
Abstract
This study examines the psychological factors linking childhood abuse and HIV/sexually transmitted infection outcomes among 190 single homeless women in New York City. Participants were assessed for mental health symptoms, sexually transmitted infections, and exposure to childhood sexual and physical abuse. Findings indicate that the relationship between childhood abuse and HIV/sexually transmitted infection diagnoses during adulthood is mediated by a combination of posttraumatic stress disorder and borderline personality disorder symptoms. Screening single homeless women who report childhood abuse histories for symptoms of both disorders may aid in the identification of individuals particularly vulnerable for HIV infection. Implications for clinical interventions are discussed.
Introduction
The HIV/AIDS pandemic continues to affect women at a steadily increasing rate. Women in the United States currently represent 27 percent of individuals living with the virus, up from 8 percent in 1985 (Centers for Disease Control and Prevention (CDC), 2011). Women with histories of interpersonal violence, abuse, and trauma exposure are at heightened vulnerability for infection. Studies have shown a strong association between interpersonal abuse and behaviors that increase the risk for HIV infection, including using substances during sex, engaging in unprotected sex, and having multiple sexual partners (Jewkes et al., 2002; Raj et al., 2004).
Abuse experienced during childhood, particularly sexual abuse, has been associated with sexual risk–taking during adulthood (Newman et al., 2004; Senn et al., 2006) in addition to sexually transmitted infections (STIs) and HIV (Ohene et al., 2005). This problem reflects a larger pattern seen on a global level, where childhood physical abuse (CPA) and childhood sexual abuse (CSA) have been related to long-term negative health outcomes among women (Sickel et al., 2002; So-kum Tang et al., 2011).Some women may be at greater risk of experiencing adverse health consequences connected to early abuse. For example, women who are homeless or unstably housed report experiencing physical and sexual abuse throughout the course of their lives at substantially higher rates than women in general community samples (Henny et al., 2007; Rayburn et al., 2005), thus exacerbating their risk for HIV and STIs, drug abuse, and other health-related problems. Several studies indicate that homeless and unstably housed women are disproportionately affected by HIV/AIDS and STIs (Forney et al., 2007; Kilbourne et al., 2002). Within this population, single homeless women may be particularly vulnerable to infection risk, given that they experience higher levels of stressful life events and more frequently report histories of domestic violence and sexual violence compared to homeless women with children (Zugazaga, 2004).
Research has identified posttraumatic stress disorder (PTSD) as a psychological factor linking interpersonal abuse, such as CSA and CPA, with HIV/STI diagnoses during adulthood. Research shows that PTSD symptomatology (e.g. avoidance, hyperarousal, dissociation, and re-experiencing) may interfere with information processing, risk perception, and self-protective responses in a manner that increases risk for revictimization and sexual behaviors associated with HIV/STI diagnoses (Chu, 1992; Fortier et al., 2009). Little is known, however, about other psychological disorders that may play a role in mediating this relationship among homeless women. Clarifying the pathways through which homeless women may become vulnerable to risk-taking and infection is critical for the development of effective HIV/STI preventive interventions.
Aside from PTSD, one plausible psychological factor that could further elucidate the link between childhood abuse and HIV/STI diagnoses is borderline personality disorder (BPD). The frequency of PTSD among individuals with BPD is high based on comorbidity studies (Pagura et al., 2010; Zanarini et al., 2003). Given the strong association between the disorders and childhood abuse, it has been proposed that BPD and PTSD have a common pathogenesis (Lewis and Grenyer, 2009). One common pathologic process could involve early traumatic experiences, which are often reported among individuals diagnosed with PTSD and BPD (Gunderson and Sabo, 1993; Lewis and Grenyer, 2009). Along these lines, some researchers have proposed that trauma stemming from early CSA may put an individual at greater risk for developing both disorders (Heffernan and Cloitre, 2000). More studies are needed to examine this issue, particularly since many people with BPD do not report experiencing any early traumatic event (Chapman and Gratz, 2007). Clearly, investigating the roles that PTSD and BPD play in the relationship between childhood abuse and HIV/STIs may strengthen our understanding of the underlying processes that affect risk-taking (Messman-Moore et al., 2010).
In this cross-sectional study, we explored a potential mediational model in which PTSD and BPD symptoms served as mechanisms in explaining the link between childhood abuse and HIV/STI diagnoses during adulthood. The purpose of the study was to compare the roles of these disorders among single homeless women in the relationship between early abuse and sexual risk outcomes (i.e. an HIV/STI diagnosis). We focused on single homeless women due to their relatively high levels of lifetime stress and violence. Specifically, we wanted to know whether the link between abuse experienced during childhood and subsequent risk outcomes in this vulnerable population is explained by either heightened levels of PTSD or BPD symptoms alone, or as a combination of heightened symptom levels from the two disorders. We predicted that while PTSD and BPD symptoms would be associated with both forms of childhood abuse and sexual risk outcomes, a combination of heightened symptom levels from the two disorders would mediate this relationship.
Methods
Participants
Women were eligible for the study if they were 18 years of age or older, could communicate in English or Spanish, and could comprehend the terms and conditions of voluntary informed consent. In all, 329 women living in New York City shelters were interviewed and tested for HIV and STIs. The current study is based on sample participants who reported their marital status as “single/never married” during study interviews (n = 190).
Procedure
The study was carried out in cooperation with the Department of Homeless Services, the municipal agency responsible for the provision of shelter care in New York City. Homeless women living in shelters located throughout the city were recruited for the study between 2007 and 2008. Study sampling occurred in two phases. During the first phase, 28 shelters (emergency and transitional) were randomly selected from 126 facilities in New York City. The 28 shelters were stratified by shelter type (e.g. shelters for families with children, shelters for families made up of two or more adults, and shelters for single adults with or without services for people with mental illness or substance abuse) and size (under 40 units and over 40 units). Within each stratum, shelters were sampled with probability proportional to sample size. In the second phase, bed or room numbers were randomly selected from each of the 28 selected shelters. Research staff mailed a description of the study to residents occupying the selected bed or room and requested interested participants to contact them during an on-site scheduled visit. There were no medical or psychiatric exclusion criteria.
Trained research staff conducted HIV and STI testing and study interviews on-site in a private area in shelter facilities. Interviews were carried out on the day of entry into the study. Recruitment and interviews were conducted in both English and Spanish. Each study participant received a gift card valued between US$35 and US$50 for participation in the study. When the study was planned, the gift card amount was set at US$35. Shortly after data collection began, it was suggested by some shelter staff members that a US$50 gift card would be more of an incentive, so the amount was increased early during study implementation. The Columbia University Medical Center and New York City Department of Homeless Services Institutional Review Boards approved all study procedures.
Measures
Demographic data
Participants provided demographic data, including information on their homelessness history, education, age, children, and marital status through the use of an Audio Computer-Assisted Self-Interview (ACASI; Metzger et al., 2000).
PTSD
We used the Posttraumatic Stress Checklist (PCL-C; Weathers et al., 1991) to assess for PTSD symptom levels based on a standardized self-report scale and Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) criteria.
BPD
To assess for BPD, we used the McLean Screening Instrument for BPD (MSI-BPD; Zanarini et al., 2003). The instrument consists of 10 questions self-administered by the participant. As suggested by Zanarini et al. (2003), a participant was classified as screening positive for BPD if she endorsed 7 of the 10 items from the MSI-BPD.
CSA
The Childhood Sexual Abuse Interview (CSAI), which consists of questions for adults that evaluate a history of specific sexual experiences before the age of 15 years, was used in the study. Interview questions were generated from a list created by Finkelhor (1979) and supplemented with questions by Sgroi (1982). Participants were asked if they had experiences related to inappropriate touching by or sex with an adult. Participant responses were converted into a dichotomous categorical variable to indicate the experience of any CSA.
CPA
We used the Childhood Trauma Questionnaire–Short Form (CTQ-SF; Bernstein et al., 2003) to assess childhood maltreatment histories. Participant responses were converted into a dichotomous categorical variable to indicate whether the individual experienced CPA.
HIV/STI diagnoses
To assess for HIV and STIs, we used a measure based on a combination of laboratory and self-reported information. We biologically confirmed the presence of HIV (Orasure fluid test with Western blot confirmatory test), chlamydia, and gonorrhea (urine tests) and obtained information from participants on previous diagnoses with STIs. We gathered data on the following infections: HIV/AIDS, hepatitis B, hepatitis C, syphilis, gonorrhea, herpes, chlamydia, trichomoniasis, genital warts, and “any other” STIs. The number of STIs combined with any HIV seropositive test diagnoses derived from laboratory results and self-report were summed and then converted into a dichotomous categorical variable to indicate the existence of an HIV/STI diagnosis.
Data analytic strategy
Data analysis was performed using the Predictive Analytics Software (PASW) 18.0 (also known as SPSS; SPSS, 2009). For the purposes of analysis, we divided the sample into four distinct subgroups consisting of participants who (1) screened positive for PTSD but did not for BPD, (2) screened positive for BPD but not for PTSD, (3) screened positive for both PTSD and BPD, and (4) screened positive neither for PTSD nor for BPD.
To compare differences between sample subgroups in age and homelessness duration, we used analyses of variance (ANOVAs). To compare the differences in education, race/ethnicity, number of children under 18 years of age, and reports of interpersonal violence or abuse, we used the chi-squared test. We also used the chi-squared test to compare the differences in HIV/STI diagnoses. The significance level for all statistical tests was set at 95 percent (α = 0.05).
Race/ethnicity analyses were based on the African-American, Hispanic, multiethnic, and other/unknown categories. Due to the small sample sizes for Caucasians (n = 12), Asians (n = 3), American Indians/Alaskan Native (n = 4), and Native Hawaiian/Pacific Islander (n = 1), these participants were collapsed into the category designated as “other/unknown.” Adjusted residuals were calculated for contingency tables. An adjusted residual greater than or equal to the absolute value of 2.0 was considered contributing to significance.
The current study explored potential mediational models that depicted a causal link between childhood abuse and HIV/STI diagnoses, with three psychological dummy variables (i.e. PTSD symptoms, BPD symptoms, or a combination of a PTSD and BPD symptoms) serving as mediators. We used Baron and Kenny’s (1986) model for mediation to examine whether the psychological variable served as an underlying mechanism explaining the relationship between early abuse and HIV/STI diagnoses.
Results
Sample description
Demographic, childhood abuse history, and HIV/STI diagnoses for the sample are presented in Table 1. The table provides a breakdown of these characteristics for the entire sample (n = 190) as well as for participants based on whether they screened positive only for PTSD, only for BPD, a combination of both, or neither. Overall, participants who screened positive only for PTSD represented 17 percent of the sample (n = 32). Participants who screened positive for BPD accounted for 7 percent of the sample (n = 13). Participants who screened positive for both PTSD and BPD represented 12 percent of the sample (n = 23). Overall, 64 percent of participants (n = 122) had neither PTSD nor BPD symptoms at screening level cutoffs. In general, based on columns 2 and 4 in Table 1, 29 percent (n = 55) of the sample met screening criteria for PTSD. Combining columns 3 and 4 shows that 19 percent (n = 36) of participants had BPD symptoms that reached screening levels.
Demographic, childhood abuse history, and HIV/STI diagnoses of 190 homeless women in New York City grouped by screening positive for PTSD, BPD, and both disorders.
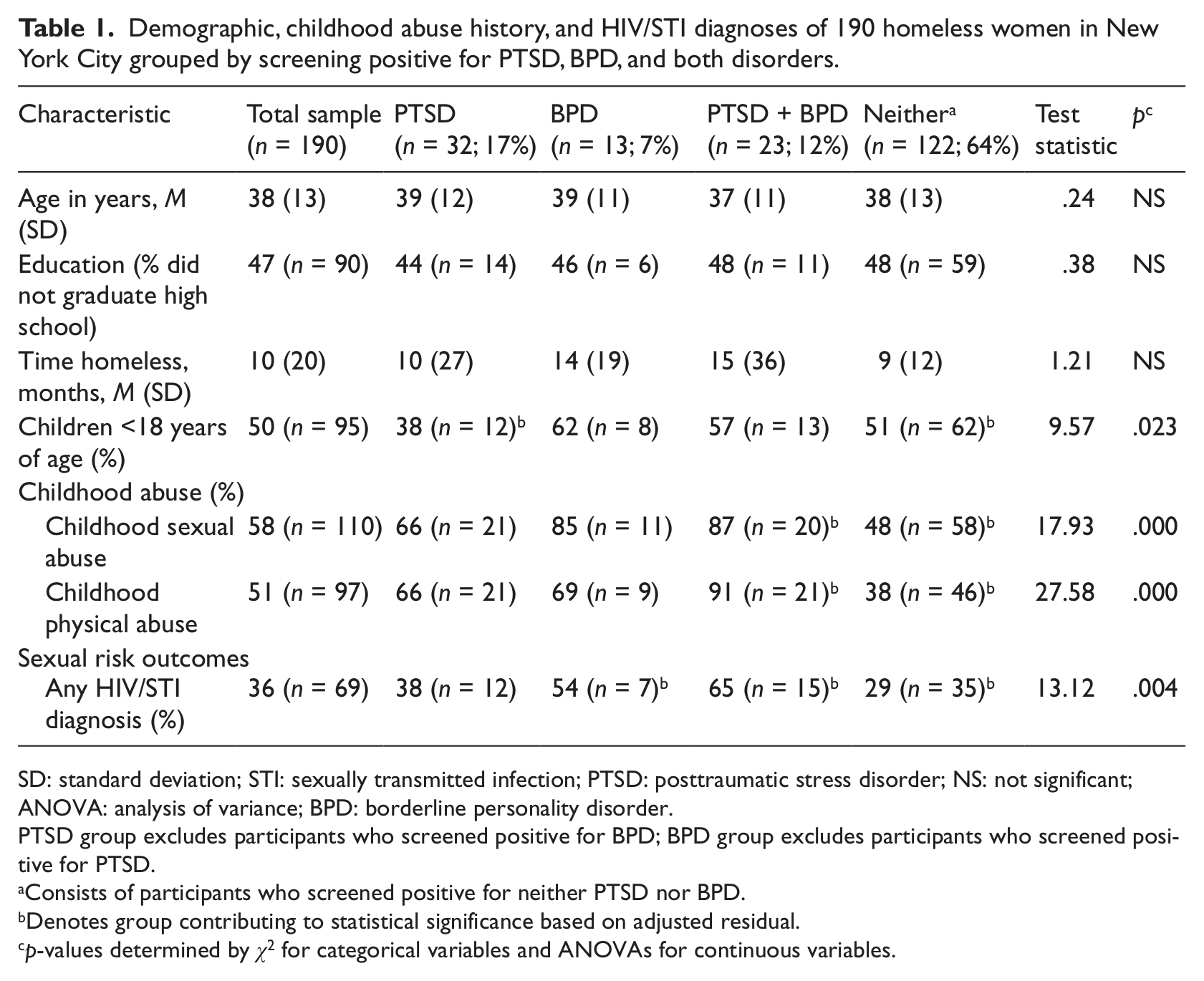
SD: standard deviation; STI: sexually transmitted infection; PTSD: posttraumatic stress disorder; NS: not significant; ANOVA: analysis of variance; BPD: borderline personality disorder.
PTSD group excludes participants who screened positive for BPD; BPD group excludes participants who screened positive for PTSD.
Consists of participants who screened positive for neither PTSD nor BPD.
Denotes group contributing to statistical significance based on adjusted residual.
p-values determined by χ2 for categorical variables and ANOVAs for continuous variables.
Participants reported a mean age of 38 years (range = 18–65 years), 47 percent did not graduate high school, and most identified as African-American or Hispanic (67.3%; n = 120). As shown in Table 1, there were no statistically significant differences between participants in the four subgroups with regard to demographic characteristics such as age, education, or length of homelessness status. There were, however, significant differences between the subgroups with regard to whether a participant had children under 18 years of age. Women who screened positive for PTSD without heightened BPD symptom levels were less likely than other women in this sample to have younger children, that is, 54 percent versus percentages ranging from 68.4 percent to 88.9 percent for the other three subgroups, χ2 (3, n = 124) = 9.6; p < .05.
Relationship between childhood abuse, PTSD, and BPD symptoms
A history of CSA and/or CPA was reported by nearly 66 percent (n = 125) of the sample. A total of 58 percent of participants reported CSA while 51 percent reported CPA. As shown in Table 1, there was no statistically significant relationship between either form of child abuse and whether a participant screened positive only for PTSD diagnosis or BPD symptoms. In contrast, participants who screened positive for both PTSD and BPD were more likely to report such early histories of abuse. Compared to other participants, women in this subgroup reported the highest rates of CSA and CPA (87% and 91%, respectively). Women who had neither screened positive for PTSD diagnosis nor BPD were less likely to report either form of childhood abuse. Within this subgroup, CSA and CPA rates fell considerably below figures for the overall sample (48% and 38%, respectively).
HIV/STI diagnoses
HIV/STI diagnoses were associated with both CSA (Spearman’s rho = .18, p = .01) and CPA (Spearman’s rho = .17, p = .02). Women with a history of CSA were significantly more likely than women without such a background to have been diagnosed with HIV or a STI (43.6% vs 26.3%). Similarly, women with a history of CPA were more likely to have ever had an HIV/STI diagnosis than those who did not report this form of early abuse (44% vs 21.5%).
With regard to psychological factors, there was no significant relationship between whether a woman screened positive only for PTSD and had HIV/STI diagnoses. However, participants were more likely to have an HIV/STI diagnosis if they had either screened positive only for BPD or PTSD combined with BPD (see Table 1). Participants who had symptom levels of PTSD and BPD that did not reach screening cutoff levels for either disorder were less likely to have been diagnosed with HIV or a STI.
Psychological factors linking abuse and HIV/STI diagnoses
To function as a mediator, a variable must be significantly related to both the independent variable and the dependent variable (see Baron and Kenny, 1986). As indicated earlier, an examination of correlations indicated that only one of the psychological variables, PTSD and BPD symptoms at screening cutoff levels, met this requirement. Thus, we tested a mediational model with this variable as a mediator in two separate analyses with both forms of childhood abuse as the predictors and HIV/STI diagnoses as the criterion. Both mediational analyses tested in this study controlled for the independent effects of PTSD symptoms, BPD symptoms, or not having sufficient symptoms of either disorder at screening cutoff levels by entering each psychological subgroup simultaneously in the mediational model along with the combined PTSD–BPD variable.
We found that the model testing the effect of the combined PTSD–BPD variable in the relationship between CSA and HIV/STI diagnoses met each of the three conditions for mediation (see Figure 1). When having PTSD and BPD symptoms was added to the link between CSA and HIV/STI diagnoses, the association was attenuated: the odds ratio decreased from 2.18 to 1.67, and the association was no longer statistically significant(p = .13).

Model depicting relationship between childhood sexual abuse (CSA) and HIV/STI diagnoses with PTSD combined with borderline personality disorder symptoms as mediator.
Similarly, as depicted in Figure 2, we found that the PTSD–BPD variable mediated the relationship between CPA and HIV/STI diagnoses (see Figure 2). When the PTSD–BPD variable was added, the odds ratio decreased from 2.02 to 1.46 and the association between CPA and HIV/STI diagnoses became nonsignificant (p = .27). Thus, PTSD symptoms combined with the symptoms of BPD mediated the relationship between both forms of childhood abuse and HIV/STI diagnoses among participants in this sample of homeless women.
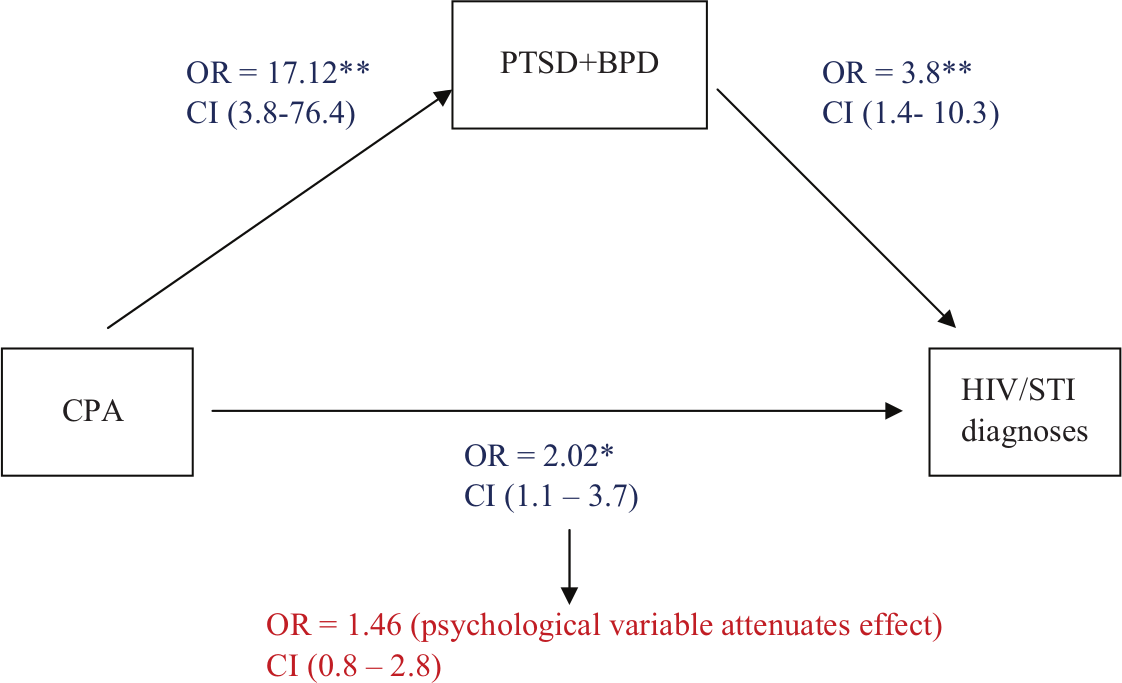
Model depicting relationship between childhood physical abuse (CPA) and HIV/STI diagnoses with PTSD combined with borderline personality disorder symptoms as mediator.
Discussion
The primary goal of this study was to examine the psychological factors linking sexual and physical abuse experienced during childhood with subsequent HIV/STI diagnoses among single homeless women. While childhood abuse was significantly related to HIV/STI diagnoses during adulthood, there were no significant associations between either form of childhood abuse and either symptoms of PTSD or BPD when symptoms of the two disorders were examined independently. Our findings showed that for participants in this sample, abuse was related to the symptoms of these disorders only when symptoms of both disorders reached screening cutoff levels. These findings contrast with other studies investigating the link between childhood abuse and sexual risk outcomes during adulthood in that PTSD symptoms alone did not have a significant relationship (Limberg et al., 2011; Schulze et al., 2011). Given the overlap between PTSD and BPD, this study has several implications for future research and clinical interventions targeting homeless women with histories of early abuse.
There are limitations to this investigation that deserve mention. One limitation is that the sample consists of homeless women in New York City shelters, and thus, our findings may not be generalizable to other groups of homeless women. Future studies should examine the link between child abuse and sexual risk outcomes in other samples of homeless women in other geographical areas. A second limitation is that the sampling procedure we used did not include facilities associated with the HIV/AIDS Services Administration (HASA), a separate municipal system of shelter care for residentially unstable persons known to be HIV positive who meet specific stage of illness admission criteria. For this reason, it is likely that HIV/STI diagnoses reported here represent a conservative estimate of actual levels found among single homeless women. In a similar vein, HIV/STI diagnoses may have been further underestimated in this study because they were based on a combination laboratory assessments and participant self-reports. In contrast to biological or laboratory data, self-reports of HIV STIs have been viewed as presenting reliability concerns. These limitations notwithstanding, we believe our study makes an important contribution to our understanding of the psychological factors linking childhood abuse with HIV risk behaviors among single homeless women.
Our finding that the relationship between childhood abuse and HIV/STI diagnoses during adulthood among single homeless women was mediated by PTSD symptoms only when combined with BPD at screening cutoff levels should draw renewed attention to the connection between the two disorders, particularly as it relates to the development of interventions. The conceptual and phenomenological relationship between PTSD and BPD has long been recognized (Lewis and Grenyer, 2009; Pagura et al., 2010). The two disorders often overlap, and their connection to trauma has been well supported in the research literature. One domain where the two disorders appear similar relates to emotion dysregulation, or deficits in an individual’s ability to recognize and manage extreme and changing emotional states (Bradley et al., 2011; Weiss et al., 2012). This characteristic has been linked to HIV risk behaviors in other studies (e.g. Messman-Moore et al., 2010) as well as impulsivity and substance use.
Much of the research literature to date has focused on PTSD as a psychological factor in explaining the relationship between childhood abuse and sexual risk behavior outcomes (Henny et al., 2007; Rayburn et al., 2005; Simoni and Ng, 2000). In contrast to other studies, our findings indicate that PTSD symptoms alone did not have a significant relationship in the link between early abuse and sexual risk outcomes during adulthood. Heightened impulsivity is characteristic shared by individuals with either PTSD or BPD. It is possible that for this sample of single homeless women, however, symptoms related to impulsivity were not strong enough to prompt risk-taking behaviors unless PTSD symptoms were accompanied by BPD symptoms as well. This would be consistent with previous research that indicated that among women diagnosed with PTSD, the addition of a BPD diagnosis resulted in significantly greater levels of impulsivity and general dysfunction (Zlotnick et al., 2003). Furthermore, in this vein, research indicates that individuals with both PTSD and BPD are more adversely affected by emotion dysregulation, psychological distress, and suicidal and nonsuicidal self-injury than those with BPD alone (Harned et al.,2010; Marshall-Berenz et al., 2011). As suggested by Marshall-Berenz et al. (2011), emotion dysregulation among individuals with comorbid symptoms may reach threshold levels that dramatically alters their ability to engage in adaptive coping when faced with distress. Future research should examine the role of emotion dysregulation in sexual risk outcomes among single homeless women with histories of early abuse and how interventions may be designed to address this factor.
Few studies have examined the role of Axis II disorders on risk outcomes among homeless women with histories of early abuse (Ball et al., 2005). Even though many personality disorders are comorbid with Axis I disorders, such as PTSD, little attention has been directed to examine their role in HIV/STI diagnoses among homeless populations. Findings from the current study provide clear rationale for more comprehensively screening individuals for mental disorders, particularly victims of child abuse. Such information could be particularly valuable in developing HIV/STI preventive interventions tailored for these individuals.
Footnotes
Acknowledgements
We would like to thank Beth Brodsky, Curtis Dolezal, Zoe Edelstein, and Martina Pavlicova for their assistance and support in completing this report..
Funding
Dr. Houston was supported by a training grant from the National Institute of Mental Health (T32 MH019139; Behavioral Sciences Research in HIV Infection; Principal Investigator, Theodorus Sandfort, Ph.D.). This research was supported by Grant R01 DA 019399 from the National Institute on Drug Abuse to the Center for Homelessness Prevention Studies at Columbia University (Carol L.M. Caton, Ph.D., Principal Investigator). The content is solely the responsibility of the authors and does not necessarily represent the official views of NIDA or the NIH.