
Abstract
Aim
This study aims to compare changes in rates of suicidal ideation (SI) and attempts (SA) among adolescents during pre, mid and later periods of the pandemic.
Material and Method
This study included adolescents who presented to the adolescent medicine clinic in Turkey between March-May 2019 (prepandemic = T0), March-May 2021(mid period of the pandemic = T1) and March-May 2022 (late period year of the pandemic = T2). SI and SA data were assessed through the electronic hospital records of the “HEEADSSS” inventory.
Results
The charts of 2113 adolescents were evaluated. The rates of both SI (p = .015) and SA (p = .026) were determined to be higher during the pandemic (T1+T2) compared to the pre-pandemic period, with a 1.4-fold increase in SI and a 1.5-fold increase in SA. The rates of SI did not differ according to gender, (p = .090). In contrast, SA rate was significantly higher in females (7.3%) than males (3.6%) (p = .001).
Conclusion
This study reveals an increase in SI and SA among adolescents during the first 2 years of the pandemic. In challenging times, health professionals should prioritize the identification and treatment of mental health issues, including screening for depression and suicide risk.
Introduction
During the coronavirus disease 2019 (COVID-19) pandemic, both the disease itself and the public health measures implemented have had several detrimental effects on the mental health and well-being of adolescents (Pierce et al., 2020). Factors such as social isolation, uncertainty, chronic stress, and economic difficulties have contributed to the onset or exacerbation of psychiatric disorders like depression, anxiety, eating disorders and substance abuse, which all have been associated with suicidal behaviors (Xiong et al., 2020; Çöp et al., 2022). Furthermore, the mental health consequences of COVID-19 are expected to have long-lasting effects, with the peak occurring in the later stages of the pandemic (Sher, 2020).
A systematic review conducted in May 2020, found an increase in symptoms of depression, anxiety and post-traumatic stress disorder during the pandemic, particularly among females, younger individuals, and those with pre-existing psychiatric conditions (Pierce et al., 2020; Xiong et al., 2020). Previous studies have also demonstrated a heightened risk of suicide among individuals who have contracted COVID-19 (Sher, 2020). A questionnaire study conducted in France, including university students in quarantine, revealed an increase in mental health problems with 11.4% reporting suicidal thoughts (Wathelet et al., 2020). Similarly, another study observed an increase in suicidal thoughts of adolescents during the initial phase of the pandemic, particularly during months with significant restrictions (Hill et al., 2021). However, in some of the studies no significant change was observed in psychiatric admissions or suicide rates in the early stages of the pandemic (Davico et al., 2021; Isumi et al., 2020). On the contrary, in another study in Japan, suicide rates showed a slight decrease in the early stages of pandemic but a subsequent increase was observed in the later periods (Tanaka & Okamoto, 2021).
There is limited global evidence linking COVID-19 pandemic to increased suicidal ideation (SI) and suicide attempts (SA) among adolescents and most studies conducted thus far have focused on the early phase of the pandemic. Further research is necessary to elucidate the long-term effects of the pandemic on mental health, especially in different cultural and geographical settings (Chadi et al., 2022; Rogers et al., 2021). Therefore, this study aimed to assess changes due to the pandemic in SI and SA among adolescents in Turkey.
Material and methods
This retrospective study examined adolescents who presented to the adolescent medicine clinic of a tertiary hospital in the pre, mid and late pandemic periods during the same three-months of interval. The clinic offers a comprehensive range of medical services, encompassing primary care as well as specialist treatments, with a particular focus on eating disorders, obesity, substance addiction, adolescent gynecology, chronic illness management, and sports medicine.
The study classified the period between March - May 2019 as the pre-pandemic period (T0), between March - May 2021 as the mid pandemic period (T1) and between March -May 2022 as the late pandemic period (T2). The period between March 2020 and May 2020, which could be defined as the early pandemic period were excluded from the study due to the significantly reduced patient visits resulting from the COVID-19 related restrictions.
On March 11th, 2020, Turkey officially confirmed its first COVID-19 case. The World Health Organization (WHO) proclaimed COVID-19 a pandemic the same day. As of March 16th, all schools and universities in Turkey were closed. Following that, in contrast to all other countries, an age-based lockdown was implemented for all children and young people under the age of 20 (from April 5th to June 11th, 2020) and those over the age of 65 (from March 21st) (Kanbur & Akgül, 2020). Sports complexes, shopping centers, and entertainment venues were also closed. On January 13, 2021, the first vaccination process in Turkey began with the inactive COVID-19 vaccine (CoronaVac®) (Şahin et al., 2023). Flexibility in restrictions began in the country in June 2020. Schools began face-to-face education based on the present number of cases, but shifted to online education if the number of cases increased. Beginning in June 2021, restrictions began to be eased, and by January 2022, all restrictions were lifted; schools opened and in-person education commenced.
Adolescents between the ages of 10–19 years, with a recorded “HEEADSSS” “(Home (home), Education/Employment (Education/Work), Eating (eating attitude), Activities (activity with peers), Drugs (substance use), Sexuality (sexuality), Suicide/depression (suicide and depression), Safety (safety))” psychosocial interview that encompassed SI and SA questioning were included in the study. The HEEADSSS inventory is routinely conducted one-on-one with every adolescent who applies to our clinic, in a confidential environment. In this interview, adolescents are asked questions one by one in accordance with the order in the inventory, and they are directly asked whether they have SI or SA. The answers given after the interview are kept in a password protected patient file so that only the physician following the adolescent can see it.
Adolescents were grouped into three stages of psychosocial development: early adolescence (10–13 years), mid-adolescence (14–17 years), and late adolescence (>17 years) (12). Patient data were retrospectively collected from the hospital electronic medical records system. Those with missing data were excluded. Data was collected from the first visit for all participants and data from revisits were excluded. Variables recorded included date of clinic presentation, age at the initial visit, gender, presence of SI and SA disclosed during the HEEADSSS assessment.
Ethical approval for the study was obtained from the Ethics Committee of Hacettepe University Medical Faculty (decision no: GO 2022/14-51, dated: 20.09.2022).
Statistical analysis
Data were statistically analyzed using IBM SPSS Statistics for Windows, Version 22.0 (Armonk, NY: IBM Corp.). Descriptive analyses of the general characteristics were performed. The conformity of numerical variables to normal distribution was assessed using the Shapiro Wilk goodness of fit test. As numerical variables did not demonstrate a normal distribution, descriptive statistics were stated as the median and the 25th-75th percentile values. The Mann–Whitney U test was applied for comparing two groups of parameters that did not exhibit a normal distribution. Categorical variables were compared using either the Chi-square test or the Friedman test, accordingly. The Binary Logistic Regression analysis was used to determine the effect of age on SI and SA. A p-value of less than .05 was accepted as the level of statistical significance.
Results
A total of 2899 adolescent electronic medical records were reviewed for the study. After exclusion, due to not being in the study age range, missing data and reapplication a final number of 2113 adolescents were included in the study, with 726 in T0, 540 in T1, and 847 in T2. The flow chart presenting the exclusion process is shown in Figure 1. Flow chart of the study.
Changes in descriptive variables and rates of suicidal ideation and attempts in the pre- (T0) and post-pandemic (T1, T2) periods.

SI: suicidal ideation; SA: suicidal attempts.
When the male adolescents were evaluated by year, SI was reported by 9.3% in T0, and insignificantly increased to 12.4% in T1 and 13.7% in T2 (χ2 = 2.4, df = 2, p = .301). SA was reported by 3.4% of the male adolescents in T0, and it was 3.7% in T1 and 3.8% T2 (χ2 = .07, df = 2, p = .965). For female adolescents, the prevalence of SI was 12.5% in T0, which insignificantly increased to 17.4% in T1 and 14.7% in T2 (χ2 = 4.9, df = 2, p = .084). In terms of SA, the prevalence was 5.1% in T0, 8.2% in T1 and 8.6% in T2 (χ2 = 5.26, df = 2, p = .072).
Change in suicidal ideation and attempt rates according to adolescence stages and years.
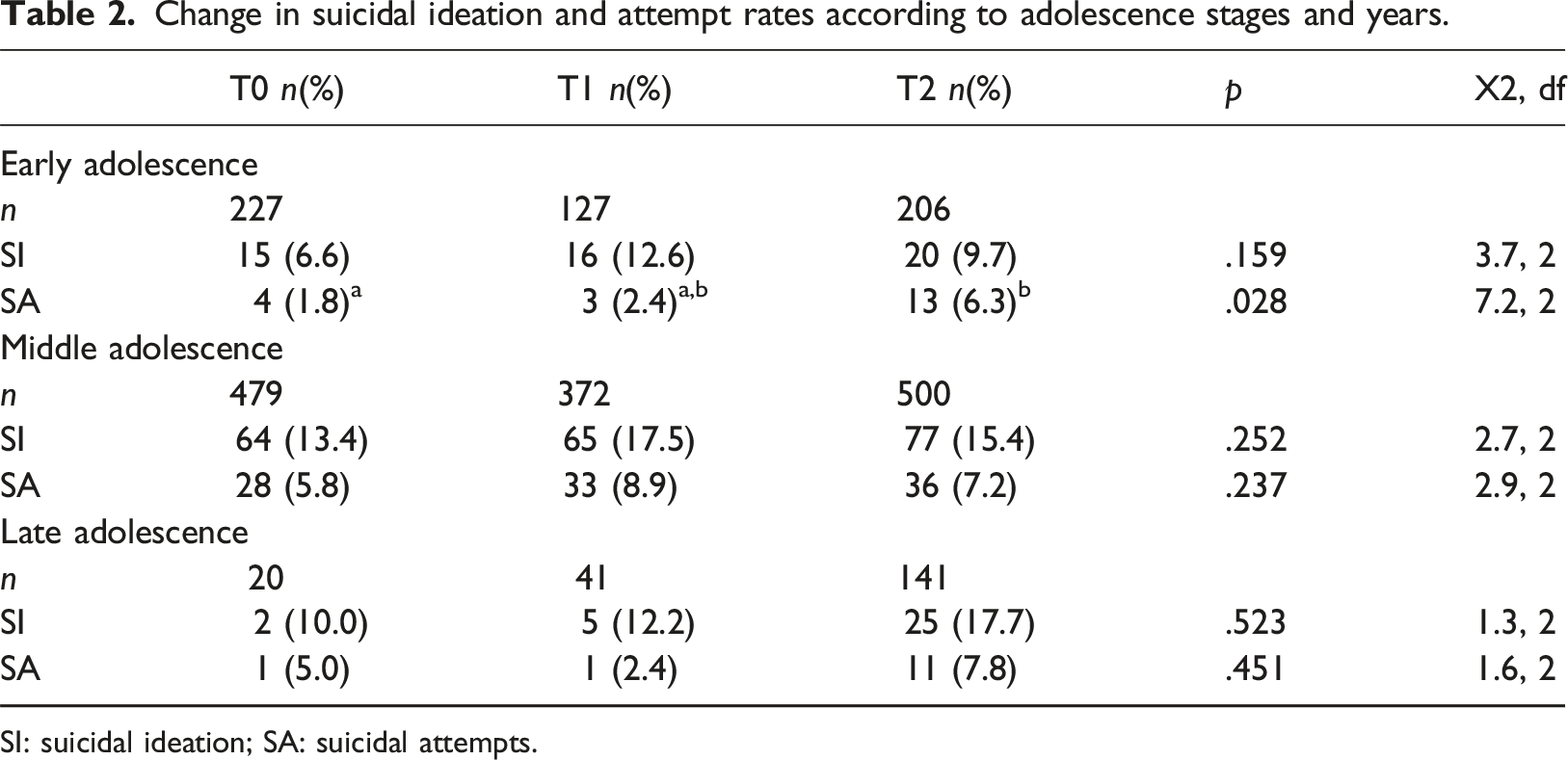
SI: suicidal ideation; SA: suicidal attempts.
Discussion
The aim of this study was to determine the change in SI and SA during the COVID-19 pandemic in adolescents presenting at a tertiary health center in Turkey. The study findings revealed a significant increase in the prevalence of SI and SA during the pandemic compared to the corresponding pre-pandemic period. However, no significant change was observed between the mid and late periods of the pandemic. Furthermore, the rate of SA among early adolescents increased during the pandemic, while no significant difference was observed among middle and late adolescents.
Suicide is the second most common cause of death in the 15–19 years age group, with approximately 80% of suicides occurring in low-income countries (World Health Organization, 2020). The COVID-19 pandemic has had an additional detrimental impact on mental health, particularly among adolescents. The increase in SI and SA prevalence may have been caused by various mental health issues triggered by the implementation of safeguard measures such as social isolation and school closures to curb the spread of the virus, limited access to mental health services, reduced physical activity, heightened social and economic concerns, and family conflicts (Chadi et al., 2022; Meherali et al., 2021; Que et al., 2020).
It is also critical to recognize that mental health problems are not the only risk factors for SI and SA. Stressful life circumstances can also serve as a trigger (Howarth et al., 2020). COVID-19 caused rapid changes in the living conditions of youth. The quarantine measures described above disrupted their routines, led to loneliness and caused peer isolation (Ezpeleta et al., 2020). Similarly, parents may have been compelled to find new options for child care or quit their jobs, resulting in economic hardships. These COVID-related stressors may have led to family conflicts and weakened positive relationships (He et al., 2022; Patrick et al., 2020), thereby contributing to the observed increase in adolescent SI and SA rates.
During adolescence, significant physical, emotional, and mental changes occur. During this time, a healthy growth and development should be prioritized. Despite the fact that a majority of adolescents are physically very healthy, engaging in risky behaviors during this period can have lifelong repercussions and cause morbidity and mortality. Due to these factors, adolescents have unique health and psychosocial needs that must be addressed at each hospital visit; however, this should be done directly with the adolescent, as opposed to through the parents as in pediatric practice. (Doukrou & Segal, 2018). The HEEADSSS system review is a fast, practical and safe tool that can be utilized by healthcare professionals to assess risk-taking behaviors in order to comprehend adolescent behavior and provide the appropriate interventions. Also, using the HEEADSSS system review is an effective way to engage with young people and address the many challenges this age group faces. It is essential that young people speak freely about their true concerns and clearly understand their needs. When the standard of routine psychosocial history taking is established, it becomes easier for health professionals to build bridges with this large group of patients and help protect them from preventable causes of death and illness (Kanbur, 2016; Rome & Strandjord, 2016; Smith & McGuinness, 2017)
A study by (Thompson et al., 2021) revealed an increase in SI and SA among hospitalized adolescents during the pandemic, whereas (Hawton et al., 2021), found a significant decrease in hospital presentations for self-harm in the 3 months following the implementation of confinement restrictions. Additionally, while some studies have shown increased rates of SA in both developed and developing regions, some have reported no change in high-income societies with robust mental health support services (Mamun et al., 2021; Manzar et al., 2021; Pirkis et al., 2021).
In line with the literature we found, a significant increase in the rates of SI and SA during the pandemic compared to the pre-pandemic period in Turkey which is a middle-low income country (Pirkis et al., 2021). It appears that COVID-19 has had a more severe impact on mental health in economically disadvantaged developing countries (Kola et al., 2021). Time trend regression model studies during the pandemic also indicate that an increase in economic hardship leads to higher suicide rates (McIntyre & Lee, 2020). In developing countries, the effects of unemployment, income loss, reduced social support, and disrupted education are more pronounced compared to developed countries. Additionally, there has been a significant decrease in the utilization of healthcare services which may all explain our results (Kola et al., 2021).
Although research has been conducted on the mental health effects of pandemics, the majority of studies have primarily focused on the early pandemic period, and little is known about the long-term effects of the pandemic on adolescents’ mental health. Despite some restrictions being lifted in the later stages of the pandemic such as the school closures, and the partial alleviation of the disease’s impact, the pandemic continued to disrupt daily routines. Additionally, previous research has shown higher rates of SI and SA among adolescents in school settings often because of peer bullying, exam pressure, and academic concerns (Lathabhavan & Griffiths, 2020). Therefore, the prevalence of SA and SI might increase in the later stages of the pandemic due to pandemic and school related stress. A study conducted in Japan reported that suicide rates did not increase in the early stage of the pandemic when schools were closed, but an increase was observed after schools reopened (Isumi et al., 2020). In contrast in our study no difference was observed between the mid and later pandemic periods. The reasons could be attributed to several factors, such as increased access to healthcare services, the rise in social support and reduced isolation, reopening of schools and face-to-face teaching leading to enhanced peer relationships, increased resilience and more effective coping strategies, the opportunity of physical activity, and a decreased fear of being infected with COVID-19 in the later stages of the pandemic (Samji et al., 2022; van Harmelen et al., 2017).
In our study, we observed that the prevalence of SA in the early adolescent period significantly increased during the later stages of the pandemic. During early adolescence, conflicts between adolescents and their parents tend to intensify, and the adolescents may exhibit more defiance towards authority (Sanders, 2013). Moreover, friendships play a significant role during this period. The pandemic might have had a more detrimental mental health impact on early adolescence, potentially due to the heightened vulnerability of this age group to the effects of social restrictions, which hindered peer relationships and led to increased family conflicts during extended periods spent together (Berndt, 1982)
Previous research has indicated a correlation between increasing age and elevated mental health issues (Ademhan Tural et al., 2020; Fitzpatrick et al., 2021). We also demonstrated that the risk of SA increased 1.2-fold and the risk of SI increased 1.15 fold, as age increases.
A majority of studies have reported significantly higher SI and SA among female adolescents compared to males (Gracia et al., 2021; Halldorsdottir et al., 2021; Yard et al., 2021). Although we did not find a gender difference in terms of SI, the prevalence of SA was higher in female adolescents, consistent with the literature. Moreover, although not significant, the increase in the SA and SI rates of female adolescents during the pandemic was more pronounced than males. Studies indicate that mental health problems during pandemic have had a more pronounced impact on women compared to men and that women need more mental health support in challenging periods (Liu et al., 2020; Rose & Rudolph, 2006). This can be attributed to various factors. Young girls and women often encounter significant challenges and inequalities, which have been further exacerbated by the impact of the pandemic. The prolonged periods spent at home with family members have exposed them to an increased risk of domestic and intimate partner violence and abuse. Moreover, the heightened vulnerability of women to economic difficulties has contributed to their mental health struggles. Lastly, the closure of schools and subsequent disruption of education have disproportionately affected women (Liu et al., 2020; Pirkis et al., 2021; Rose & Rudolph, 2006; van Harmelen et al., 2017; Yard et al., 2021).
Strengths and limitations of the study
This study had several limitations, including its retrospective design and reliance on direct questioning of adolescents regarding SI and SA. It is possible that some information was not disclosed and therefore could not be obtained from the records. Additionally, the study did not explore the underlying causes of suicidal thoughts or their potential relationship to the COVID-19 pandemic. In addition, SA methods and additional psychiatric comorbidities of adolescents such as depression, anxiety and post-traumatic stress disorder were not evaluated. As the study population was drawn from a tertiary institution, the results may not be generalizable to the general population, as this cohort may have contained a higher proportion of adolescents with chronic disorders. Furthermore, we were unable to examine the early pandemic period due to a decline in patient admissions caused by COVID-19 restrictions. However, despite these limitations, this study is valuable as a study with a relatively large sample to compare the prevalence of SA and SI in a developing country before, during, and after the pandemic.
Conclusion
The findings of this study demonstrating a significant increase in both SI and SA during the pandemic, highlight the negative impact of the pandemic on the mental health of adolescents, residing in a middle-income country. The presence of stressors related to COVID-19 in several areas of life, such as financial difficulties and instability in the home environment, may have also been linked to an increased risk of SI and SA. Particularly females and those in the early adolescent period were found to be more vulnerable to the mental effects of the pandemic. Healthcare professionals caring for adolescents, should prioritize the identification and support of mental health issues, including depression and suicide risk, during challenging times. Comprehensive interventions that encompass accurate information dissemination, mental health support, and stress management strategies are crucial to address the long-lasting consequences of the pandemic on the mental wellbeing of adolescents. Further research is needed to better understand the underlying factors and develop effective preventive measures to safeguard the mental health of this vulnerable population in future crises.
Footnotes
Author contributions
Şeyma Erdem Torun: Literature scan, data collection, writing the manuscript, interpretation of results. Melis Pehlivantürk Kızılkan: Literature scan, Data analysis, writing the manuscript, interpretation of results. Sinem Akgül: Study design, writing the manuscript, literature scan, interpretation of results. Orhan Derman: Literature scan, writing the manuscript, interpretation of results.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.