
Abstract
One-third of adults living with HIV/AIDS are over the age of 50. This study evaluated the structure of coping among 307 older adults living with HIV/AIDS. Participants completed 61 coping items and measures of anxiety, depression, loneliness, and coping self-efficacy. Exploratory factor analyses retained 40 coping items loading on five specific first order factors (Distancing Avoidance, Social Support Seeking, Self-Destructive Avoidance, Spiritual Coping, and Solution-Focused Coping) and two general second order factors (Active and Avoidant Coping). Factors demonstrated good reliability and validity. Results suggest that general coping factors should be considered with specific factors when measuring coping among older adults.
One-third of adults living with HIV/AIDS in the United States are 50 years of age or older and, by 2015, half of those living with HIV/AIDS will be over 50 (Justice, 2010). Older adults with HIV/AIDS experience more physical and psychosocial stressors and comorbid health conditions compared to their non-infected peers and younger individuals with HIV/AIDS (Goulet et al., 2007; Lyons et al., 2010). This includes higher rates of chronic diseases associated with aging as well as heightened risk of bone, cardiovascular, kidney, liver and lung disease associated with prolonged exposure to HIV/AIDS and antiretroviral therapies (Justice, 2010; Vance, 2010). Further, older adults living with HIV/AIDS are ‘doubly stigmatized’ because of their advanced age and HIV-seropositive status, increasing their risk for depression (Emlet, 2006, 2007). Approximately one-third of these individuals report elevated depressive symptoms and suicidal thoughts (Heckman et al., 2002; Kalichman et al., 2000).
In fact, living and aging with HIV infection is accompanied by numerous stressors (DeMarco et al., 1999; Moskowitz et al., 2009), and evidence clearly supports that the experience of stressful life events can lead to the progression of HIV/AIDS and other health problems (Leserman, 2008; Leserman et al., 2005; Schnurr and Green, 2004). Chronic stress and the experience of stressful life events can activate and alter the hypothalamic-pituitary-adrenal axis, resulting in the suppression of the immune system (Marshall, 2011). Additionally, physical and psychosocial stress can lead to negative health behaviors such as substance use, over-eating, and non-adherence to medical care (Leserman, 2008; Marshall, 2011).
The strategies employed to cope with physical and psychosocial stressors have been linked to health outcomes among people living with HIV/AIDS (Moskowitz et al., 2009). For example, pessimism and negative expectancies were related to CD4 count decline and onset of HIV/AIDS physical symptoms among bereaved men (Reed et al., 1999). Also, the use of avoidant coping was associated with a 1.7 times greater loss of CD4 count and six times greater increase in viral load among men and women over a two year period (Ironson et al., 2005), and men expressing more denial showed faster progression to AIDS over a 7.5 year period (Leserman et al., 2000). Other studies have found that among people coping with stressors associated with living with HIV/AIDS, avoidant and disengagement coping styles are related to increased anxiety and depression (Gonzalez et al., 2009; Gore-Felton et al., 2006), while decreases in avoidant coping following interventions were related to decreased depression and grief (Hansen et al., 2006; Smith et al., 2009).
To date, however, little research has focused on how older adults cope with HIV/AIDS and illness-related stressors. In one of the only studies of coping among this population, African American elders reported significantly fewer depressive symptoms, more support from family members and friends, greater coping self-efficacy, and more use of multiple coping strategies compared to Caucasian elders (BD Heckman et al., 2011). In another study, older adults used religion and spirituality to cope with stressful events relating to their disease (Siegel and Schrimshaw, 2002). Despite these studies, there remains a dearth of information on the measurement and health consequences of adaptive and maladaptive strategies used by older adults to cope with the stress of living and aging with HIV/AIDS.
The current study applied a new measure to evaluate the structure of coping in older adults living with HIV/AIDS with a gender- and ethnically diverse sample of elders living with HIV/AIDS. Furthermore, we hypothesized that specific coping factors identified using exploratory factor analysis (EFA) would be interrelated, thus we explored higher order factors by conducting a second order factor analysis. Finally, we computed the Schmid-Leiman Solution (SLS) using the results of our factor analyses to evaluate the direct relationship between coping items and both general and specific factors. SLS allows for easier interpretation of results by: (a) calculating direct relationships between variables and higher order factors; (b) showing each factor’s individual influence on the variables under study; and (c) showing the unique contribution of factors to variables by separating these into independent, non-overlapping elements (Wolff and Preising, 2005).
Methods
Participants and procedure
Between November 2004 and February 2007, individuals living with HIV infection who were 50 years of age or older enrolled into a randomized, controlled trial of a coping improvement group intervention (TG Heckman et al., 2011). Participants were recruited through AIDS service organizations (ASOs), medical and mental health care providers, print and online media, and displayed print material in New York City, Columbus, Ohio, and Cincinnati, Ohio. A total of 405 individuals were screened for eligibility based on the following criteria: (a) 50 years of age or older; (b) self-reported HIV infection; (c) a Beck Depression Inventory II (BDI-II; Beck et al., 1996) score between 10 and 40; (d) a Modified Mini Mental State Examination (3MS; Teng and Chui, 1987) score of 75 or greater; and (e) voluntary provision of informed consent. Persons with severe depression (BDI-II > 40) were disqualified and referred for immediate mental health treatment. A 3MS score less than 75 indicated a level of cognitive impairment that might interfere with the ability to complete study activities. Of 405 individuals screened, 51 scored below 10 and two scored above 40 on the BDI-II, three scored below 75 on the 3MS, and 349 (86.2%) met study inclusion criteria. Eligible participants completed the study pre-intervention assessment at a local ASO or community health center. This assessment was administered using an audio-computer assisted self-interview (ACASI). Of 349 eligible individuals, 310 completed the pre-intervention assessment. Three participants failed to respond to the majority of the coping questions and were excluded from the present study, leaving a final sample of 307 participants.
Measures
Coping items
A total of 61 items assessing coping strategies that participants may employ to cope with HIV-related stressors were included in the assessment. Of these, 32 were from the Ways of Coping Questionnaire (WCQ; Folkman and Lazarus, 1988) and 11 items from the Coping with Illness inventory (CWI; Murphy et al., 2003). Eighteen additional items were created specifically for this study. The WCQ is a 66-item questionnaire that assesses thoughts and actions individuals utilize to cope with stressful encounters, and the CWI is a 31-item questionnaire that assesses coping responses related to HIV illness. Prior to answering coping items, participants completed a 15-item HIV-related stress scale, the last item of which asked which of 13 HIV-related stressors had been the most stressful over the past four months (DeMarco et al., 1999). Participants responded to each coping item in regard to this stressor using a four-point Likert scale ranging from 1 (‘Not at all’) to 4 (‘Most of the time’). For the current study, we selected five WCQ subscales and 11 CWI items that provided the closest fit to a coping model containing five domains relevant to people living with HIV, including Active Coping, Social Support Seeking, Spiritual Coping, Avoidant Coping, and Self-Destructive Coping (Sikkema et al., 2009; Tarakeshwar et al., 2005). From the WCQ, items from the subscales Planful Problem Solving and Positive Reappraisal were selected to reflect Active Coping Strategies, items from the subscale Seeking Social Support were selected to reflect Social Support Seeking Strategies, and items from the subscales Distancing and Escape-Avoidance were selected to reflect Avoidant Coping Strategies. Additional items were selected from the CWI or created to reflect Social Support Seeking Strategies (four items), Spiritual Coping Strategies (six items), Growth and Meaning Seeking Coping Strategies (six items), Avoidant Coping Strategies (four items), and Self-Destructive Coping Strategies (nine items). All 61 coping items were used in initial exploratory factor analyses to identify the underlying structure of coping strategies employed by older adults living with HIV infection to cope with HIV-related stressors.
The following measures were used to evaluate convergent and divergent validity of the coping factors identified through factor analysis of the coping items described above.
Beck Anxiety Inventory (BAI; Beck and Steer, 1993)
The BAI is a 21-item self-report measure that assesses the severity of anxiety symptoms on a Likert scale ranging from 0 (‘Not at all’) to 3 (‘Severe, it bothered me a lot’). The BAI demonstrated very good internal consistency in the current sample (α = .92).
Geriatric Depression Scale (GDS; Yesavage et al., 1983)
The GDS consisted of 30 items using a ‘yes/no’ response format. Items focused solely on cognitive and behavioral aspects of depression; no somatic items were included, thereby avoiding potential overlap between somatic symptoms of depression, HIV disease manifestation, and potential medication side-effects. The GDS had good internal consistency in the current sample (α = .85).
UCLA Loneliness Scale (ULS; Russell et al., 1980)
The ULS is a 10-item version of the UCLA Loneliness Scale, which used a four-point response scale ranging from 1 (‘Never’) to 4 (‘Often’), and had good internal consistency in the current sample (α = .86).
Coping Self-Efficacy Scale (CSS; Chesney et al., 1996)
The CSS is a 26-item scale that assessed participants’ beliefs about their ability to cope with illness-related stressors. The CSS uses an 11-point scale ranging from 0 (‘Cannot do at all’) to 10 (‘Certain can do’) and had excellent internal consistency in the current sample (α = .95).
Statistical analysis
The statistical analysis for this study was completed in four stages.
Stage 1: First order exploratory factor analysis
Stage 1 involved completing an iterative process to identify the simple factorial structure described by the coping items. As factors were expected to be correlated, an oblique rotation method (promax) was used. Parallel Analysis, which compares the observed eigenvalues resulting from an EFA with random data sets produced through Monte Carlo simulation, was used to estimate the number of factors to retain (Floyd and Widaman, 1995). After computing an EFA, the pattern matrix of factor loadings was examined. Items that failed to load on any factor at greater than .40, or that cross-loaded on two or more factors at greater than .30, were removed, and the remaining items were reevaluated (Floyd and Widaman, 1995). This continued until a clear simple structure emerged.
A minimum of five response categories are suggested for ordered-categorical data for standard estimation techniques to be considered reliable (Wirth and Edwards, 2007). As coping items were answered using a four-point Likert scale, the EFA was conducted using the weighted least squares mean-and variance-adjusted (WLSMV) estimator, available in the computer program Mplus 5.21 (Muthen and Muthen, 2007). WLSMV was developed for modeling categorical data, uses the polychoric correlation matrix, and is suitable with smaller samples (Nussbeck et al., 2006; Wirth and Edwards, 2007).
Stage 2: Second order exploratory factor analysis
Because first order factors were expected to be correlated, the possibility of first order factors loading on one or more second order factors was evaluated (Loehlin, 2004; Wolff and Preising, 2005). The factor correlation matrix of the final factor solution resulting from Stage 1 above was entered into an EFA to examine the factor structure of the coping factors. This EFA was conducted using unweighted least squares (ULS) as the estimator and promax rotation. Additionally, if two or more correlated second order factors were identified, third order EFAs would be considered.
Stage 3: Compute Schmid-Leiman Solution
To fully evaluate the structure of first- and second order factors, the Schmid-Leiman Solution (SLS) was computed using syntax prepared for the SPSS MATRIX processor (Wolff and Preising, 2005). While the influence of individual items in second order factor analysis can only be observed indirectly through the item loadings on first order factors, the SLS relates individual items to second order factors directly. This is done hierarchically, with the second order factors being allowed to account for as much of the variance in individual items as possible. As a result, the item loadings on first order factors are partial correlations independent from higher order factors as the contribution to higher orders has been partialed out (Gorsuch, 1983; Loehlin, 2004; Wolff and Preising, 2005).
The SLS aids in interpretation of the factor solution and identifies the relative contribution of each item to general higher order factors and more specific lower order factors. If higher order factors account for 40% or more of the extracted variance, then general factors are of importance and should be considered in interpretation of factors (Gorsuch, 1983).
Stage 4: Factor reliability and validity
Cronbach’s alpha coefficients were calculated to assess internal consistency of each factor. Convergent and divergent validity was assessed using the measures described above. These calculations were performed using SPSS 17.0.
Results
Sample characteristics
The sample was comprised of 205 men and 102 women. The average age of study participants was 55.5 (4.8), and participants had been living with HIV for 13.4 (5.3) years on average. Men were infected with HIV an average of two years earlier than women (14.1 [5.4] years vs 12.0 [4.8] years, t (305) = 3.23; p < .05). The sample was diverse in race/ethnicity (49.8% African American, 29.0% Caucasian, 15.3% Hispanic, and 5.9% Other) and sexual orientation (48.0% gay/lesbian, 43.0% heterosexual, and 9.0% bisexual). The majority of the sample (76.2%) had completed high school. Education level differed by gender (χ2 (2) = 37.13; p < .001) with women less likely to have graduated from high school (39.2% vs 16.1%), while men were more likely to have attended some college (62.4% vs 26.5%). In general, the sample was poor and unemployed, with 87.0% reporting annual incomes less than $20,000.
Stage 1: First order exploratory factor analysis
A parallel analysis comparing observed eigenvalues from the initial EFA with random data generated based on 61 items and 307 participant across 100 simulations suggested retaining seven factors. After computing the EFA with Promax rotation, the pattern matrix of the seven retained factors for the 61 item was examined. Eight items failed to load on any factor based on our critical value of .40, and five items cross-loaded on two or more factors at greater than .30, thus these 13 items were removed. The 48 remaining items were reevaluated, and a parallel analysis suggested retaining five factors. Two items failed to load on any factor and five items cross-loaded on two or more factors, thus these seven items were removed. The 41 remaining items were again evaluated, and a parallel analysis suggested retaining five factors. At this point, a clear simple structure with all items loading uniquely on a single factor emerged. Based on the items that loaded together on each factor, the factors were labeled Distancing Avoidance, Social Support Seeking, Self-Destructive Avoidance, Spiritual Coping, and Solution-Focused Coping. However, after examining the items loading in each factor, it was determined that the item ‘I came out of the experience better than when I went in’ did not conceptually fit the Solution-Focused Factor, and this item was removed. The factor analysis was rerun with the 40 remaining items, resulting in no further changes. Factor loadings for each item on the five factors are presented in Table 1.
Final Promax rotated factor loading for simple structure of five factor EFA solution

Note: Numbers in italic signify the specific factor where each item loads highest. F1 = Distancing Avoidance; F2 = Social Support Seeking; F3 = Self-Destructive Avoidance; F4 = Spiritual Coping; F5 = Solution-Focused Coping.
Stage 2: Second order exploratory factor analysis
To evaluate the possibility of first order factors loading on higher order factors, the factor correlation matrix of the final five factor solution was entered into an EFA to examine the factor structure of the first order coping factors. The second order EFA identified two factors. Social Support Seeking, Spiritual Coping, and Solution-Focused Coping loaded together on a general factor which we labeled Active Coping. Distancing and Self-Destructive Avoidance loaded together on a second general factor which we labeled Avoidant Coping. As these two general factors were orthogonal, the presence of a third order factor was not evaluated. The correlation matrix of the five specific factors and their loadings on the two general factors are shown in Table 2.
Correlation table of specific (first order) factors used to conduct second order factor analysis, and resulting factor loadings of specific factors on general (second order) factors
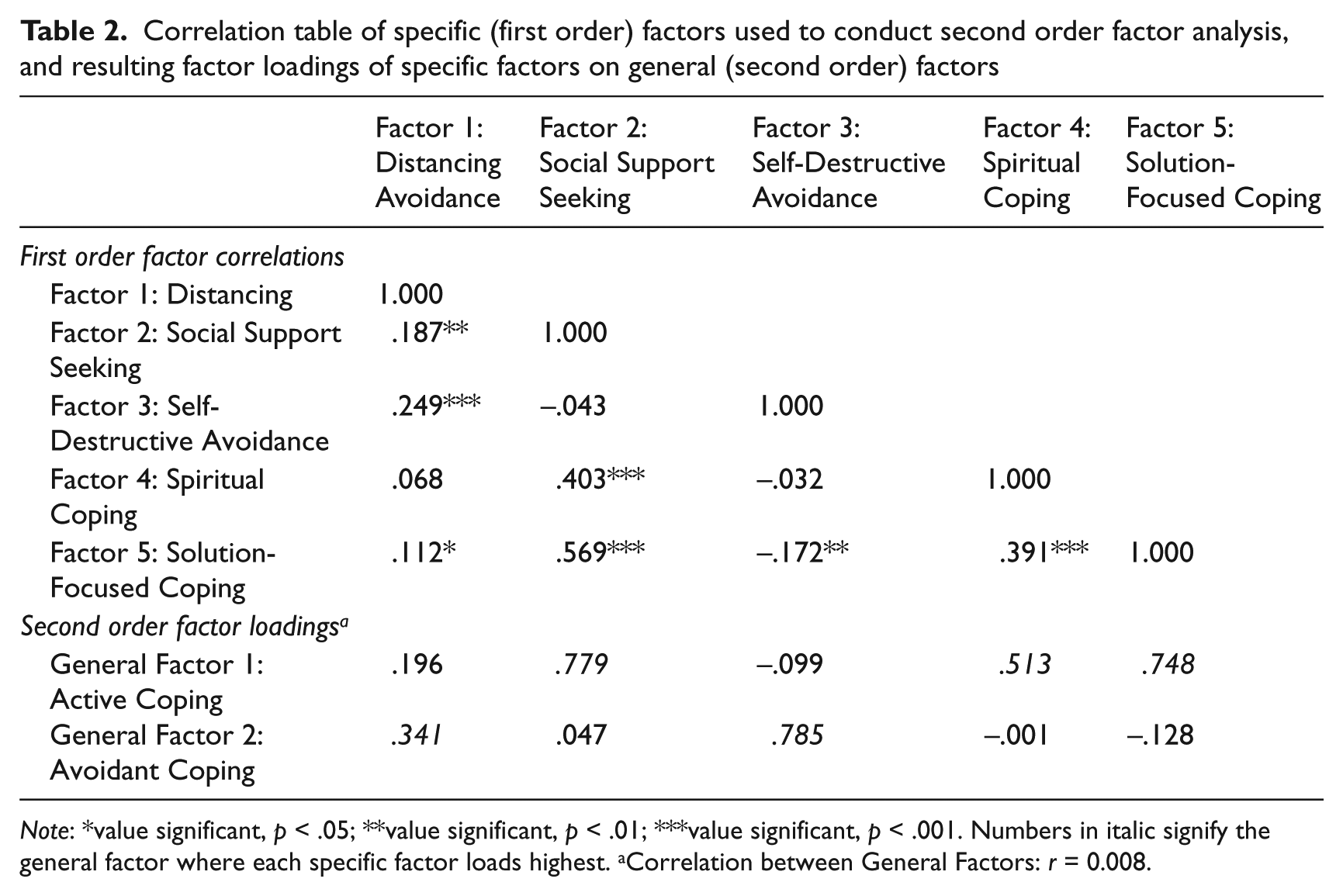
Note: *value significant, p < .05; **value significant, p < .01; ***value significant, p < .001. Numbers in italic signify the general factor where each specific factor loads highest. aCorrelation between General Factors: r = 0.008.
Stage 3: Compute Schmid-Leiman Solution
To fully evaluate the structure of first and second order factors, the SLS was computed. Results are presented in Table 3. The numbers in columns G1 and G2 represent the factor loadings of each item on the general, or second order, factors. The numbers in columns F1 to F5 are partial correlations representing the factor loadings of each item on the first order factors independent of the loadings on the second order factors. The numbers in columns H2 Tot, H2 2nd, and H2 1st represent the total communality (variance explained) of each item, the communality of second order factors, and the communality of first order factors, respectively.
Final factor loading of coping items on general (first order) and specific (second order) factors as determined by the Schmid-Leiman Solution (SLS), total and partial communalities (variance explained) of each item, and factor loading and reliability statistics

Note: aCronbach’s alpha. Numbers in italic signify the general and specific factor where each item loads highest and is thus included in computing scores and internal consistency estimates.
The bottom rows of Table 3 present the Sums of Squares and percent of variance attributed to each general (second order) and specific (first order) factor, as well as the combined general and combined specific factors. As 46.8% of the extracted variance is attributable to the second order factors, these should be considered in the interpretation of factors (Gorsuch, 1983).
Stage 4: Factor reliability and validity
Cronbach’s alpha coefficients were calculated to assess internal consistency of each general and specific factor. These coefficients are displayed at the bottom of Table 3.
Convergent and divergent validity were assessed based on correlations of each general and specific coping factor with the Beck Anxiety Inventory (BAI), Geriatric Depression Scale (GDS), UCLA Loneliness Scale (ULS), and Coping Self-Efficacy Scale (CSS). Table 4 presents the correlation table based on general and specific coping factors and validation scales. Table 4 shows that the BAI, GDS, and ULS are positively correlated, and the CSS negatively correlated, with the general Avoidance Coping factor. The GDS and ULS are negatively correlated with the general Active Coping factor, while the CSS is positively correlated with Active Coping.
Convergent and divergent validity as indicated by Pearson correlations between specific and general coping factors and validation measures
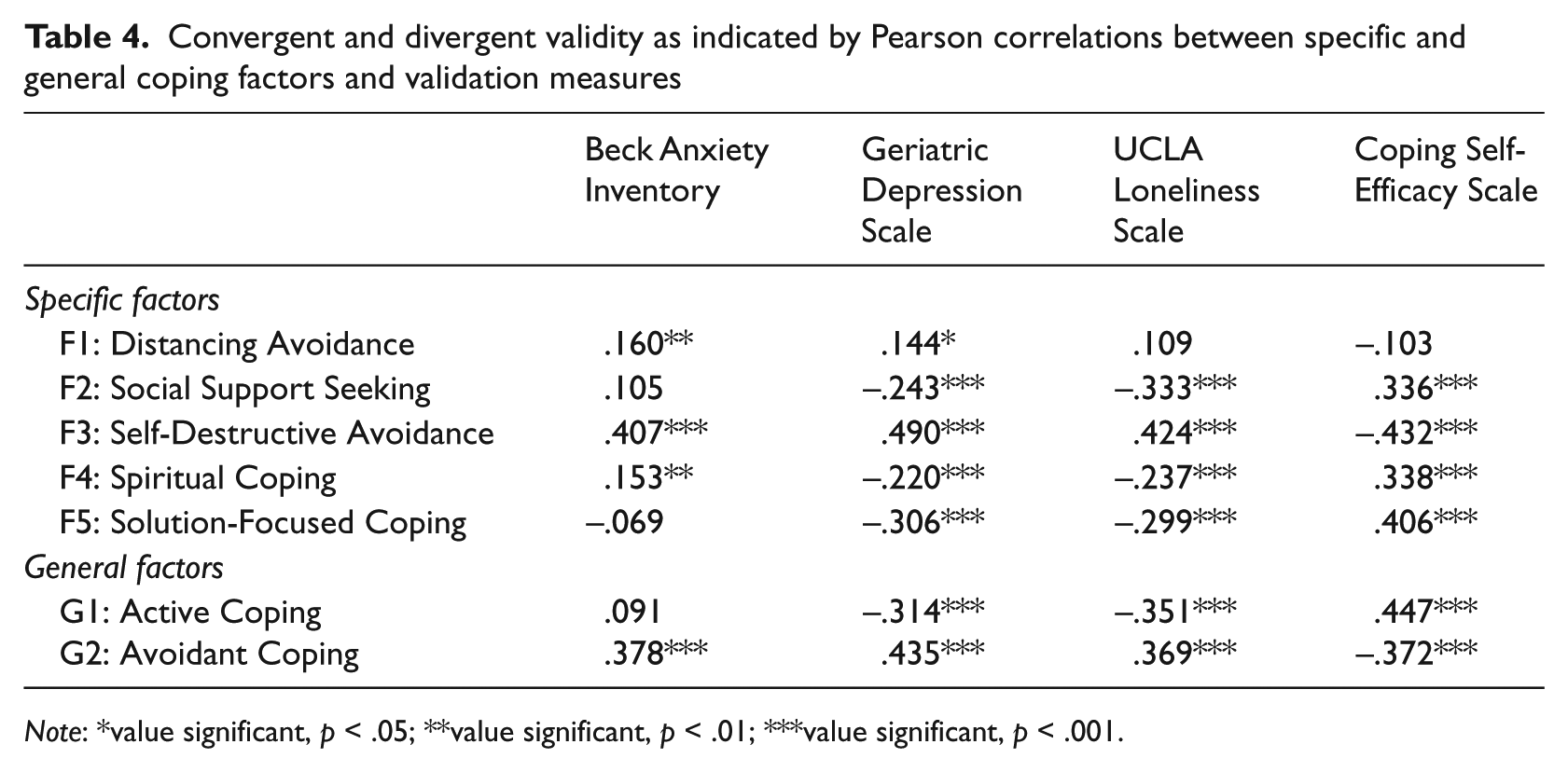
Note: *value significant, p < .05; **value significant, p < .01; ***value significant, p < .001.
Additionally, the BAI, GDS, and ULS have strong positive correlations with Self-Destructive Avoidance, while the BAI and GDS have weaker positive correlations with Distancing Avoidance. The GDS and ULS, on the other hand, are negatively correlated with Solution-Focused Coping and Social Support Seeking, with weaker negative correlations with Spiritual Coping. Finally, the CSS is positively correlated with Solution-Focused Coping, Spiritual Coping and Social Support Seeking and negatively correlated with Self-Destructive Avoidance.
Discussion
Older adults face ageism, compounded stigma associated with living with HIV/AIDS as an older adult, and increasing age- and HIV-related comorbid medical conditions (Emlet, 2006, 2007; Justice, 2010). Yet, to date, little is known about the coping strategies employed by older adults facing these difficulties. In this study, we sought to identify coping strategies among a sample of older adults dealing with the physical and psychological stressors associated with aging with HIV/AIDS. This is one of the first studies to address this issue. Additionally, we replicated a five factor model of coping identified in prior studies among individuals living with HIV (Sikkema et al., 2009; Tarakeshwar et al., 2005), and expanded prior findings by: (1) adding and testing additional coping items; (2) identifying the presence of general, higher order factors of Active and Avoidance Coping; (3) evaluating the relative association of individual items with, and variance explained by, general and specific factors; and (4) creating an adapted measure with good internal consistency and convergent and divergent validity for assessing coping among older adults living with HIV.
We hypothesized that coping factors would be interrelated, and that measuring the structure of coping would be improved by accounting for these interrelations (Loehlin, 2004; Wolff and Preising, 2005). Thus, we conducted a higher order factor analysis, identifying two general factors, Active and Avoidance Coping. Further, we computed the SLS to identify the contribution of individual items to general and specific factors, as well as the variance explained by these factors. As nearly half of the extracted variance (46.8%) was explained by the general factors, these should be considered in the evaluation of coping among older adults living with HIV/AIDS. This supports the notion that coping is best understood hierarchically (Skinner et al., 2003: 217), with lower order categories of coping strategies classified within higher order categories of adaptive strategies representing ‘longer term processes of adaptation and development’. The advantage of this approach is that it meaningfully links individual instances of coping with coping as an adaptive process (Skinner et al., 2003). Additionally, a recent meta-analysis of studies of coping with HIV examined both specific and general classifications of coping strategies, revealing that Active Coping approaches at both levels were associated with lower levels of distress, more health protective behavior, and better physical health, while Avoidant Coping approaches at both levels had the opposite effect (Moskowitz et al., 2009). A latent variable modeling approach to evaluating the role of coping on health has been suggested (Moskowitz et al., 2009; Skinner et al., 2003) as a possible strategy to resolve instances where the shared variance from higher order factors may exaggerate or disguise the unique effects of lower order factors on health outcomes. Further, future research should focus on differentiating the short and long term impact of specific instances of coping nested within higher order adaptive (or maladaptive) coping processes across time. Research should also address the mechanisms used in the appraisal of stressors and selection of coping strategies from both state (situational) and trait (strategic or adaptive process) perspectives.
Findings from the current study regarding the association of coping factors with psychological variables are consistent with the existing literature on coping with HIV (Moskowitz et al., 2009), and support the construct validity of the coping factors identified here. For example, the general factor Active Coping, as well as the specific factors Social Support Seeking, Spiritual Coping and Solution-Focused Coping, were positively related to coping self-efficacy and negatively related to depression and loneliness. Alternatively, the general factor Avoidant Coping, as well as the specific factors Distancing Coping and Self-Destructive Coping, were negatively related to coping self-efficacy and positively related to anxiety, depression, and loneliness. One difference between the current findings and a recent meta-analysis of coping with HIV was that Spiritual Coping was related to both positive and negative psychological variables in this study, while it was only related to positive psychological and affective variables in the meta-analysis (Moskowitz et al., 2009). The current findings indicate that participants who were experiencing depression or loneliness were significantly less likely to utilize spiritual coping techniques, while participants experiencing anxiety were more likely to utilize spiritual coping techniques. However, it is unclear whether this relationship represents the use of spiritual coping in response to anxiety, perhaps in a search for calm and inner-peace, or the experience of anxiety in response to the use of spiritual coping techniques, perhaps representing feelings of personal responsibility.
The current study has several limitations. First, cause–effect conclusions cannot be based upon the study’s findings due to its cross- sectional design. Second, all information was obtained through self-report, which is subject to reporting and recall bias. Third, no information was available linking the use of a coping strategy and the effectiveness of the strategy. Fourth, the items measuring avoidant coping were predominately negatively toned, thus we did not capture potential adaptive uses of avoidant coping strategies. Fifth, participants were selected from large cities in the Midwestern and Northeastern regions of the United States. Findings may not be generalizable to rural areas or different geographic regions in the country. Sixth, while we assessed coping in relation to HIV-related stress, more specific measures of stress may elicit different results. Finally, all participants in this study had mild to moderate depression, which could limit the generalizability of these findings. We note, however, that depression is common among older adults with HIV (Heckman et al., 2002; Kalichman et al., 2000). Our recruitment material noted that this was a study of older adults living with HIV infection and did not mention depression as an inclusion criterion. Yet 87.4% of the 405 individuals screened met the criterion of having mild to moderate levels of depression.
Despite these limitations, our study had numerous strengths. First, the sample was diverse in gender, race/ethnicity and sexual orientation, which increases the generalizability of study findings. Additionally, our study used diverse recruitment methods and venues, including ASOs, community outreach efforts, and advertisements in AIDS-related materials, further ensuring that the sample population is representative of older adults living with HIV/AIDS. Second, the study focused on older adults living with HIV/AIDS. As the HIV/AIDS population continues to age, it is becoming even more critical to understand how older individuals with HIV/AIDS cope with the disease. Third, this study broadened the scope of the HIV/AIDS literature by looking at coping strategies used by individuals to manage living with HIV/AIDS, as opposed to focusing on specific stressors such as bereavement or trauma related to HIV/AIDS. Fourth, the results of this study provided evidence that both specific and general coping strategies should be taken into account when studying coping among individuals with HIV/AIDS, although these findings should be confirmed in future research, including confirmatory factor analysis. Future research should also examine the use and effectiveness of specific and general coping strategies in regard to both specific and general stressors, and by linking coping strategies to physical and mental health outcomes.
As individuals with HIV/AIDS are living for extended periods of time, more attention should be devoted to the specific medical and psychosocial needs of this aging population (Justice, 2010; Vance, 2010). Health professionals are going to require innovative strategies and tools to understand and improve physical and mental health outcomes for HIV-positive adults over the age of 50. Effective coping may lead to better physical and psychological functioning among older persons with HIV/AIDS (TG Heckman et al., 2011). Conversely, when used maladaptively or exclusively, avoidant and destructive coping strategies can be detrimental, or even fatal (Ironson et al., 2005; Leserman, 2008; Leserman et al., 2000; Marshall, 2011). This study’s results enhance our understanding of how older adults living with HIV/AIDS cope with the disease. Greater understanding of how various subgroups cope with HIV/AIDS will lead to improved interventions to enhance health, potentially prolonging and improving the quality of lives of individuals with HIV/AIDS.
Footnotes
Acknowledgements
This research was funded by grants R01 MH067566, K23 MH076671 and T32 MH020031 from the National Institute of Mental Health. We are grateful to all study participants and our community collaborators at The Columbus AIDS Task Force, AIDS Volunteers of Cincinnati, and Callen-Lorde Community Health Center in NYC.
Competing Interests
None declared.