
Abstract
Little is known about the psychosocial circumstances under which children develop excessive body mass. A community sample was followed up from age 2–10 years to determine which early problems were predictive of increased body mass index. Hypothesized mediators (i.e. eating habits, physical activity, and “screen time”) were also examined. After controlling for parental psychopathology, family income, child’s gender, and child’s body mass index, externalizing behaviors, aggressive behaviors, and anger predicted a relatively high body mass index. Exploratory analyses did not support hypothesized mediators, although low power was an issue.
Introduction
Obesity is a leading cause of preventable death in the United States (Flegal et al., 2005), and epidemiological studies have demonstrated that the prevalence of obesity is increasing among American children (Hedley et al., 2004). Although the primary cause of overweight and obesity is well known (i.e. caloric intake that exceeds caloric expenditure), few studies have explored the psychosocial circumstances under which caloric overconsumption is most likely to occur during childhood. Identification of psychosocial predictors of childhood obesity may lead to the development of effective prevention programs and may allow clinicians help children and adolescents to avoid experiencing the unfortunate correlates of being obese (e.g. poor body esteem; Mak et al., 2013).
To date, a few robust predictors of childhood obesity have been identified. Cross-sectional studies have shown that children living in low socioeconomic status (SES) conditions are more likely to be overweight or obese than peers living in average or high SES environments (Grow et al., 2010). Additionally, cross-sectional studies have demonstrated that children whose parents are overweight are more likely to be overweight or obese than children whose parents are of normal weight (Danielzik et al., 2004). Documented prospective psychosocial/environmental risk factors for childhood obesity include short sleep duration (Touchette et al., 2008), low physical activity levels (Reichert et al., 2009), and frequent television viewing (Hancox and Poulton, 2006).
Some cross-sectional studies have examined the specific link between increased body mass index (BMI) and psychopathology. In a community sample of children and adolescents, Lamertz et al. (2002) found no association between obesity or overweight and any mental disorder. Britz et al. (2000), in contrast, reported higher rates of mood, anxiety, somatoform, and eating disorders in a clinical sample of obese adolescents than in control adolescents, and Erermis et al. (2004) reported higher rates of depression among obese adolescents than among normal weight adolescents. Thus, results from cross-sectional studies have been inconsistent.
Less research has been conducted on the types of maladaptive emotions and behaviors that may increase a child’s risk for the development of overweight or obesity prospectively. Mustillo et al. (2003) found a link between chronic obesity in childhood and Oppositional Defiant Disorder among both boys and girls, and a link between chronic obesity and depression in boys. Anderson et al. (2010) also found a prospective link between externalizing disorders in early childhood and increased BMI at age 12. Furthermore, Goodman and Whitaker (2002) demonstrated that depression prospectively predicted obesity among adolescents. In contrast, Bradley et al. (2008) reported that neither internalizing nor externalizing problems in early childhood predicted increased BMI by late childhood.
To date, no theoretical models have been put forth that attempt to explain the link between psychosocial factors and subsequent obesity among children. Therefore, we present a theoretical model that exemplifies our conceptualization of how early life psychosocial variables are linked to an elevated BMI in late childhood (see Figure 1).
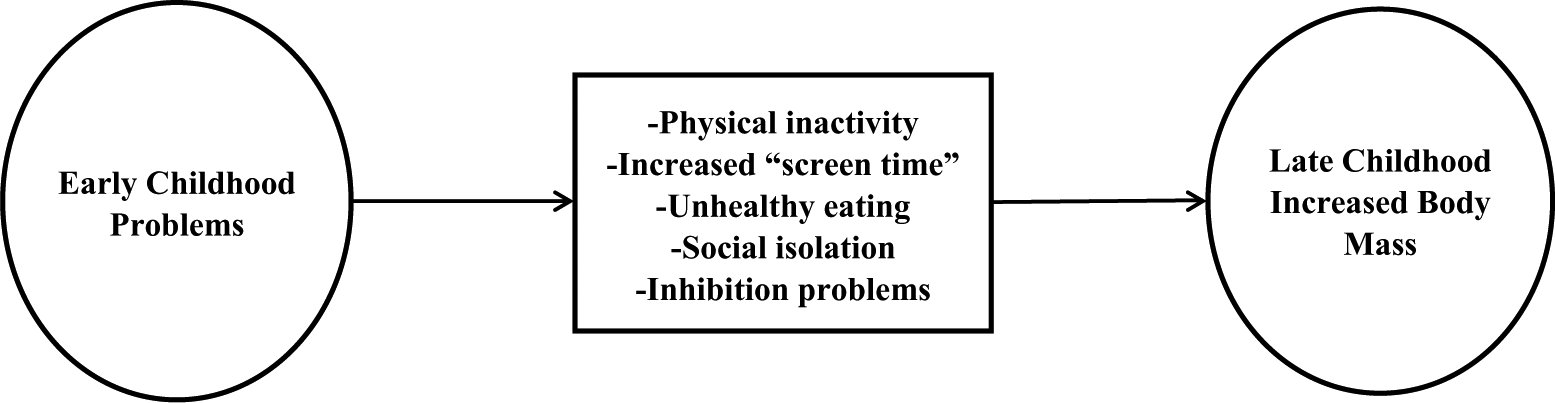
Theoretical model of early childhood problems leading to elevated body mass in late childhood.
Furthermore, most of the published research on obesity and psychopathology in children has used clinical samples recruited because of obesity and/or mental health concerns (e.g. Csabi et al., 2000); however, the prevalence of psychiatric disorders among referred samples may differ from the prevalence among community samples (Cohen and Cohen, 1984). Thus, the primary purpose of this study was to determine whether maladaptive emotional and behavioral patterns (i.e. internalizing and externalizing problems) in 24-month-old children from a community sample prospectively predict BMI and body shape/size in late childhood (i.e. at age 10). Furthermore, this study was designed to conduct an exploratory test of the mediational model depicted in Figure 1.
Method
Participants and procedure
The initial pool of participants was selected randomly from nine senior high schools and participated in three assessments from 1987 to 1999 as part of the Oregon Adolescent Depression Project (OADP). Detailed descriptions pertaining to recruitment, sampling, and participation rates have been documented elsewhere (Lewinsohn et al., 1993, 1999). During the period of 1997–2002, those OADP participants who had a newborn infant, became pregnant or whose partner became pregnant over a 3-year recruitment period, lived in Oregon, and wished to participate were recruited for an adjunct study called the Infant Development Study (IDS). These individuals were, henceforth, referred to as IDS probands. Participation rate for eligible families was 83 percent (n = 167), and demographic differences between those who did and those who did not participate were small (see Forbes et al., 2004).
Families were originally recruited to bring their children in at 24 months to fill out questionnaires, complete diagnostic interviews, and participate in laboratory assessments. In 2009 (i.e. approximately 8 years later), we attempted to reestablish contact with these families. Due to funding constraints, we randomly selected half of the original sample (n = 83) to contact and requested that they (a) have the mother complete a questionnaire packet and (b) have their IDS child complete a questionnaire packet. Participating families were offered US$50 in compensation. Attempts to contact nonresponders were extensive (e.g. nonresponders were sent two additional mailings and were called several times, family members of nonresponders were contacted via mail, and Internet search engines were used to establish updated contact information). Informed consent was received from mothers, assent was received from children, and procedures were approved by the Oregon Research Institute (ORI) and the University of Denver Institutional Review Boards.
Of the 83 randomly selected families, 12 (14%) declined to participate, 33 (40%) were not able to be reached due to outdated contact information, and 38 (46%) participated in the current data collection effort. When data were collected at 24 months, there were no differences with regard to race, parental marital status, annual household income, child’s BMI, Child Behavior Checklist (CBCL; Achenbach and Rescorla, 2000) internalizing/externalizing scores, Toddler Behavior Assessment Questionnaire (TBAQ; Goldsmith, 1996) scores, mother’s BMI, or parental psychopathology between those who participated and those who were randomly selected and either declined to participate or were not able to be reached.
The final sample for this study included 38 children (45% female) and their mothers. Children were approximately 10.0 years old (SD = 0.84), whereas their mothers were approximately 36.9 years old (SD = 2.7). The majority of children were White (78.4%), with 18.9 percent of mixed racial/ethnic background and 2.7 percent Asian. The majority of mothers were married (74%), 10 percent were divorced, and the rest were either single or dating. All the mothers had graduated from high school and 53 percent had received a bachelor’s degree or higher. Annual household income was as follows: 1 percent made <US$20,000; 16 percent made between US$21,000 and US$40,000; 18 percent made between US$41,000 and US$60,000; 16 percent made between US$61,000 and US$80,000; 16 percent made between US$81,000 and US$100,000; 13 percent made >US$100,000; and 3 percent did not report household income. Based on time 2 (T2) self-report, mothers’ weights in the current sample were similar to population estimates of weights in adult women (sample mean BMI = 27.50; SD = 6.67; population mean BMI = 28.2; standard error of the mean = 0.2), and mothers’ reports of fathers’ weights suggested that fathers in the current sample had similar body types to those found in population-based studies of American men (mean BMI = 28.50; SD = 6.67; population mean BMI = 27.9; standard error of the mean = 0.1) (Ogden et al., 2004).
Measures
CBCL
The parent-report version for preschool-aged children (i.e. 1.5- to 5-year-olds) was completed by mothers when IDS children were 24 months old. On the CBCL (Achenbach and Rescorla, 2000), caregivers rate each of the items from 0 (not true of child) to 2 (very true or often true of child). The CBCL provides scores on syndrome scales (e.g. Anxious/Depressed, Somatic Complaints) and Diagnostic and Statistical Manual–oriented scales (e.g. Oppositional Defiant Problems). The CBCL has been shown to have strong test–retest and multi-informant reliability (Achenbach and Rescorla, 2000). To test the primary hypothesis, initially, only CBCL Internalizing and Externalizing scores were examined. Whenever either of these scores demonstrated a significant relationship with an outcome variable of interest, its contributing subscales (e.g. Aggressive Behaviors is a subscale of Externalizing Disorders) were also examined in follow-up analyses.
TBAQ
The TBAQ (Goldsmith, 1996) is a measure of temperament that was designed for use with children aged 18–24 months. It measures temperamental dimensions of activity level, tendency to express pleasure, social fearfulness, anger proneness, and interest/persistence. Items are rated on a scale ranging from 1 = never to 7 = always during the past month. TBAQ scores have been shown to have strong reliability and validity (Goldsmith, 1996). This measure was given to the mothers of IDS probands to complete at T1.
Structured Clinical Interview for DSM-IV, nonpatient version
The Structured Clinical Interview for DSM-IV (SCID-IV; First et al., 1994) is a widely used semistructured interview that yields DSM-IV diagnoses. Mothers were interviewed with the SCID-IV to assess their current psychopathology when their children were 24 months old (i.e. at T1). Diagnostic interviewers were carefully trained (e.g. interviewers were required to demonstrate a minimum kappa value of .80 for all symptoms across two consecutive interviews and on one videotaped interview of a participant with evidence of psychopathology). Based on a randomly selected subsample (25%) of interviews, interrater reliability was moderate to excellent (i.e. ranged from .69 to .88) for a variety of disorders.
Child’s BMI
At T1, mothers reported the current height and weight of their children in the questionnaire packet. At T2, mothers again reported the height and weight of their child on a questionnaire. BMI and BMI percentiles were calculated using age and gender norms at T1 and T2 for the children (Centers for Disease Control and Prevention, 2010).
T2 questionnaire packet
For T2, the authors created a questionnaire asking mothers to report demographics and information about their child’s body shape/size, eating habits, physical activity levels, and leisure habits (e.g. video game usage, television watching). From this packet, we used mother’s report of frequency of child’s fast food consumption (using a single item: on average, how many servings of fast food does your child eat per week?), mother’s report of duration of child’s “screen time” (using the total number of hours from the following two items: on average, how many hours of television does your child watch per day? and on average, how many hours of video games does your child play per day?), and mother’s report of child’s body shape/size (using a single item: how would you rate your child’s current body shape/size? 1 = thin, 2 = average, 3 = plump, 4 = fat) as outcome variables. At T2, we also asked children to complete the Physical Activity Questionnaire for Older Children (PAQ-C; Kowalski et al., 1997), and the frequency of physical activity reported on this measure as indicated by the total score of the measure’s nine scoreable items (Cronbach’s alpha = .88) was used as another outcome variable.
Data analytic strategy
The primary aim of this study was to examine whether internalizing or externalizing behaviors were predictive of later childhood BMI; thus, we first examined correlations between T1 variables (i.e. child CBCL Externalizing and Internalizing scores) and T2 variables (i.e. child BMI, child BMI percentile, child fast food consumption, child body shape, child physical activity, child “screen time”) using PASW Statistics 18, Release Version 18.0.3 (2010). The T1 CBCL Externalizing Behavior scores were significantly correlated with several T2 variables; therefore, we examined the correlations between other, more-specific T1 measures of externalizing behavior, which were CBCL Aggressive Behavior, CBCL Destructive Behavior, and TBAQ Anger. Intercorrelations for these variables are provided in Table 1.
Study intercorrelations, means, and standard deviations between all variables.
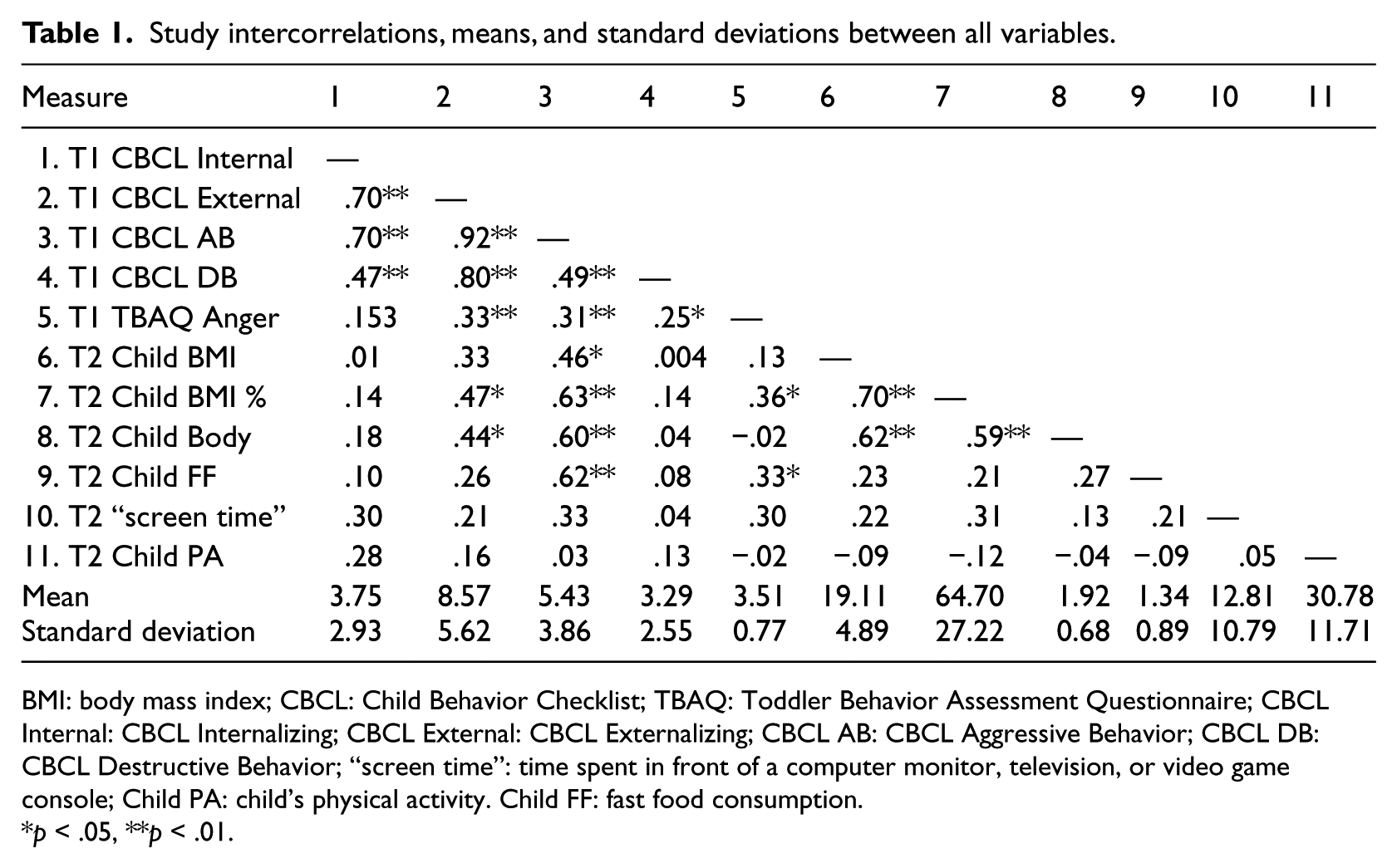
BMI: body mass index; CBCL: Child Behavior Checklist; TBAQ: Toddler Behavior Assessment Questionnaire; CBCL Internal: CBCL Internalizing; CBCL External: CBCL Externalizing; CBCL AB: CBCL Aggressive Behavior; CBCL DB: CBCL Destructive Behavior; “screen time”: time spent in front of a computer monitor, television, or video game console; Child PA: child’s physical activity. Child FF: fast food consumption.
p < .05, **p < .01.
Follow-up tests revealed that T1 CBCL Aggressive Behavior, CBCL Externalizing Behavior, and TBAQ Anger were significantly correlated with at least one of our T2 outcome variables. Therefore, a series of hierarchical multiple regression analyses were conducted using these predictor variables. In each of the regression analyses, child’s gender, child’s BMI at 24 months, annual household income, mother’s psychopathology, and father’s psychopathology were entered as covariates. Next, a measure of externalizing behavior was entered in the second step. We report ΔR2 and f2 for significant effects. ΔR2 is the incremental increase in the model R2 resulting from the addition of a predictor, or set of predictors, to the regression equation. f2 is a measure of effect size; by convention f2 values of 0.02–0.15 are considered small, 0.15–0.35 medium, and >.35 large.
To examine mediators listed in the theoretical model depicted in Figure 1, the PRODuct Confidence Limits for INdirect effects (PRODCLIN) program (MacKinnon et al., 2007) was used. This program tests mediational effects without some of the problems inherent in other methods of testing for mediation (e.g. inflated rates of type I error; see MacKinnon et al., 2002). PRODCLIN examines the product of the unstandardized path coefficients divided by the pooled standard error of the path coefficients (αβ/σαβ) and a confidence interval is generated, wherein a statistically significant mediation effect is indicated by the absence of zero in the confidence interval. A series of mediational analyses were conducted in which various early life psychosocial and psychopathological problems were conceptualized as independent variables, physical activity, fast food consumption, and “screen time” were conceptualized as potential mediators, and late childhood BMI and body shape/size were considered dependent variables.
Results
Descriptive statistics
See Table 1 for means and standard deviations. Based on mothers’ reports at T1, children’s T1 BMI ranged from 13.84 to 22.68 (M = 16.99, SD = 1.77) and associated BMI percentile ranged from the 1st percentile to the 99th percentile (M = 56.42th percentile, SD = 20.39th percentile). Based on mothers’ reports at T2, children’s T2 BMI ranged from 12.2 to 39.10 (M = 19.11, SD = 4.89) and associated BMI percentile ranged from the 5th percentile to the 99th percentile (M = 64.70th percentile, SD = 27.22th percentile).
Hierarchical multiple regression analyses
Child’s gender, child’s BMI at 24 months, annual household income, and parents’ psychopathology were entered in step 1. In step 2, CBCL Externalizing Behavior was added as the independent variable. Controlling for these other variables, CBCL Externalizing Behavior was significant in the prediction of child’s body shape at age 10, β = .67, p = .04, ΔR2 = .23, and f2 = .49 (see Table 2).
T1 CBCL Externalizing Behavior predicting body shape at T2.
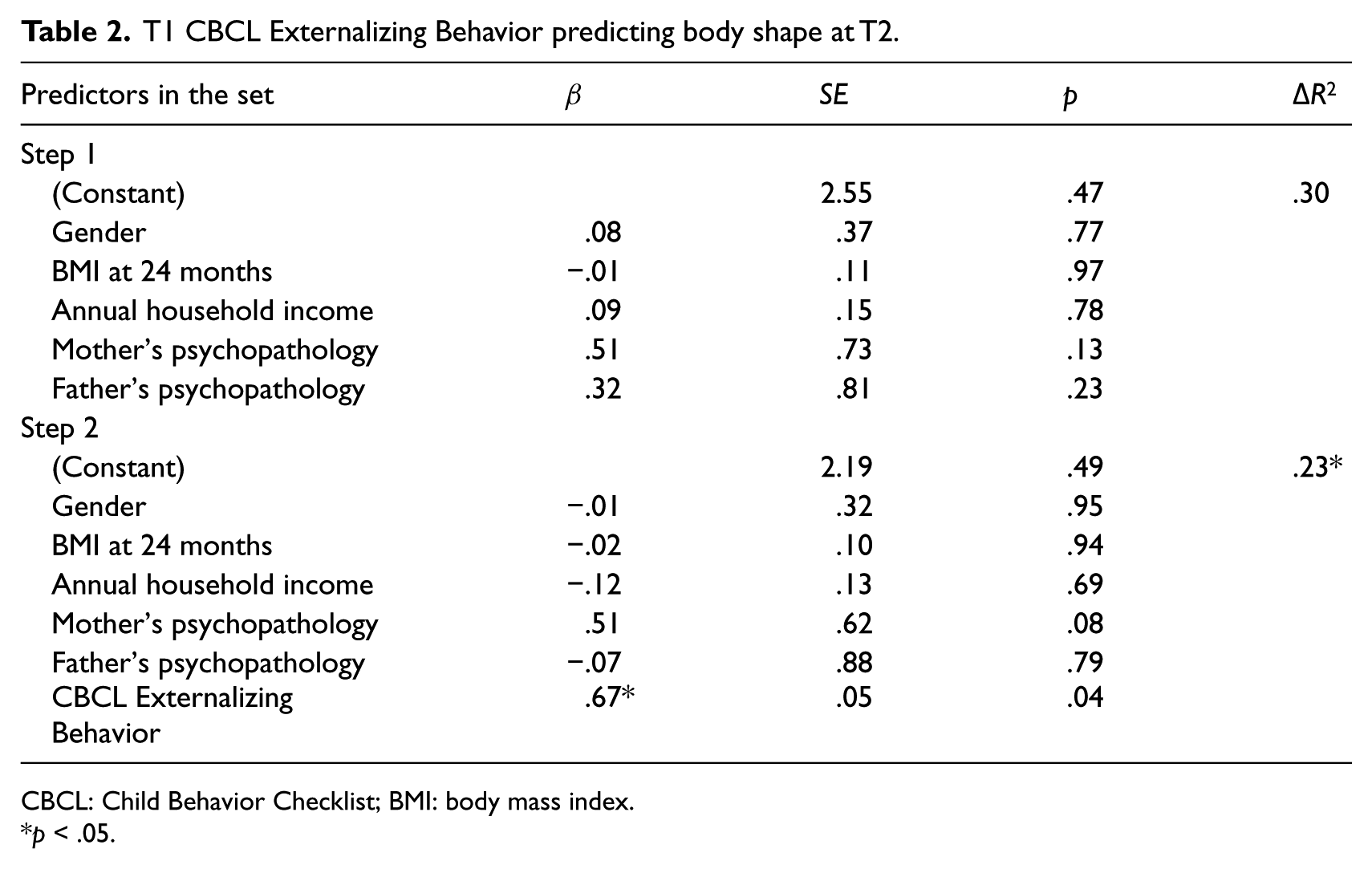
CBCL: Child Behavior Checklist; BMI: body mass index.
p < .05.
Follow-up tests were conducted to assess whether certain types of externalizing behaviors were more predictive of our outcome variables than others. Controlling for the covariates listed above, CBCL Aggressive Behavior significantly predicted BMI percentile at age 10, β = .80, p = .03, ΔR2 = .31, and f2 = .54 and child’s body shape at age 10, β = .94, p = .002, ΔR2 = .43, and f2 = 1.59. As can be seen from Table 3, the presence of an Axis I disorder in the mother also predicted child’s body shape at age 10, β = .64, p = .01.
T1 CBCL Aggressive Behavior predicting BMI percentile, fast food consumption, and body shape at T2.
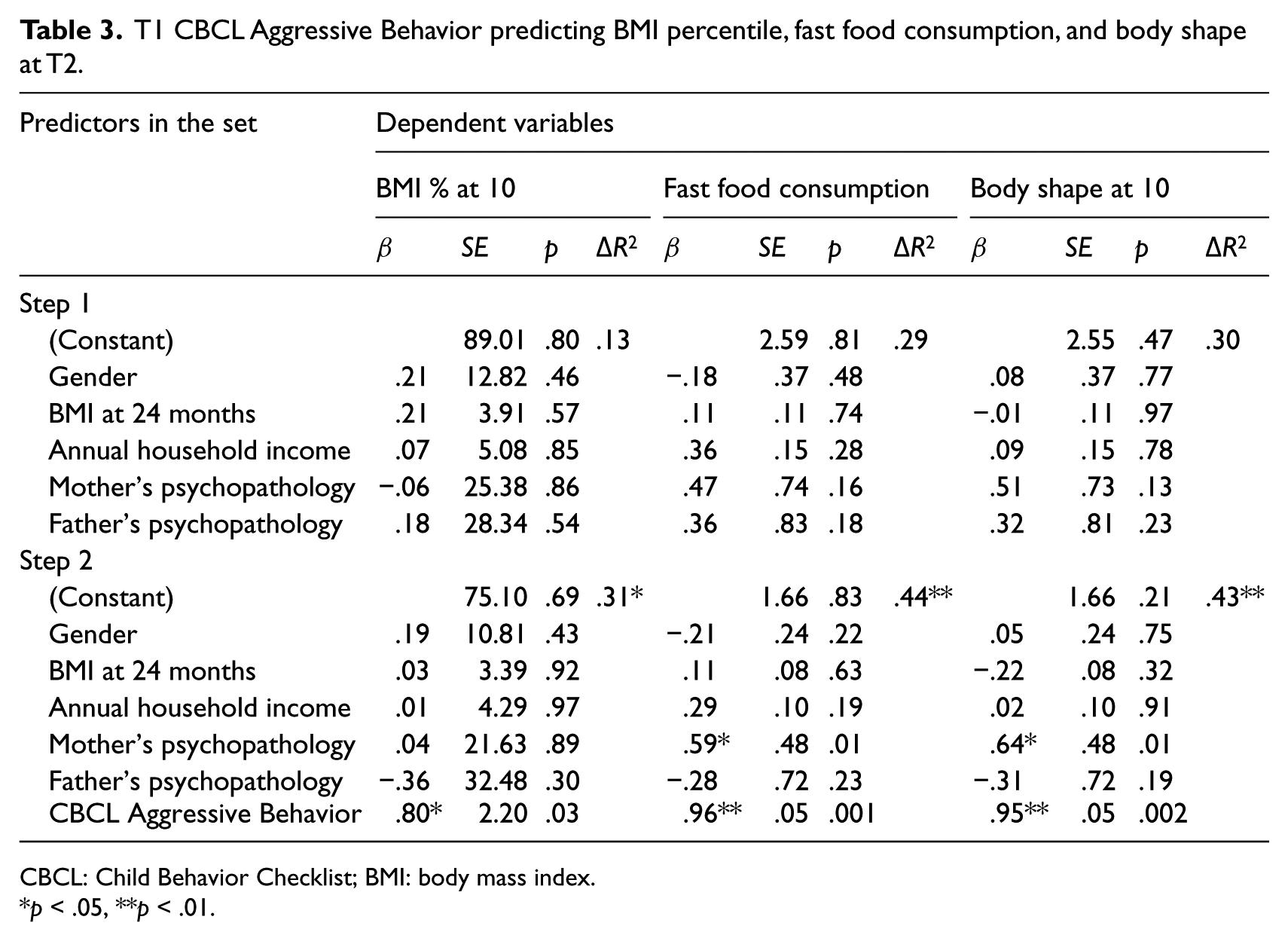
CBCL: Child Behavior Checklist; BMI: body mass index.
p < .05, **p < .01.
After controlling for gender, child’s BMI at 24 months, annual household income, and parents’ psychopathology, TBAQ Anger also significantly predicted child’s BMI percentile at age 10, β = .49, p = .03, ΔR2 = .19, and f2 = .27 (see Table 4).
T1 TBAQ Anger predicting BMI percentile at T2.
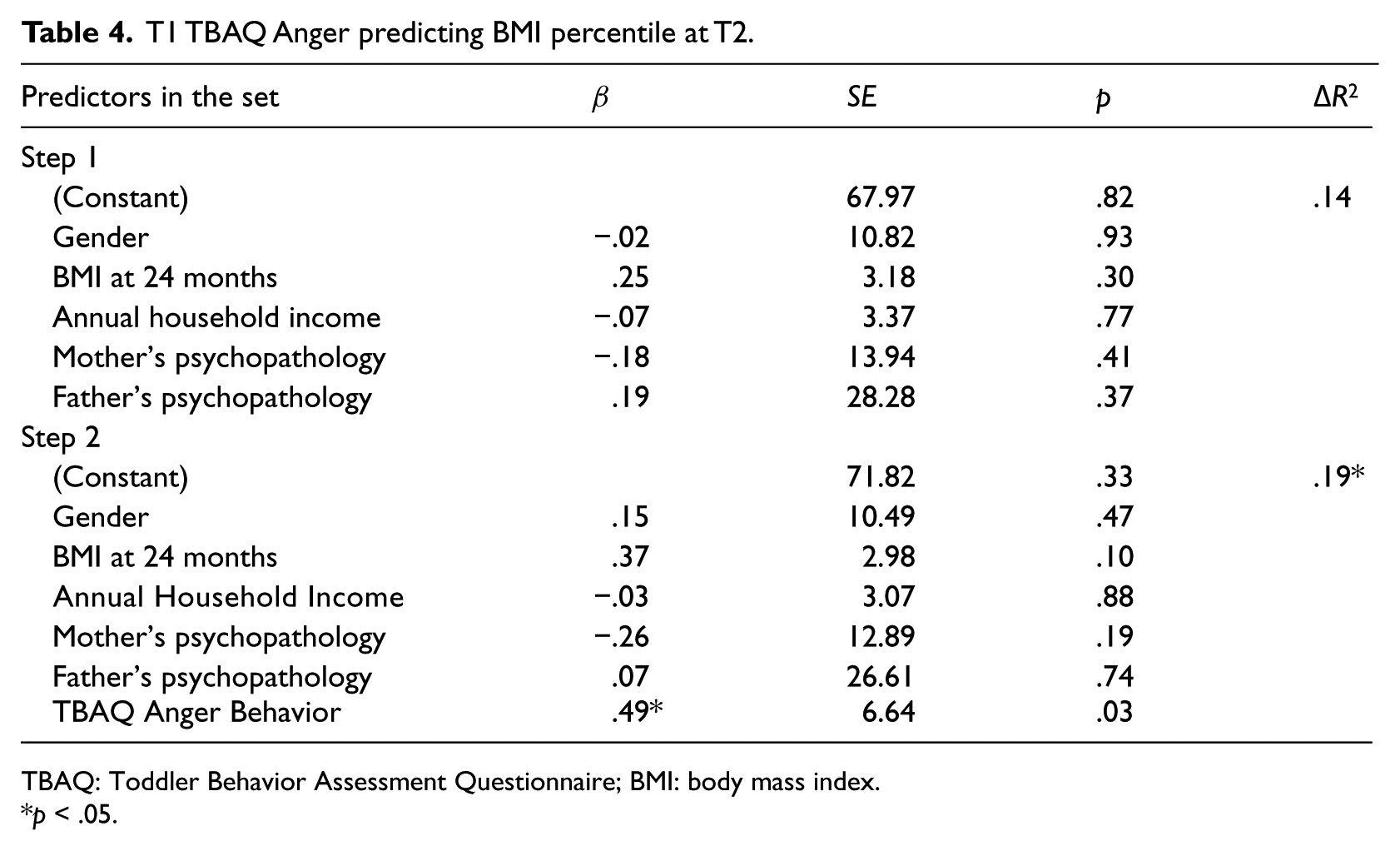
TBAQ: Toddler Behavior Assessment Questionnaire; BMI: body mass index.
p < .05.
Exploratory mediational analyses
A series of mediational analyses were conducted in which early childhood CBCL Externalizing Behavior score was the independent variable and late childhood BMI, BMI percentile, or body shape/size was the dependent variable. In these analyses, none of the putative mediational variables examined in this study (i.e. physical activity, fast food consumption, or “screen time”) were found to significantly mediate the relationship between early childhood CBCL Externalizing Behavior scores and late childhood body size.
A similar series of mediational analyses were conducted using CBCL Aggressive Behavior scores as the independent variable; results again failed to identify physical activity, fast food consumption, or “screen time” as significant mediators of early childhood CBCL Aggressive Behaviors and late childhood increased BMI.
Finally, mediational analyses were conducted using TBAQ Anger scores as the independent variable, and again our putative mediational variables were not found to be significant mediators of the early childhood TBAQ Anger and late childhood increased BMI relationship.
Discussion
The current study examined psychosocial predictors of BMI in late childhood using a prospective design and a community sample. Our analyses revealed significant, positive correlations between externalizing problems at age 2 and BMI percentile and child body shape/size at age 10. Furthermore, hierarchical regression analyses indicated that after controlling for child gender, child BMI at age 2, household income, and parents’ psychopathology, externalizing behaviors at age 2 predicted increased body mass at age 10.
To our knowledge, the only previous study that demonstrated a prospective link between behavior problems during early childhood and overweight or obesity in late childhood did not control for baseline BMI (Anderson et al., 2010). Furthermore, to our knowledge, we were the first researchers to conduct a series of exploratory mediational analyses evaluating a theoretical model of how early childhood problems may lead to elevated BMI in late childhood. Our analyses failed to identify physical inactivity, fast food consumption, or “screen time” as significant mediators. This may be because these variables are truly not mediators of early childhood externalizing problems and late childhood overweight or because our power was limited.
Future researchers should also assess other potential mediators. For instance, as our theoretical model suggests, social isolation/lack of social support is a strong mediational candidate. Children with behavior problems often have fewer social ties than their peers who do not display externalizing behaviors (Dodge, 1983), and this may subsequently lead externalizing children to increase time spent in socially isolative activities (e.g. television watching). Moreover, low levels of social interaction have been shown to be associated with increased rates of overweight and obesity (Falkner et al., 2001). Another possible mediator is weakened inhibitory control and/or executive functioning problems (e.g. Batterink et al., 2010; Verbecken et al., 2009). Perhaps children with poor inhibition are likely to engage in a number of appetitive behaviors including overeating, alcohol and/or tobacco use, and so on (Nigg et al., 2006). It is also possible that children who are unable to regulate their emotions appropriately both act out behaviorally and engage in unhealthy/uncontrolled food consumption in an attempt to cope with distressing situations. Finally, given that negative affect is related to overweight and the use of unhealthy weight control strategies in adolescents (Vander Wal, 2012), and that adolescents with high rates of externalizing problems endorse elevated rates of depressive symptoms (Little and Garber, 2005), future researchers should examine whether depressive symptoms may mediate the link between early life externalizing behaviors and subsequent elevated BMI.
We also assessed whether certain broader psychosocial variables predicted high BMI and/or large body shape at age 10. When using CBCL Aggressive Behavior scores as a predictor variable, history of an Axis I disorder in the child’s mother also predicted the child’s large body shape/size at age 10. In contrast to the results of other studies (Grow et al., 2010), we did not find a link between annual household income and obesity-relevant variables.
Our results should be interpreted in light of our study’s strengths and limitations. One noteworthy limitation is our small sample size; therefore, our power was restricted. Despite this, we uncovered significant, prospective links between early childhood externalizing problems and increased body size and unhealthy eating habits in late childhood of medium-to-large effect sizes. In relation to this, our response rate was not high; however, analyses indicated that those who participated in the T2 assessment did not differ in meaningful ways from those who did not participate. Another limitation is that weight was not objectively measured, and although studies have demonstrated that people can accurately report their height and weight (Cash et al., 1989; Shapiro and Anderson, 2003), we are not aware of research indicating how accurately mothers report the weights of their children. Additionally, for practical purposes, we obtained most parent-report information from mothers only. Future studies could improve upon the current design by also including father reports.
In sum, our study demonstrated that among a community sample of boys and girls, externalizing behaviors, aggressive behaviors, and anger at age 2 predicted a relatively high BMI at age 10. Future researchers should explore the mechanisms that may account for the link between early life externalizing problems and late childhood increased body mass.
Footnotes
Funding
This work was supported, in part, by NIMH grant R01 MH 56604 to Peter M. Lewinsohn.