
Abstract
This article explores the concept and measurement of health literacy in the context of shared health decision-making. It draws upon a series of qualitative and quantitative studies undertaken in the development and evaluation of a bowel cancer screening decision aid for low literacy populations. The findings indicate that different types of health literacy (functional, interactive and critical) are required in decision-making and present a set of instruments to assess and discriminate between higher level health literacy skills required for engagement in decision-making. It concludes that greater sophistication in both the definition and measurement of health literacy in research is needed.
Keywords
Introduction
Health literacy is a complex and evolving phenomenon that has generated global interest and debate concerning its definition and measurement. Since the 1970s, health literacy has been defined and conceptualized in multiple ways (Sorensen et al., 2012), ranging from the ability to perform health-related literacy and numeracy tasks (Ad Hoc Committee on Health Literacy for the Council on Scientific Affairs, American Medical Association, 1999), to a much wide range of cognitive and social skills that enable people to obtain, understand and use information to enhance their health and well-being, and engage in health-care decision-making (Institute of Medicine, 2004; Nutbeam, 1998, 2000). The concept has also evolved concurrently from two different settings – in clinical care where health literacy is seen as a risk factor for poor health and poor compliance with health-care advice and in public health where health literacy is seen as a personal asset offering greater autonomy and control over health decision-making (Mårtensson and Hensing, 2011; Nutbeam, 2008; Pleasant and Kuruvilla, 2008).
Recent conceptualizations, derived from qualitative studies with patients and health-care professionals, have identified a range of abilities considered important for accessing, understanding and using health information (Buchbinder et al., 2011; Jordan et al., 2010). These include knowing when and where to seek health information, the capacity to retain and process information, and the communication and application skills necessary to act on it. A generic framework put forward by Edwards et al. (2012) states that health literacy develops over time and is represented by stages of building health knowledge, developing health-related skills and practices, displaying health actions, the production of informed options and making an informed decision; outcomes include increased knowledge and greater participation in decision-making (Edwards et al., 2012).
Although it is variously defined and conceptualized, there is consistent evidence that health literacy is a key determinant of health and may explain variations in health status among populations across a range of outcomes. Adults with low health literacy have been shown to have poorer health knowledge and understanding of disease, poorer self-care management and higher rates of morbidity and mortality from chronic disease (Berkman et al., 2011). At the same time, these populations experience greater difficulties participating in shared decision-making (also termed informed decision-making or informed choice) – the practice of understanding the nature or risk of a condition, being aware of the possible preventative or treatment options and the likelihood of benefits and harms of each option, being able to integrate personal values and preferences into decision-making, participate in the decision to a level desired and have the confidence to implement the decision (Barry and Edgman-Levitan, 2012; Charles et al., 1997). There is some evidence that these capabilities can be developed through educational intervention and the use of literacy-sensitive materials (Coulter and Ellins, 2007).
This article draws upon a series of qualitative and quantitative studies undertaken between 2005 and 2009 to inform the development and evaluation of a decision aid for bowel cancer screening. The decision aid was designed to help adults with lower education and literacy participate in shared decisions about whether or not to participate in a nationally available faecal occult blood test (FOBT) screening program. Data from these studies have been used to examine relative differences in health literacy (functional, interactive and critical) suggested by Nutbeam’s conceptual model and some of the related challenges arising in the measurement of health literacy.
Relative differences in health literacy: functional, interactive and critical health literacy
A well-established model of health literacy is that proposed by Nutbeam (Box 1). This distinguishes between three different types of health literacy: functional, interactive and critical health literacy (Nutbeam, 2000). This multi-level approach to health literacy is highly relevant for shared decision-making as it reflects the relative differences in skills required to obtain and use information in ways that progressively lead to greater autonomy and empowerment in health-related decision-making.
Nutbeam’s conceptual model has been practically applied to a variety of health and geographical settings (Levin-Zamir and Peterburg, 2001; St Leger, 2001; Wang, 2000). More recently, it has been used to tackle the social determinants of health through critical health literacy skill development (Mogford et al., 2011) and better understand how carers use their interactive skills to coordinate their children’s care (Pizur-Barnekow et al., 2011). There is however scope to explore the usefulness of this model in other health contexts, to consider how the different dimensions operate and can be measured.
Nutbeam’s three-level model of health literacy.
Functional health literacy is the ability to obtain, understand and use factual information on health risks and on how to use the health system. Information will generally convey limited goals directed towards improved knowledge of health risks and services, and compliance with prescribed actions. Typically, such information does not invite interaction, critical thinking or autonomy in decision-making.
Interactive health literacy is defined as the ability to extract health information and derive meaning from different forms of communication, and to apply new information to changing circumstances. It is characterized by the self-confidence to act independently on advice, and to interact successfully with the health-care system and providers.
Critical health literacy reflects the literacy and numeracy skills that support critical reflection on information or advice received, including recognition of the influence of wider social determinants of health. These include the ability to obtain, understand and critically appraise different sources of information, and the ability to engage in shared decision-making.
The way health literacy is conceptualized has implications for how it is measured. Just like literacy, health literacy can be measured in absolute terms by distinguishing between those who can perform tasks (e.g. reading health materials) and those who cannot, and in relative terms, by assessing the differences in skill between those who are able to perform relatively challenging tasks (e.g. participating in shared decision-making) and those who are not (Nutbeam, 2009). Most established health literacy instruments focus on functional health literacy (Davis et al., 1991; Parker et al., 1995; Weiss et al., 2005). Although these measures play a critical role in research, they are less capable of assessing differences in the levels of skill and understanding that are required for more complex health-related tasks (Nutbeam, 2009).
To date, few attempts have been made to develop health literacy measurement tools that capture the multidimensional nature of the construct and incorporate assessments of interactive and critical health literacy skills (Baker, 2006; Pleasant et al., 2011). Ishikawa et al. (2008) have developed a self-report measure to assess perceived functional, communicative and critical health literacy skills among diabetic patients. Similarly, Rubin et al. (2011) have developed an instrument, the Measure of Interactive Health Literacy, to directly assess the extent to which people participate in health consultations (Rubin et al., 2011). Initiatives are also underway to develop comprehensive measures (e.g. the Health Literacy Measurement Scale), incorporating a range of competencies identified by patients and health professionals as important for understanding and using health information (Buchbinder et al., 2011, Jordan et al., 2010).
Methods
Overview of study elements
This article draws upon a series of qualitative and quantitative studies undertaken between 2005 and 2009 to inform the development and evaluation of a decision aid booklet designed to help adults with lower education and literacy participate in shared decisions about bowel cancer screening.
The decision aid presented tailored information for men and women aged 55–64 years for different family history groups about the possible outcomes of screening (and not screening) using the FOBT. This included bowel cancer mortality with and without screening; the chances of having a false-positive or false-negative result; interval cancers; removal of polyps detected by colonoscopy and bowel cancer detected by screening. Copies of the decision aids can be found at http://sydney.edu.au/medicine/public-health/step/publications/decisionaids.php. It was specifically targeted to populations with lower education and literacy using strategies such as reducing the amount of text on each page, minimizing the use of jargon, explaining medical terms in a glossary, using the active voice, providing contextual information before factual information and integrating visual illustrations to support key concepts and messages (Doak et al., 1996; Doak et al., 1998; Houts et al., 2006).
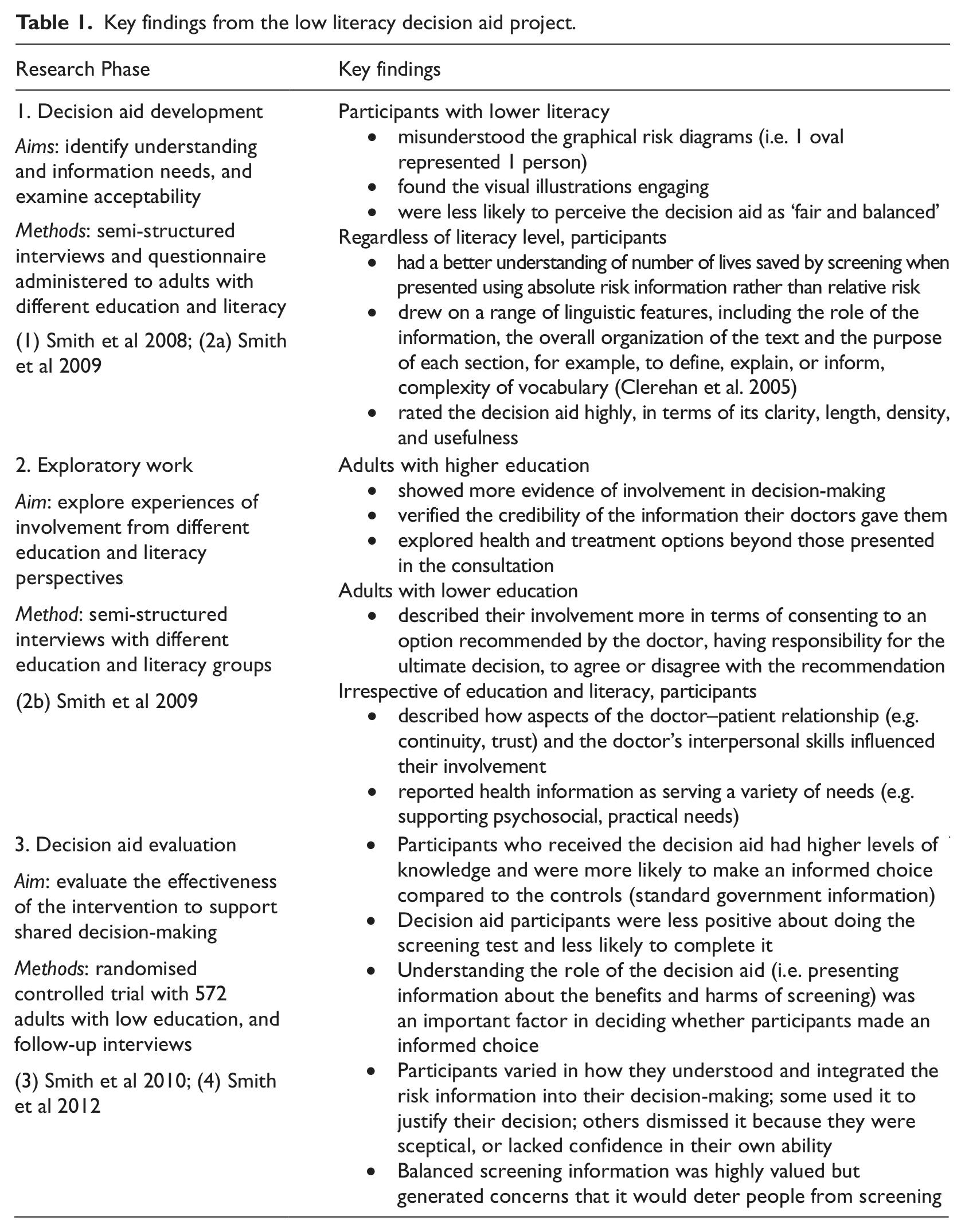
This mixed methods study design comprised three phases; relevant findings from each phase are summarized in Table 1:
Decision aid development involving semi-structured interviews and survey work with high and low literacy groups to examine information needs, design preferences and understanding (1) Smith et al 2008; (2a) Smith et al 2009.
Exploratory work involving semi-structured interviews with different education and literacy groups, to compare and contrast their experiences of involvement in health decision-making (2b) Smith et al 2009.
Decision aid evaluation among low education and literacy groups, involving a randomized controlled trial and a follow-up interview study (3) Smith et al 2010; (4) Smith et al 2012.
Key findings from the low literacy decision aid project.
Examining and measuring the relative differences in health literacy
Consideration of the relative differences in health literacy has been guided by Nutbeam’s (2000) original definitions of functional, interactive and critical health literacy, and adapted accordingly. The framework displayed in Table 2 illustrates how the three levels of health literacy potentially operate during decision-making about bowel cancer screening. Furthermore, it identifies the relevant skills at each level and the potential measures that could be used to assess outcomes. Combining the insights from our original study (Table 1) afforded the opportunity to (re)examine how the different levels of health literacy functioned during the decision-making process.
A framework depicting the practical application of the different levels of health literacy in the context of decisions about bowel cancer screening.
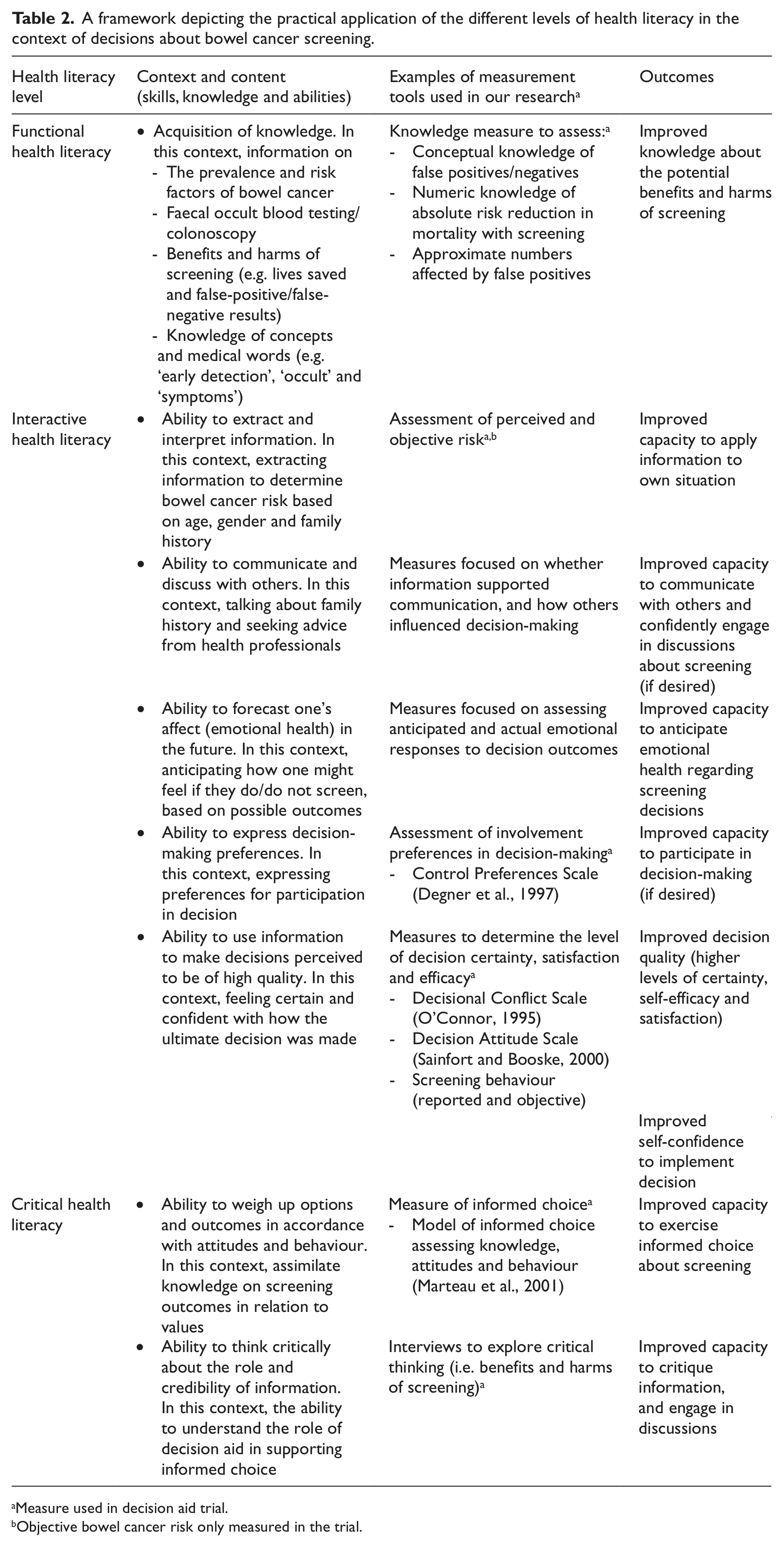
Measure used in decision aid trial.
Objective bowel cancer risk only measured in the trial.
Findings
Examining the relative differences in health literacy for shared decisions about bowel cancer screening
The following results are organized to reflect the relative differences in functional, interactive and critical health literacy that we observed by re-examining the data. These findings provide evidence (or not) for how each level of health literacy functioned in this specific decision-making context among high and low education and literacy groups.
Functional health literacy: a basic understanding of factual health information
From our study, it was evident that functional literacy skills in basic reading (i.e. word recognition and reading sentences) were essential for a person to be able to decode and make sense of the textual information in the decision aid. These basic reading comprehension skills formed an important basis in which individuals could attain specific knowledge, grasp abstract concepts, and subsequently go onto to perform higher level literacy tasks such as making inferences from the text.
It was also important for individuals to possess numeracy and graphical literacy skills – the ability to process and interpret the statistical risk information presented in a graphical format. This was because the decision aid contained risk information using graphical formats (systematic oval diagrams), to communicate the potential benefits and harms of screening outcomes. Specifically, these skills enabled participants to estimate how many lives were saved by screening (compared to no screening), and the likelihood of experiencing a false-positive or false-negative test result.
Interactive health literacy: cognitive and social skills required to extract meaning and apply information
Our data provide evidence that participants (including those with basic reading skills) engaged in advanced cognitive activities to make sense of the information. These higher order processes involved retaining, extracting and assimilating new and pre-existing information. This enabled participants to verify whether the new information fitted (or conflicted) with their existing knowledge. In more concrete terms, we observed that the prior knowledge that people had about cancer screening information (i.e. screening is beneficial) seemed to conflict with the new information in the decision aid, promoting informed choice ((1) Smith et al 2008; (2a) Smith et al 2009). People may not expect to receive balanced information about the possible benefits and harms of participating nor realize that they have a choice in the matter. In this regard, participants constructed their own meaning based on their prior knowledge. Participants’ prior knowledge (or ‘schema’) was therefore challenged by information offering them a choice and asking them to consider the potential harms of screening. To explain these findings, we draw on an alternative model of health communication based on systemic functional linguistics that (a) highlights the importance of the cultural and social context within which the reader acquires information and (b) considers how the readers’ beliefs influence the way they construct meaning from the text (Clerehan et al., 2005; Hirsh et al., 2009).
Our combined observations demonstrated that participants used their communication skills to discuss the information with significant others (family and peers) ((2b) Smith et al 2009). Most people seemed to use the information to facilitate conversations with family members to identify their bowel cancer family history and inform others about the FOBT. Some participants also consulted their doctor and sought their opinion as to whether they should do the test (1) Smith et al 2008; (2a) Smith et al 2009. The ability to formulate questions, express concerns and query advice were identified as relevant skills, enabling people to communicate effectively with health-care professionals.
It was evident that once the decision to screen had been made, participants needed the confidence to act on the information and implement their decision. The FOBT is a self-sampling kit, so completing the test requires individuals to have reading and practical skills to follow instructions and complete forms.
Critical health literacy: higher level cognitive and social skills to critically analyse information and use information to exert greater control over situations
Building on the higher level literacy skills outlined earlier, participants critiqued the information, both in terms of questioning its credibility and in terms of critically thinking about the purpose of the decision aid in the broader social context (1) Smith et al 2008 (4) Smith et al 2012. With regard to the former, we observed that some participants were sceptical of the risk information and questioned the extent to which population statistics could be applied to their individual situation due to the inherent uncertainty associated with statistical information. As a result, they did not integrate it into their decision-making.
In terms of understanding the role of the decision aid, participants were often confused by its function, and that it was offering them a choice rather than encouraging them to do the screening test (1) Smith et al 2008. Thus, having a choice in this context seemed unfamiliar, and participants were surprised that the information was not promoting the benefits of screening. Knowing that there was a decision to be made about screening and that a choice exists appeared to be critical factors influencing people’s ability to make an informed choice (4) Smith et al 2012, that is, their ability to weigh up their options (i.e. screening vs no screening) and related outcomes (bowel cancer mortality, chance of false positives, false negatives, interval cancers and risks associated with follow-up testing), in relation to their values.
Practical implications for health literacy measurement
Designing an instrument to measure functional, interactive and critical health literacy
The results provided evidence that all three levels of health literacy operated during people’s decision-making process. This has implications for health literacy measurement, and how one might use these observations to develop an instrument to (a) operationalize the measurement of health literacy skills in this specific context, from basic health literacy skills through to higher health level skills and (b) assess the relative differences in people’s health literacy skills to make informed decisions.
Table 1 provides examples of relevant measures we selected or adapted for the health literacy instrument used in the trial ((3) Smith et al 2010). Most of the measures were quantitative and assessed people’s perceived capabilities, including the ability to make an informed choice, express preferences for involvement, appraise the materials and elicit decision uncertainty, satisfaction and confidence. Qualitative approaches were also used to explore how people critically engaged with the material.
Discussion
Through our study, we were able to gain insight into the role of different types of health literacy (functional, interactive and critical) for shared decisions about bowel cancer screening and demonstrate the feasibility of developing and using a measurement tool designed to examine relative differences in health literacy. All three levels of health literacy were equally important in this decision-making context: functional health literacy for acquiring screening knowledge; interactive health literacy for extracting information, communicating with others and expressing preferences for involvement; and critical health literacy for critically thinking about the role and credibility of the information.
Our study advances our understanding of health literacy by shedding light on how the three different types of health literacy might correspond to one another. Notably, the interaction between the three levels appeared to be an iterative process, with participants’ moving back and forth between them as they made their decision, affording greater knowledge, informed choice and involvement in decision-making. For example, participants’ decision may have been the result of acquiring knowledge (functional health literacy), discussing bowel cancer family history with a family member (interactive), considering the risk information in relation to personal circumstances (interactive), questioning the information about the number of lives saved by screening (critical), seeking advice from a health-care professional (interactive), re-reading the information (functional) and so on. Thus, there are multiple sequences in which the different types of health literacy could have operated, suggesting that this process was not a linear one. It might therefore be best to view health literacy, in this context, as a continuous interplay between the three levels and place equal value on all forms of the concept (Kickbusch, 2009).
We found that people with lower education and literacy exhibited interactive and critical health literacy skills, implying that although a certain base level of literacy is required to engage with information, understanding the gist or bottom-line meaning of the information (i.e. screening involves potential benefits and harms) appeared sufficient to engage in activities requiring interactive and critical health literacy, such as seeking advice from others and understanding the role of the information. The reverse is also valid: high functional (health) literacy is no guarantee that an individual will demonstrate interactive and critical literacy skills. Similarly, Ishikawa and Yano (2011) reported that functional health literacy scores on a subjective measurement scale poorly correlated with interactive and critical health literacy scores. Together, this suggests that each component encompasses a different set of skills and capabilities that are not entirely dependent on each other; a person may achieve critical health literacy without possessing high functional skills (Chinn, 2011). Furthermore, an individual’s confidence and ability to engage in discussions with a health professional may be unrelated to their functional skills; a person’s perceptions of their social position in relation to the doctor’s might influence discussions rather than their literacy skill (2b) Smith et al 2009.
Our findings support the idea that health literacy should be regarded context and content specific; what it means to be health literate in one setting will be different in another. Bowel cancer screening is a discrete health decision that requires specific skills and content knowledge to make a shared decision. Thus, being able to demonstrate critical literacy skills in one context (e.g. in making informed choice in screening) is no guarantee that the same individual would be able to apply the same skill set in another context (e.g. in the management of a chronic condition that requires different knowledge and applications over a prolonged period of time) (Von Wagner et al., 2009).
We found striking similarities in the way health literacy has been conceptualized by the existing models compared to our own insights. Jordan et al. (2010) identified seven core abilities considered important for accessing, understanding and using health information (Jordan et al., 2010). These include knowing when to seek health information and knowing where to seek health information, verbal communication skills, assertiveness, literacy, capacity to retain and process information and application skills. Some of the abilities overlap with the key skills derived from our own research, namely, reading comprehension skills, oral communication skills and cognitive skills in retaining, processing and synthesizing information. We also note that two of the abilities identified in the study of Jordan et al. were not observed in our study, namely, knowing when and where to seek health information. However, this may be because the information was sent to participants and they were not expected to seek it themselves.
Similarly, there is overlap between the current study and the themes presented in Buchbinderet al.’s (2011) model. For instance, the skills described in three of Buchbinder et al.’s themes are similar to those found in the current studies: (a) expression/communication skills (e.g. ability to ‘say no’, ‘communicate with health-care professionals’ and ‘express values and priorities to health-care professionals’); (b) information skills (e.g. ‘reading, understanding and retaining information’, ‘learning how to work with health information’, ‘putting information into context’, ‘being critical/sceptical’, ‘discerning reliable from unreliable information’, ‘synthesizing information’, ‘having a sense of perspective (relative importance of all information and experiences)’, ‘understanding disease’, ‘receiving knowledge’ and ‘working out what you want to know’ and (c) management skills (e.g. making comparisons, weighing up options and making choices).
Our study supports Edwards et al.’s (2012) theoretical pathway model that suggests that health literacy develops along a trajectory through the development of greater knowledge, and improved self management and engagement in decision-making (informed and shared). Although the model was developed in the context of people living with long-term conditions, it is still relevant for thinking about how people participate in decision-making in a relatively shorter period of time. Through our study, we observed that participants progressed through a series of stages as they made their screening decision – participants built their health knowledge through reading the decision aid – applied their health literacy skills, displayed health actions such as seeking advice from health professionals, identified their options and participated in decision-making. This, in turn, led to increased levels of knowledge and greater participation in decision-making.
Traditionally, health literacy tools have largely focused on assessing functional health literacy (Abel, 2008). If health literacy is defined more broadly in terms of using cognitive and social skills to negotiate with a health-care professional or to critically evaluate information, then existing instruments are not appropriate (Baker, 2006; Nutbeam, 2008; Pleasant et al., 2011). Through our broader assessment of health literacy, we were able to discriminate between participants’ abilities to acquire knowledge and apply their skills to participate in shared decision-making. Furthermore, we suggest that the measures commonly used to evaluate shared decision-making (e.g. decisional conflict and decision self-efficacy) can be applied to the assessment of the multi-levelled concept of health literacy, particularly interactive and critical health literacy. We do however note the limitations of our study. First, the framework is focused on a very specific health setting and is therefore limited in application. Nonetheless, it does provide a foundation for others to draw on when considering how health literacy might be operationalized and measured in other shared decision-making contexts.
Our research also prompts consideration of the way health literacy is measured. Except for our assessment of knowledge, most of the measures used in the trial were self-report. Although this method of assessment might be particularly useful in low literacy populations by reducing feelings of shame associated with direct measurement (Jordan et al., 2010), they do not offer an assessment of a person’s actual capabilities. Further research might consider including direct assessments of skills. For example, in the context of the current study, the Measurement of Interactive Health Literacy could have been applied to assess the extent to which the decision aid enabled participants to confidently engage in discussions with their doctor about screening (Rubin et al., 2011).
Overall, the experiences gained from this set of studies point to the need for greater clarity in the definition of health literacy in reported studies. In particular, we highlight the need to distinguish between the relative differences in health literacy required to obtain, understand and use information for health in different contexts. Our study also illustrates the challenge of developing valid and reliable instruments to measure these different levels of health literacy both directly, and through self-report.
Footnotes
Acknowledgements
We thank all the participants who took part in the various studies throughout this program of research.
Conflict of interests
None declared.
Funding
This research was supported by project grants awarded to Associate Professor Kirsten McCaffery from the National Health and Medical Research Council of Australia (no. 457381) and the University of Sydney Cancer Research Fund. The funders had no role in the design or conduct of the studies, in the collection, analysis and interpretation of data, or in the preparation or approval of the article. Dr Sian Smith is funded by an Australian National Health and Medical Research Council Early Career Fellowship (no. 1034912).