
Abstract
Insights for action in the relatively new field of health literacy have been constrained by the emphasis on the literacy skills of the individuals. Early studies into the relationship between literacy and health outcomes were not appropriately balanced with examinations of individuals’ skills and health system demands. Most studies focused on the measures of patients’ reading skills without due attention to the health tasks undertaken, the health materials used, or the skills of providers with whom patients were interacting. Furthermore, public health is founded on the epidemiologic notion of the reciprocal relationship between individuals and environments. Early studies in health literacy did not attend to context—the physical and social environment of health-care settings. New initiatives in health literacy must bring attention to the demands and expectations of health systems and to the proficiencies of the various health professionals who prepare documents and information for the public and who interact with communities and patients.
Keywords
Introduction
Health literacy research was spurred by the findings from the initial International Adult Literacy Surveys (IALS) of the 1990s (Kirsch et al., 1993) and the Adult Literacy and Lifeskills Survey (ALLS) in the early part of this century (Statistics Canada, 2005). Over the years, health researchers have successfully answered the initial research question generated by the dissemination of findings in the health field: given the limited literacy skills of large numbers of adults in industrialized nations, are there health consequences? The answer, provided through a wealth of studies, is yes. Indeed, limited literacy, as measured by reading skills, is associated with limited participation in health promoting and disease detection activities, with diminished management of chronic diseases, with increased hospitalization and rehospitalization, and with increased morbidity and mortality (Berkman et al., 2011; Rudd et al., 2007).
More recently, researchers have expanded the scope of inquiry to examine a broader range of literacy skills. For example, studies of numeracy skills (Apter et al., 2006, 2008; Montori and Rothman, 2005), listening skills (Rosenfeld et al., 2011), and speaking skills (Martin et al., 2011) add further insight into the findings of links between literacy skills and health outcomes. Consequently, the topic of health literacy has attracted the attention of practitioners and policy makers who seek to apply research insights into practice and policy guidelines.
Because of the attention given to measuring the skills or deficits of patients, the logical policy and practice consequences appear to focus on the education sector and call for improved skill development through primary and secondary schools. Indeed, health practitioners are not, after all, literacy educators. However, evidence of health disparities and of increased morbidity and mortality among those with limited literacy skills raises issues of social justice and does not allow for the time needed to improve the public’s skills. Unfortunately, research findings did not initially provide clear action options for those of us in the health sector beyond increasing the public’s literacy skills.
The narrow focus on skills of individuals evident in the emerging field may well have been tied to the definition of terms adapted from Nutbeam’s (1998) very early definition and adopted by the US Department of Health and Human Services (2000) and the Institute of Medicine (2004): the degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions. This focus on individual capacity appears to ignore the broader health context within which people function, often referred to as the demand side. The adopted definition of health literacy had initially shaped the field by influencing the focus and scope of inquiry—as do all definitions. Furthermore, measurement tools, rightly focused on articulated and defined variables, are shaped by definitions of key terms. In this way, definitions influence the rigor of any individual study and a field as a whole (Rudd et al., 2012).
Insights for efficacious action may well have been constrained by this research emphasis on the literacy skills of individuals and by a critical omission. Early studies into the relationship between literacy and health outcomes were not appropriately balanced. Educators, for example, do not offer measures of individual’s reading skills without measures of text difficulties and complexity nor would they measure listening skills without attention to the clarity of the speaker. Most health literacy studies, in contrast, focused on the measures of patients’ reading skills without due attention to the health tasks undertaken, the health materials used, or the communication skills of the professionals.
Furthermore, early studies in health literacy did not factor in attention to the physical or social environment of health-care settings. Public health is founded on the epidemiologic notion of the reciprocal relationship between individuals and environments. As we examine people’s ability to access health information, navigate health systems, and partner with health professionals, we must also consider the quality of the information, materials, and tools provided to the members of the public and to the environments within which professionals and members of the lay public are expected to act. New initiatives in health literacy are bringing attention to the demands and expectations of health systems and to the proficiencies of the various health professionals who prepare documents and information for the public and who interact with communities and patients.
Access to information
As is noted earlier, definitions of basic health literacy emphasize the expectation that people will access and act on health information (Institute of Medicine, 2004; Nutbeam, 1998). However, well over 1500 peer-reviewed studies indicate that health materials, across a wide swath of content areas and formats (such as patient brochures; discharge instructions; or medicine directions, forms, lists, and charts), have been poorly designed, poorly written, and geared to a very sophisticated audience. A strong body of evidence establishes a clear mismatch between the literacy demands of health materials (in print and on-line) and the literacy skills of adults with secondary school education (Rudd et al., 2007). Consequently, health information is not truly accessible. Logically, the first call to action requires change in the way health information is offered in print, on-line, or in discussions (often referred to as the oral exchange).
Thus, important insight for action has been gleaned from this second strand of health literacy research focused on the assessments of written and posted health communication materials. Findings indicate that the problem is not entirely located in the literacy deficits of patients. Recommendations related to print and on-line materials include calls for institutional review boards with well articulated minimum requirements for rigorous pilot testing with the members of intended audiences, evidence of revisions related to ease of use and clarity, and reports of assessment processes and findings.
Recommendations for “talk,” so essential for information exchange, problem identification, and action, are drawn from the studies of professional/patient communication. In addition, plain language associations are encouraging health professionals to relearn their first language, sometimes referred to as “kitchen-talk” or “living room language” for use with the public and patients. Professional organizations, such as the American Medical Association, the American Dental Association, the American College of Physicians, and the American Psychological Association, are considering plain language as a critical skill, along with other articulated communication competencies, for schooling and possibly for licensing examinations.
Studies, editorials, and myriad guidebooks encourage health providers to offer definition of terms, concrete examples, illustrations, narratives, and to provide tools for review and reminder cues. Furthermore, providers are encouraged to focus on problem solving and action steps and to use a “what to do if …” format in discussion with and instructions for patients.
Studies of the oral exchange are providing insights for action as well. Normative restructuring suggested by researchers has long called for actively encouraging and supporting question asking (Roter, 2004; Stewart, 1995). Current best practice guidelines in health literacy call for the use critical communication checks such as teach-back where the professional avoids the question: do you understand and instead checks by asking for help: I want to be sure that I included all the important information about your medicine; tell me what you will do … (Harper et al., 2007; Schillinger et al., 2003).
Overall, health literacy recommendations to improve access to information call for all health professionals to improve the clarity and quality of their written and spoken health information. Although emerging studies of changes in text and in talk offer evidence of improved outcomes, additional efforts are called for. Rigorous evaluative studies are needed to establish gold standards.
Access to care and services
Institutions are complex structures and busy work environments with multiple entrances, busy hallways, layered signs, and postings and are filled with the sounds of the foreign languages of medicine, nursing, and varied allied health professionals. Such institutions require sophisticated navigation skills (Rudd et al., 2005). Best practices call for shame-free environments where patients and visitors feel comfortable asking for help, where people feel welcomed, where help is offered to all, where clear signs and postings ease the burden of way finding, where materials are provided and are well-designed for use, and where talk is friendly and jargon free. For example, the Joint Commission of Accreditation of Healthcare Organizations (2007) calls upon institutions to take action and responsibility for patient safety with attention to health literacy.
Studies of the literacy demands of health institutions have been launched (Groene and Rudd, 2011) but clear standards have not yet emerged. The Institute of Medicine’s Round Table on Health Literacy has disseminated an initial report to spur such discussions (Brach et al., 2012; Hernandez, 2012). The proposals assert that health literacy organizations are attentive to workforce communication skills and to accessible information. Specific and well-tested action steps are needed to establish gold standards of quality of care. At the same time, multiple tools are readily available to help both clinical staff and administrators experience health-care settings from the perspective of patients and visitors, to examine and assess the social and physical environments of health and health-care settings and to identify and remove barriers (Agency for Healthcare Research and Quality, 2010; DeWalt et al., 2011; Rudd and Anderson, 2007; Rudd et al., 2004).
The emerging strategy draws from Kurt Lewin’s Force Field Theory (Lewin, 1948). Lewin calls for an identification of facilitating factors and barriers but he urges attention to the removal of barriers as a first step. One cannot, for example, urge people to access information that is inaccessible or to ask questions in an environment that discourages interruptions. Initial studies conducted in health facilities have found multiple but similar barriers across countries and locations. They include problematic websites, phone interactions, and street signs; poorly marked entrances, passageways, and destination points; complex maps that do not match signs or place colors; and jargon-filled forms for health and family background information, for legal documents such as informed consent, and for critical directions such as those for test preparations or for discharge home care. Recommendations point to the need for orientation booklets, staff training, way finding measures, and improved documents that have been rigorously developed and tested (Groene and Rudd, 2011).
Efficacious action
There are calls, across most industrialized nations, for evidence-based research to shape policy decisions. Research focused on the links between literacy skills of patients and health outcomes has clearly established the untoward health outcomes related to patients’ limited literacy skills (although, as noted, without needed attention to the demand side). However, there is a comparative paucity of research studies focused on efficacious action.
The two dominant strands of research in health literacy have successfully documented the health literacy skills of individuals and the complex burden of health materials in print across many health topics and specialty areas. Missing from the literature are studies that document the contribution of professionals’ communication skills and techniques. Measures of the communication skills of public health and health-care professionals are needed. Furthermore, the literacy-related demands and assumptions of health and health-care institutions must be more systematically captured. Such actions would set the foundation for studies of change and for examinations of links between skills/demands and health outcomes of patients. This would then enable us to develop action options and engage in comparative analyses of change strategies.
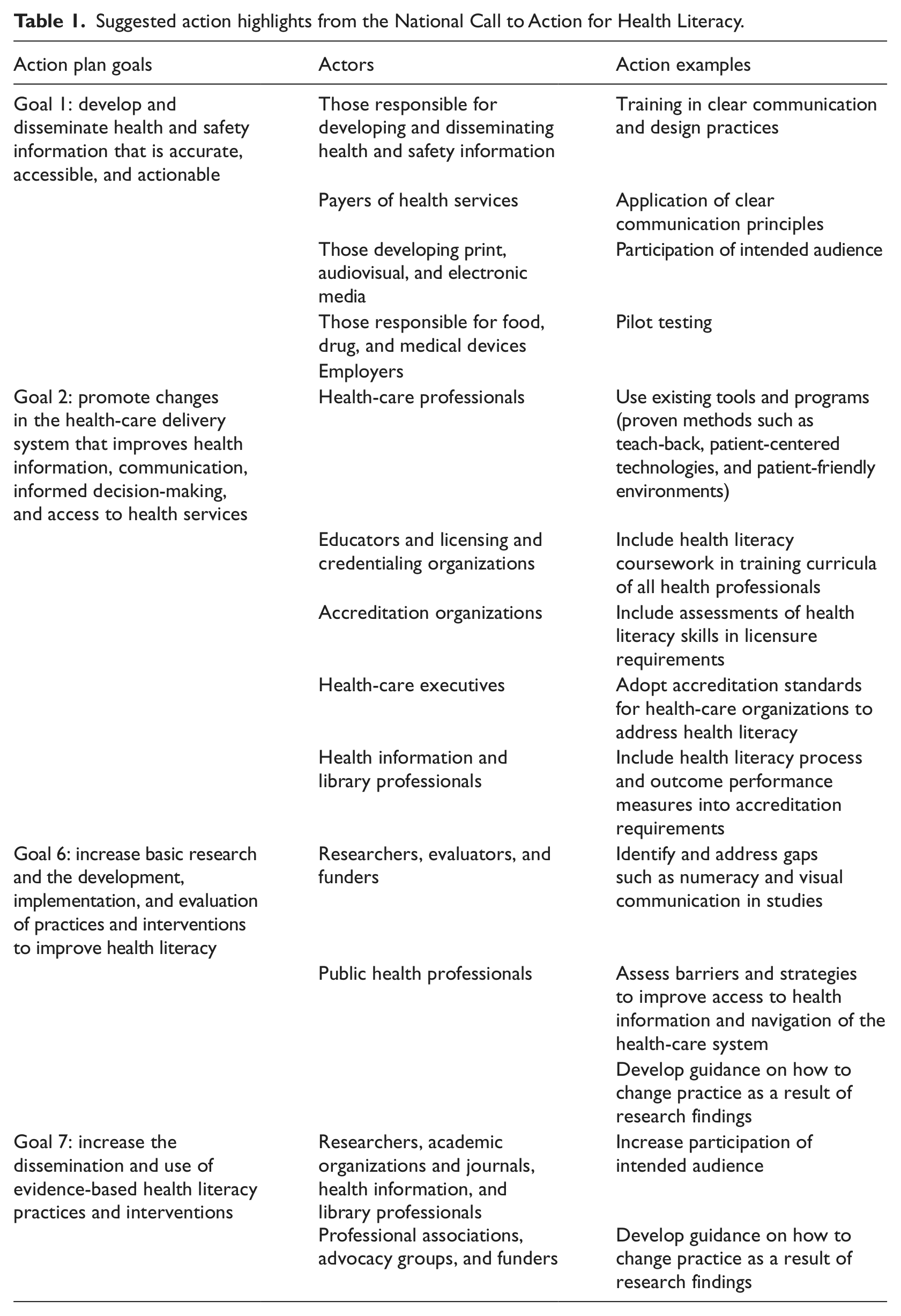
Many guidelines for action can be found in The National Action Plan to Improve Health Literacy. This document calls for government and institutional responsibilities for making health and safety information accessible, for improving professional education, and for developing standards of professional skills. In addition, the National Action Plan encourages researchers to develop measures of professional skills; to establish measures of literacy-related barriers to information and care; and to encourage a focus on intervention studies, the development of gold standards, and the subsequent use of evidence-based health literacy practice. Table 1 offers highlights of suggested action. These recommendations indicate a shift away from mere identification of the problem toward the development of professional standards and institutional policy regulations (Office of Disease Prevention and Health Promotion, 2010).
Suggested action highlights from the National Call to Action for Health Literacy.
Conclusions
While we must call on the education sector to improve the literacy skills of our populations, we in the health fields must take action to remove literacy-related barriers to information, to services, and to care. As we seek to improve health literacy, research attention and institutional resources must be given to the removal of the barriers that constrain efficacious action.
Careful examinations of the social and physical environments of health services are needed. Here, attention must be paid to the aspects of institutional cultures such as written and spoken languages, expectations, and procedures. Initial studies point to the need for awareness building, orientation for all staff, and plain language training. In addition, policy regulations must address the design and development of critical texts that can have life and death consequences. Such texts include directions on medicine labels, instructions related to self-care, as well as legal documents. These needed actions are not confined to medicine and health care. Indeed, the Plain Writing Act of 2010 (the Act) (2010) calling for writing that is clear, concise, and well organized is spurring the development of training programs for all personnel in government offices—including all those focused on health information and all health-related agencies such as Centers for Disease Control (Office of Management and Budget, 2011). At the same time, consideration must be given to professional education and licensing and to institutional procedures and protocols.
Health literacy studies must now provide insights for needed change to make information more accessible, tools more usable, information exchanges more productive, and navigation of institutions easier and more dignified. Documented untoward health outcomes as a result of the mismatch between skills and demands make a call to action an ethical imperative.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.