
Abstract
The article investigates whether illness beliefs and beliefs about rehabilitation are predictors of short and middle term outcome in depression even when adjustments are made for variables, which are known to be predictors of the course of depression. Within the context of a non-controlled prospective study design, data were analyzed using forced entry hierarchical multiple regression analyses. The sample comprised N = 98 patients. Adjusting for a range of sociodemographic and medical predictors, illness beliefs and beliefs about rehabilitation predict outcome in depression. Illness beliefs and beliefs about rehabilitation are relevant starting points for designing patient-oriented interventions.
Keywords
Introduction
With lifetime prevalences between 15% and 17% (Ebmeier et al., 2006), unipolar depression is one of the three leading causes of disease worldwide, and it is projected to advance to first place in 2030 (WHO, 2008). Various risk factors for the onset, course, and prognosis of depression, have been identified (DGPPN et al., 2009) which can be classified mainly in illness-related, sociodemographic, and social factors. Some examples of these are a large number of previous episodes of depression (Müller et al., 1999), the existence of psychological or somatic comorbidity (Keitner et al., 1992), young age at the initial manifestation (Giles et al., 1989), female gender, and being unmarried (Müller et al., 1999). According to the German guideline ‘Unipolar Depression’ (DGPPN et al., 2009), there are four primary treatment strategies for treating depression: ‘watchful waiting’, medication, psychotherapy, and a combination of medication and psychotherapy. However, in view of the differences in efficacy and effectiveness of the treatment options, according to the guideline, there is a need for differential effect research in order to identify patient-related influence factors in addition to the factors mentioned above. In this context, special significance is accorded to the exploration of patient preferences, illness beliefs, and the resulting treatment expectations (DGPPN et al., 2009).
A theoretical model that might provide an appropriate framework to further explore illness representations in depression is the Common Sense Model of self-regulation (CSM) (Leventhal et al., 1980, 2001). According to the CSM, individuals who are faced with a health threat develop cognitive and emotional representations of the illness, which determine the selection of coping procedures – such as adherence – and health outcomes. The cognitive representations of the illness are composed of five interrelated components – identity (the symptoms and the ‘diagnostic label’ associated with the illness), causal beliefs, timeline beliefs, beliefs about control or cure, and consequences (Petrie and Weinman, 2006). Focusing on treatment beliefs in addition to illness beliefs, Horne (1999, 2003) postulated an extended self-regulatory model.
In the past 15 years, research has yielded evidence about the basic principles of the CSM (Hagger and Orbell, 2003). Although in the illness representations literature thus far there has been considerable emphasis on patients with chronic somatic diseases, recently research is also developing in the area of mental illnesses (Petrie et al., 2007). The fundamental applicability of the CSM was confirmed for these patient groups as well (Quiles and Terol, 2011), and there is growing evidence for the impact of illness beliefs and treatment beliefs on health-related outcomes, for example in patients with eating disorders (Quiles and Terol, 2011), fibromyalgia (Glattacker et al., 2010), and bipolar affective disorders (Hou et al., 2010). Furthermore, in many somatic diseases such as cardiovascular (Stafford et al., 2009) or oncology diseases (Dempster et al., 2011), multiple sclerosis (Vaughan et al., 2003), rheumatoid arthritis (Sharpe et al., 2001) and in haemodialysis patients (Chilcot et al., 2011), there is evidence that illness beliefs are related to depressive symptoms.
Illness beliefs and beliefs about medicines were also examined in patients with depressive disorders. One result was that in many cases, patient beliefs are not in concordance with scientific evidence. For example, patients often view antidepressants as addictive (Prins et al., 2008), and the patients’ subjective treatment preferences sometimes differ from those of their physicians (Löwe et al., 2006). Regarding public beliefs, Jorm et al. (2006) found the Australian public’s beliefs have changed between 1995 and 2003 to become more similar to those of mental health professionals. However, the percentage believing in the helpfulness of antidepressants was still lower than for vitamins or minerals (Jorm et al., 2006). There are also some findings that indicate that treatment beliefs such as skepticism concerning the necessity of antidepressants are associated with illness beliefs (Aikens et al., 2008; Riedel-Heller et al., 2005), and that illness beliefs and beliefs about medicines are related to health-related outcomes such as adherence (Brown et al., 2005; Burra et al., 2007), coping strategies (Kelly et al., 2007), seeking medical treatment (Edwards et al., 2007), and the course of depressive symptoms and well-being after rehabilitation (Horn et al., 2010).
However, studies on illness beliefs and treatment beliefs in patients with depressive disorders – especially using the CSM – are comparatively narrow (Fortune et al., 2004; Kelly et al., 2007). In particular in terms of the specific predictive value of illness beliefs and treatment beliefs in predicting outcome, little evidence is available, as other relevant predictors such as the baseline health status are frequently not controlled for. Furthermore, most of the studies are based mainly on beliefs about medicines. Beliefs about multimodal treatment concepts, such as those offered in psychosomatic rehabilitation for example, which in Germany is the second most important sector for inpatient care of mental illnesses after psychiatric treatment (Steffanowski et al., 2007), have not yet been studied on the basis of the CSM to the best of the authors’ knowledge. Therefore, the aim of this study was to examine a sample of rehabilitation patients with depressive disorders to determine whether illness beliefs and treatment beliefs (here: beliefs about rehabilitation) are predictors of short and middle term rehabilitation outcome, even when adjustments are made for other illness-related, sociodemographic, and social factors that are known predictors for the course of depressive illnesses. This was preceded by the question about changes in health outcomes in the short and middle term.
Method
Design
In the context of a project which was funded by the German Pension Insurance in the funding priority ‘Versorgungsnahe Forschung’ (Patient-oriented Research), the study was conducted between December 2008 and April 2010 in five inpatient psychosomatic rehabilitation centers. With the aim of preventing or mitigating impairment of participation in working life and in social life, patients with depressive disorders are offered psychotherapeutic treatments there, mainly in the form of group therapy, but also in individual therapy settings. Further important elements of therapy are physical therapy, sport and exercise therapy, occupational therapy, psychoeducation, and clinical social work (DGPPN et al., 2009). The multimodal treatment is given in a multidisciplinary team that in addition to physicians also includes psychologists, physiotherapists, social workers, occupational therapists, and so on. Inpatient psychosomatic rehabilitation lasts an average of four to six weeks and the patient generally has four to five therapy sessions a day on workdays.
The study followed a prospective design, where data were obtained at three time points. Two weeks before the start of rehabilitation, illness beliefs, beliefs about rehabilitation, and baseline health status were measured. At the end of rehabilitation and at a six-month follow-up, short and middle term outcome was assessed. Furthermore, the physicians at the rehabilitation centers documented the ICD 10 diagnoses at the start of rehabilitation. All patients over age 18 diagnosed with a depressive episode (mild, moderate, severe without psychotic symptoms or not otherwise specified; ICD 10 F32) or with recurrent depressive disorder (currently mild, moderate or severe episode without psychotic symptoms; ICD 10 F33) were included in the sample. Criteria for exclusion were bipolar disorder, acute suicidal tendency, addiction, disorientation, or ongoing early retirement proceedings. Testing for inclusion and exclusion criteria was done by a physician in the rehabilitation centers. Only those patients were included in the study who had given their written informed consent to participate. The study was approved by the Ethics Committee of the University Medical Center of Freiburg.
Response rate and sample characteristics
With respect to patients who were addressed before the start of rehabilitation (N = 224), 44% of the patients could be included in the study (N = 98). At the end of rehabilitation, the response rate was 98% and at the follow-up 82%.
Table 1 presents the distribution of patient characteristics in the sample. At follow-up, N = 18 patients dropped out of the study. With respect to gender (chi2 = .076) and depressive burden (t-test p = .334) there were no differences between dropouts and responders. However, the dropouts were about seven years younger than responders (t-test p = .003).
Patient characteristics (N = 96)
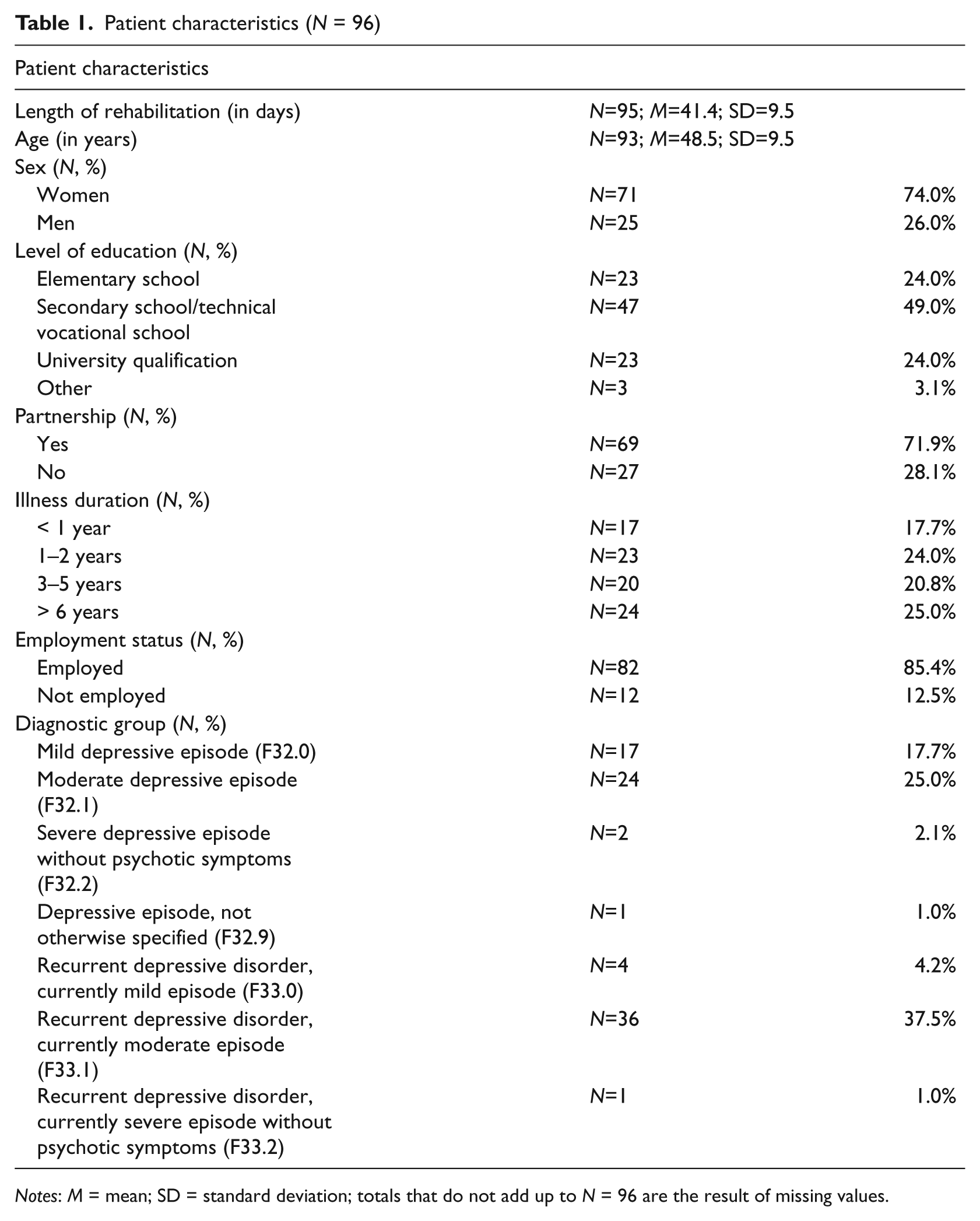
Notes: M = mean; SD = standard deviation; totals that do not add up to N = 96 are the result of missing values.
Measures
The outcome was operationalized using the German versions of the SF-36 (Bullinger and Kirchberger, 1998; Ware and Sherbourne, 1992) and of the CES scale (Center for Epidemiological Studies Depression Scale, Radloff, 1977; German Version ADS; Hautzinger and Bailer, 1993). Furthermore, physicians completed a questionnaire that included questions about disease-related variables such as somatic comorbidity (Glattacker et al., 2007). Modeled after instruments such as the Cumulative Illness Rating Scale (Linn et al., 1968), this score assesses the existence of 14 somatic diseases (e.g. diabetes or hypertension) and their impact on functioning.
To operationalize illness beliefs and beliefs about rehabilitation, instruments based on the extended CSM were used. Illness beliefs were measured using the German version (Gaab and Ehlert, 2005) of the Illness Perception Questionnaire-Revised (IPQ-R, Moss-Morris et al., 2002). Data on the psychometric quality of the German version are available (Glattacker et al., 2009a). The first section of the IPQ-R addresses the question as to whether patients have experienced different symptoms in the course of the disease and whether they believe these symptoms are caused by the illness (‘Identity’ scale). The items in the second section can be assigned to the scales ‘Timeline Chronic-Acute’, ‘Timeline Cyclical’, ‘Consequences’, ‘Personal Control’, ‘Treatment Control’, ‘Coherence’, and ‘Emotional Representation’. In the third section, the patients’ causal beliefs are measured. In the present study, the generic version of the questionnaire (‘my illness…’) was replaced by a disease-specific formulation (‘the depressive symptoms’). Furthermore, in the first section, depressive symptoms were added (see Fortune et al., 2004). In our sample, Cronbach’s alpha is between .69 and .87, however, the value of .40 for the scale ‘Timeline Cyclical’ was too low, so this scale was excluded from further analyses.
Beliefs about rehabilitation are measured using the ‘Beliefs about Rehabilitation Questionnaire’ (BRQ; Glattacker et al., 2009b), which was developed along the lines of the Beliefs about Medicines Questionnaire (Horne et al., 1999). Psychometric testing of the BRQ in patients with back pain and patients with depressive disorders was satisfactory (Glattacker et al., 2009b). With 23 items on four scales, the BRQ reflects the ‘psychological outcome expectation’ (Cronbach’s alpha .82), ‘somatic outcome expectation’ (Cronbach’s alpha .72), ‘process expectations’ (e.g. ‘My expectation of this rehabilitation is that all measures and treatments will be explained in the initial meeting with the physician’) (Cronbach’s alpha .88), and rehabilitation-related ‘concerns’ (e.g. ‘I am afraid that the rehabilitation will have negative consequences for my private life (such as long absences from my family’)) (Cronbach’s alpha .83).
Statistical analyses
Changes in health outcomes were analyzed using T-tests for dependent samples; standardized effect sizes were calculated to quantify the effects. The question as to whether illness beliefs and beliefs about rehabilitation are predictors of rehabilitation outcome was investigated using forced entry hierarchical multiple regression analyses. The scales of the SF-36 and the ADS score formed the dependent variables. As predictors, baseline health status was entered into the regression in Step 1, sociodemographic and illness-related variables (age, sex, partnership, employment status, level of education, duration of illness, diagnostic group, length of rehabilitation, and somatic comorbidity) were entered in Step 2, and illness beliefs and beliefs about rehabilitation were entered in Step 3. Categorical variables were dummy coded (see Tables 2 and 3). To avoid multicollinearity, of the dummy variables, only the parameter value that correlated best with the criterion variables in bivariate analyses was included in the final model. The variance inflation factor (VIF) was calculated to assess multicollinearity. Values above 5 can be considered an indication of multicollinearity (Menard, 2002).
Prediction of short-term outcome using hierarchical regression analyses; missing listwise

Notes: SF-36: Higher scores indicate better health (Range 0–100); ADS: Higher values represent higher depressive symptomatology (Range: 0–60); IPQ-R and BRQ: Values represent the scale content; standardized beta-coefficients that are significant are in bold print; – = Dummy not in the regression model.
Prediction of middle term outcome using hierarchical regression analyses; missing listwise

Notes: SF-36: Higher scores indicate better health (Range 0–100); ADS: Higher values represent higher depressive symptomatology (Range: 0–60); IPQ-R and BRQ: Values represent the scale content; standardized beta-coefficients that are significant are in bold print; – = Dummy not in the regression model.
Results
At the end of rehabilitation and at the follow-up, significantly better scores were achieved on all SF-36 scales and on the ADS-score than at the start of rehabilitation. In the short term, the effects with respect to the SF-36 scales ‘Vitality’, ‘Role-Emotional’, ‘Mental Health’, and ADS were strong (ES .85 to 1.7). In the medium term, the effects for the scales ‘Role-Emotional’, ‘Mental Health’, ‘Social Functioning’, and ADS were moderately strong (ES .49 to.66) and for ‘Vitality’, the effect was still strong (ES .85) after half a year.
Table 2 shows the results of the hierarchical regression analyses for the short-term outcome and Table 3 for the medium-term outcome. The VIF values in the final regression models were all less than 5.
The total explanation of variance for the health status at the end of rehabilitation was between 2% and 52%. Unlike Step 1, which includes only baseline health status, the addition of sociodemographic and illness-related variables in Step 2 and the addition of illness beliefs and treatment beliefs in Step 3 did not always lead to an improvement of the model. The corrected explanation of variance can be improved through sociodemographic and illness-related variables by a maximum of 8% and through illness beliefs and treatment beliefs by a maximum of 12%. With respect to the beliefs about rehabilitation, psychological outcome expectations predict general health, mental health, and less depressive symptomatology, while less somatic outcome expectations predict better outcomes regarding bodily pain. Regarding illness beliefs, treatment control predicts better outcomes regarding vitality and mental health, and illness identity predicts better physical functioning.
In the medium term, the total explanation of variance of health status lies between 30% and 57%. While the inclusion of sociodemographic and illness-related variables in the second step does not always lead to an improvement of the model (a maximum of 9% additional variance can be predicted), the corrected explanation of variance can be improved by up to as much as 19% by adding illness beliefs and treatment beliefs. With the exception of the scale ‘Role-Emotional’, baseline health status is always the strongest predictor. With respect to treatment beliefs, psychological outcome expectations and less pronounced process expectations predict better physical functioning, while somatic outcome expectations predict worse general health. Less pronounced rehabilitation-specific concerns predict better outcomes regarding bodily pain and social functioning. Regarding illness beliefs, illness identity, timeline acute-chronic, personal control, treatment control, and coherence are significant predictors of health status in the medium term. With respect to role emotional, beta-coefficients of the identity scale and the coherence scale are even larger than the beta-coefficient of baseline health status.
Discussion
With respect to the instruments used to operationalize illness beliefs and beliefs about rehabilitation, it was seen that the BRQ and the IPQ-R were both largely internally consistent when used for depressive patients and can thus be assessed as reliable for this aspect. One exception was the IPQ-R scale ‘Timeline Cyclical’. Here the Cronbach’s alpha coefficient was unsatisfactory – as in other samples of depressive patients as well (Horn et al., 2010; Vollmann et al., 2010). This can possibly be explained by the fact that some items of this scale deal explicitly with cyclical day-to-day fluctuations of symptoms, while other items are related more to the overall cyclical course of the disease, so that homogeneity of the scale contents cannot necessarily be assumed for patients with depressive disorders. The recently developed ‘Beliefs about depression questionnaire’ (Lynch et al., in press), which also refers to the CSM, might offer a solution for this problem.
Regarding the prediction of the outcome, the results initially show that the inclusion of sociodemographic and illness-related variables and – for short-term outcomes – illness and treatment beliefs does not always lead to an improvement of the model. This result can be explained by the fact that the corrected coefficient of determination R2 – unlike the uncorrected coefficient – accounts for the complexity of the model, that is, the number of independent variables. While the uncorrected R2 is larger regardless of whether the other variables actually contribute to making a prediction, the corrected R2 is stricter and increases only if R2 increases sufficiently to offset the opposite effect by including several variables.
However, illness beliefs as well as beliefs about rehabilitation predict short-term outcome, even if other relevant variables whose predictive significance has been proven for the course of depressive conditions are taken into consideration. The result that in the short term, illness identity predicts better physical functioning may be surprising. This may possibly be explained by the fact that patients who ascribe many symptoms to depression at the start of rehabilitation have a greater chance of experiencing improvement in many areas during treatment, which may have a positive impact on the assessment of physical functioning. In the medium term, the predictive power of illness beliefs and treatment beliefs increases; the corrected explanation of variance can be increased by up to 19% by including illness beliefs and treatment beliefs about all outcome criteria. With respect to treatment beliefs, psychological outcome expectations are associated with better health status, while somatic outcome expectations and rehabilitation-specific concerns predict worse health status in the follow-up. For illness beliefs, identity, timeline, personal control, treatment control, and coherence are significant predictors of health status in the middle term. With respect to role emotional, beta-co-efficients of the identity scale and the coherence scale are even larger than the beta-coefficient of baseline health status. Overall, the results show a tendency similar to the study by Horn et al. (2010), which also showed the relevance of perceived consequences and treatment control for the course of depressive symptomatology and of perceived personal control, treatment control, and coherence for the course of a positive affect for depressive patients. However, they did not adjust for other potential predictors.
On the one hand, the findings highlight the significance of illness beliefs and treatment beliefs in patients with depressive disorders. On the other hand – as Fortune et al. (2004) point out – it may be argued that investigating illness beliefs in people with depression might be less relevant because mood may influence illness and treatment beliefs and therefore depression and cognitive illness models may interfere with each other. However, we agree with them that even if mood does influence the patient’s beliefs, this does not make it less likely that the beliefs will also influence the patient’s behavior such as adherence or help seeking. Furthermore, illness beliefs of depressed people are not necessarily more pessimistic than illness beliefs of persons without a history of depression (Vollmann et al., 2010). And finally, our results showed that illness beliefs are predictors of depressive burden, even if the baseline values of the depressive symptomatology is controlled for. They thus make a specific predictive contribution to the depressive burden which goes beyond the depressive symptomatology.
Limitations
One limitation of the study is related to the representativity of the sample. Only 44% of the patients who were addressed before the start of rehabilitation were included in the study and it is conceivable that the more severely affected patients decided against participating in the study. However, as the non-responders did not give their consent to having their data analyzed, it is not possible to conduct a non-responder analysis. Both at the end of rehabilitation as well as at the follow-up, the response rate was relatively high. However, patients who dropped out of the study at follow-up were about seven years younger than responders, which further limits the generalizability to the initial sample. Moreover, not all variables whose influence on the course of depression is known were measured. In addition to the variables included, future studies could also take the number of prior depressive episodes or comorbid personality disorders into consideration as predictors.
In view of the fact that multimodal therapy concepts such as those offered in psychosomatic rehabilitation have a major significance in treating patients with depressive disorders, treatment beliefs were conceptualized as beliefs about rehabilitation. Beliefs about medicines were also measured. However, the sample of those who took medication to treat depression was too small to allow the beliefs about medicines to be included in the regression models. Since the medication therapy presents a relevant strategy for treating depressive disorders, the parallel consideration of beliefs about medicines and beliefs about rehabilitations might be the subject of further research, which would make it necessary to have a larger sample. Finally, the number of regressions carried out needs to be taken into consideration. Since the subscales of SF-36 and the ADS were used as indicators of outcome, alpha error inflation cannot be ruled out. Therefore, the weaker but significant beta values in particular may be chance findings and should be interpreted with caution.
Clinical implications
With respect to the clinical implication of our results, illness beliefs and beliefs about rehabilitation provide concrete starting points for designing therapeutic interventions which aim for modifying dysfunctional cognitive (illness-related) schemas in depression. In addition, according to Fortune et al. (2004), an important application might be in understanding people’s treatment preferences and – by developing adequate illness beliefs – in supporting the selection of an adequate treatment option. In the context of chronic somatic diseases, interventions, which are guided by the CSM, are promising (Broadbent et al., 2009; Glattacker et al., in press; Jansen et al., 2011; Lee et al., 2011). Future studies should aim to implement these efforts into the context of mental illnesses as well.
Conclusion
Using the extended CSM as a theoretical basis, applying a longitudinal design, and adjusting for a range of sociodemographic and medical predictors, we showed that illness beliefs and treatment beliefs make a specific predictive contribution to the short and middle term outcome in depression. With this in mind, in this patient group as well, patients’ representations about illness and treatment provide concrete starting points for designing patient-oriented interventions.
Footnotes
Acknowledgements
The project ‘Bedarfsgerechte Patienteninformation auf der Basis subjektiver Konzepte’ (Individualized patient information following patient’s illness beliefs and treatment beliefs in the context of rehabilitation) is funded by the German Pension Insurance in the funding priority ‘Versorgungsnahe Forschung’ (Patient-oriented Research). We would like to thank the funders, the cooperating centers Rehabilitationsklinik Frankenhausen DRV-Bund, Bad Frankenhausen; Rehabilitationsklinik ‘Garder See’, Lohmen; Klinik am Homberg, Bad Wildungen; DE’IGNIS Fachklinik GmbH, Egenhausen; Psychosomatische Fachklinik Schömberg, Schömberg and the participating patients.
Competing Interests
None declared.