
Abstract
The purpose was to examine a sample of Stockholm residents’ social representations of their physical and mental health and ill-health. Four open-ended questions were answered by 1240 people between 18–80 years. A thematic analysis revealed nine aspects of health: physical, lifestyle, psychological, social, recreational, work and study, treatment, other and multifactorial aspects. Some cross-cutting themes were described to have an impact on health: empowerment, health-conscious lifestyle, life balance and life perspective. A key result is the interdependence between physical and mental health that was described by the respondents.
There are health beliefs that emanate from the medical expert sector as well as from the lay sector. The present study focuses on the latter. Regarding theories about health, the World Health Organization definition of health is well known: ‘Health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity’ (WHO, 1946). Doyal and Gough (1991), however, argued that health only can be defined negatively (eg, minimization of death, disablement and disease). Marks et al. (2011, p. 6), on the other hand, define health as ‘a state of well-being with physical, cultural, psychosocial, economic and spiritual aspects, not simply the absence of illness’. Seedhouse (1997) suggested that there are universal foundations for health as well as more specific foundations depending on individual abilities and circumstances, which is in line with Nordenfelt (1986), who described health as a balance between a person’s goals and abilities. Antonovsky (1979) argued that human health is a state of fulfilment and that one needs a constructive flexibility to manage different life situations. Mental health can be described more specifically, such as ‘a state of well-being in which the individual realizes his or her own abilities, can cope with the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to his or her community’ (Herrman et al, 2005, p. XVIII).
Health and illness can be studied from different perspectives such as the biomedical, behavioural, societal and cultural (Radley, 1994). The present study applied a bio-psychosocial perspective. Self-rated health can be studied, where lay representations of health and ill-health are in focus, as well as objective health indicators. A theoretical perspective that is important in this context is that humans strive to satisfy their needs to gain a healthy life. People’s needs are objective and physical as well as subjective and psychological (Doyal and Gough, 1991). However, basic human needs vary greatly between cultures and over time.
Within the human science tradition, one significant line of research about people’s accounts of health and illness is based on the theory of social representations (Farr and Moscovici, 1984), which has been applied here as a theoretical framework. This is a useful thought system when studying people’s everyday conceptions about health and illness (Farr and Marková, 1995). Representations about health and ill-health can be said to be ‘natural’ or common sense knowledge as compared to scientific knowledge. A representation is defined as a person’s internal construction of reality, which includes cognitive aspects (knowledge, thoughts and beliefs) as well as affective aspects (feelings, sensations and experiences). Hall (1997) claimed that social representations include processes by which language is used to create meaning out of empirically experienced phenomena. There are, therefore, no objects, people or events that have true or definitive meanings. Social representations are needed by people to orientate themselves and communicate, which they do by naming the different parts of the world and what they share with others. However, people do not just have an individual stance (or attitude); rather, they also take part in the general beliefs about the nature of the world that exists. A ‘representation’ or ‘cognition’ therefore is a socially shared activity (Radley and Billing, 1996). Although it is a socially shared activity, individuals create different meanings due to contextual and individual variation. Representations regarding health and illness furthermore relate to what is socially acceptable as ‘real’ (Farr and Moscovici, 1984). Herzlich (1973, p.139) writes: ‘Health and illness appear as a mode of interpretation of society by the individual and as a mode of relation of the individual to society.’
It is a part of human nature to interpret and give meaning to different things in life. Social representations are formed to create meaning and control about why one is sick or healthy. There is extensive literature about lay perspectives regarding disease and illness (eg, Blaxter, 1983; Fitzpatrick, 1984; Mercado-Martinez and Ramos-Herrera, 2002; Räty et al, 2006; Stainton Rogers, 1991; Williams and Calnan, 1996) although not all embedded within the theoretical framework of social representations. However, there is a lack of studies that focus on people’s explanations as to why they are healthy and also studies that emphasize both mental and physical health and ill-health, as in the present study. Factors such as age, cultural background, social class, education and profession are important when the representations of health and ill-health are formed. These also vary according to the individual’s current state of health. The social representations are also influenced by medical knowledge. In addition, it can be assumed that lay perceptions of health and ill-health coincide in part with those health determinants described by experts that involve people’s social networks, upbringing, lifestyles and living conditions (Dahlgren and Whitehead, 1991). There is also a possible relationship to individual ‘health literacy’, our ability to understand and interpret various factors that have an impact on health and find relevant health information (Adams et al., 2009). Closely linked with representations regarding health and ill-health are issues about responsibility. A person with a bad lifestyle can, through ideological beliefs and victim-blaming that exists within society, be made to feel responsible for his or her ill-health (Marks et al., 2011; Seedhouse, 1997). Conversely, if the causes are assigned to the outside world, the individual is relieved from responsibility. In a culture were individualism is strong, a healthy behaviour might be seen a moral obligation, also in the eyes of health-care givers. Illness, on the other hand, can be seen as an individual moral failure and may therefore be associated with guilt and stigmatization (Asbring, 2002).
The purpose of the present study was to explore how people living in Stockholm County, Sweden, describe the causes of their physical and mental health and ill-health.
Method
A questionnaire was sent out in late autumn, 2008, by the Central Statistical Office of Sweden to 4,000 randomly selected individuals residing in Stockholm County. 2,000 questionnaires were sent to people in the 18–30 year old age group (the age group of primary interest to the basic study) and 2,000 to people in the 31–80 year old age group. The aim of the survey, which was stated in the questionnaire, was to gain a deeper understanding of everyday conceptions about health and spreading this knowledge. The questionnaire included a number of specific issues, various measuring instruments and some open questions. This article deals with only the responses from the open-ended questions. The open questions in the questionnaire were: 1) If you have any physical problems – what do you think is the cause of this? 2) If you’re mainly physically healthy – what do you think is the cause of this? 3) If you feel mentally ill in any respect – what do you think is the cause of this? 4) If you are feeling mainly mentally well – what do you think is the cause of this?
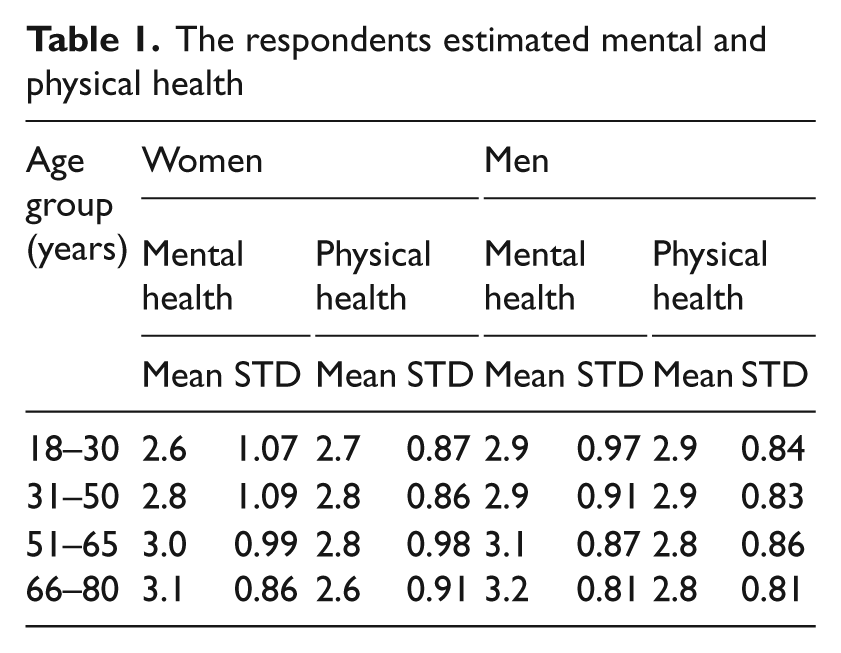
The questionnaires were sent out with a stamped and addressed envelope attached. After about three weeks, all 4,000 persons were sent a reminder as well as a new questionnaire. Participation was voluntary and anonymous as stated in the cover letter. The response rate for the sample was 36 percent (N = 1,425) (26% for the 18–30 year old age group and 41% for the 31–80 year old age group). The mean age in the sample was 43 years. 37 percent were between 18–30 years old and 60 percent of the respondents were women. 84 percent were born in Sweden. 73 percent had a relationship (married, boy- or girlfriend) and 27 percent were single. 54 percent had high-school education or less and 46 percent had a university degree/equivalent. 78 percent were employed or students and the rest of the sample were unemployed, in sick-leave or retired. The respondents’ physical and mental health was estimated on a 5-point Likert-scale between 0 (very bad) and 4 (very good - see Table 1).
The respondents estimated mental and physical health
Of the 1425 questionnaires that were answered and sent in, there were 1240 persons who answered one or more of the four open questions in the questionnaire that focused on everyday ideas about physical and mental health and ill-health. The answers to these questions were written down verbatim and were gathered in a text file that was subjected to a thematic analysis. Thematic analysis is a method used to identify, analyze and describe patterns (themes) in the data material, that is, text (Braun and Clarke, 1996). A theme describes something significant about the material in relation to the research question and can be said to be a carrier of meaning. The approach in the present study was to first analyze the responses question by question and summarize common themes for each question. Then the analysis included a movement back and forth across the entire data material to find patterns/categories that covered all the questions/issues. The themes identified were revised until they felt appropriate and meaningful in relation to the study’s aim and empirical material. The project was examined and approved by the regional Ethics Review Board at Karolinska Institutet in Stockholm, Sweden (2008/5:7).
Results
The themes that came out in the analysis of the answers, specified in the following list, reflect the most central aspects in the participant’s answers about causes of their physical and mental health and ill-health. Yet, the quotes should not be seen as representative for all the answers but instead as reflecting both specific and more general perceptions. It is the breadth of the responses and themes that are crystallized from this diversity that contributes to a deeper understanding.
Physical aspects – for example, heritability, the body’s health status, physiology and other aspects that have an impact on the body (eg, environment).
Lifestyle aspects – sleep, exercise, eating habits, etc.
Mental aspects – for example, attitude to life, personal characteristics, life events and coping strategies as well as mental health and illness.
Social aspects – mainly about relationships and security/insecurity in various respects (eg, housing, economy).
Recreational aspects – includes interests, leisure and other committed activities.
Work and study aspects –- positive and negative consequences of work and study life.
Treatment aspects – positive and negative consequences of treatment or encounters with healthcare providers or alternative practitioners.
Other aspects – aspects not included in the above categories.
Multifactorial aspects – a combination of the aspects mentioned above.
The following text describes the participant’s views about what is thought by them to give rise to health and ill-health. The nine aspects in the list then are related to perceived physical ill-health, physical health, mental ill-health and mental health. The responses reflect a process of psychological organization of experiences and perceptions regarding health and ill-health that becomes representations of one’s ‘world’ as well as a construction of ideas (Herzlich, 1973).
Physical aspects
The physical aspects that were believed to contribute to physical ill-health included heredity, physical disadvantages, heavy work, weight and age. The foundations for physical health were, for example, good genes, youth or having a good physical condition. Some other factors were frequent hand-washing and dressing appropriately for the weather.
The physical aspects considered to lead to mental ill-health were most often different diseases and ailments but also, for example, sleep disturbances, overweight, alcohol dependence, pregnancy or conditions that can accompany ageing: It is sad to feel the power of the body wane and that pains and wears takes out its right. Ageing is a hard even mentally. (Woman, 63 years)
Physical aspects that contribute to mental health were, for example, being physically healthy, having energy and good genes.
Lifestyle aspects
The lifestyle aspects that were thought to cause physical ill-health were most of all bad food or eating habits, inactivity, poor sleeping habits, smoking, alcohol and drug abuse. Conversely, the opposites of these same aspects were described as leading to physical health. However, a few considered themselves to be healthy in spite of an unhealthy lifestyle because of luck or good genes.
A bad lifestyle could lead to mental vulnerability and negative feelings. A good lifestyle, on the other hand, seems to be very relevant to mental health. According to the respondents, a healthy lifestyle includes a good diet, exercise, healthy sleep, time spent outdoors, good daily routines, moderate consumption of sweets and alcohol and being a non-smoker. A good lifestyle can, according to some, be a buffer when life pressures occur: Periods when I lose a little weight and exercise, I feel pretty much better mentally and can handle e.g. stress better. (Man, 50 years)
Mental aspects
The mental aspects that were thought to cause physical ill-health were often imbalances in life such as stress or lack of spare time (Worth noticing is that the terms ‘stress’ represent different things for different people). Depression, an earlier experienced trauma, grief and worry was also brought up as factors. Several of the respondents thought that ill-health can be ascribed to whether one wants to become ill or not. Sometimes participants described a direct link between mental aspects and physical symptoms: If I am much stressed, my eczema blooms up more easily. (Woman, 30 years)
A variety of mental aspects were considered as having a positive impact on physical health, including empowerment (ie, having the resources to manage one’s life), self-knowledge and self-esteem. Respondents often raised the importance of positive thinking and having a balanced life. Many noted a relationship between their physical and mental state: According to my own experiences, I believe that if one is psychologically happy, the body becomes healthier. (Woman, 21 years)
Participants described seven partially overlapping aspects relevant for mental ill-health: 1) negative thoughts, 2) imbalances in life, 3) a stressful life situation, 4) anxiety, 5) a difficult childhood, 6) mental health problems and diseases and 7) negative personal characteristics. Negative thoughts included not being able to forgive and move on and beliefs about not being able to affect one’s life. Imbalances in life regarding for example activity versus rest lead to a poor everyday rhythm. A stressful life situation is usually due to external or internal requirements sometimes dictated by a high level of ambition. Anxiety was related, for example, to the economy, the housing situation, work or one’s own or others’ ill-health. A difficult childhood includes traumatic experiences in childhood, for example, because of mentally ill parents, sexual abuse, rape or harassment. The mental health problems and diseases mentioned were psychosis, neurosis, anxiety, anorexia, depression, sadness, crisis and sorrow. The perception of negative personal characteristics described included poor self-confidence and shyness as well as problems with setting limits, prioritizing and planning ahead. Also, lack of reflection in regard to one’s situation is believed to cause mental problems: I only continue in old habits and do not see the reasons for not feeling well and haven’t implemented any changes. (Woman, 45 years)
Seven partially overlapping mental aspects were seen as important for good mental health: 1) awareness, 2) balance, 3) personal satisfaction, 4) internal drive, 5) optimism, 6) existential conditions and 7) personal characteristics. Awareness means having an insight about what is important for health including listening to the body’s signals and being clear about one’s values and priorities. Balance between activities and taking the time to rest was seen as important, as well as having a healthy balance in regards to one’s personal budget, exercise, food, sleep, relationships and home situation. Personal satisfaction involves experiencing feelings of joy, gratitude and contentment. It also encompasses accepting life with equanimity and letting go of trivialities and worry: I have a positive attitude and do not hung up on little things. Life goes up and down. (Woman, 45 years) Am I here and now or concerned about things that have happened or will happen? The first makes me feel good. (Man, 18 years)
An internal drive was also considered to be important, that is, to have motivation, energy and life goals. Optimism means seeing opportunities instead of setbacks and obstacles and refusing to dwell on things that you cannot influence. There are also existential conditions which were considered to have an impact on mental health, such as believing that life has a meaning. Belief in God or another kind of spiritual interest was seen as important by some. Certain personal characteristics such as being flexible, open, humble, patient and able to forgive were viewed as important, as well as having a sense of humour. Also, self-esteem, self-confidence and self-knowledge as well as coping capabilities were seen as essential for mental health.
Social aspects
The social aspects that were believed to lead to physical ill-health were unemployment, violence, a recent divorce, having small children or being a single parent. Several social aspects were considered to contribute to physical health, such as having a rich social life, good relationships and a loving and healthy family. The importance of love and a good sexual relationship was sometimes raised. Security regarding the home situation, housing, economy and work were also seen as essential aspects: Good life with my partner, good housing, a healthy family, ok economy = generally happy [relates to physical health]. (Man, 37 years)
The social aspects that were considered to cause mental ill-health were: 1) poor social relationships, 2) a vulnerable social situation and 3) social exclusion. Poor social relationships involve conflicts and harmful relationships. A vulnerable social situation includes unemployment, homelessness or not having a permanent place of residence, a recent separation, economic problems, addiction, abuse and racism. Social exclusion was described as, for example, lack of social contact, the absence of love and emotionally intimate relationships and not having children. Respondents also mentioned social difficulties.
The two social aspects that stood out as causes of good mental health were: 1) a good social life in general and 2) security. Relationships are important for a good social life, which includes spending positive time with friends, family and others. For some, it is important to have a large social network. Social life can also include a beloved pet or contacts on the Internet. Security involves having a stable relationship, steady work, good and stable accommodation, good financial situation and living in a welfare society.
Recreational aspects
No recreational aspects were raised in relation to ill-health, but they were thought to have an impact on good health, in particular mental health. The importance of being involved in activities and taking part in different social contexts was brought up alongside with the positive effects of personal development, commitment, creativity and having fun.
Work and study aspects
Many of the work and study aspects which were believed to cause physical ill-health were related to a stressful work environment. Other factors such as poor ergonomics at ones workplace or other health and safety problems (eg, noise, chemicals) were also described. In relation to physical health it is, above all, essential to enjoy one’s work or studies and not work too much. The value of using protective equipment and correct work techniques was also mentioned.
Work and study aspects were most often raised in relation to mental ill-health and included an excessive workload, time pressures, bad planning, uncertainty about the future, unclear/unachievable objectives, low levels of agency in one’s work environment, under-stimulation, lack of appreciation, conflicts, poor social work environment, poor management, poor self-performance and disliking one’s job. Being unable to work was another aspect that was mentioned, which includes unemployment.
The reverse of these aspects were brought up in relation to good mental health, including having a fun, stimulating, meaningful and creative job. It was also seen as essential to be able to affect one’s work situation, to feel satisfied with one’s own performances, to feel appreciation and support, having a moderate workload and reasonably challenging work as well as good colleagues and a competent manager.
Treatment aspects
Certain treatment aspects, mostly deficiencies in care and treatment, were believed to cause physical ill-health. Respondents referred for example to medicinal side effects and unsuccessful operations. Some thought that they had not received appropriate help from health care providers. Positive grounds for physical health included having received help from caregivers and in some cases from alternative medicine practitioners.
In regard to mental ill-health, some of the respondents said that they were affected by bad encounters with health caregivers or because they themselves or a relative had not received help. Some had been exposed to a mistake in the healthcare sector. When it comes to descriptions of what contributes to mental health, the participants listed aspects such as having a good doctor, receiving helpful medicines and treatment, being offered psychological therapy and having a successful alternative treatment.
Other aspects
There are some other aspects that have come to light. One of those is to not describe any cause for a certain illness/disease. This may be because one has not arrived at any conclusions, not reflected on it, or because there is medical uncertainty surrounding the illness/disease. Two of the respondents reflected on some aspects relevant to diabetes and epilepsy: I have diabetes. No relative has it. I have always had it, difficult to say what it depends on. (Woman, 29 years) Epilepsy, I have just as the doctor, no idea about the cause. (Man, 60 years)
Some believed that certain conditions but not others are due to misfortune: I have had herniation and kidney inflammation. It was sheer bad luck. On the other hand, herpes zoster, that I’ve had, may be stress related. (Man, 22 years)
A few other aspects were raised, including that ill-health is the will of God or a signal about that something is wrong in a person’s life: Disease belongs to life. For me, as a believer, everything has a sentence, if we are healthy or sick. It is a trial. (Woman, 40 years)
Multifactorial aspects
In relation to physical ill-health as well as physical health, different factors, such as family history, social life, lifestyle and psychological aspects, were often mentioned in combination. The quotes below from a young and an older man illustrate this kind of reasoning: There are many reasons [for physical health], including food, exercise, hereditary genes and how mentally healthy one is. Simply put, physical health depends on various things. (Man, 21 years) A good mix between physical activity (gardening, long walks, etc.) and intellectual activity (genealogy, reading, surfing on the Internet), family unity and other social gatherings. [relates to physical health] (Man, 79 years)
Mental health and ill-health were attributed to many different aspects, in particular regarding one’s life attitude, social relationships, work situation and lifestyle. Often several lifestyle aspects were brought up in the same excerpt, but other aspects were simultaneously thought to have an impact on the process, which is described by a young and an older woman: [To] feel physically well, have good relationships, good life situation, good food, exercise, health, positive thinking [relates to mental health]. (Woman, 29 years) Good genes. I have never smoked. Positive thinking. I have a nice man, fine children and grandchildren. I have always been active, cycling, skiing, trekking, orientation and so forth. I have never eaten too much food and sweets. I also have a strong psyche [relates to mental health]. (Woman, 68 years)
Synthesis
The social representations that are illuminated in the respondent’s answers reflect their relation to health, ill-health and society, based on their construction of reality. A close relationship was described between physical and mental health. Although this is not something new to the research community, it becomes very apparent in the present findings, and is illuminated in the text and quotations (eg, ‘If I am much stressed, my eczema blooms up more easily’). It is also worth noting an awareness about one’s own impact on health. What is more, there is a breadth as well as a unity regarding certain aspects. Also, the participants relate their personal needs to their health and those needs differ between individuals. In general, ill-health was thought to arise due to bad health habits or because one had not received the necessary replenishment of positive health factors. Sometimes an event chain was described in which one negative event (eg, ‘stress’) is alleged led to other adverse events (eg, insomnia), which in turn could have further negative consequences. Some disorders were considered to be outside one’s control (eg, hereditary diseases) and others attached to one’s own responsibilities (eg, bad diet). Good health was described as dependent on: self-motivated activities carried out in order to stay healthy and feel good (eg, exercise), good conditions that already exist (eg, a good family life), absence of negative health aspects (eg, stress), avoidance of what is perceived as bad for health (eg, smoking) and the moderation of unhealthy habits (eg, alcohol). The term ‘stress’, however, is not a uniform concept, as mentioned. In the literature, stress can be defined as feelings experienced when a person perceives that demands exceed the personal and social resources (Lazarus, 1966). However, in daily life, the stress concept has a wider meaning such as feelings of exhaustion, not having enough time for different activities, frustration or worry.
In relation to the demographic variables the results shows that young people (18–30 years), women in particular, brought up mental health aspects more often than the other respondents. People between 31 and 65 emphasized issues relating to life balance and one’s life perspective more often than people in the younger and older age groups. Older people (66–80 years) described to a greater extent physical and treatment aspects. A healthy lifestyle was seen as important in all age groups, but was somewhat more prominent among men. The women, in general, described social and recreational aspects as more important for one’s health than the men did.
Summarizing the key elements of what was described as important for physical and mental health and ill-health, there are some themes that are especially prominent, namely: empowerment, a health-conscious lifestyle, life balance and life perspective. ‘Empowerment’ concerns having resources to manage one’s life and feeling a certain control over things that happens in your life. ‘A health-conscious lifestyle’ relates to healthy life habits regarding food, exercise and so on. ‘Life balance’ includes a beneficial life rhythm and sense of influence over the time spent on different activities. ‘Life perspective’ involves the personal stance individuals have to different life events, such as optimism, which has consequences for internal and/or external strategies. These four themes are related to both mental and physical health and ill-health. Of course, there are other important aspects that are central. Empowerment, health awareness in terms of lifestyle, balance in life and one’s life perspective, however, are aspects that are regularly mentioned and capable of being affected by an individual. These themes also relate to existing representations and ideologies within the western society today.
Discussion
Nine themes emerged from the respondents’ answers about their perceptions of and beliefs about the basis for their mental and physical health and ill-health. These themes, as well as the four cross-cutting themes discussed previously, are influenced by the cultural context, since the values and information that exist in society are integrated into images, ideas and beliefs about health and ill-health. Social representations are, thus, a set of codes linking the individual to his or her world. The representations formed are based on cognitive as well as affective aspects and most often relate to socially suitable explanations. The individual’s responsibility in relation to their health, in particular in regard to lifestyle issues, becomes apparent. Their basic physical and psychological needs, as well as the moral choices made in this respect, can be seen in the text. Guilt or satisfaction therefore exists side by side. However, several aspects were seen as being outside the individuals own control and hence responsibility. Multifactorial descriptions were common (see also Blaxter, 1983; Kuyken et al., 1992; Lindholm, 1997; Millstein and Irvin, 1987; Risør, 2009). Also noted is that there seem to be universal foundations for health as well as more specific ones relating to individual characteristics. Health in general seems to relate to a definition of health that includes physical, cultural, psychosocial, economic as well as spiritual aspects (Marks et al., 2011). Mental health, if looked at separately, relates in to a definition that includes well-being, realization of one’s own abilities, coping with normal life stressors and taking part in societal life (Herrman et al, 2005).
There can sometimes be a substantial gap between a patient’s lived experience of illness or disease and the scientific explanations of the same condition. These different definitions of the problem can be a source of conflict between the patient and the caregiver, which also may lead to non-compliant behaviour or ‘doctor-shopping’ (Asbring, 2004). Therefore, it is important that health care providers take into account the individual’s perceptions regarding what is relevant to their health and illness (Toombs, 1993). Such knowledge could facilitate the relationship between the patient and caregiver, the degree of compliance and possibly also the healing process. It may, for example, be easier for health care givers to motivate individuals to adopt a more health-conscious lifestyle and strengthen their empowerment power in relation to potential problems. Therefore it is also important adopting a consumer-centric perspective when studying behaviours and health motivation (Shaw Hughner and Schultz Kleine, 2008).
As a complement to the traditional focus on lifestyle issues within public health work, it would be valuable to grasp other aspects such as empowerment, life balance and life perspective issues. These have, in different studies, been showed to have implications for health and also relate to physical health (Antonovsky, 1979; Cowley and Billings, 1999; Rasmussen and Scheier, 2009). This would be a holistic public health challenge that spans over multiple areas, which would be in line with a contemporary way of thinking. It is possible to direct these issues in public health messages or discussing them on a regularly basis in schools, workplaces and so on. Primary health care providers could organize groups that discuss and reflect over these topics. Health promotion activities in the field should, however, take into consideration the within culture diversity that exist, for example, in terms of health determinants and individual needs, in a step towards more equal health possibilities. Most important here is, however, to highlight that social representations are based on people’s own thoughts about health and ill-health that relate to their endeavour to satisfy their needs of a healthy life, and therefore should be given much more importance in research and development than they are accorded today.
Compared to other studies in the field, the present study related the representations to both mental and physical health and ill-health. Because of this, the relation between physical and mental health becomes more apparent. Nevertheless, it is probably true that people living in Stockholm have similar social representations on a general level as those that live in countries with the same cultural context. It is, however, not possible to see the within cultural variations that exist here, which could be interesting to look into in a forthcoming study.
Limitations
Some methodological shortcomings of the study should be mentioned. Since the response rate was low, the possibilities to generalize the results to a larger population are limited. Also, the questions stated in the questionnaire were not truly open, since the participants were forced to think of causes only. Furthermore, an interpretation has been made in respect to which categories (lifestyle, etc.) the participants’ statements should be placed, which sometimes could be difficult. The categories are, therefore, not completely distinct. Also, it is important to bear in mind that the representations not are fixed states, but can vary from day to day or situation to situation (see also Tamm, 1993). No true or definitive reality does exist.
Conclusions
The findings indicate that there is a close link between mental and physical health. This is a core result in the study, as well as the broad and multifactorial set of representations regarding health that is exemplified. The nine themes as well as the four key themes that were seen as essential also provide new knowledge in this field. In public health work, efforts are needed to improve health in the population. Since many of the representations in this study show interdependence between mental and physical health, this is something that health care providers as well as public health workers, should take into account much more. Improved mental health may result in a perception of better physical health, that is, a double benefit for the individual as well as society as a whole.
Footnotes
Acknowledgements
This study was performed on mission of Stockholm County Council, Sweden.