
Abstract
The aim of this study was to determine the effect of art therapy on post-traumatic growth in patients with haematological malignancies in a non-randomised trial (n = 36, intervention group; n = 129, control group). Art therapy was administered over a period of 22 weeks in small groups. Post-traumatic growth was measured with the Stress-Related Growth Scale. After controlling for the effect of potential confounders, no difference in post-traumatic growth was observed between the intervention and control groups after 22 weeks. There was no evidence for an effect of weekly group sessions with art therapy on post-traumatic growth in patients with haematological malignancies.
Introduction
Being diagnosed with cancer together with the often-necessary intense treatment can be a traumatic experience (Schmitt et al., 2003), resulting in severe anxiety over long periods of time (Bringmann et al., 2008). For many patients, receiving such a diagnosis is associated with the fear of intense pain, loss of control, stigmatisation and death (Holland and Rowland, 1989).
During the last decade, increasing interest has been focused on whether these potentially traumatic events despite being challenging and often highly distressing can result in beneficial or constructive consequences, that is, whether traumatic experiences can lead to emotional growth in patients and relatives (Demirtepe-Saygili and Bozo, 2011; Fromm et al., 1996; Hungerbuehler et al., 2011; Kahana et al., 2011; Kim et al., 2011; Love and Sabiston, 2011). Such post-traumatic growth has been defined as positive psychological change experienced as a result of the struggle with highly challenging life circumstances (Calhoun et al., 2000; Calhoun and Tedeschi, 2001). It describes the experience of individuals whose development has surpassed what was present before the struggle with the crises occurred, that is, people feel that they did not simply ‘go back to life as usual’ but that they feel enriched, wiser, grown and so on after the crisis.
According to Tedeschi and Calhoun (2004), positive changes can be found in five dimensions, representing different types of post-traumatic growth: greater appreciation of life and changed sense of priorities; warmer, more intimate relationships with others; a greater sense of personal strength; recognition of new possibilities of paths for one’s life and spiritual development (Tedeschi and Calhoun, 2004). Other researchers argued that post-traumatic growth should be measured one-dimensionally (Park et al., 1996).
Individuals’ experience of post-traumatic growth depends on several predictors. Many facilitating factors have been reported: younger age, female gender, low levels of viral load in patients with HIV, low consumption of alcohol, low levels of pessimism and depression, high life satisfaction, high levels of extraversion, having an active sexual life and receiving counselling (Barskova and Oesterreich, 2009; Cormio et al., 2010; Jansen et al., 2011; Milam, 2004; Mols et al., 2009; Paul et al., 2010; Sheikh, 2004).
Whether or not psychosocial interventions can help to increase post-traumatic growth after traumatic events or serious illness has been investigated by only a few studies to date. Post-traumatic growth was increased through psycho-education in college students who had experienced a crisis (Dolbier et al., 2010) and through Internet-based cognitive therapy in a group of individuals who had experienced sexual abuse, death of a close person or a severe illness (Knaevelsrud et al., 2010). However, in another randomised controlled trial, no effect was found after cognitive therapy in a group of motor vehicle accident survivors with post-traumatic stress disorder (PTSD) (Zoellner et al., 2011).
Another option for supporting post-traumatic growth could be the application of art therapy. In cancer patients, it has been shown that art therapy can help to develop new ways in expressing emotions, in coping with the disease, in reducing anxiety and fatigue, in increasing emotional well-being and in supporting communication with family and friends (Bar-Sela et al., 2007; Geue et al., 2010; Heiney and Darr-Hope, 1999; Luzzatto and Gabriel, 2001; Wood, 2009; Wood et al., 2011; Öster et al., 2006).
Art therapists often assume that their work enables patients to develop emotional strength and hence post-traumatic growth. This assumption is in line with the theoretical concept of Tedeschi and Calhoun (2004), who suggested that the degree to which individuals engage in self-disclosure about their emotions and about their perspectives on the disease, both aspects playing important roles in art therapy, are predictors of growth. A non-randomised study by Garland et al. (2007) supported that assumption, but evidence is still sparse. It is interesting to note that cancer patients mentioned personal growth as both an important motivation and a goal for participation in creative art education (Visser and Op ’T Hoog, 2008).
According to the results of a qualitative study we performed previously (Götze et al., 2007; Singer et al., 2010; Weiss et al., 2005), cancer patients reported positive changes that could be seen as signs of post-traumatic growth, after an art education intervention. Therefore, in this study, we aimed at proving this effect in a controlled intervention study using quantitative measures. Our hypothesis was that patients with haematological malignancies who attend an art therapy intervention would report higher levels of post-traumatic growth after the intervention than non-participants.
Methods
Design and procedure
This was a non-randomised controlled intervention study with two assessment points: before (t1) and immediately after the intervention (t2).
Adults who provided written informed consent, who were diagnosed within the last few years with a haematological malignancy and who had completed acute oncological treatment were eligible for this study. Participants for the intervention were recruited over a period of 20 months (October 2007 to May 2009) by written invitations mailed to every patient who had been treated for a haematological malignancy at Leipzig University Hospital and who lived within and in the vicinity of the city. In addition, advertisements were placed in local newspapers, in medical practices specialising in haemato-oncological diseases and on the institution’s website. Flyers were also handed to patients who were seeking support in a cancer counselling centre attached to the university. If a patient indicated interest, he or she was invited to the study centre to receive more information on the intervention, to have the possibility to ask questions and to confirm or refrain from consent. This consultation was done by the artist who led the program together with the psychologist who was in charge of data collection and analysis.
A control group was formed by a group of haematological patients who lived too far away from the university to be able to take part in the program. They received mailed questionnaires together with a stamped return envelope at the same time as the participants of the intervention.
The staff member performing the assessments was not involved in any aspect of delivering the intervention. Similarly, the questionnaires were sent out by mail and collected by the psychologist in charge of data management, so the person delivering the intervention was not involved in data collection. The study protocol was approved by Leipzig University’s Institutional Review Board.
Intervention
The intervention consisted of 22 weekly sessions of 90 minutes in small groups of 6–9 participants at an outpatient psycho-oncology unit of a university hospital led by a psychologically trained and supervised artist. At the beginning of the sessions, participants were requested to perform simple drawing techniques. The aim of this first phase of the program was to make people feel comfortable with the group situation and with creative working. From the sixth session on, participants gradually started exploring and expressing their feelings, for example, by drawing their current mood and by painting a self-portrait. In the final phase of the program, patients were encouraged to create a book containing, for example, their ideas about the disease and their coping processes. A detailed description of the intervention and its concept was published prior to the beginning of this evaluation study (Geue et al., 2011; Singer et al., 2010; Weiss et al., 2005). To increase adherence to the intervention, participants were asked to inform the group leader if they could not attend a session, and non-attendees were phoned by the group leader if apologies had not been received. The reasons for non-attendance were documented. The group leader tried to motivate each participant to attend the sessions regularly.
Instruments
Post-traumatic growth was measured with the Stress-Related Growth Scale (SRGS) (Park et al., 1996) in its German translation ‘Persönliche Reifung nach Belastungen’ (Maercker and Langner, 2001). This self-administered 15-item measure is a unidimensional instrument based on a three-dimensional concept of personal and social resources and specific coping strategies (Schaefer and Moos, 1992). However, factor analyses have demonstrated that a one-factor solution was most appropriate to summarise the items (Maercker and Langner, 2001; Park et al., 1996). The scale’s internal consistency has been reported to be satisfactory with Cronbach’s alpha ranging from 0.89 to 0.91 (Maercker and Langner, 2001; Park et al., 1996). In our sample, the alpha was 0.90 and 0.92 at the two assessment points, respectively. At time t1, participants were asked to assess their growth since the tumour diagnosis, whereas at t2, they were asked to assess growth since the last measurement.
Socio-demographic data were collected from the participants using questions developed by the research team. Information about the clinical diagnosis was extracted from the hospital’s electronic documentation system.
Social support was self-assessed by the patients using the German Questionnaire for Social Support (Fragebogen zur Sozialen Unterstützung) in its short form (Fydrich et al., 1987). This instrument comprises 14 Likert-scaled items that are summarised into one total score. Its internal consistency measured with Cronbach’s alpha is 0.94 (Fydrich et al., 2007).
Data analysis
First, descriptive statistics were calculated (means and standard deviations (SDs)) to describe baseline and post-intervention levels of post-traumatic growth, and sample characteristics were defined. Second, differences in post-traumatic growth after the intervention between the control and intervention groups were investigated using the analysis of covariance, adjusting for the potential confounding effects of age, sex, education level, religion, time since diagnosis, social support and baseline levels of post-traumatic growth. Statistical analyses were performed using the software package SPSS 13.0 (SPSS Inc., Chicago, IL, USA).
Results
Sample
A total of 648 patients had been treated at Leipzig University for a haematological malignancy within the past 5 years and were eligible for this study. Those who lived within the vicinity (40 km) of our department were eligible to be offered the intervention.
Intervention group
In total, 410 patients were contacted and informed about the intervention study; 365 of them did not reply or declined to participate and 45 were enrolled into the intervention arm. Ten additional patients were enrolled via newspapers and flyers, and three of them had received the flyers at the cancer counselling centre. They lived also within the vicinity of the department. Forty-nine of the enrolled patients came to the initial interview where the study was explained in person. After that interview, two withdrew their consent to participate and five were excluded for different reasons, for example, because they were still in acute oncological treatment. Forty-two patients were assigned to the intervention arm, of whom five attended no sessions. Four participants stopped attending the sessions during the course of the study; they are treated in the analysis as if they were in the intervention arm (intent to treat).
Control group
The remaining 238 patients received mailed questionnaires without being informed about the intervention. Fifty-five of these patients were subsequently excluded because of the following reasons: patient was deceased (n = 47) and patient without haematological malignancy (n = 8). A further 19 patients declined because they felt physically not able to complete a questionnaire (n = 2), they were not interested in research (n = 6) or without giving a reason (n = 11). In total, 164 patients in the control group completed the questionnaire at t1.
The number of participants who completed the first and second measurements was 42 and 36, respectively, in the intervention group and 164 and 143, respectively, in the control group. From these, 36 and 129 complete datasets were available and are used in the following analyses (Figure 1).
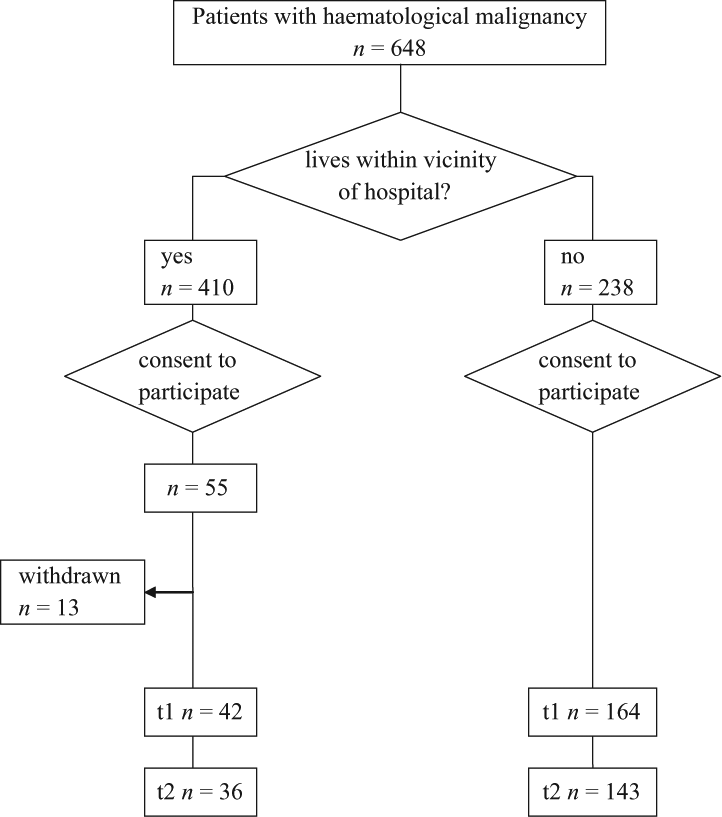
Flow chart of sampling.
Sample characteristics
Socio-demographic and medical characteristics of the two groups are displayed in Tables 1 and 2. Both groups were comparable concerning age, marital status, time since diagnosis and haematological diagnosis, but sex distribution and educational level were different: In the intervention group, the participants were more often female and higher educated. Both variables were controlled in the group comparison as potential confounders.
Socio-demographic characteristics of sample at baseline.
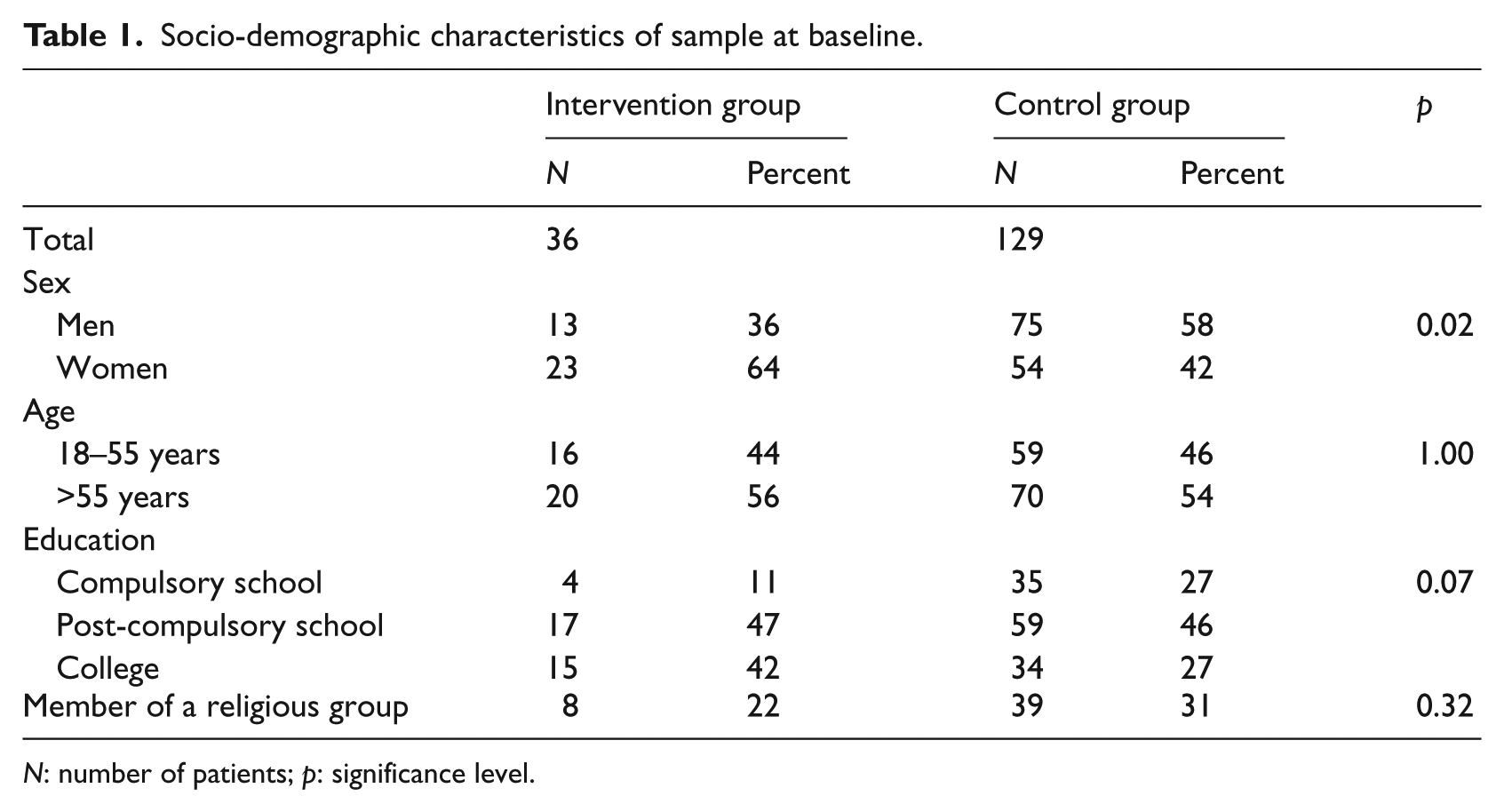
N: number of patients; p: significance level.
Clinical characteristics of sample at baseline.
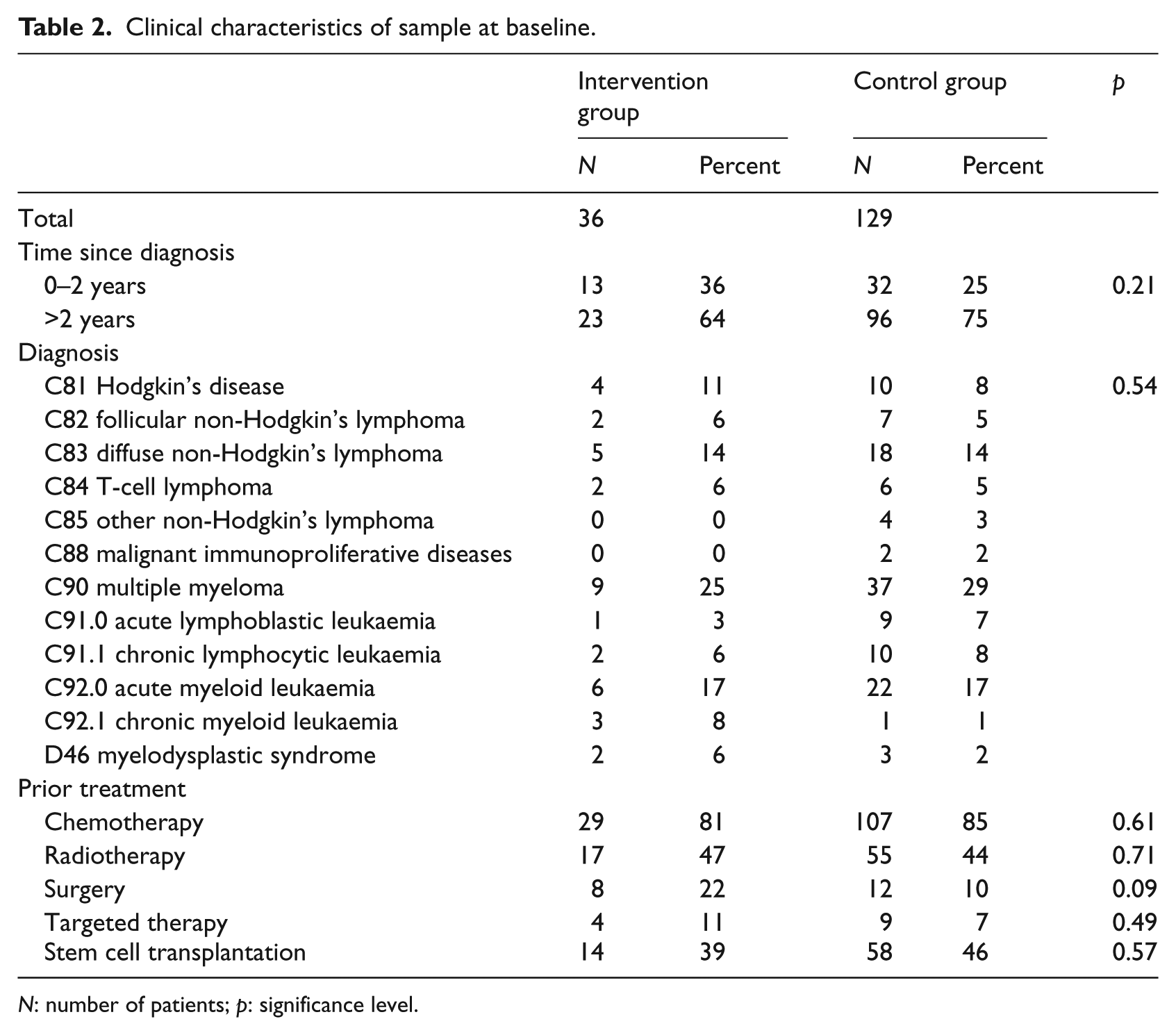
N: number of patients; p: significance level.
Post-traumatic growth
Descriptive statistics
Post-traumatic growth as measured by the SRGS was higher in the control group at both measurement points compared to the intervention group. At baseline (t1), the mean score was 15.5 (SD = 6.7) in the intervention group and 18.3 (SD = 6.8) in the control group. Half a year later (t2), the scores were 15.9 (SD = 7.7) and 18.6 (SD = 7.4), respectively. Those scores should not be interpreted longitudinally as the instruction in the questionnaire was different at the two measurement points, that is, the patients referred to different time windows. Post-traumatic growth at t2 (i.e. after the intervention) represents the additional changes patients experienced after baseline. Therefore, these scores were regarded as outcome measure in the following analyses.
Multivariate analysis
Differences in post-traumatic growth at t2 between men and women were observed. While women in the intervention group showed lower post-traumatic growth than men, the opposite was found in the control group (see Table 3). Age was associated with post-traumatic growth in the intervention group but not in the control group.
Post-traumatic growth 0.5 year after baseline.
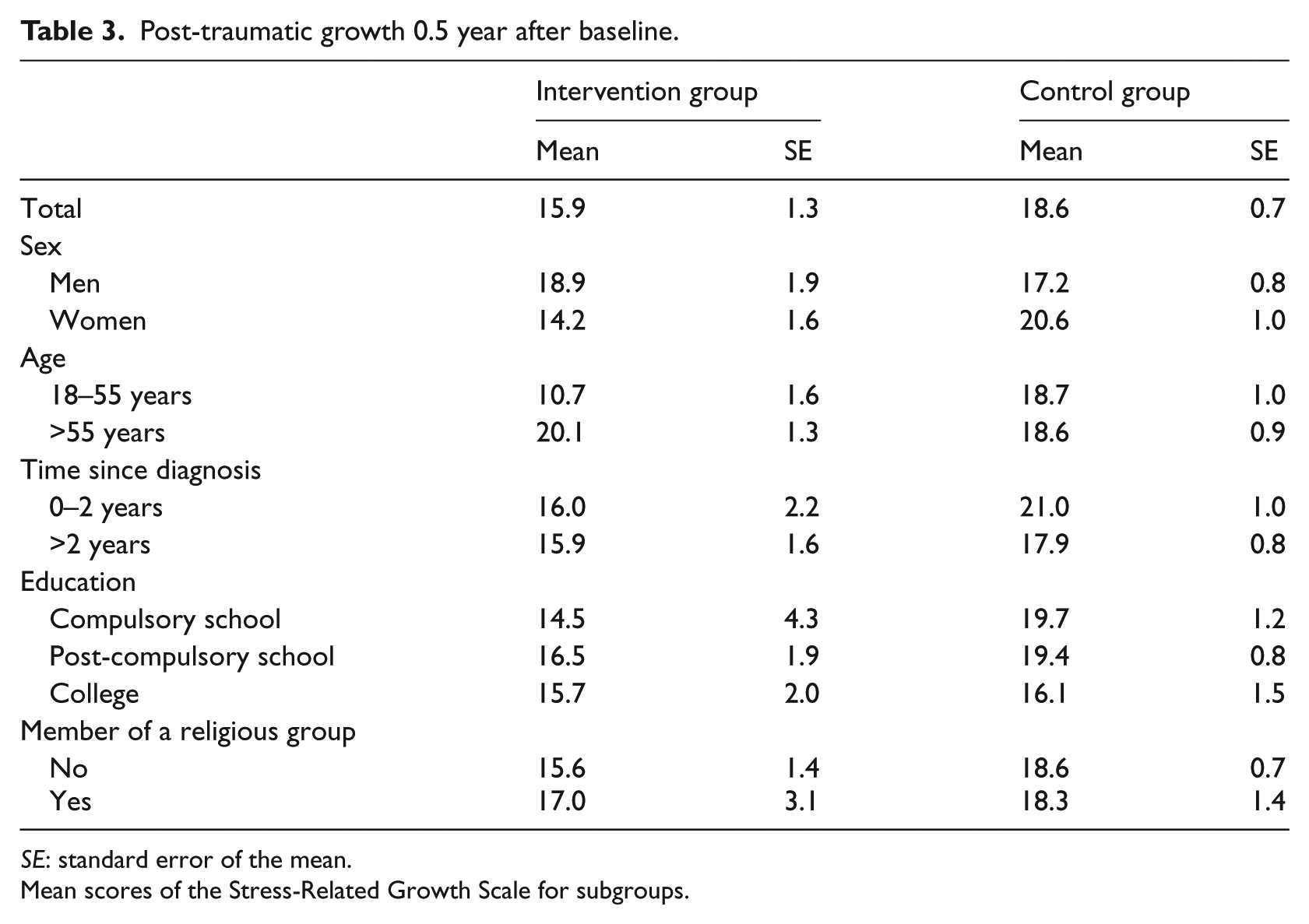
SE: standard error of the mean.
Mean scores of the Stress-Related Growth Scale for subgroups.
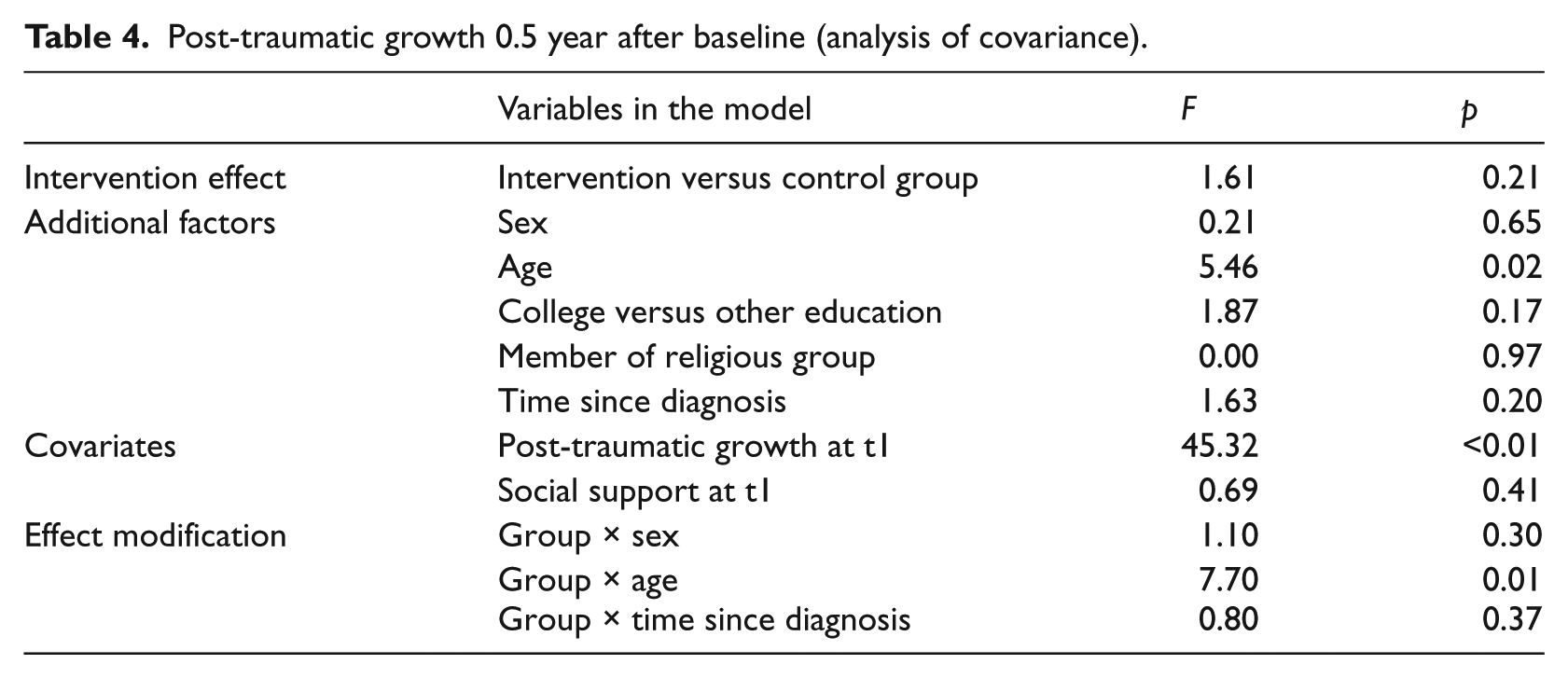
In the multivariate model (Table 4), no differences between intervention and control groups were observed while controlling for the effect of sex, age, time since diagnosis, education, religious group, social support and baseline post-traumatic growth. The latter appeared to be the major predictor of post-traumatic growth at t2 (F = 45.3, p > 0.01). Younger participants had lower scores in post-traumatic growth (F = 5.5, p = 0.02), although there was also a significant effect modification of the group effect by age (F = 7.7, p = 0.01), that is, in the intervention group, patients up to 55 years reported less growth than older participants, but in the control group, no age differences were observed. No evidence for the effect of age, time since diagnosis, social support, membership in a religious group, education and other effect modifications was found.
Post-traumatic growth 0.5 year after baseline (analysis of covariance).
Discussion
The aim of this trial was to identify potential effects of an art education program developed for an outpatient setting on post-traumatic growth in patients with a haematological malignancy. Based on our results, there was no evidence of an effect of art therapy on post-traumatic growth. Several explanations for this finding are possible.
First, this was a non-randomised trial, and though we controlled for known confounders based on the literature, residual confounding could have been present. In order not to compromise the power of this study, we had to keep the model parsimonious and thus the number of cofactors and covariates at a minimum. Some of the factors that were assumed to be relevant a priori, for example, social support and membership in a religious group, appeared to be unrelated to growth. Therefore, future trials could possibly exclude those factors and include others. Care should be taken to include age as a confounder without testing if there is an effect modification present as this was the case in our study.
Second, there was a striking difference in baseline post-traumatic growth in the two groups, indicating that people with less experience of growth may wish to attend such an intervention more frequently. In the multivariate model, this was controlled for by including baseline scores of growth in the model; however, other selection processes might have been overlooked. Another bias could have occurred if patients from the control group, who lived further away from the university hospital, represented a group with more complex diseases. Such patients are treated more often at the university cancer centres, whereas patients with ‘standard’ haematological diseases can more often be treated closer to home. This potential selection bias was tested by investigating differences in disease frequency and type of treatment in both groups, and no such differences were found.
Had we performed a randomised trial, no baseline differences in post-traumatic growth should have occurred. However, it was rather difficult to recruit patients to this intervention even without randomising them to the two study arms; therefore, it seemed more feasible to perform this trial without randomisation. Patients often did have a strong preference for attending an art therapy intervention; therefore, a randomised allocation to a non-intervention (or waiting group) study arm would have possibly resulted in poor adherence to the study condition as patients could seek other opportunities for attending similar courses.
A third explanation would be that although the intervention had an effect on post-traumatic growth, it was not measured appropriately by the instrument we used, the SRGS (Park et al., 1996). As participants of the intervention in our previous qualitative study (Geue et al., 2011; Götze et al., 2007; Singer et al., 2010; Weiss et al., 2005) had indicated that personal growth was one of the major effects of the program, this explanation is likely to be true. It is possible that some kind of emotional growth is experienced during the program but that this experience is something other than post-traumatic growth as conceptualised by Park et al. (1996). Another difficulty could have been that the SRGS was not sensitive enough to measure changes within a period of half a year. However, variance of SRGS scores was relatively high within our study population: there were patients who experienced a lot of growth between the first and second measurement points and some who did not. Therefore, insensitivity to change is not a likely explanation for missing differences between the two study groups.
Notably, all intervention studies so far that have shown an intervention effect on post-traumatic growth have not used the SRGS but the Post-traumatic Growth Inventory (PTGI) instead (Dolbier et al., 2010; Garlan et al., 2010; Knaevelsrud et al., 2010). However, we chose to use a unidimensional instrument as this was reported to be conceptually and empirically more valid (Joseph and Linley, 2006).
The final explanation for our results is that the intervention did not in fact enhance post-traumatic growth. This would be in accordance with studies in similar areas such as the sense of coherence research (Antonovsky, 1985; Antonovsky and Sagy, 1986). It has been shown that those constructs are relatively stable, that is, they are mainly changed by major life events but short-time psychosocial interventions are not likely to have a major impact on them (Broda et al., 1996; Sack et al., 1997; Wydler et al., 2000).
Another important premise is that post-traumatic growth results from the struggle with major life crises, not from the crisis itself (Calhoun and Tedeschi, 2001; Joseph and Linley, 2006). Therefore, if someone feels already strong and struggles little, then there will be less growth. This implies that patients with high distress do not necessarily experience less post-traumatic growth but possibly even more (Tedeschi and Calhoun, 2004). The patients in our intervention group had higher baseline levels of distress; this did however not translate into more growth.
Our hypothesis was that art therapy can aid in post-traumatic growth by providing a way to craft narratives about the changes that have occurred and by offering perspectives, both of which are expected to be important factors in successful growth because these narratives force patients to confront questions of meaning and how it can be reconstructed (Tedeschi and Calhoun, 2004). These narratives can produce comprehensibility and through this support growth. Another hypothesised mechanism was that the social support often experienced by participants of group interventions can aid post-traumatic growth. The findings about the role of social support have been varied in the literature. While some studies found an association between perceived support and growth (Cadell et al., 2003; Weiss, 2004), others did not (Maercker and Langner, 2001). However, social support was not related to growth in our trial.
Our conclusion at this point must be that there is no evidence for an effect of weekly art therapy group sessions on post-traumatic growth in patients with haematological malignancies, at least when growth is measured with the SRGS. This finding is in accordance with scepticism towards the concept of growth in the context of adversity, including serious illness, and towards positive psychology in general (Coyne and Tennen, 2010).
Footnotes
Acknowledgements
We would like to acknowledge the time and effort of all the patients who have put into this study, and we are most grateful to them. This article follows the publication guidelines for intervention studies that are published in Journal of Health Psychology 2010, 15: 5–7 and the Transparent Reporting of Evaluations with Nonrandomised Designs (TREND) statement in American Journal of Public Health 2004, 94: 361–366.
Funding
This study was funded by German José Carreras Leukaemia Trust (#DJCLS R 07/38p).