
Abstract
Functional neurological symptom disorders (FNSD) pose a common challenge in clinical practice, particularly in pediatric cases where the clinical phenotypes can be intricate and easily confused with structural disturbances. The frequent coexistence of FNSDs with other medical disorders often results in misdiagnosis. In this review, we highlight the distinctions between FNSD and various psychiatric and neurological conditions. Contrary to the misconception that FNSD is a diagnosis of exclusion, we underscore its nature as a diagnosis of inclusion, contingent upon recognizing specific clinical features. However, our focus is on a critical learning point illustrated by the case of a 14-year-old male initially diagnosed with FNSD, but subsequently found to have a rare primary monogenic movement disorder (paroxysmal kinesigenic dyskinesia, PKD). The crucial takeaway from this case is the importance of avoiding an FNSD diagnosis based solely on psychiatric comorbidity and suppressible symptoms. Instead, clinicians should diligently assess for specific features indicative of FNSD, which were absent in this case. This emphasizes the importance of making a diagnosis of inclusion. Extended follow-up and clinical-oriented genetic testing might help identify comorbidities, prevent misdiagnosis, and guide interventions in complex cases, which cannot be simply classified as “functional” solely because other conditions can be excluded.
Plain language summary
Understanding and Avoiding Mistakes in Diagnosing Children with Functional Neurological Symptom Disorders: A Review and Case Report: This article discusses Functional Neurological Symptom Disorders (FNSDs), focusing on misdiagnosis, differential diagnosis, and other diagnostic challenges, particularly in pediatric cases. FNSDs involve motor or sensory symptoms that are inconsistent over time and unexplained by neurological disease, often associated with psychosocial factors. The article highlights the complexity of distinguishing FNSDs from other neurological and psychiatric conditions, emphasizing the importance of careful evaluation. The authors review various conditions that can mimic FNSDs, such as epileptic seizures, syncope, and different motor disorders. They emphasize the need to consider psychiatric conditions in the differential diagnosis, including factitious disorders, and malingering. The article presents a case study of a 14-year-old with involuntary movements, initially diagnosed as having a Functional Movement Disorder. After careful evaluation, the patient was diagnosed with a genetic dystonia (PRRT2 mutation). The case shows the importance of not rely solely on psychological problems, bizarre presentations or suppressible symptoms when diagnosing FNSDs.
Keywords
Introduction
Functional Neurological Symptom Disorders (FNSDs), as defined in DSM-5 TR (and previously known as conversion disorder) (American Psychiatric Association, 2022), encompass variable and common conditions including Functional Seizures (FS), also known as psychogenic non-epileptic seizures, and Functional Motor Disorders (FMDs), but also chronic dizziness and cognitive dysfunction (Hallett et al., 2022). FNSDs are commonly associated in clinical practice with psychosocial and psychiatric comorbidities, disability, and relevant health costs. (Kozlowska et al., 2007) Despite involving all ages, a high prevalence of FNSD has been reported in young females (Yong et al., 2023).
Functional Neurological Symptom Disorders (FNSDs) mainly refer to incongruent and time-inconsistent motor or sensory symptoms, that are unexplained by neurological disease and caused by altered brain networking, rather than structural abnormalities. However, the pathophysiological processes are still largely unknown (Hallett et al., 2022).
Functional dystonia was the first FNSD described with specific diagnostic criteria (Fahn & Williams, 1988), later adapted by other authors for other FNSDs as well (Ganos et al., 2014; Gupta & Lang, 2009; LaFrance et al., 2013). However, neurological signs and symptoms in children are often complex, thereby challenging classical diagnostic criteria for FNSDs. In this regard, a recent systematic review found significant variability and low reproducibility of diagnostic criteria for paediatric FMDs (Kirkwood & Mark, 2022).
Furthermore, it has also been outlined that some patients with presumed functional symptoms revealed unexpected non-functional diagnoses during follow-up (Stone et al., 2009). These conditions are often rare and genetically based disorders, usually detected by the increasing use of genetic testing tools.
Finally, as frequently occurs for FS and epileptic manifestation, functional and neurological motor symptoms may coexist in some patients, making the differential diagnosis even more challenging for clinicians (Hallett et al., 2022; Kurtis & Pareés, 2021).
Here we present a brief review of available literature regarding misdiagnosis, differential diagnosis, and other diagnostic issues involving FNSDs, particularly in paediatric age. We then propose a relevant case of a young patient with a rare monogenic neurological disorder, previously supposed as FMD and mistreated over 10 years, highlighting the importance of careful evaluation and prolonged follow-up.
Functional neurological symptom disorder mimics
Functional Neurological Symptom Disorders (FNSDs) are a complex and multifaceted group of conditions that have been the subject of extensive scientific interest in recent years.
While some might assume that FNSDs are frequently misdiagnosed due to the absence of specific instrumental or laboratory findings, this is not necessarily the case. Some authors (Stone et al., 2009) conducted a prospective cohort study involving 1444 patients referred from primary care to neurology clinics. They found that only 0.4% of these patients had an unexpected structural non-functional diagnosis that could explain their initial symptoms at follow-up. Similarly, other authors (Walzl et al., 2019) observed that a comparable percentage of patients initially diagnosed with a structural neurological disease were later identified as having a functional diagnosis that better explained their symptoms. As shown by a previous systematic review and metanalysis (Stone et al., 2005), the relatively low rate of misdiagnosis of functional symptoms since 1970s (similar to other neurological or psychiatric conditions) could be due to improved diagnostic accuracy or better study methods.
However, van der Salm et al. (van der Salm et al., 2013) highlighted that even experienced movement disorder specialists sometimes disagree on the clinical diagnosis of FS. Furthermore, there are documented instances of misdiagnosis related to FNSD (van der Feltz-Cornelis et al., 2020) that suggest the hypothesis that the actual number of diagnostic errors might be underestimated.
In particular, misdiagnosis of FNSD has become a growing concern within emergency rooms, inpatient or outpatient units, and other clinical contexts (Yong et al., 2023). Despite the recent attention to FNSD and the development of clear diagnostic criteria, there is still a significant challenge in diagnosing these disorders due to their resemblance to other medical conditions. This risk of misdiagnosis is particularly concerning in paediatric populations. Therefore, it is important to approach these cases with caution and to consider the possibility of either missing an FNSD diagnosis or misdiagnosing another neurologic disorder as FNSD.
There are specific conditions that are more at risk of being misdiagnosed. These include disorders that have no specific signs and those whose specific clinical signs are difficult to obtain. For example, in some cases, specific tools or skills may be required, including genetic analysis or neuroimaging techniques. Furthermore, there may be conditions where the signs are ambiguous or unknown to the clinician, therefore differentiating functional presentations from traditional neurological diseases necessitates a diagnostician’s ability to identify the subtle distinctions between them.
FNSD and psychiatric differential diagnoses
When considering the differential diagnosis of FNSD is crucial to take into account not only other neurological disorders but also other psychiatric or behavioral conditions.
With regard to the latter, the most important distinction to make is between functional disorder, factitious disorder, and simulation or malingering. The distinction between the three conditions is significant as it may determine further workup and treatment (Bass & Halligan, 2016). In this context, another condition, not explored in detail here, is Factitious Disorder Imposed on Another (FDIA), where, for instance, a caregiver actively produces factitious symptoms in a child. However, in FDIA, the diagnosis is potentially assigned to the caregiver rather than the minor, and the diagnostic-therapeutic path differs significantly from the other conditions we are about to discuss (Walters et al., 2019).
Differential Diagnosis Between Functional Neurological Symptom Disorder, Factitious Disorder, and Malingering.

Despite the clear theoretical distinction between these conditions, it should be noted that differentiating among them in children and adolescents can be difficult (Kozlowska, 2014). This is particularly true from a semeiological standpoint, where functional and simulated movement disorders can be impossible to differentiate, even if several functional magnetic resonance imaging (fMRI) studies have shown differences in regions of activation (Hassa et al., 2016; Perez et al., 2021). Additionally, an accurate psychosocial history must be taken when evaluating these conditions, as both functional and factitious disorders often have experienced traumatic adverse events in childhood (Hausteiner-Wiehle & Hungerer, 2020; Peebles et al., 2005; Steffen-Klatt et al., 2019).
Moreover, as it has been pointed out (Kozlowska, 2014), distinguishing between volitional and non-volitional processes is already a challenge in adults, let alone in children and adolescents. The adaptive use of dissimulation and deception can develop very early before explicit cognitive processes arise, which makes differential diagnosis even more complex. These difficulties probably contribute to relatively low rates of factitious disorders in neurology settings (Kanaan, 2022; Kanaan & Wessely, 2010). For this reason, it is essential to involve different specialists in the assessment of children and adolescents with neurological symptoms, given that the interaction between biological, psychological, and social factors should always be considered (Hallett et al., 2022; Onofrj et al., 2023).
Differential diagnoses of Functional Seizures
Main diagnostic characteristics used to differentiate functional seizures (FS) from two other common paroxysmal events (Epileptic seizures and syncope).
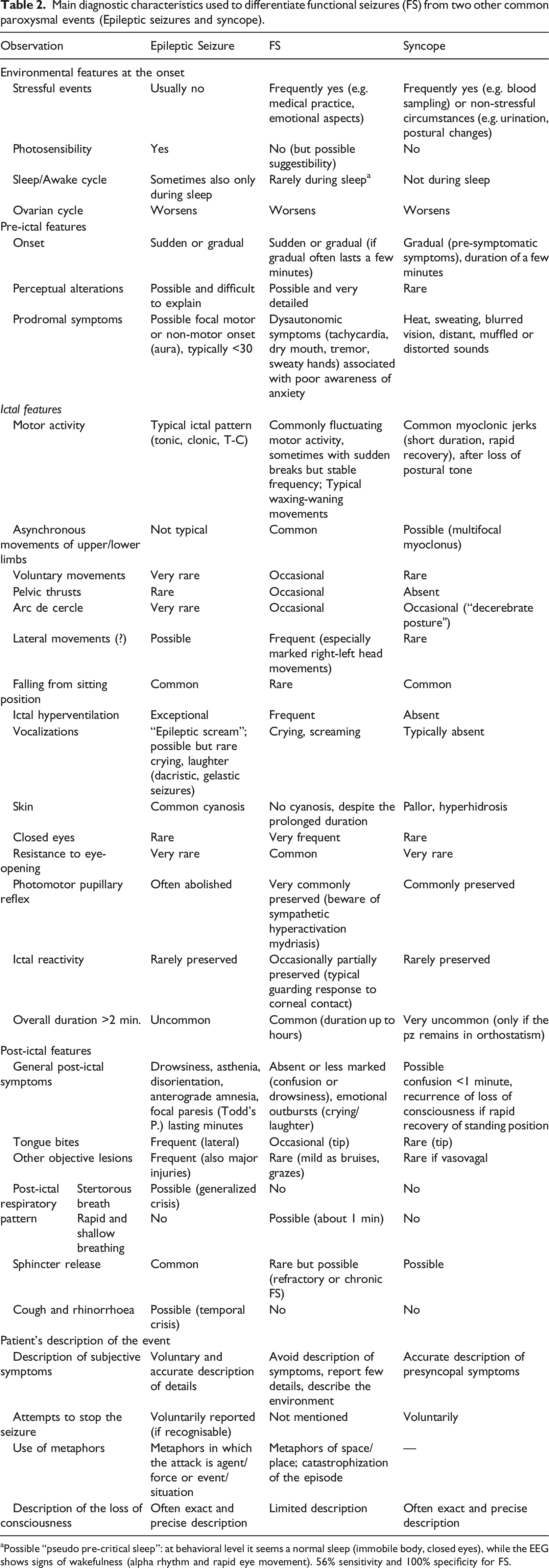
aPossible “pseudo pre-critical sleep”: at behavioral level it seems a normal sleep (immobile body, closed eyes), while the EEG shows signs of wakefulness (alpha rhythm and rapid eye movement). 56% sensitivity and 100% specificity for FS.
Differential diagnoses of functional motor disorders
While there is extensive literature discussing FNSD with seizure presentations and their mimics, there is a relative paucity of literature on mimics of FNSD with motor presentations or FMD.
Reports of misdiagnosis of FMD as other disorders include multiple sclerosis (Walzl et al., 2022), stroke (Gibson & Whiteley, 2013; Jones et al., 2020; Popkirov et al., 2020; Sequeira et al., 2018), myelopathy (Ginsberg, 2017; Teasell & Shapiro, 2002), myasthenia gravis (Harrison et al., 2023), serotonin syndrome (Nisbet & Penfil, 2008), autoimmune encephalitis (Flanagan et al., 2023; Wilkinson-Smith et al., 2020), sarcoma-induced osteomalacia, cerebellar medulloblastoma, Huntington’s chorea, dystonia (Teasell & Shapiro, 2002), astasia-abasia (Stanković et al., 2015), paresis/paralysis (Gelauff et al., 2019).
On the other hand, reports of misdiagnosis of other neurological disorders as FMD include the following: prionic disorders (Gómez-Mayordomo et al., 2023; Jiang et al., 2019), dystonia (Erro et al., 2014; Yilmaz et al., 2011), Kleine-Levin syndrome (Masi et al., 2000), acute disseminated encephalomyelitis (Abay et al., 2005), paresis/paralysis (Fishbain & Goldberg, 1991), Guillain-Barrè syndrome (Edelsohn, 1982; Wherry et al., 1991), progressive supranuclear palsy (van Meerkerk-Aanen et al., 2017), spinal cord arteriovenous malformation (Spratt & Thomas, 2008).
Furthermore, with specific regard to neurodevelopmental age, there has been recent interest in functional stereotypies and tic-like disorders (Forsyth, 2021; Martino et al., 2023; Pringsheim et al., 2023).
This brief synopsis underscores the importance of thorough differential diagnosis and the potential pitfalls in diagnosing FMD.
Moreover, the most recent systematic review on criteria for diagnosing FMDs (Kirkwood & Mark, 2022) has highlighted that such criteria must refrain from employing subjective and unscientific language, such as “bizarre” and “unusual”, and avoid labeling symptoms as being incongruent with other neurological conditions. On the contrary, FMDs should be diagnosed through the detection of specific clinical positive signs.
Some relevant bedside clinical signs to diagnose functional movement disorders (FMDs) adapted from Aybek and Perez (2022). Specificity, sensibility, and specific reference for each sign are reported as well.
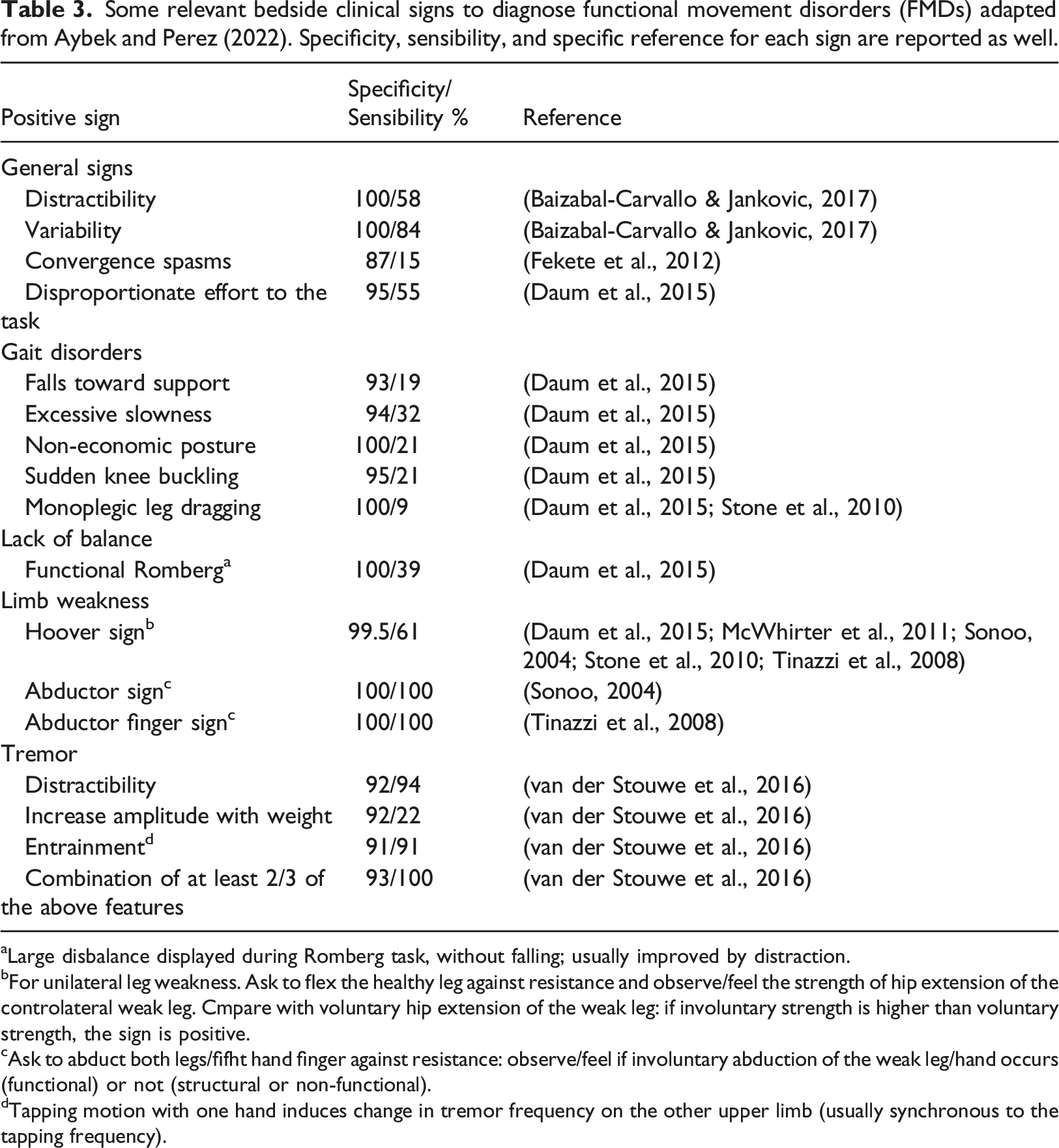
aLarge disbalance displayed during Romberg task, without falling; usually improved by distraction.
bFor unilateral leg weakness. Ask to flex the healthy leg against resistance and observe/feel the strength of hip extension of the controlateral weak leg. Cmpare with voluntary hip extension of the weak leg: if involuntary strength is higher than voluntary strength, the sign is positive.
cAsk to abduct both legs/fifht hand finger against resistance: observe/feel if involuntary abduction of the weak leg/hand occurs (functional) or not (structural or non-functional).
dTapping motion with one hand induces change in tremor frequency on the other upper limb (usually synchronous to the tapping frequency).
FNSD comorbidities
Building on the diagnostic complexities of FNSDs, it is crucial to consider that the DSM-5-TR’s Criterion C, which states that “the symptom or deficit is not better explained by another medical or mental (health) disorder”, should not be misconstrued. It does not imply that a patient cannot simultaneously have FNSD and other coexisting neurological or psychiatric conditions. Understanding FNSD comorbidities is vital for a comprehensive differential diagnosis.
For instance, recently, a group of authors (Carle-Toulemonde et al., 2023) provided a narrative review that highlighted several comorbidities associated with FNSD, including fatigue, cognitive symptoms, and psychiatric disorders (ranging from 40% to 100% of FNSD patients, with anxiety disorders being the most common). The presence of non-functional disorders, including neurological conditions like epilepsy in patients with FS (20%) and FMD in Parkinson’s disease (7%), was also noteworthy. Furthermore, somatic symptom disorders and hypermobile Ehlers-Danlos Syndrome were also frequently linked to FNSD, with a prevalence of about 50% each.
Case report
We report the case of a 14-year-old male born to healthy non-consanguineous parents. Their family history was unremarkable. Delivery and neonatal period were uneventful. Motor milestones were on time, while a mild language delay was reported. The first involuntary movements arose at the age of 5 years, diagnosed as stereotyped movements, mainly involving the right lower limb (LL) but also the right upper limb (UL). At the age of 8, he underwent his first hospitalization due to further involuntary movements, clinically characterized by progressive involvement of LLs and trunk with an axial twisting, till opisthotonus, sometimes associated with fallings, without loss of consciousness. These episodes were usually triggered by excitement, anxiety, or stress, typically lasting less than 1 minute and occurring 3-4 times a day. The boy reported that each episode was preceded by a physical sensation and urge, suppressible only for a little time. Physical and neurological examinations revealed only mild motor coordination difficulties.
A normal neurocognitive profile was found, while at the psychopathological evaluation, a social anxiety disorder was revealed. Laboratory tests and electroencephalograms were unremarkable.
At the age of 10 years, he was diagnosed with FMD, because of the bizarre clinical presentation, characterized by involuntary movements, partly suppressible, linked with emotional triggers, and for the related psychopathological features. Thus, cognitive behavioral therapy was suggested and administered for over 3 years.
At the age of 13, he was admitted to our Paediatric Movement Disorders (MD) Unit, because of the recurrence of twisting-like movements, which also involved progressively the ULs. The frequency was 3-4 times per week, mainly during school activities. The patient also described recurrent headaches and increasing social and school anxiety with panic attacks due to his motor disorder, and a consequent significant daily life impairment. Furthermore, the constant oversight of caregivers also caused a severe limitation in his personal autonomy.
According to the anamnesis and the clinical evaluation he presented a characteristic involvement of the right part of the body, with a following caudo-rostral progression. Moreover, during the paroxysmal episodes, the motor manifestations were not stoppable or modulated by distractible maneuvers; in subsequent evaluations, no signs of inconsistency were found.
Prolonged clinical observation and home video analysis also revealed that episodes of involuntary movement attacks were triggered by sudden voluntary movements.
In the suspect of paroxysmal kinesigenic dyskinesia, a Next Generation Sequencing (NGS) panel for genetic MDs was carried out, revealing a de novo heterozygous pathogenic variant in the PRRT2 gene (c.649delC; p.Arg217fs*12), compatible with the diagnosis of genetic dystonia type 10 (DYT-10).
Mutation of the proline-rich transmembrane protein 2 (PRRT2) gene has been widely studied as a causative gene of paroxysmal kinesigenic dyskinesia and clinical data showed an effective response to very low doses of carbamazepine (Ebrahimi-Fakhari et al., 1993; Méneret et al., 2012).
Consequently, carbamazepine was titrated up to 100 mg/day, with a dramatic improvement of the symptomatology, presenting after the first week of pharmacological treatment a complete remission of symptoms. He still reports the sporadic presence of premonitory urges without consequent motor manifestations.
Discussion
The presented case highlights the challenging differential diagnosis between structural and functional motor disorders, often due to atypical presentations and overlapping features occurring in paediatric neurology, as discussed above. Non-specific and complex clinical pictures at onset may result in misdiagnosis and subsequent errors up to adulthood (Ganos et al., 2014). In our patient, red flags for non-functional MD, such as the early onset of motor symptoms and their stereotyped phenomenology, emerged after repeated evaluations, leading to a revision of the diagnosis. As it is known, clinical onset of FMD is commonly reported in early adolescence, but rarely in childhood. Furthermore, the motor symptoms are mainly inconsistent over time, presenting high clinical variability with respect to motor patterns and triggers, differently from our case. The duration of the episodes was also evaluated, revealing that all attacks typically lasted less than 1 minute in our patient. FMDs, on the contrary, usually show higher variability in the duration of episodes in the same patient (e.g. between seconds and hours/days) (Gupta & Lang, 2009; Yong et al., 2023).
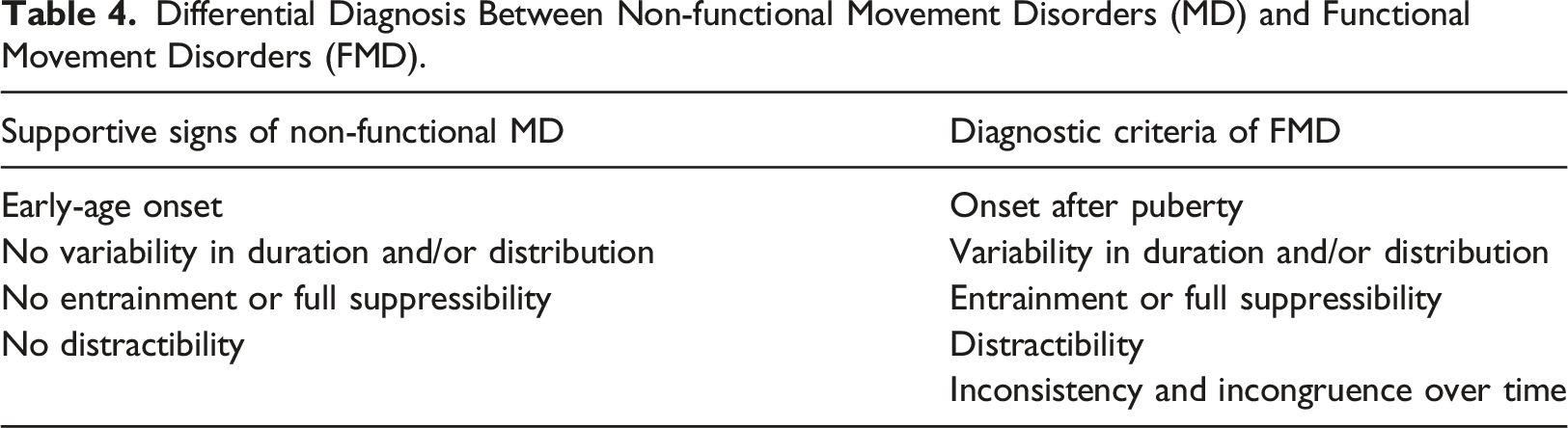
Differential Diagnosis Between Non-functional Movement Disorders (MD) and Functional Movement Disorders (FMD).
Confounding features in this case were represented instead by psychopathological issues that led clinicians to consider FNSD. Anxious disorder and significant impairment of the quality of life and daily autonomy probably arose as secondary symptoms, due to the chronic disease experience and to the concern associated with the involuntary manifestations. Considering a broader lens, it is essential to acknowledge the potential impact of psychopathological factors and consider a more multidisciplinary approach in the differential diagnosis, particularly when confounding features such as anxious disorder or overprotective parents significantly impact the patient’s quality of life.
In literature, PRRT2 mutations are largely reported as a major cause of paroxysmal kinesigenic dyskinesia (Ebrahimi-Fakhari et al., 1993; Méneret et al., 2012; Ohira et al., 2023), and the genetic confirmation is fundamental because of the possibility of available treatment with a positive outcome. Moreover, paroxysmal kinesigenic dyskinesias (PKD) have frequently been noted as prone to misdiagnosis, particularly given their occasional association with anxious-depressive symptoms (Junewtar et al., 2014; Pan et al., 2018; Cao et al., 2021). Therefore, despite being rare conditions, genetic MDs should be carefully considered as a differential diagnosis of FMDs, especially when clinical and anamnestic data are limited and inconclusive.
Notably, the same genetic condition has been very recently reported in the literature in comorbidity to FNSD (Ohira et al., 2023). The authors described a case of a young woman with paroxysmal kinesigenic dyskinesia genetically determined with functional weakness that significantly worsened the whole clinical presentation. In our paediatric case, on the contrary, FNSD should be more accurately considered as a misdiagnosis, given that his symptoms were better explained by the PRRT2 mutation and highly responsive to a specific treatment. In conclusion, our presented case underscores the intricate challenges in distinguishing between functional and non-functional motor disorders in paediatric neurology, emphasizing the need for a meticulous diagnostic approach. It is imperative to recognize that FNSD is a diagnosis of inclusion based on typical clinical features, cautioning against its sole reliance on unusual, unexplained, or psychologically triggered symptoms.
Therefore, we suggest that child psychiatrists, paediatric neurologists and other clinicians should consider careful evaluation of typical features and possibly prolonged follow-up, combined with clinical-oriented genetic testing, in children presenting with apparent FNSDs, to avoid misdiagnosis and to promote accurate treatment strategies. This approach may help to achieve a correct diagnosis and the development of tailored treatment for young patients.
Footnotes
Author contributions
Research project: Conception (VB, DE), Organization and Execution (VB, KB, DE, MN, VZ). Manuscript Preparation: Writing of the first draft (KB, DE, MN), Review and Critique (VB, SG). All authors have read and agreed to the published version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Institutional review board statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments. We confirm that we have read the Journal’s position on issues involved in ethical publication and affirm that this work is consistent with those guidelines.
Informed consent
Informed consent was obtained from all subjects involved in the study and their parents when required.