
Abstract
The aim of this study was to examine the relation between the public perceptions and reactions to the pandemic influenza A(H1N1) in Crete, Greece. It was conducted in two phases: at the early phase of the outbreak and during the peak. The Common Sense Model was used as an appropriate theoretical framework. Participants were 273 healthy adults. Perceptions, especially perceived control and emotions, were related to protective behaviours, infection management behaviours and detachment at both phases of the study and also predicted follow-up reactions. Moreover, emotions predicted changes in behaviour and moderated the effects of several perceptions on pandemic-related behaviour.
The outbreak of an epidemic or even a pandemic influenza is a rather common phenomenon in human history. Just during the previous century, five influenza pandemics have been recorded (Patterson, 1985). Also, two influenza epidemics were recognized as global threats in 2003–2004 (WHO, 2008). Very recently, a new epidemic, influenza A(H1N1) or ‘swine’ influenza, broke out in spring 2009 in Mexico and by June 2009, the World Health Organization had declared it a global pandemic (WHO, 2010). The outbreak of an influenza epidemic or pandemic typically represents a serious challenge for health care services and may have a significant psychological and economic impact (Blendon et al., 2004). Thus, the investigation of the factors that are involved in the epidemic-related attitudes and behaviour is important in order to understand public response in such conditions, improve containment and preventive measures (ie, decrease infection rates, transmission and disease severity), as well as examine the validity of relevant psychosocial models.
Existing research on influenza outbreak has shown that a significant proportion of the population (about 20–35%) worries about being a victim or about a family member contracting the virus (eg, Lau et al, 2009; Wong and Sam, 2011). However, these reactions seem to decline over time and be sensitive to media reports (Jones and Salathé, 2009; Leung et al., 2005). Generally, however, most people carry out several preventive (eg, hand washing, vaccination), avoidant (eg, avoiding public places) or management of disease behaviours (eg, taking antiviral medication) after an epidemic outbreak in order to get protected (Bish and Michie, 2010).
In most studies, perceptions such as perceived susceptibility to, and perceived severity of, contracting the influenza virus have been found to significantly predict the adoption of preventive and avoidant behaviours (Bish and Michie, 2010; Sypsa et al., 2009; Tang and Wong, 2004). Also, perceptions of risk and severity have been related to the reported levels of anxiety and fear (Leung et al., 2005), which in turn have been associated with more intense behavioural responses (Bish and Michie, 2010; Leung et al., 2005). However, relevant research is faced with certain shortcomings: most studies are cross-sectional, most studies have been carried out in Asia and their findings may not be generalizable to Western populations and many studies lack an explicit theoretical framework (Bish and Michie, 2010). Furthermore, epidemic-related research is usually constricted to cognitive judgments about risk (eg, perceived likelihood of contracting the virus), and pays little attention to the significant role of emotions in decision making and the prediction of health behaviours (Bish and Michie, 2010; Leppin and Aro, 2009).
The purpose of this study was to examine the relations of perceptions about the recent pandemic influenza A(H1N1) to relevant reactions. Moreover, the study aimed at overcoming certain shortcomings of previous research: the cross-sectional design, the lack of a clear theoretical background and the infrequent examination of the role of emotions. To the first end, we used a simple prospective design and examined the perceptions – reactions relation at two periods of the pandemic. To the second and third end, we employed the Common Sense Model (CSM) of illness representations (Leventhal et al., 1980; 1992) as a suitable theoretical framework. We employed the CSM for two main reasons. First, it provides the appropriate framework for understanding the cognitive and emotional factors that influence adaptation to a health threat and has frequently been employed in the study of illness (Hagger and Orbell, 2003). Second, it emphasizes the role of emotions as an integral part of the self-regulation process regarding health threats. Yet, contracting an influenza virus represents only a possibility and the perception of this possibility may be important for the overall understanding of the condition. Therefore, besides perceptions included in the CSM, we also examined the role of perceived susceptibility to the pandemic. Perceived susceptibility has repeatedly been related to influenza-related behaviours (Bish and Michie, 2010).
In summary, the specific hypotheses of this study were: (a) perceptions about the pandemic influenza A(H1N1) are related to reactions at both phases of the study (ie, at the early phases of the pandemic outbreak, as well as during the peak). We hypothesized that a perception of the pandemic as more controllable, severe or fearsome is associated with the adoption of more protective behaviours; (b) baseline perceptions can predict follow-up behaviours, as well as changes in behaviour. As previously, we expected a perception of the pandemic as more controllable, severe or fearsome to predict the adoption of more protective behaviours; and (c) provided that the cognitive and the emotional processing of the pandemic outbreak are inter-related, as suggested by the CSM, we expected emotions to interact with perceptions in their relation to pandemic-related behaviours. Specifically, we expected the relations between perceptions and protective behaviours to be stronger at the higher levels of negative emotions (ie, we expected that participants would adopt more measures when feeling fear but also more in control or more susceptible to an infection, etc).
All relations were examined after controlling for gender, age, marital status, educational level and overall personal health as there is evidence that these factors impact responses to epidemic influenza outbreaks (Bish and Michie, 2010; Leppin and Aro, 2009).
Method
Participants and procedure
A convenience community sample of 273 healthy adults from Rethymnon, Crete, participated in the two phases of the study. They were recruited during a visit of a research assistant at their homes. In the first phase of the study, 318 persons participated. However, 45 refused to participate or were not located by the research assistants in the second phase. Thus, statistical analyses were performed using data from 273 participants (119 males; 154 females) who completed questionnaires at both time points. There were no significant differences concerning gender, age, marital status and education level between those who participated at both times and those who did not. The participants’ mean age was 37.53 years (SD=12.25). Most (81.10%) were living with their family or partners/friends; 18.90 percent were living alone. Also, 16.80 percent had finished the 9-year mandatory education, 53.80 percent had finished high school and 29.40 percent were holders of a higher education degree.
The first phase of the study was conducted during the first two weeks of October 2009, while the second phase was conducted four months later, during the first two weeks of February 2010. According to KEELPNO (Hellenic Center for Disease Control and Prevention, 2010), the first A(H1N1) virus infection cases in Greece were reported in May 2009. The ‘bulge’ of infection cases in Greece begun in November, peaked in December 2009 and again in March 2010 and weakened at late March. No new case was recorded after the middle of May until October 2010. Across the country, 18230 laboratory-confirmed cases and 149 deaths were reported by May 2010; 2196 cases were reported in the island of Crete, as well as seven deaths. From October 2009 to May 2010, almost all laboratory-confirmed influenza cases (98.8%) were infected by the A(H1N1) virus, suggesting that almost all influenza cases, even those that were not laboratory tested, had contracted the A(H1N1) virus.
Measures
Pandemic-related perceptions
In order to assess perceptions about the pandemic influenza, we employed a single-item approach, similar to the method used in the Brief Illness Perception Questionnaire (Broadbent et al., 2006), which assesses illness-related perceptions according to the CSM. Participants were asked to reply to the following questions using a Likert-type scale ranging from 0 (not at all) to 10 (very much/very well): ‘how much do you feel that your life would be affected in case you got infected by the pandemic influenza virus?’ (possible consequences); ‘how much do you feel that the protective measures you are taking, if any, can protect from getting infected?’ (control); ‘how well do you feel that you know what the new pandemic influenza is and what the symptoms are?’ (identity); ‘how much does the possibility of contracting the influenza virus affect you emotionally (eg, make you feel afraid or scared)?’ (emotion); ‘how long do you think that getting ill from the pandemic influenza and relevant consequences last?’ (timeline). However, the last question was omitted from the analyses due to extreme skewness (almost 85% of the participants reported values equal or lower to 3). Besides perceptions derived from the CSM, perceived susceptibility was also assessed with a single question: ‘how possible is for you to contract the pandemic influenza virus?’ Pandemic-related perceptions were assessed at baseline and follow-up. 1
Epidemic-related reactions
In order to assess reactions related to the pandemic outbreak, participants were asked to respond to 21 questions regarding possible ways of dealing with the pandemic and the infection risk. The items were derived from existing research on influenza outbreaks (eg, avoid public places, wash hands regularly), as well as from research on coping with distressing situations (eg, information seeking or avoidance). A principal component analysis with varimax rotation revealed three clear factors that explained 58.27 percent of the total variance. The first factor, ‘protective behaviours’, includes preventive and avoidant behaviours (eight items, eg, wash hands regularly, avoid crowds, get information from the internet and the press, ask my doctor for guidelines; 30.92% of the variance, eigenvalue=5.40, Cronbach’s α=.87 at both baseline and follow-up). The second factor, ‘infection management behaviours’, included four items referring to possible behaviours in case of an infection (eg, avoid contacting other people, in case I felt unwell; take antiviral medications, in case I felt unwell; 18.07% of the variance, eigenvalue=1.85, Cronbach’s α=.74 at baseline and .75 at follow-up). The third factor, ‘detachment’, consists of three behaviours that refer to the avoidance of carrying out any specific behaviour (eg, not considered it as a big issue, think of more pleasant issues; 10.38% of the variance, eigenvalue=1.44, Cronbach’s α=.62 at baseline and .65 at follow-up). Participants were asked to reply to the items by using a frequency Likert-type scale ranging from 1 (not at all) to 5 (very much).
Self-rated health
A single item was used to measure overall personal health. Participants were asked to rate their current overall health on a Likert-type scale ranging from 1 (bad health) to 5 (excellent health). Self-rated health was assessed at baseline and was used as a covariate in the statistical analyses.
Results
Table 1 presents the correlations between perceptions and reactions at both phases of the study. Most perceptions were positively related to protective behaviours and infection management behaviours. On the other hand, detachment was related only to control in a positive way and negatively to perceived susceptibility at baseline, and not to any perception at follow-up. Perception of control and emotions presented the higher correlations with reactions at both phases, while possible consequences were strongly associated with protective and infection management behaviours at follow-up. Several baseline perceptions were associated with follow-up behaviours, with emotions presenting the stronger correlations.
Descriptive statistics and intercorrelations of pandemic–related perceptions and reactions at both phases of the study (N = 273)
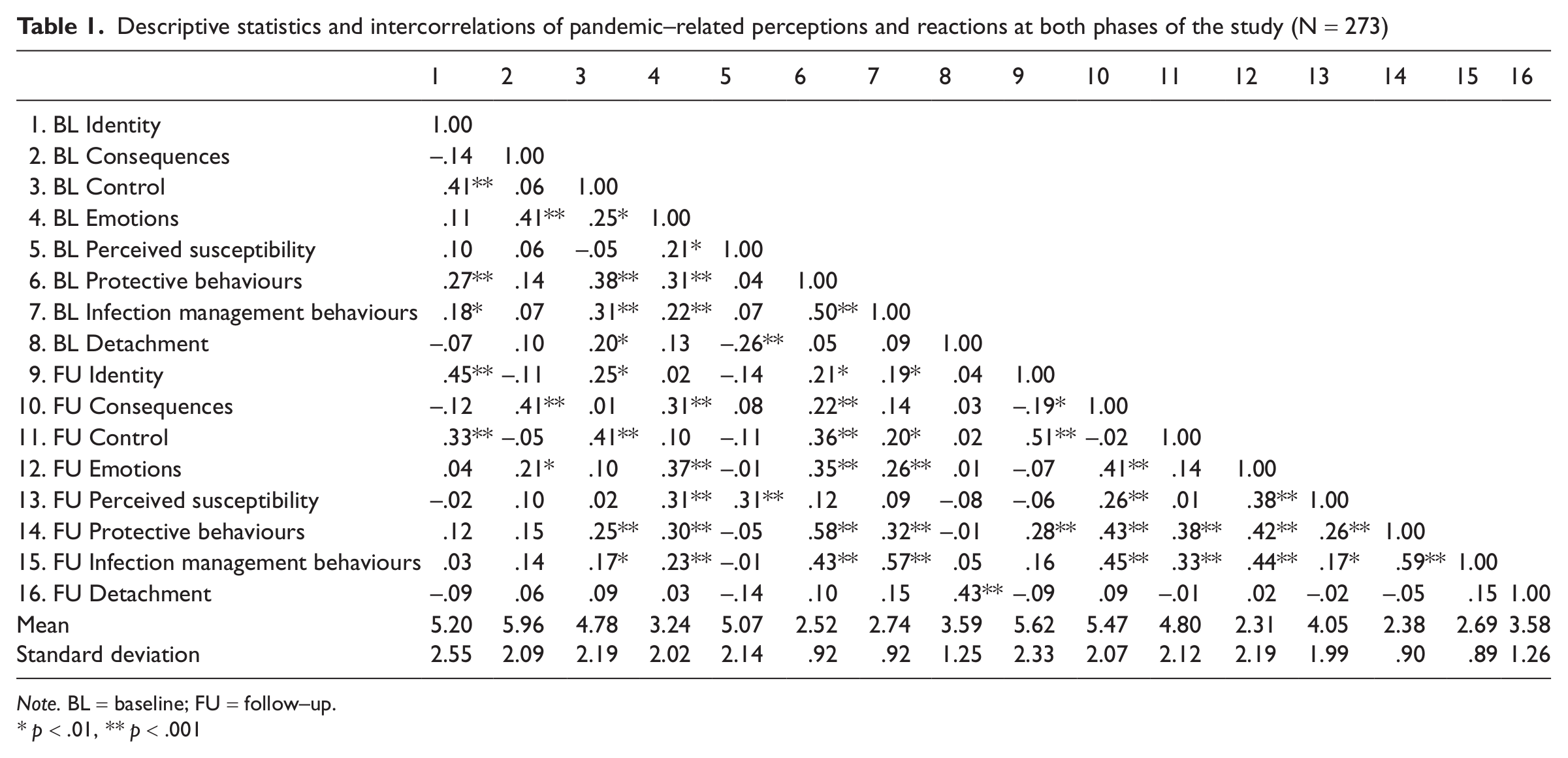
Note. BL = baseline; FU = follow–up.
p < .01, ** p < .001
A series of paired-t test analyses revealed that perceived susceptibility, possible consequences and emotions, as well as protective behaviours, were reduced at follow-up [ts(272)=2.62 – 9.65, ps<.01], whereas perception of control was increased [t(272)=-2.74, p<.01]. No other differences were observed. At both phases, detachment was the most frequent reaction.
At the early phases of the outbreak, perceptions were associated with reactions, even after controlling for demographic variables and overall health. Protective behaviours [R2 change =.18, F change (5, 263)=12.30, p<.001] were significantly associated with the perception of control and emotions (β=.24 and .22, t=3.81 and 3.38, respectively, ps<.001); infection management behaviours [R2 change =.09, F change (5, 263)=5.69, p<.001] were related to the same variables (β=.23 and .13, t=3.42 and 1.99, p<.001 and .05, respectively); and detachment [R2 change =.15, F change (5, 263)=8.88, p<.001] was related to perception of control and perceived susceptibility (β=.19 and −.30, t=2.84 and −4.75, respectively, ps<.01). Compared to baseline, at follow-up perceptions explained more of the protective and infection management behaviours variance. Identity, consequences, control and emotions were positively associated with protective behaviours [βs=.21–.37, ts=3.81–7.20, ps<.001; R2 change =.40, F change (5, 263)=37.67, p<.001]. Possible consequences, control and emotions were positively associated with infection management behaviours [βs=.24–.37, ts=4.25–6.84, ps<.001; R2 change =.36, F change (5, 263)=30.66, p<.001]; no perception was, however, related to detachment [βs<.08, ts<1.20, ps>.05; R2 change =.02, F change (5, 263)=.76, p>.05].
Prospectively, even after controlling for covariates, certain baseline perceptions predicted follow-up reactions [R2schange =.05–.14, Fschange (5, 263)=2.42–8.41, ps<.05] (see Table 2). Emotions predicted protective and infection management behaviours in a positive way; perceived control predicted protective behaviours in a positive way, whereas identity predicted detachment negatively. Regarding the ability of the baseline perceptions to predict changes in the pandemic-related reactions, negative emotions were the only ones that significantly predicted changes; even after controlling for baseline reactions, as well as covariates, emotions predicted follow-up protective (β=.21, t=2.98, p<.01) and infection management behaviours (β=.19, t=2.67, p<.01) in a positive way. That is, higher levels of negative emotions at baseline were associated with an increase in protective and infection management behaviours. None of the baseline perceptions predicted changes in detachment (see Table 2).
Summary of hierarchical regression analyses for baseline perceptions predicting follow–up and changes in pandemic–related reactions (N=273)
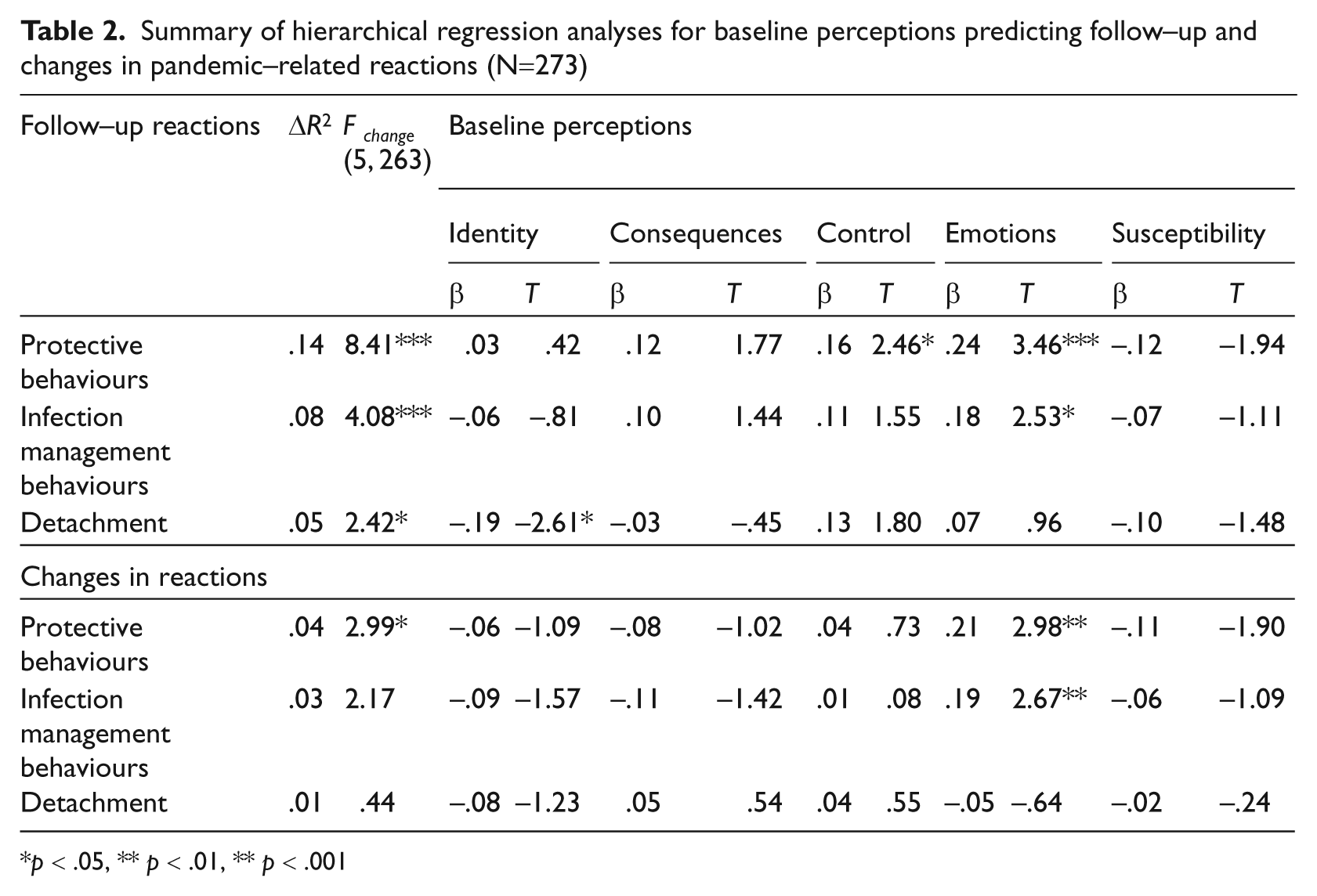
p < .05, ** p < .01, ** p < .001
To examine whether emotions interact with perceptions, we used MODPROBE, a computational aide for SPSS for probing interactions (moderations) developed by Hayes and Matthes (2009). MODPROBE, in addition to estimating interaction effects, produces tests of the conditional effect of the independent variable on the dependent at specific values of the moderator (by default, at mean, one standard deviation (SD) above the mean and one SD below the mean), as well as controls for covariates.
At baseline, statistically significant moderation effects of emotions, after controlling for demographic variables and overall health, were identified for the relations of perceived control (B=−.06, t=−2.73, p<.01) and perceived susceptibility (B=.06, t=2.49, p<.05) to detachment. Conditional effects at specific values of the moderator for the statistically significant interactions are presented in Table 3. At higher levels of emotions, there was no relation between perceived control or perceived susceptibility and detachment. At follow-up, no significant interaction was noticed (ts<1.80, ps>.05). Prospectively, statistically significant moderation effects of baseline emotions, after controlling for covariates, were identified for the relation of baseline identity to follow-up preventive behaviours (B=−.10, t=−1.96, p<.05), for the relations of baseline perceived susceptibility to follow-up infection management behaviours (B=.11, t=4.19, p<.001), and to follow-up detachment (B=.10, t=4.18, p<.001). As presented in Table 3, these relations were not statistically significant at the higher levels of emotions.
Conditional effects (B–values; t–values in parentheses) of pandemic–related perceptions on reactions at specific values of emotions and confidence intervals
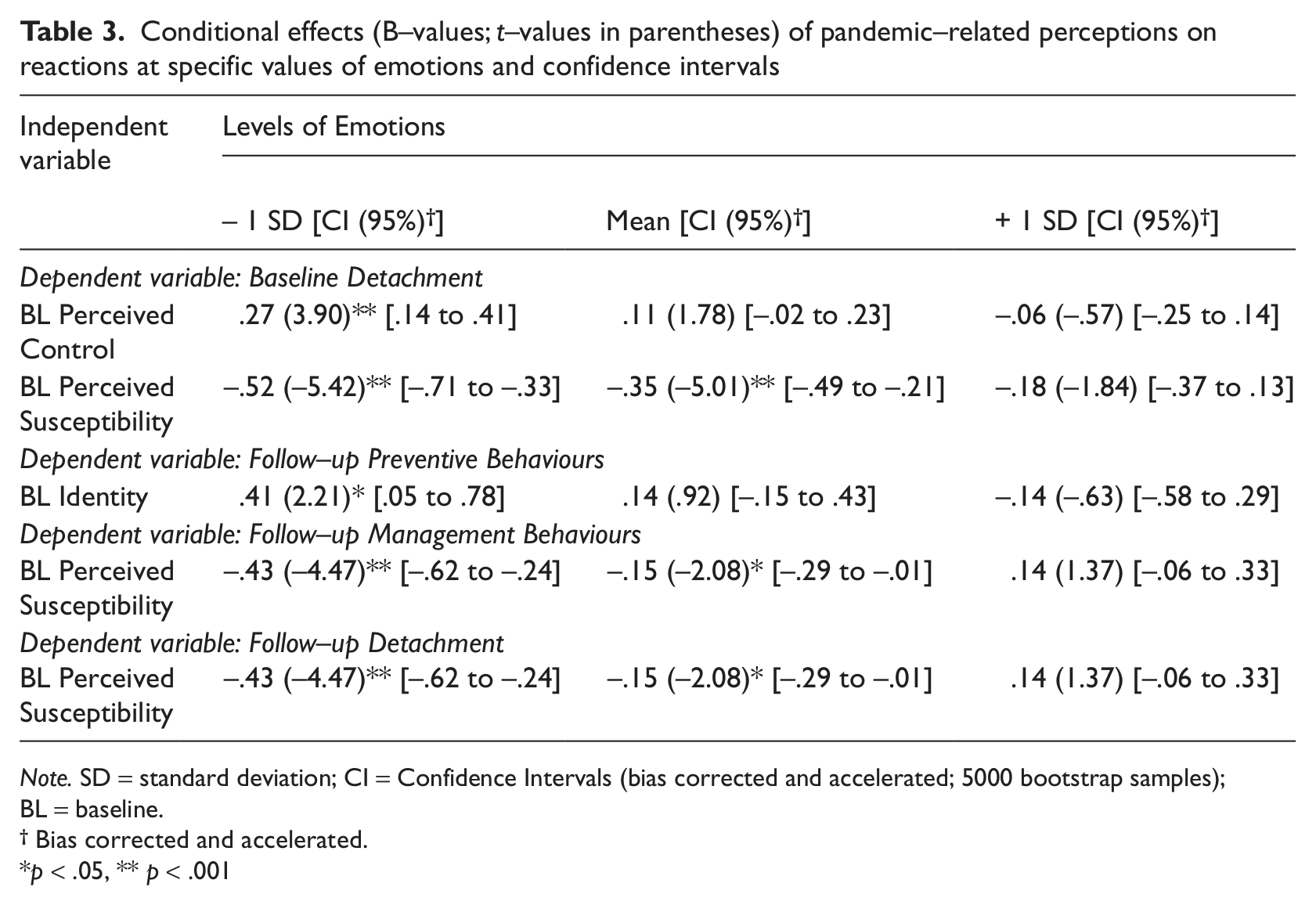
Note. SD = standard deviation; CI = Confidence Intervals (bias corrected and accelerated; 5000 bootstrap samples);
BL = baseline.
Bias corrected and accelerated.
p < .05, ** p < .001
Discussion
The purpose of this study was to examine the relation between public perceptions and reactions during the outbreak of the pandemic influenza A(H1N1) by using the CSM of illness representations (Leventhal et al., 1980) as a theoretical framework. The study was conducted in two periods: at the early phases of the outbreak in Crete, Greece (early October 2009) and during the peak (early February 2010). This provided the opportunity to examine the perceptions – reactions associations at two different periods of the outbreak, as well as whether baseline perceptions predict follow-up reactions and corresponding changes in behaviour.
According to the results, perceptions were related to reactions at both phases of the study, even after controlling for demographic variables and overall health. Existing research has already shown that epidemic influenza perceptions, such as perceived severity, are related to behaviour (Bish and Michie, 2010). In addition, our study showed that baseline perceptions can predict future pandemic-related reactions, as well as that negative emotions can predict changes in these behaviours, indicating thus a continuity of the pandemic perceptions – behaviours relation over time.
Although several perceptions in this study were associated with reactions, including identity and possible consequences, it is noteworthy that the perception of control and negative emotions (ie, fear) were the two factors more frequently and strongly associated with reactions. As hypothesized, the perception of a fearsome or of a controllable condition was (concurrently and prospectively) associated with the adoption of more primary and secondary prevention measures (ie, protective and infection management behaviours). The role of control in determining behaviour has been stressed in several theories about health behaviour (Bandura, 1997; Leventhal et al., 1980) and demonstrated in numerous studies (Helgeson, 1992; Litt, 1988; Tennen and Affleck, 2000). Also, existing research, although restricted, shows that emotions are important regarding epidemic-related behaviour (Bish and Michie, 2010; Leppin and Aro, 2009). Emotions are part of the decision making process and their impact on subsequent behaviour, especially in stressful conditions, is substantial (Joffe, 1996; Slovic, 1987). Moreover, Slovic (1987) suggests that laypersons conceptualize danger rather in terms of emotional responses to a negative situation.
Indeed, our findings indicate that emotions are a powerful predictor of reactions and changes in behaviour, as well as that they interact with perceptions and, therefore, can moderate their impact on reactions. In several cases, the relations of perceptions to reactions (at the first phase of the study, as well as prospectively) were weakened at the higher levels of emotions and not strengthened as hypothesized. In other words, the ‘perceptions-behaviours’ path seems to be interrupted when fear is high: when people are afraid, reactions tend to be intense irrespectively of other perceptions. This suggests that emotions may have a ‘primacy’ as far as the epidemic response is concerned. Yet, most relevant studies do not include measures of emotions or they centre on worry, which refers to risk rather as cognition than as emotion (Leppin and Aro, 2009). Findings like the present underline the need to incorporate the assessment of emotional representations into the study of epidemic-related responses, and employ models that emphasize both cognitive and emotional processes.
A further interesting finding was that during the peak of the pandemic outbreak, participants reported a more ‘positive’ perception of the situation and the adoption of less protective behaviours. A decline in reactions over time has been reported in previous studies (Leung et al., 2005). However, this finding could also reflect the fact that the actual impact of the pandemic in Greece was far less intense than anticipated (eg, it had no particular effect on young persons and children and the death rate was not really higher than the typical for seasonal influenza; MMWR, 2010). Also, during the peak, perceptions were more closely related to protective and infection management behaviours than at the earlier phases of the outbreak. Such findings imply that perceptions, reactions and their relationships may change over the course of an epidemic influenza outbreak and may depend on several factors. Therefore, findings regarding public response at one epidemic phase may not apply to another. Prospective studies that will examine the psychosocial impact of epidemic influenza at different phases of the outbreak are needed to clarify this issue.
A final finding should be highlighted. This refers to detachment, which was revealed from the factor analysis of the pandemic-related reactions. Detachment, or the avoidance of carrying out any preventive or management action, has not been considered in research about epidemics, although it seems to be a plausible reaction. According to our findings, a more positive perception of the pandemic (ie, higher levels of perceived control, lower levels of perceived susceptibility) was related to more detachment, but only when the level of emotions was moderate or low (as shown by the moderation analyses). In other words, detachment was associated with a feeling that the situation is not fearsome and, at the same time, the risk of infection is low or it can be managed. In fact, detachment seems to reflect a perception of the situation like ‘nothing is at stake, no need to take any measures’. It is a question, however, whether such a response reflects a corresponding ‘true’ representation or a defensive process (eg, denial). Moreover, as reported by participants, detachment was the most frequent reaction at both phases of the study. Therefore, we believe this is an important issue that should be further examined in future studies.
This study does have some limitations. We employed a one-item approach to assess pandemic perceptions, which is a significant limitation; the outbreak of influenza A(H1N1) may not represent a typical example of pandemic, as it was anticipated to have a large impact on public health but was soon realized that this was not the case (as least as far as Greece is concerned); the findings were based on self-reported data; our sample was a convenience one and coming from only one part of the country. On the other hand, however, our study employed a specific theoretical background to assess pandemic perceptions (ie, the CSM), focused on emotions and assessed perceptions and reactions prospectively.
During the outbreak of an epidemic or pandemic, the focus of the health services and the authorities is usually on the identification of the pathogenic agent, and the successful prevention and treatment. Yet, the effective implementation of preventive and containment measures ultimately depends on public response. Therefore, the examination of epidemic or pandemic perceptions and behaviours, as well as of the related factors, is crucial. In this context, our study provided some evidence that: perception of control and, especially, emotions seem to play a central role in public response to an epidemic outbreak; emotions interact with perceptions suggesting that the cognitive-analytic and the emotional-experiential systems are intertwined and may depend on each other for guidance, as proposed by Slovic (1987); the CSM of illness representations provides a valid framework for examining epidemic perceptions and their relation to subsequent reactions, as it emphasizes both cognitive and emotional processes.
We believe that our findings are important for both theory (ie, the development of more accurate models regarding risk perception and response) and practice. For example, in order to decrease avoidant and increase preventive behaviours at the early stages of an epidemic outbreak, an intervention programme could generally focus on: (i) the enhancement of a public sense of control by indicating specific (yet, simple and, where possible, tailored to the needs and practices of the public) behaviours as capable of preventing/stopping contamination; and (ii) raising personal concern by means of detailing the dangers towards self and others that are inherent in avoidance behaviours. In other words, through emotional arousal and the parallel use of suggestions about suitable and easy to implement ways of coping with the situation (such as hand washing), public health services could increase the use of preventive behaviours. However, these are just some indicative suggestions based on our findings. Future research that will focus on the emotional representation of risk, as well as on the interplay between the cognitive-analytic and the emotional-experiential processes, will provide us with further knowledge about the most efficient ways of enhancing the adoption of containment behaviours in the different phases of an epidemic outbreak.