generally given a written report stating the suspicion or diagnosis of ASD.
Parental assessment of the characteristics of the situation
On a scale of 1 to 5, parents marked their perception of the presence of the factors that are recognized in both the literature and clinical practice as playing a positive role in the process of communicating a suspicion or diagnosis of ASD. A small number of statements (five out of 27) were presented in the questionnaire in such a way that an affirmative answer indicated an undesirable/negative behaviour. This was done to avoid double negations and to make the text of the questionnaire clearer. These items were inverted during data processing so that all items show the presence of a desired behaviour in the same direction. Additionally, these items are marked with an asterisk in the tables that follow.
Space and time characteristics
Spatial and temporal characteristics.
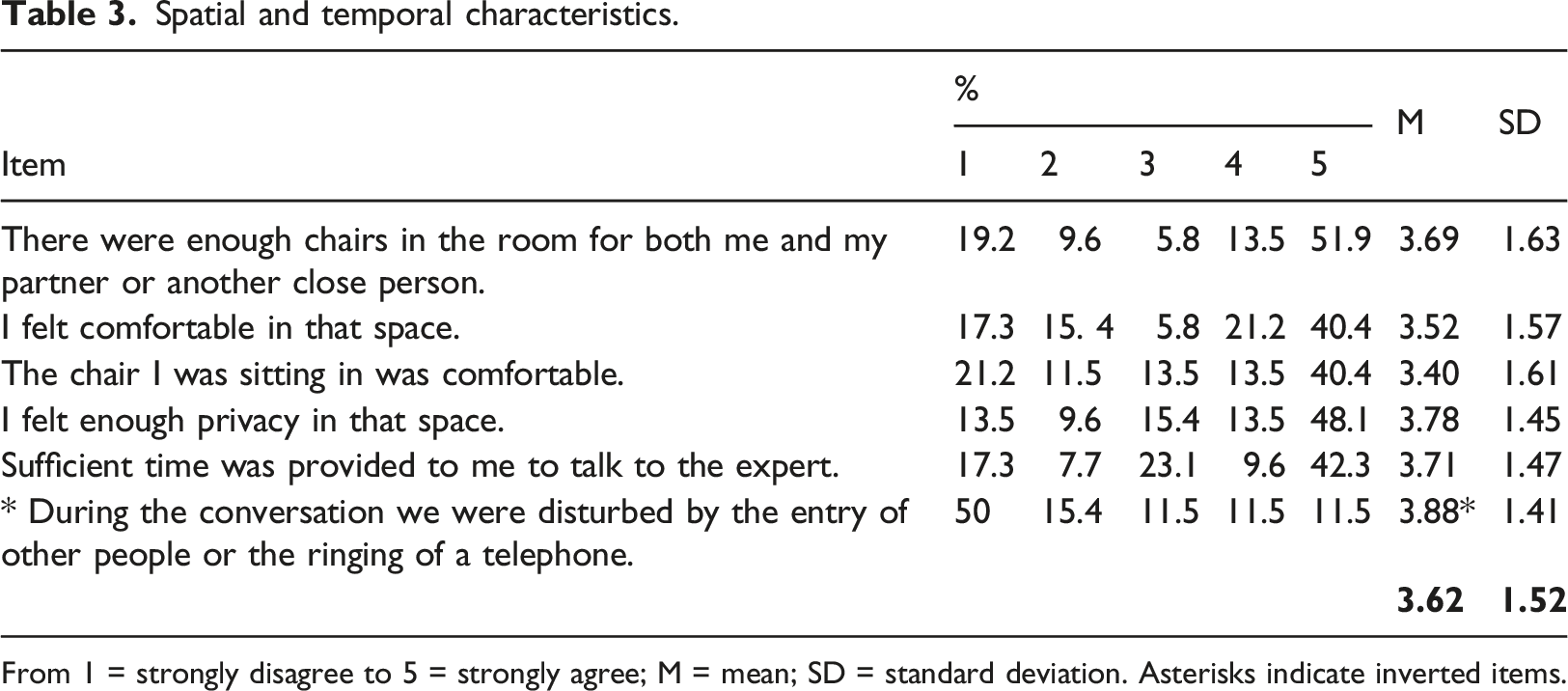
From 1 = strongly disagree to 5 = strongly agree; M = mean; SD = standard deviation. Asterisks indicate inverted items.
Characteristics of experts’ behaviour
Characteristics of verbal and nonverbal communication of professionals.

From 1 = strongly disagree to 5 = strongly agree; M = mean; SD = standard deviation. Asterisks indicate inverted items.
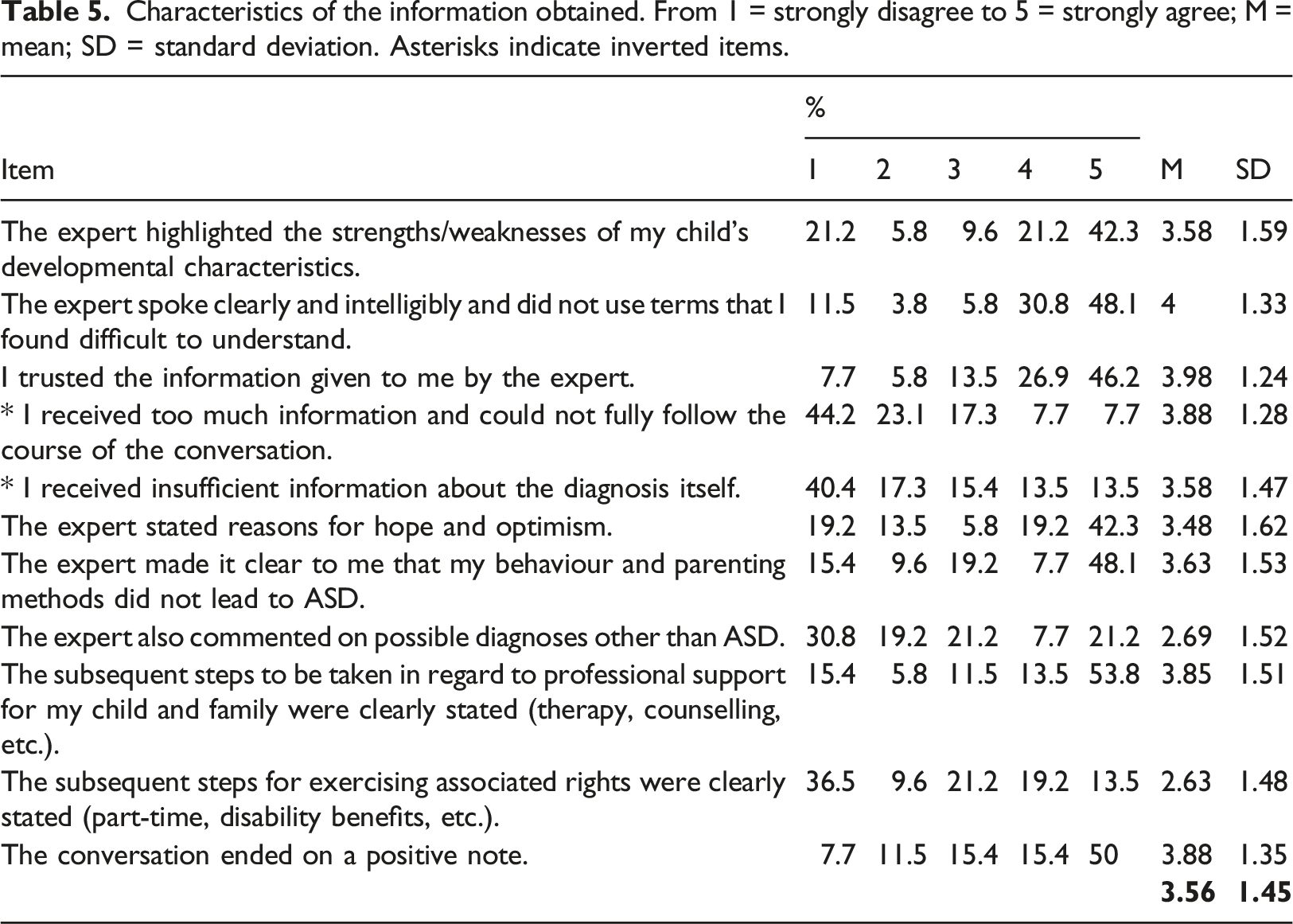
Characteristics of the information obtained
Characteristics of the information obtained. From 1 = strongly disagree to 5 = strongly agree; M = mean; SD = standard deviation. Asterisks indicate inverted items.
Overall parental satisfaction
The results show a relatively high degree of parental satisfaction with the procedure of communicating an ASD diagnosis (M = 7.61 on a scale of 1 to 10; SD = 2.51). As many as 82.6% of the participants expressed their satisfaction by providing a score ranging between 6 and 10, while less than 20% of the participants stated that they were not satisfied with the procedure of communicating a suspicion/diagnosis of ASD.
To determine the correlation of the participants’ overall satisfaction with the characteristics of the procedure (space and time, experts’ communication, information obtained), the Pearson correlation coefficient between these constructs was calculated. The data show that there is a significant correlation between the assessment of overall parental satisfaction and the presence of positive characteristics in all three groups of items, i.e., experts’ communication (r = .437, p < .01), space and time characteristics (r = .479, p < .01), and the information obtained (r = .480, p < .01).
Discussion
Circumstances of ASD suspicion/diagnosis communication
Almost half of the parents (47.7%) reported that the suspicion/diagnosis of ASD was made in the third year of their child’s life, which supports the trend of diagnosing ASD at an earlier age (Goin-Kochel et al., 2006).
In many cases, the suspicion/diagnosis was communicated by an expert whom the parents met on the same day as the report was given (59.6%), which significantly reduced the possibility of the professional recognizing parental strengths and competencies that could be used during the communication of the diagnosis; this situation could have negatively affected the parent’s acceptance of the diagnosis.
Additionally, a considerable number of parents reported that they were alone during this difficult situation (48.1%), and that no one had previously informed them that it was desirable that both parents attend the appointment. It is recommended that experts arrange a date for diagnostic procedures that suit all family members so that anyone who wishes to participate can do so (Austin et al., 2014; Baile et al., 2000).
Many parents (80.8%) reported that they received a written finding, including a written suspicion/diagnosis of ASD. However, one parent stated that the expert did not mention a diagnosis of ASD, while such a diagnosis was written in the report that they received. Given that communicating such a diagnosis is a challenge for both parents and professionals, it is possible that some experts try to avoid reporting unwanted news, as they often feel responsible or even guilty for the unsolicited news that they must communicate (Maynard, 1996).
The data show that tissues were rarely available to parents. Although this detail may seem trivial, the presence of tissues in a visible place in the room is an important element in regard to letting the parents know that it is okay to feel sad and cry (Baile et al., 2000; Girgis & Sanson-Fisher, 1995), which prevents the interruption of the flow of the conversation should the parents become anxious (Nissenbaum et al., 2002).
Often, the child was present when their diagnosis was communicated (76.9%). This situation is usually the case for the objective reason that there is often no other place for the child to be at that time. The presence of younger children can be disruptive to both professionals and parents in communicating the diagnosis. Parents usually need time for themselves to be able to express their emotions without having to worry about what their child is doing at a given moment (Nissenbaum et al., 2002). Therefore, if possible, it is advisable for the experts to arrange a subsequent time to meet with the parents alone without their child being present (Austin et al., 2014). Otherwise, professionals should prepare toys and/or activities to keep the child occupied and consider having a person who is in charge of these activities be present with the child.
Parental assessment of the characteristics of the situation in which the diagnosis is communicated
The diagnostic process is not always carried out under optimal conditions. This is often due to organizational, personnel, financial, technological, spatial and time conditions. However, the data clearly show specific changes that experts can make to improve the process of communicating cases of suspected/diagnosed ASD.
Our data suggest a greater level of positivity regarding the parental experience compared to that found in other studies in which 40% (Goin-Kochel et al., 2006) to 50% of parents (Howlin & Moore, 1997) expressed dissatisfaction with the diagnostic process. The authors of these studies attributed such dissatisfaction largely to the age at which the diagnosis was made, as well as the longer waiting period for such a diagnosis to be made after the parents’ initial expression of concern.
The level of parental satisfaction found in this study largely coincides with the findings of the study by Hasnat and Graves (2000), according to which as many as 82.6% of parents reported a high degree of satisfaction with the process of communicating a diagnosis of ASD. These authors associated this greater level of parental satisfaction with the way in which the professionals communicated with parents, including offering both direct access while respecting parental concerns and a greater amount of information to parents.
Spatial and temporal determinants
The parents’ reported perceptions of the spatial and temporal conditions of such meetings are devastating, as they indicate the very poor spatial and organizational conditions under which such diagnostic procedures often take place, even though these characteristics could be changed without many organizational or financial requirements. Although most parents pointed out positive indicators, many still reported that there were not enough chairs in the room for both partners (28.8%), that the chairs were uncomfortable (32.7%) and that overall, they felt mostly or completely uncomfortable in the space (32.7%). This feeling of discomfort was contributed to further by distracting factors, such as other people entering the room or the ringing of a telephone (23.0%), a short period of allowed time (25.0%) and a lack of privacy (23.1%).
In separate comments, several parents added that the space seemed “cold and sterile”. In clinical practice, “cold and sterile” spaces are desirable in the process of diagnosing young children so that children are focused only on the specific material. However, parents are generally unfamiliar with this information. It should be explained to parents in advance what the diagnostic procedure will look like, including the spatial and temporal characteristics of the environment and the reasons for such an space. Alternatively, experts should consider separating the diagnostic space from the space used to provide feedback. In general, it would be good for the feedback area to be comfortable, slightly dark, and free of distractions.
Behaviour of experts
A diagnosis of ASD leaves parents with many of the following questions: Is it my fault? How do we tell friends/relatives? Will my child have a normal life? Although experts cannot give a clear answer to some of these questions, their manner of communication can contribute to making parents feel supported and empowered (Austin et al., 2014). In addition to the information that professionals provide to parents verbally, they also (often unknowingly) provide a wealth of information through nonverbal communication. Professionals also experience stress when they communicate such a diagnosis (Brand-Gothelf et al., 2021), which suggests that it is important to work on the training of these professionals.
A relatively high percentage of parents reported undesirable traits regarding the way in which professionals communicate. In 30.8% of the cases, the experts were not focused on the interview and spent a large amount of time looking at their files, which may indicate that they were insufficiently prepared for the interview. It is advisable for experts to thoroughly review and prepare in advance all the documentation needed for such interviews, write notes on key information, and determine the order in which the information should be provided (Austin et al., 2014).
Parents highly value directness in regard to communication (Abdelmoktader & Elhamed, 2012); however, beating about the bush is still not uncommon (25%). Parents pointed out that experts often fail to show understanding for their concerns (26.9%), which is related to levels of parental dissatisfaction (Brogan & Knussen, 2003). Parents reported that some experts were either not ready to answer their questions (30.8%) or answered them indirectly (25%). Providing parents with an opportunity to ask questions is a key component of a successful conversation about a child’s diagnosis.
Considering all the above information, certain characteristics of experts have been shown to be insufficiently represented in their communication with parents, which affects whether these parents feel respected, supported and informed or, alternatively, confused, angry, sad or humiliated (Brogan & Knussen, 2003).
Information given to parents
In addition to the way in which experts communicate, the quantity and quality of the information provided is important. Parents who are most anxious about a diagnosis of ASD need to be given more information, and this should be done in a positive, warm, and direct way (Anderberg & South, 2021).
In contrast, the experiences of Croatian parents show that too often the child’s strengths (27%) and the experts’ reasons for having hope and optimism (32.7%) are not highlighted in interviews, which is not in line with numerous guidelines. A poor prognosis is an additional source of stress (Grubić et al., 2013), while optimism motivates parents and encourages them to face the diagnosis and seek appropriate forms of support (Nissenbaum et al., 2002).
Parents reported that they were not always told clearly that neither their behaviour nor their parenting methods led to their child’s diagnosis of ASD (25%). Since parents very often feel guilty for their child’s diagnosis, it is very important to clarify the neurobiological basis of ASD to parents and emphasize that they are in no way responsible for their child’s behaviour or diagnosis (Austin et al., 2014).
Parents’ comments provided on the questionnaire suggest that, in their opinion, experts often “lightly” raise their suspicion or diagnosis of ASD. Thus, it would be advisable for experts to discuss other possible diagnoses with parents, i.e., to list behavioural characteristics that deviate from the targeted diagnosis. In addition, it should also be clearly stated and discussed that a child may have more than one diagnosis (Austin et al., 2014). Diagnosing directly, but with sufficient explanation and support, can help reduce the level of stress experienced by parents (Osborne & Reed, 2008).
A very large percentage of parents reported being dissatisfied with the amount and clarity of the information provided related to their rights (exercise of part-time rights, disability benefits, etc.) (46.1%), which certainly contributes to feelings of helplessness and makes it difficult to plan future steps. Experts should be well acquainted with the “situation on the ground” and have written materials prepared that outline further steps for parents.
Limitations of the research
When interpreting the results of this research, its limitations should be considered. The online survey could not be accessed by those parents who do not have a computer or internet access. For this reason, the experiences of a particular group of parents, i.e., those of a probably lower socioeconomic status or level of education, are not included in the current research.
The sample of participants was collected through organizations in which parents and/or children are involved in some form of support, which suggests that the results may not represent the experiences of families who are not associated with such organizations. It is possible that the group of parents who participated in the research are more satisfied than those parents who are not involved in some form of support or cannot access such organizations. Additionally, it is possible that the questionnaire was completed only by those parents who had a more positive experience with both experts and the diagnostic procedure.
Conclusion
The results of this study show that parents are largely satisfied with the process of communicating the suspicion/diagnosis of ASD. However, at the same time, the careful analysis of the data indicates a significant percentage of parents who noticed several shortcomings in the process. For example, the experiences of parents in the Republic of Croatia show that there is much room for improvement in regard to the conditions and the manner in which this unwanted news is expressed, both in spatial and organizational terms, in terms of communication with parents, and in terms of the quality and quantity of the information provided to parents. The obtained data leave room for experts to think about the changes that they can introduce in regard to their way of communicating their suspicions/diagnoses of ASD in order to achieve greater parental satisfaction and enable parents to more easily accept and cope with such a diagnosis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.