
Abstract
The study investigated the quality of sexual life of male obstructive sleep apnoea patients. Apnoea and non-apnoea participants were assessed with Golombok Rust Inventory of Sexual Satisfaction (GRISS) and Structured Clinical Interview for DSM-IV (SCID) before the sleep test. Folicule Stimulating Hormone (FSH), Luteinising Hormone (LH), prolactin, testosterone and oestrogen levels were also evaluated. The apnoea group had a higher BMI and lower LH and testosterone levels than the non-apnoea group. There were no differences between the apnoea, non-apnoea groups and within the apnoea groups (mild, moderate and high apnoea) in terms of sexual satisfaction. Although there was a change in the hormonal levels of obstructive sleep apnoea patients, the sexual life of apnoea patients was not affected at the clinical level.
Introduction
Arrest of respiration for at least 10 seconds during sleep is defined as sleep apnoea. There are three types of sleep apnoea: obstructive, central and mixed, and 90–95 percent of apnoeas are of the obstructive type (Aydin, 2007). Obstructive sleep apnoea (OSA) is characterized by episodes of complete or partial pharyngeal obstruction during sleep. According to the American Academy of Sleep Disorders Task Force definition, it is a condition characterized by repetitive episodes of flow limitation lasting greater than 10 seconds (hypopneas) and/or apnoeas (Macrea et al., 2010; Zias et al., 2009). Hypopnoea is characterized by decreased oxygen saturation by at least 4 percent and the formation of arousal with at least 50 percent decrease in respiratory volume at least for 10 seconds. The Apnoea-Hypopnoea Index (AHI) is achieved by sleep duration in hours divided by the total number of apnoea and hypopnoeas during sleep. This is also called the ‘respiratory disturbance index’ (RDI). People whose apnoea index is between 5–15 is considered as mild, 16–30 as moderate and those over 30 is considered as severe sleep apnoea syndrome (Aydin, 2007; Meurice et al., 1996). Obstructive sleep apnoea is one of the sleep disorders which affect the patients’ quality of life (Akashiba et al., 2002). Studies showed high co-morbidities of sleep apnoea/hypopnoea syndrome and chronic fatigue syndrome (Libman et al., 2009), sexual dysfunctions (Andersen and Tufik, 2008; Zias et al., 2009), neuropsychologic deficits including decreased concentration, memory loss, irritability, moodiness, depression, psychosis, decreased libido, and impotence (Guilleminault et al., 1978; Sullivan and Issa, 1985).
Androgens play a key role in the formation of male sexual characteristics. Three steroids that have primary importance for male reproductive function are testosterone, dihydrotestosterone and estradiol. The most important of these is testosterone. It is absolutely essential for the development of male sexual characteristics (Schenck et al., 2007). Reproductive function is primarily regulated by the hypothalamus, anterior pituitary, gonads and reproductive systems. The hypothalamus secretes Gonadotrophin-Releasing Hormone (GnRH) and provides LH and FSH secretion from the anterior pituitary gland. FSH induces spermatogenesis at seminiferous tubules in the testes of men and LH stimulates the secretion of testosterone from interstitial Leydig cells (Andersen and Tufik, 2008; O’Connor et al., 2011). Sleep is very important for healthy working of this axis. In addition, there is a bi-directional relationship between breathing and these hormones. For example, while testosterone plays a role in the regulation of breathing through various mechanisms, it have been reported that a change in hormone level occurs when breathing is impaired, such as in OSA cases (Andersen and Tufik, 2008; Luboshitzky et al., 2002; O’Connor et al., 2011; Schenck et al., 2007).
Reduction of morning testosterone concentration has been shown in research investigating the effects of OSA on sexual life (Grunstein et al., 1989; Santamaria et al., 1988). It has been suggested that OSA can cause an increase in the level of prolactin related with stress due to hypoxia and increase of prolactin may also cause inhibition of GnRH and secondarily to hypogonadism (Macrea et al., 2010). In their study of 308 male patients (aged 30–69), Peterson et al. (2010) described that sexual dysfunction is more prevalent in patients with OSA than the general population. However, this dysfunction was identified as a complex problem that is associated with factors such as age, obesity, social factors and concomitant medications rather than the severity of OSA.
Most previous studies of the effects of OSA on sexuality in men have focused on erectile dysfunction (ED) (Andersen and Tufik, 2008; Zias et al., 2009). OSA is considered to be one of the possible risk factors for erectile dysfunction. Literature review emphasize that OSA may contribute to erectile dysfunction because of abnormalities at regulation of neural, hormonal and vascular. More work is required to establish a causal connection, but case series and expert opinion support that relationship. There is also evidence that treating OSA may reduce ED (Meurice et al., 1996; Schenck et al., 2007; Petersen et al., 2010; Stannek et al., 2009).
We designed this study to investigate whether reproductive hormones or the quality of sexual life and the severity of the loss of function are affected in male patients with untreated OSA.
Method
Participants
Eighty-five male participants (42 apnoea and 43 non-apnoea controls) ranging from 21 to 60 years old (M=38.29±8.36) participated in the study. Male participants admitted to a sleep centre due to the complaints of snoring were enrolled. At the interview before the sleep test, patients were assessed with Golombok Rust Inventory of Sexual Satisfaction (GRISS), SCID and the standard interview form. After the evaluation at the sleep laboratory, fasting blood samples were taken at 08:00 to evaluate their hormonal profile (FSH, LH, prolactin, testosterone and oestrogen). Sleep test results were assessed by the investigator who was blind for the blood values and other test results. At the post-test evaluation, two groups were created from those diagnosed with sleep apnoea and not diagnosed with sleep apnoea. Patients were considered to have OSA when their apnoea/hypopnoea index (AHI) was more than five events per hour. Apnoea and non apnoea patients were compared in terms of GRISS scores and hormone profiles.
Exclusion criteria from the study were usage of nitrates, abnormal hormonal status, previous ED treatment, hypertension, diabetes mellitus, peripheral neuropathic disease, prostate cancer, pelvic trauma history, renal transplantation, aortic aneurysm, spinal cord injury, endocrine disturbances, penile deformity, alcohol abuse, psychotropic drug intake, presence of chronic and severe acute psychiatric disorders, chronic medical illness, cardiovascular diseases and metabolic and neurological disorders. The body mass index (BMI) was obtained from the electronic medical records (computerized patient record system). The study was approved by the local ethics committee and patients gave written informed consents.
Psychometric assessment tool
The Golombok Rust Inventory of Sexual Satisfaction was developed to assess the nature and function of sexual contact and severity of the loss of function at heterosexual individuals. There are separate forms for men and women. Beside the assessment of sexual satisfaction, scores for erectile dysfunction, premature ejaculation, anorgasmia, vaginismus, frequency of sexual intercourse, communication, sexual satisfaction, physical contact and avoidance were also obtained. Raw scores were transformed to standard scores from 1 to 9 and scores equal or more than 5 indicates a sexual problem. Validity and reliability studies were conducted in Turkey (Tuğrul et al., 1993).
Statistical analysis
Apnoea and non-apnoea groups were compared using t-test, ANOVA and MANCOVA analysis. Moreover, multiple regression analysis was used to analyze the predictor role of the variables.
Results
There was no significant difference between the apnoea (M=40±7.10) and non-apnoea (M=36.62±9.20) groups in terms of age, t(83)= -1.88, ns.
The apnoea group had significantly higher BMI scores than the non-apnoea group. Moreover there was a significant positive correlation between BMI and AHINDEX scores (r=.42, p<.01). However, there was no significant correlation between BMI and hormone levels and between BMI and GRISS subscale and total scores.
Apnoea and non-apnoea groups were compared in terms of their hormone levels; FSH, LH, Estradiol, Prolactin and Testosterone. LH levels of apnoea group were significantly lower than in the non-apnoea group. Similarly Testosterone levels of the apnoea group were also significantly lower than in the non-apnoea group. However, the two groups did not differ in terms of their FSH, Estradiol and Prolactin levels. See Table 1 for the comparison of the two groups in terms of age, BMI, and hormone levels.
Comparison of Apnoea and non-apnoea groups in terms of age, BMI and hormones
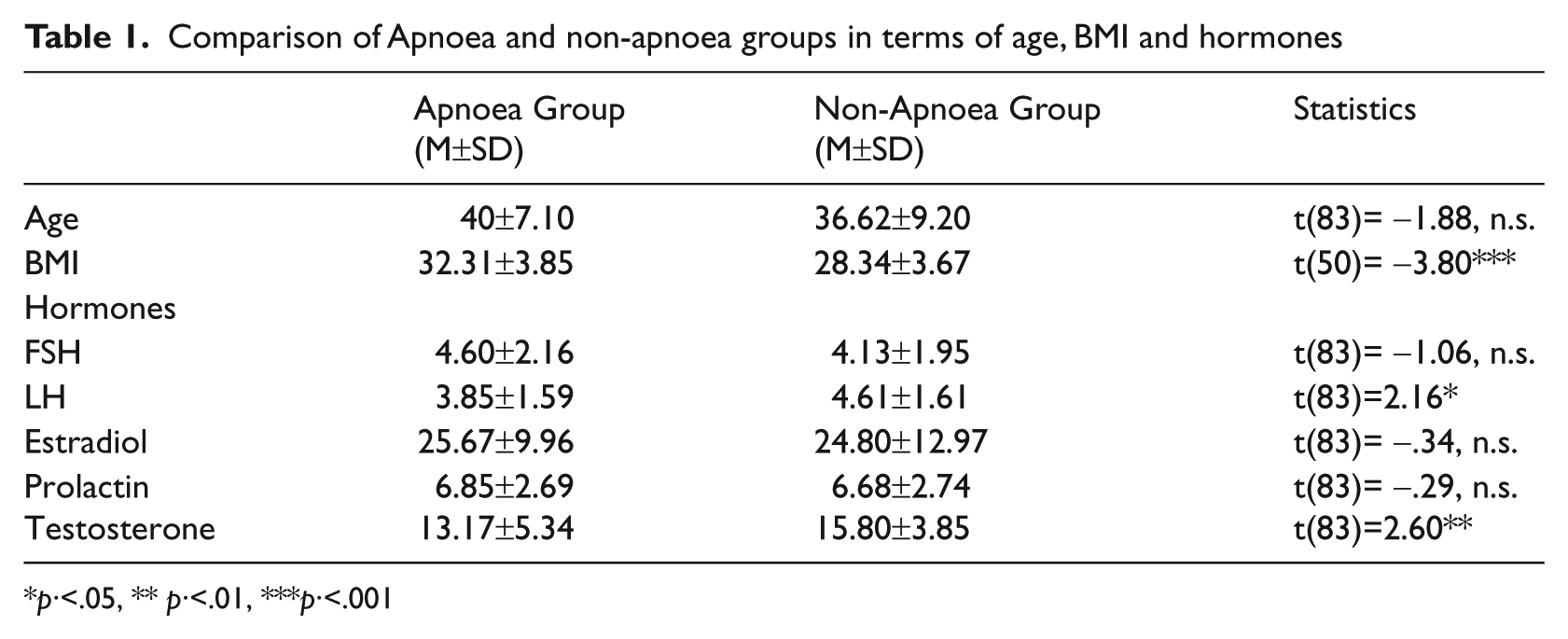
p·<.05, ** p·<.01, ***p·<.001
Apnoea patients were divided into three groups in terms of their apnoea severity (AHINDEX = 5–15, low; 15–30, medium; >30, high) and their hormone levels were compared. The results of the ANOVAs showed that high, medium and low apnoea groups did not differ in terms of their FSH [F(2,39)=.91, ns], LH [F(2,39)=1.10, ns], Estradiol [F(2,39)=1.49, ns], Prolactin [F(2,39)=.1.22, ns] and Testosterone [F(2,39)=2.69, ns] levels. The Pearson correlation coefficients between AHINDEX and hormones were also non-significant.
Sexual satisfaction levels of apnoea and non-apnoea groups, which were evaluated by GRISS subscale and total scores, were compared after controlling for age and BMI of the participants. MANCOVA results revealed that there was no significant difference between apnoea and non-apnoea groups in terms of impotence, premature ejaculation, non-communication, infrequency, avoidance, non-sensuality, dissatisfaction and total scores.
Moreover, mild, moderate and high apnoea groups and control groups were compared according to their GRISS scores first by MANOVA and then by MANCOVA after controlling for age and BMI. However, similarly no significant differences were found between the groups. The results of the MANCOVA and means and standard deviations of the groups were presented in Table 2.
Comparison of Apnoea and control group in terms of GRISS scores
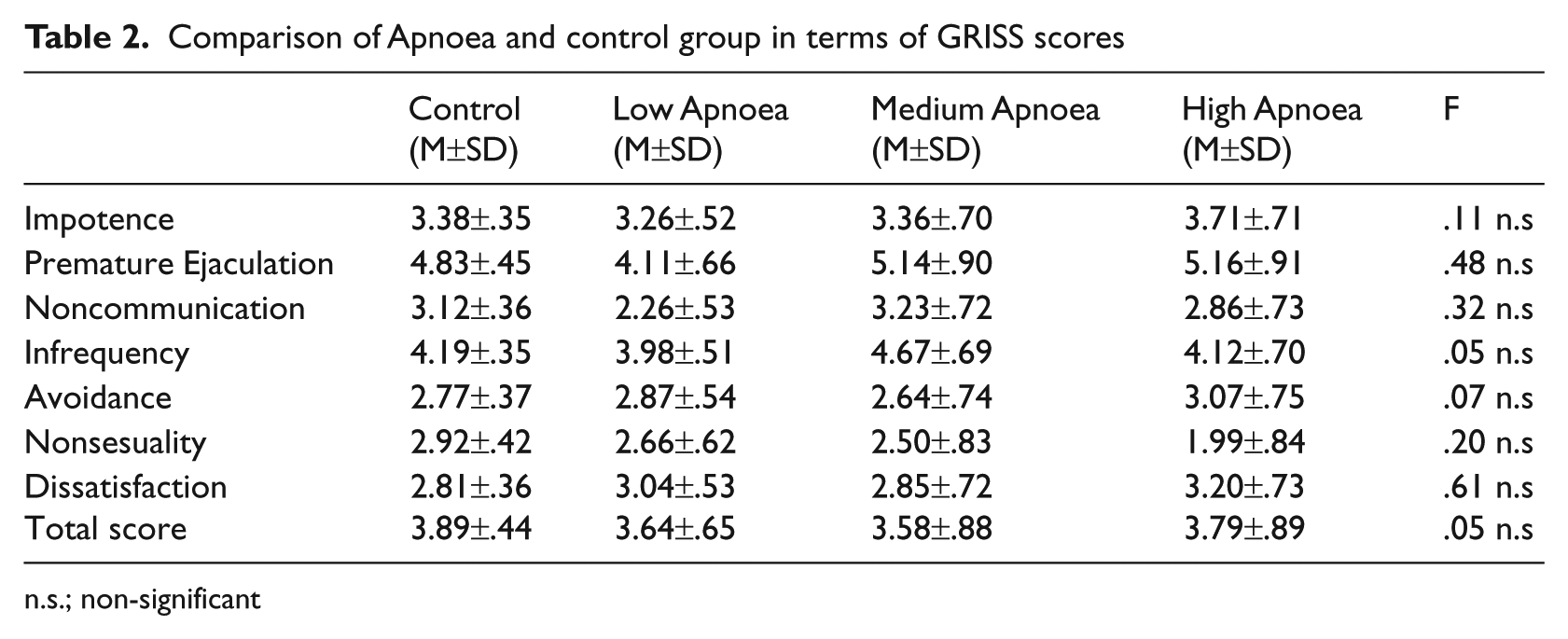
n.s.; non-significant
There was a positive correlation between impotence and FSH (r =.27, p<.05) and Testosterone (r =.23, p<.05). Moreover, premature ejaculation (r =.27, p<.05), dissatisfaction (r =.25, p<.05) and total GRISS scores (r =.32, p<.01) were also positively correlated with Prolactin. Multiple regression analysis was conducted to analyze the predictor role of hormones on sexual satisfaction. The results of multiple regression analysis revealed that FSH was a significant predictor for impotence and for total score, and Prolactin for premature ejaculation, avoidance, dissatisfaction and for total score (see Table 3).
Predictor role of hormones for GRISS subscale and total scale scores
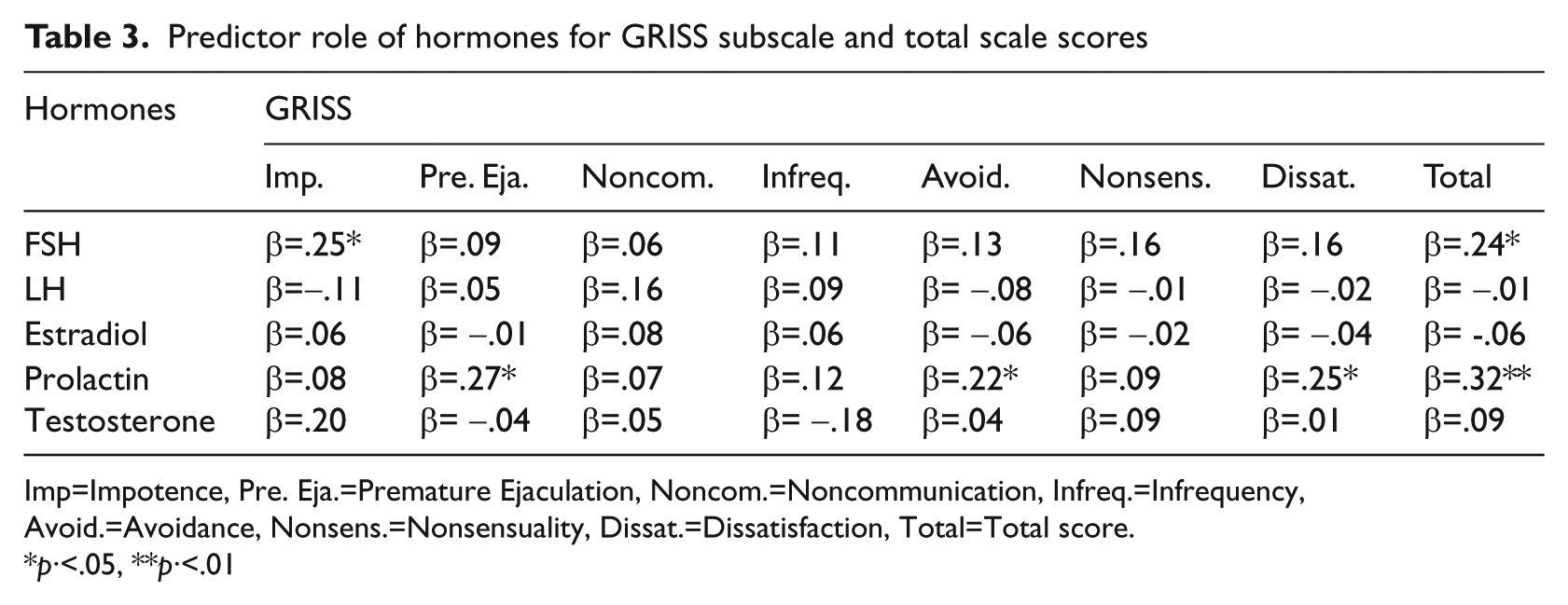
Imp=Impotence, Pre. Eja.=Premature Ejaculation, Noncom.=Noncommunication, Infreq.=Infrequency, Avoid.=Avoidance, Nonsens.=Nonsensuality, Dissat.=Dissatisfaction, Total=Total score.
p·<.05, **p·<.01
Discussion
In this study, the apnoea and non-apnoea groups did not have a significant age difference which is an important variable while evaluating sexual function and hormones. As it has been emphasized in previous studies, advanced age patients and age differences could be potential confounding factors (Petersen et al., 2010). The apnoea group had higher BMI scores than the non-apnoea group and a positive correlation was also found between BMI and the severity of the apnoea-hypopnoea index. This expected finding was compatible both with the previous studies (Margel et al., 2004; Meurice et al., 1996; Subramanian et al., 2010; Zias et al., 2009) and clinical experience. After controlling for age and BMI, there was no significant difference between apnoea and non-apnoea groups in terms of impotence, premature ejaculation, non-communication, infrequency, avoidance, non-sensuality, dissatisfaction and total scores. Similarly, when mild, moderate and high apnoea groups and control group were compared according to their GRISS scores, no significant differences were found between the groups. Although in some studies it was stated that there is a relationship between sexual dysfunction and sleep apnoea independent from variables such as obesity, mood disorders or apnoea severity (Meurice et al., 1996; Schenck et al., 2007), there are also studies suggesting that OSA is not an independent predictor within this complex interaction and obesity and other co-morbidities are main determinants (Petersen et al., 2010; Stannek et al., 2009; Zias et al., 2009).
In terms of hormones, it was found that LH and testosterone were low in the apnoea group and there was no difference in terms of FSH, estradiol and prolactin. In a study investigating the relationship between infertility and OSA=, reduction at prolactin levels were found after treatment of OSA=. Except PRL, no other hormone’s serum level, including that of FSH, LH, Test, Cor and Leptin, has changed significantly after the Continuous Positive Airway Pressure Treatment (CPAP) treatment (Macrea et al., 2010). Testosterone is important for changes in hormone levels during the sleep as well as affecting the structure of sleep as the main component of the male sexual function (Schenck et al., 2007). Male domination at sleep apnoea suggests that this hormone may be important in the pathogenesis of the disease. Again, sleep disorder is emphasized as a factor that reduces androgen levels in this study (Grunstein et al., 1989; Santamaria et al., 1988). Although there is not a significant result related to sexual function in our study, low testosterone and LH levels – that allows the secretion of testosterone – is a consistent finding with the studies describing a decrease in androgens. This may be the natural consequence of having a high BMI in the apnoea group. Weight gain and obesity is known to decrease testosterone levels (Gooren, 2003). Some other studies indicate an association between sleep apnoea and reduction in testosterone release in the absence of complications (Meurice et al., 1996; Petersen et al., 2010; Zias et al., 2009). But when obesity and OSA is together, additional severe hypoxia due to obesity may be an additional factor for decrease of testosterone levels. So both OSA and co-existing co-morbidities may contribute to low testosterone concentrations.
LH level still seems to be a natural result as being the secreting hormone of testosterone from testes. In this case, a change at both primary sexual organs and at the pituitary level may be considered. When we look at the correlations between GRISS and hormone profile, a correlation was not observed between LH and testosterone for total and sub-scores. It was interpreted as that although the disorder can be clinically reflected, it could not have been detected by GRISS.
When the apnoea group was evaluated on its own, there was no difference for hormone levels at high, medium and low apnoea groups. This supports that the severity of apnoea does not affect hormone levels and fundamental changes are determined by BMI.
As a result, the sexual lives of male patients diagnosed and not diagnosed with OSA were investigated for the first time by GRISS and no particular problems were discovered. However, it was suggested that the reduction of testosterone and LH levels are important. Since there has been a relationship between BMI and OSA, patients need to give importance to their weight control in order to increase the quality of their sexual lives as well as other areas of their lives.