
Abstract
The objective of the present article is to identify predictors of willingness to participate (WTP) in microbicide trials among African Americans. A total of 595 participants completed a survey on WTP in microbicide trials and predictors of WTP. Significant associations were observed for relationships of greater WTP with female gender, greater HIV risk, lower mistrust of research, and knowing someone with HIV/AIDS. An interaction revealed HIV risk was positively associated with WTP for women only. Accurate knowledge of the Tuskegee Syphilis Study was associated with greater WTP. These predictors may be employed in microbicide trials to enhance African American participation.
HIV/AIDS continues to be a major public health concern in the United States. The epidemic has a disproportionate impact on African Americans, who accounted for 13% of the US population and 51% of all new HIV/AIDS diagnoses in 2007 (Centers for Disease Control and Prevention (CDC), 2009). Of the new HIV/AIDS cases with known cause for African Americans, men who have sex with men (MSM) comprised 51% (CDC, 2009). Heterosexual contact resulted in 20% of cases among men and 75% of cases among women (CDC, 2009). Effective prophylaxis (e.g. microbicides) against HIV transmission that can be managed and controlled by the receptive sex partner (e.g. women, MSM) could significantly reduce sexual transmission of HIV. Although clinical trials investigating microbicides are underway, little is known about African Americans’ willingness to participate (WTP) in these trials. Difficulties recruiting individuals of ethnic and racial minority status in medical and behavioral medicine research can result in samples that are too small for conventional analyses, limit conclusions drawn from studies, and diminish the ability to improve health services for minority populations. The present article examines WTP in HIV prevention research, specifically studies of microbicides.
Microbicides are topical products applied by the receptive partner to vaginal or rectal mucosal surfaces to prevent or significantly reduce the transmission of HIV and other sexually transmitted infections (STIs) (Anderson et al., 2010; McGowan, 2006). Although the first generation of surfactant and polyanionic microbicide candidates were not efficacious in preventing HIV infection, the development of effective and acceptable microbicide products remains a key priority in HIV prevention (Morris and Lacey, 2010). Recently, potent antiretroviral agents and entry inhibitors have emerged as promising second-generation HIV microbicide candidates (McGowan, 2010; Morris and Lacey, 2010). It is essential that clinical trials involving these microbicide candidates utilize a racially diverse sample to ensure generalizability of research findings across different racial groups. A phase III HIV vaccine efficacy trial demonstrated the challenge of obtaining racial diversity in clinical trials, and how a lack of diversity can complicate and limit interpretation of research findings (Cohen, 2003). Microbicide trials may also face challenges with regard to enrolling racially diverse study samples. The willingness of African Americans to participate in microbicide trials, as well as the facilitators and barriers associated with WTP are not fully understood.
Despite the importance of minority group enrollment in clinical trials, African Americans have been historically underrepresented in medical and behavioral medicine research (Adams-Campbell et al., 2004; Corbie-Smith et al., 1999). The most cited reason for this underrepresentation is the legacy of mistrust stemming from the Tuskegee Study of Untreated Syphilis, which symbolizes ethical misconduct in clinical research. While many African Americans are clear that there was a violation of human rights in the Tuskegee study, many are misinformed about the historical facts of the study (Corbie-Smith et al., 1999). Thus, accurate knowledge of the Tuskegee study may be an important predictor of WTP. Other factors that may be associated with lack of enrollment by African Americans may include limited access and utilization of health care, racial disparities in service delivery, economic disadvantage, participant incentives, schedule conflict/role overload (serving in multiple social or occupational roles), and religious beliefs or health-related concerns associated with research (Sengupta et al., 2000; Shavers et al., 2002). Limited medical access and low socioeconomic status (SES) can result in greater WTP when a study is perceived as providing access to potentially valuable resources for care or other tangible incentives (Napoles-Springer et al., 2000). However, when an individual has accepted multiple social, occupational, and/or educational roles, role overload could serve as a barrier to WTP (Kibler and Brisco, 2006).
Within the context of HIV/AIDS, insufficient minority representation in HIV prevention research and HIV/AIDS clinical trials has been well documented, with white males constituting the majority of research participants (Gifford, 2002; Newman et al., 2006). The preponderance of male participants in HIV prevention research reflects efforts to reduce HIV transmission among gay men. However, women at risk for HIV may have high WTP in HIV prevention research (Etcheverry et al., 2010). Much of the research on WTP in HIV prevention trials has focused on HIV vaccines (Buchbinder et al., 2004; Frew et al., 2010; Pridy et al., 2006). In addition to the predictors discussed above, these studies have reported that greater perceived HIV risk, positive attitudes toward HIV vaccine research, favorable health beliefs, social support for participation, and injection drug use are associated with greater WTP in vaccine trials for African Americans. Research also suggests that knowing someone with HIV/AIDS may enhance WTP in HIV prevention trials (Crumbo et al., 1997). Another potential predictor of WTP is HIV stigma, as fear of stigmatization for at-risk individuals would be inconsistent with the positive effects of social support for participation (Moutsiakis and Chin, 2007). Correlates of WTP in HIV vaccine trials may not translate to other HIV prevention approaches. Microbicides may have particular appeal for women due to the emphasis on protection for the receptive partner (Morris and Lacey, 2010).
To identify predictors of WTP in microbicide trials, we conducted a cross-sectional survey among African Americans in the southern USA – a region with pronounced disparity in HIV incidence between African Americans and other racial/ethnic groups (Henry J. Kaiser Family Foundation, 2002). To involve populations who may benefit most from microbicides, the present study oversampled high-risk women (e.g. drug users, individuals engaging in high-risk sex) and MSM. Because data are lacking regarding acceptability of microbicide use for men, heterosexual men were also included in the sample. The purpose of the current study was to assess barriers and facilitators for WTP in hypothetical research of a microbicidal gel among African Americans with varying degrees of HIV risk.
Methods
Participants
A total of 595 African American adults were enrolled from three groups with varying degrees of HIV risk: (1) heterosexual men; (2) heterosexual women; and (3) MSM. Individuals were eligible for participation if they were between the ages of 18 and 70, HIV seronegative, and free of medical conditions (e.g. cancer, active liver disease) that may preclude them from participating in preventative biomedical intervention trials. Interviews were conducted to determine study eligibility. Women at increased HIV risk were over-sampled. Participants were classified as high-risk if they had engaged in at least one of the following activities in the past three months: (1) sex with three or more partners without consistent condom use; (2) sex partner had HIV, STI, or injected drugs; (3) exchanged sex for money, drugs, shelter, etc. (4) injected drugs or smoked crack cocaine; or (5) had an STI. Women were also considered high-risk if they had protected or unprotected sex with a recently incarcerated man in the past three months. All participants completed an informed consent. The study was conducted in accordance with the US Department of Health and Human Services and University Institutional Review Board guidelines for human experimentation.
Recruitment
Convenience sampling was used for enrollment. Participants were recruited from organizations and businesses serving African American clientele (e.g. beauty salons, barbershops, health care clinics) in an urban setting in the southern USA. To over-sample women at-risk for HIV infection, recruitment was extended to an STI clinic, drug rehabilitation centers, crack houses, and homeless shelters. To ensure an adequate sample of MSM, a night club frequented by MSM, and an MSM social organization also served as recruitment sites. Potential participants were approached by an African American female research associate and asked if they would be interested in completing a survey focusing on health-related issues such as sex, drug use, HIV, and participation in medical research. Interested individuals were provided additional information about the study and screened for eligibility using a brief standardized interviewer-administered computer-assisted screening instrument. Individuals meeting eligibility criteria completed the informed consent and were enrolled.
Study interview
The study interview was administered at the recruitment sites on tablet computers using Audio-Computer Assisted Self-Interview (ACASI) software (NOVA Research Systems, Questionnaire Development System). The interview was approximately 45 minutes in length. Prior to completing the interview, participants were oriented to the computer and ACASI software, and had any questions answered. Following a brief ACASI tutorial, participants completed the interview privately with a study staff member available nearby to answer questions. Upon completion, participants received an honorarium of $25.
Measures
The outcome measure for this study was WTP in microbicide trials. Participants were provided with basic information about microbicides and microbicide clinical trials and then asked how willing they would be to participate in a trial using a four-point ordinal response scale (1 = not at all, 2 = might be, 3 = probably, 4 = definitely). The independent measures included the following:
SES – questions on employment, income, and education.
Mistrust, health beliefs/fears, religious beliefs, incentives, and role overload – the Barriers to Research Participation Questionnaire (BRPQ) developed by Kibler and Brisco (2006) was used to assess mistrust toward researchers’ motives and government sponsorship of research, health beliefs/fears that could impact sentiments toward research, religious beliefs that may be inconsistent with participation in scientific research, incentives for participation, and role overload (the perception of serving in numerous social or occupational roles). Psychometric examination of the BRPQ indicated support for the five factors through confirmatory factor analysis, as well as good three-week test–retest reliability (r = .80) and marginal internal consistency (α = .63) in a sample of African American college students (Kibler and Brisco, 2006). In the present study, the internal consistency of the BRPQ was .75.
The BRPQ uses a five-point Likert-type scale (1 = ‘strongly agree’ to 5 = ‘strongly disagree’) for responses to all but one of the 17 items. The following are sample BRPQ items: ‘The government sometimes exposes participants to agents known to be harmful to one’s health’ (mistrust); ‘Research could provide information about my health that I would rather not know about’ (health beliefs/fears); ‘Illness and death are God’s will and are not necessarily affected by research’ (religious beliefs); ‘There isn’t anything for my community to gain by participating in research’ (incentives); and ‘It would be difficult to find time to participate in a research study’ (role overload). The instrument also includes the following question to assess role overload: ‘These roles sometimes occupy much of people’s time. Please indicate which roles apply to you by clicking on the appropriate boxes.’ The options include nine roles such as student or parent. Participants may also specify additional roles not on the list.
Awareness and knowledge of the Tuskegee Syphilis Study – a subset of questions from the Tuskegee Legacy Project Questionnaire developed by researchers from the Northeastern Minority Oral Health Research Center was used to assess awareness and accurate knowledge of the Tuskegee Syphilis Study (Katz et al., 2003). Sample questions from the measure include: ‘Have you ever heard of the Tuskegee Syphilis Study?’ (answered yes or no); ‘The study participants were injected with syphilis’ (answered true, false, don’t know); and ‘The study ended when penicillin was discovered as a cure for syphilis’ (answered true, false, don’t know).
HIV-related stigma
Additional questions were developed by the authors for this study, including: (a) Perceived access to medical care (‘Please click on the number that best shows your feelings about accessing the medical care that you need.’ Responses range from ‘I have all the medical care I need’ to ‘I have no access to medical care’); (b) HIV risk (questions on drug use, STI, sexual activities, HIV risk of sex partners, and exchange sex for money or drugs); and (c) Knowing someone with HIV/AIDS (‘Do you know anyone who is HIV positive but is not sick?’ and ‘Do you know anyone who has AIDS?’).
Data analyses
Chi-square tests of independence for categorical variables and one-way analysis of variance for continuous variables were utilized to compare groups on demographic variables. Because the dependent variable, WTP in microbicide trials, is an ordered response variable, ordinal regression analyses were utilized to assess the correlates of each independent variable to WTP in microbicide trials. Initially, the bivariate relationships of the covariates to WTP in microbicide trials were assessed by conducting separate ordinal regression analyses for each independent variable: demographic group; gender; HIV risk; knowledge of the Tuskegee Syphilis Study; SES; mistrust; health beliefs; religious beliefs; incentives; role overload; HIV stigma; access to health care; and knowing someone with HIV/AIDS. Independent variables that were significantly related to WTP in the bivariate analyses were retained for the multivariate analyses. To examine whether prediction by the independent variables differed by gender and HIV risk, the interaction of gender and HIV risk with each significant predictor was examined by entering each interaction term into an ordinal regression.
Results
Descriptive analyses
A total of 595 participants were enrolled: 126 heterosexual men, 317 heterosexual women, and 152 MSM. Demographic characteristics of the three study groups are presented in Table 1. Among the study samples, the MSM were significantly younger than the heterosexual men and women, F(2, 594) = 55.16, p < .01. More MSM endorsed ‘single’ as their marital status compared to the other two groups (p < .01). Significant differences were observed for SES among the three demographic groups, F(2, 594) = 18.32, p < .01, with women having lower SES scores compared to heterosexual men (p < .01) and MSM (p < .01). Higher HIV risk behavior was also associated with lower SES (p < .01). Due to the over-sampling of high-risk women, overall the women had significantly more HIV risk factors compared to the other two groups, p < .05.
Characteristics of the three demographic groups of African Americans
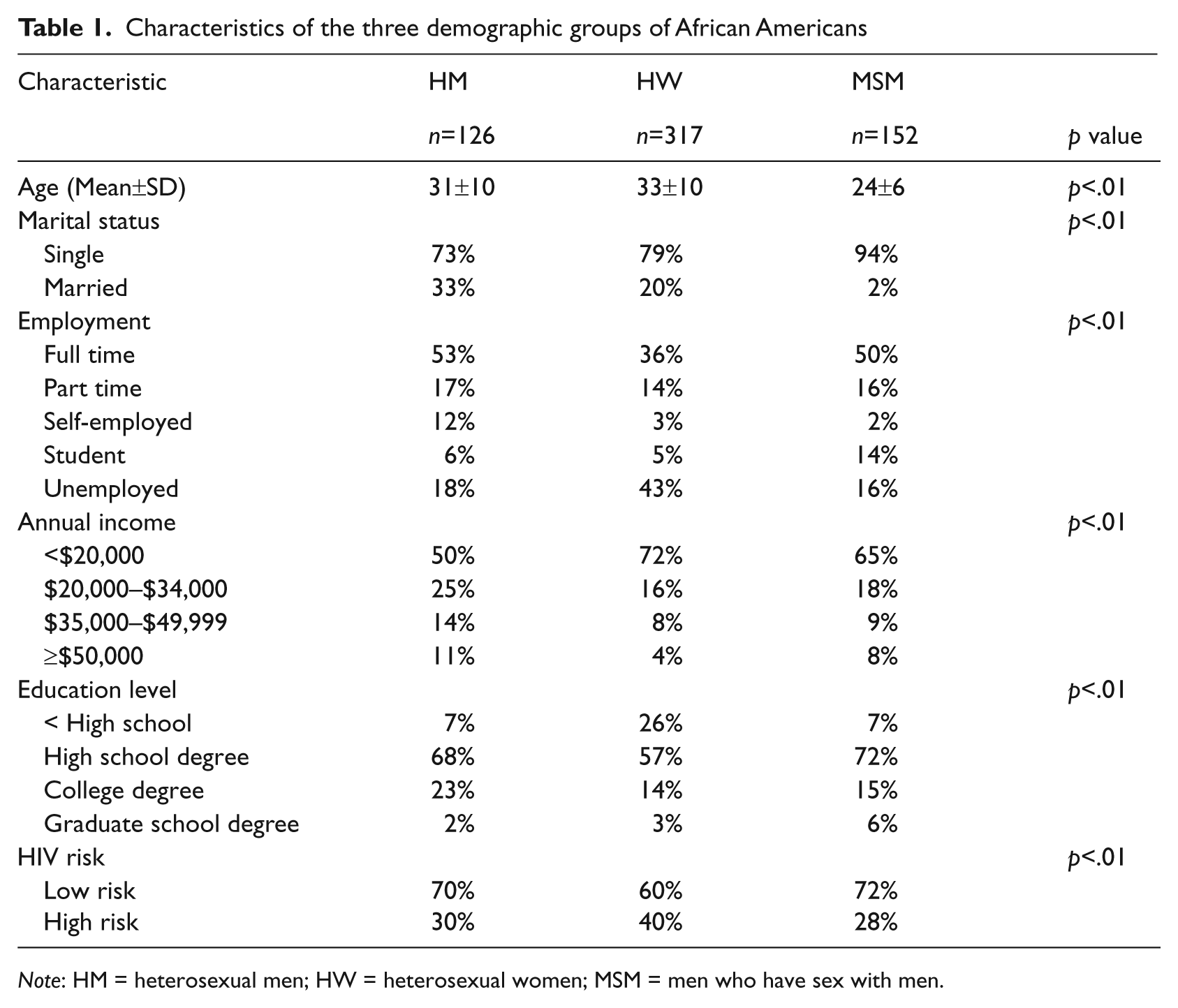
Note: HM = heterosexual men; HW = heterosexual women; MSM = men who have sex with men.
Forty-three percent of participants reported they were ‘not at all’ willing to participate in microbicide trials, 51% ‘might be’ or ‘probably’ would be willing to participate, and 6% were ‘definitely’ willing to participate. As presented in Table 2, 39% of participants had some awareness of the Tuskegee Syphilis Study. Participants who were aware of the study scored an average of 55 out of 100 points on questions to assess knowledge of the study’s historic facts. Based on the scores from the BRPQ mistrust and religious beliefs subscale, the average response was ‘neither agree nor disagree’ concerning mistrust of researchers and having religious beliefs that may be inconsistent with participation in scientific research. In general, participants ‘disagreed’ with items relating to health beliefs or fears that could serve as barriers to research participation, did not perceive personal or community incentives to research participation, and were not engaged in multiple social or occupational roles that may interfere with research participation. On average, participants reported having minimal stigmatizing attitude toward HIV-infected individuals and indicated they had good health care but not all the medical care that they needed. Sixty-one percent of the participants reported knowing someone with HIV/AIDS.
Summary scores of predictor variables

Note: a = Mean±SD.
Bivariate and regression analyses
Bivariate analyses revealed that greater WTP was associated with female gender (p < .01), high HIV risk (p < .01), lower SES (p < .01), no awareness of the Tuskegee Syphilis Study (p < .05), accurate knowledge of the Tuskegee study (p < .05), less mistrust (p < .05), lower role overload (p < .05), more access to health care (p < .01), and knowing someone with HIV/AIDS (p < .01).
With the exception of accurate knowledge of the Tuskegee study, which had a reduced sample size of 233 participants, the significant bivariate correlates were included in the multivariate ordinal regression analysis (Table 3). Four variables emerged as independent predictors of greater WTP in microbicide trials: female gender (p < .05), greater HIV risk (p < .01), lower mistrust (p < .05), and knowing someone with HIV/AIDS (p < .01). Marginal significance was observed for lower role overload (p = .05) and lower SES (p = .06).
Ordinal regression analysis with significant predictors of willingness to participate in microbicide trials

Model χ2 (8, N = 595) = 56.961 (p < .001).
Note: SES = socioeconomic status.
p < .05; **p < .01.
A gender by HIV risk interaction was observed (p < .05). Separate analyses by gender indicated that greater HIV risk was a significant predictor of greater WTP for women only (p < .01; see Table 4). Further examination revealed that these effects were independent of SES, which covaried with gender, HIV risk, and WTP. A separate analysis limiting the men in the analysis to the MSM group yielded the same interaction of gender and HIV risk, such that greater risk was a predictor of greater WTP among women but not in the MSM group.
Willingness to participate in microbicide trials by gender and HIV risk

Note: LR = low risk; HR = high risk; OR = odds ratio; CI = 95% confidence interval for odds ratio; % refers to percentage of men and women endorsing each willingness to participate rating.
= Unadjusted odds ratios reflect difference in willingness to participate ratings between HR and LR groups compared with difference in ‘Not at all’ reference group.
= Adjusted odds ratios controlling for socioeconomic status.
p < .05; **p < .01; ***p < .001.
Questions to assess participants’ knowledge of the Tuskegee Syphilis Study’s historic facts were administered only to participants who had heard of the study. Given the reduced sample size, a separate multivariate ordinal regression analysis was conducted with accurate knowledge of the Tuskegee Syphilis Study, along with the other significant variables in the bivariate analyses, as the independent variables. Although awareness of the Tuskegee study was not associated with WTP, accurate knowledge of its history emerged as a significant independent predictor of greater WTP (p < .05).
Discussion
To our knowledge, the present study is the first that examines correlates of WTP in microbicide research for HIV prevention among African Americans. The present findings indicate several factors predict WTP among three groups of African Americans with varying degrees of risk for HIV infection. Consistent with previous research (Sengupta et al., 2000; Shavers et al., 2002), the current study identified mistrust as a barrier to WTP in microbicide trials. These findings may be attributable to the long history of exploitation of African Americans by the medical establishment (Gamble, 1997). To minimize mistrust for HIV research, investigators could enhance open communication with research participants, address past historical abuses, and collaborate with the African American community. Collaborative approaches may consist of community involvement in research design/recruitment and sharing study results with participants and the community. Additionally, partnering with community-based African American physicians and researchers who may serve as collaborating investigators in microbicide research may facilitate trust-building in the community. Finally, culturally sensitive educational materials on the benefits and risks of trial participation may also reduce mistrust and bolster recruitment.
The impact of the Tuskegee Study of untreated syphilis has been frequently examined throughout the literature to explore the root of mistrust in research for African Americans. Comparable to the findings of Fouad et al. (2000) and Shavers et al. (2002), the current study showed that awareness of the Tuskegee study alone was not correlated with WTP when controlling for other predictors. Among participants who were aware of the Tuskegee Study, accurate knowledge of the study was associated with higher WTP in microbicide trials. These findings suggest that some African American’s mistrust of researchers may be based on misinformation regarding historical facts of the clinical trial. Common misconceptions include beliefs that the Government infected subjects with syphilis, that no African Americans knew about the study until 1972, and that none of the participants received penicillin (White, 2000).
Knowing someone with HIV/AIDS was associated with increased WTP. This is consistent with characteristics of volunteers in a phase I HIV vaccine trial, where 73% of participants knew someone with or at risk for HIV/AIDS (Crumbo et al., 1997). Individuals with direct contact with persons living with HIV may be more driven to participate based on altruistic motivations and/or greater fears of contracting the disease. Focusing on relatives or friends from HIV support groups and networks, and raising awareness of the local impact of HIV on the community, may assist in recruiting African Americans for microbicide trials.
The present results are consistent with research indicating high-risk women may have higher levels of WTP in HIV prevention research than other high-risk groups (Etcheverry et al., 2010). Prior research has revealed associations of HIV risk with WTP in HIV vaccine trials for both men and women (Seage et al., 2001). However, in the current study, the gender by risk interaction revealed that HIV risk was only associated with WTP for women. High-risk women may be less able to negotiate safe sex practices with their partners and more likely to perceive the benefit of a female-controlled HIV prevention method.
There are several limitations to this study. One potential limitation is the hypothetical nature of the outcome variable. However, a study by Halpern and colleagues (2001) revealed that stated WTP has a modest ability to predict actual participation. An additional limitation relates to the use of a convenience sample and the restricted geographic region we examined. Our findings reflect data from African Americans in the southern USA. These results may not generalize to African Americans in other parts of the USA. Future studies utilizing a nationally representative sample of African Americans could improve the generalizability of our findings. Given that the objective of the present study is to identify predictors of willingness to participate in microbicide research, the volunteers in our study may represent a somewhat biased sample in that they consented to be participants in the present study. However, survey research may be viewed differently than studies of microbicides for those who have reservations about study procedures. Additionally, we did not collect data on the enrollment and refusal rate of individuals who were offered participation. Such data might have further advanced our knowledge on willingness to participate in research, and would be a good component to assess in future studies. Nonetheless, our results provide valuable information on critical target groups for future microbicide trials.
Despite its limitations, the current study adds to the literature on African Americans’ WTP in HIV prevention trials. It is encouraging that over half of the study sample expressed openness to participating in microbicide research. Our findings identified several variables that contribute to a statistical model that explained 19% of the variance for WTP in microbicide trials. To enhance African American participation in future microbicide studies, approaches to recruitment should focus on enhancing trust, disseminating accurate knowledge about clinical trials and past abuses, recruiting friends and family of HIV positive individuals, and targeting women at risk.
Footnotes
Acknowledgements
The data for the present study were collected at Jackson State University. This research was supported by a grant from the Centers for Disease Control and Prevention. The authors would like to thank Madeline Sutton, MD, Marcus Durham, MS and Bradford Bartholow, PhD for their significant contributions to the study and manuscript.
Competing Interests
None declared.