
Abstract
Individuals with bleeding disorders are at increased risk of variant Creutzfeldt-Jakob disease. This study explored social cognitive predictors of screening intentions. Ninety men and women with bleeding disorders, recruited through the Haemophilia Society, completed an extended Theory of Planned Behaviour questionnaire to predict intention to screen for variant Creutzfeldt-Jakob disease. Extended Theory of Planned Behaviour variables accounted for 57 per cent of the variance in intention. Self-efficacy and anticipated affect predicted intention directly, while attitudes were mediated by anticipated affect. Simple interventions that already exist address relevant predictive components of intention to screen for variant Creutzfeldt-Jakob disease and could be used to aid decision-making.
Introduction
People affected by haemophilia and other bleeding disorders rely on treatment with clotting factor. Modern treatments include recombinant and plasma-derived concentrates and have a good safety record. However, until 1996, clotting factor treatments were derived from blood products and relying on these created a number of risks. For example, 4670 people with haemophilia were infected with Hepatitis C, and 1200 were infected with HIV prior to 1985 in the United Kingdom (Archer et al., 2009). Although steps have been taken to keep the blood supply safe, the contamination of blood products with infections that can neither be screened for nor treated remains a significant public health concern. Creutzfeldt-Jakob disease (CJD) is one infection that falls under this category.
CJD is transmissible but currently can neither be detected nor treated. CJD is a prion disease, which affects several species such as sheep (scrapie) and cows (bovine spongiform encephalopathy (BSE)). Prions are proteins found in cells, and prion diseases such as CJD, while rare, are fatal, causing the progressive destruction of the central nervous system (Duval, 1997). In the 1980s, there was an outbreak of BSE in the United Kingdom, where 3 million infected cattle entered the food chain (Ironside, 2009). Subsequently, a new form of CJD developed in humans, variant Creutzfeldt-Jakob disease (vCJD). Although it was largely due to the consumption of BSE-infected meat, blood transfusions from infected donors were also suspected leading to a concern that vCJD could potentially be transmitted via contaminated blood products (Ironside, 2009). Animal studies of CJD transmission (Ricketts et al., 1997) and clinical cases of human vCJD have confirmed the infection of individuals from blood products from individuals who were asymptomatic at the time of donation (Ironside, 2009; Llewelyn et al., 2004).
Several hundred individuals with haemophilia in the United Kingdom have been exposed to infected blood products and are currently being monitored for symptom development. People who had been treated with plasma-derived factor clotting treatment from 1980 to 2001 have been designated by the Department of Health as being at Public Health Risk for vCJD, and all those affected have been informed in writing of the theoretical risk by the Health Protection Agency (HPA).
Uncertainty can have a dramatic psychological impact, including a failure to exhibit self-protecting beliefs (Cioffi, 1991). As the risk of vCJD transmission via blood products becomes more apparent, introducing a pre-symptomatic test has been under discussion. At the time of writing, a test to detect the presence of prions for vCJD has been developed but not yet introduced (Simon Mead, personal communication). It is therefore possible only to speculate about the possible psychological effects that testing for vCJD may cause. However, comparisons with screening for other diseases may be informative. Research into the psychological effects of genetic testing shows that people often choose not to be tested because they are afraid they will lose hope, may lose their insurance, are fearful of symptoms or because there is no effective treatment or cure (Meiser and Dunn, 2000). Predictive testing for Huntington’s disease has revealed several possible harmful outcomes (e.g. depression, anxiety, stigmatisation), although pretest counselling can reduce these effects (Duncan et al., 2005). Negative psychological effects are most common in the first 2 months following testing, falling to normative levels after a year (Evers-Kiebooms and Decruyenaere, 1998), and there may be more benefits from testing than harm (Lawson et al., 1996), thought to stem from the removal of uncertainty. Both carriers and non-carriers have shown decreased distress after testing, although levels of distress fall more rapidly for non-carriers (Broadstock et al., 2000).
The Theory of Planned Behaviour (TPB; Ajzen, 1991) is a rational social cognition model of how human action is guided. In its original formulation, the TPB proposed that the likelihood of engaging in a behaviour depends on the strength of an individual’s intention. Furthermore, intentions are formed on the basis of three constructs: attitudes, subjective norms and perceived behavioural control (Ajzen, 1986). Attitudes refer to beliefs about the consequences of a behaviour and judgements about whether these are positive or negative. Subjective norms refer to an individual’s perception of the attitudes of people who are important to that individual as well as that individual’s motivation to comply with those attitudes (important others could refer to family and friends or relevant experts/professionals).Perceived behavioural control refers to one’s confidence in one’s ability to elicit a behaviour (self-efficacy) coupled with a perception that there will be opportunities to engage in that behaviour (‘perceived control over behaviour’ (PCB); Armitage and Conner, 1999). Positive attitudes towards a behaviour, positive subjective norms and a high perceived behavioural control over a behaviour are proposed to lead to the formation of a strong intention to perform a behaviour. The TPB has been widely applied to health behaviours and is a good predictor of intention and subsequent behaviour (for a meta-analysis, see Armitage and Conner, 2001). Perhaps more importantly for the present study, the TPB has also been found to predict intention and attendance in relation to screening including screening for HIV (Kakoko et al., 2006) and hereditary diseases (Nordin et al., 2004). A recent meta-analysis of 33 studies showed that intention was moderately predictive of attendance at screening, while intention was itself predicted strongly by attitudes and moderately by subjective norms and perceived behavioural control (Cooke and French, 2008).
Recent formulations of the TPB have extended the model and found that additional constructs such as anticipated affect make significant additional contributions over the standard TPB variables (Rivis et al., 2009; Sandberg and Conner, 2008). Anticipated affect refers to the expectation of feeling good or bad after a specific behaviour is performed (in contrast to attitudes that are current thoughts about a behaviour). The present study examined the role of an extended TPB in predicting intention to screen for vCJD in individuals with haemophilia and other bleeding disorders in order to identify potential points of intervention.
Methods
Participants
Questionnaires were sent by post to a random sample of 471 members of the UK Haemophilia Society who have haemophilia or other less common bleeding disorders (e.g. von Willebrand disorder, factor deficiency and platelet disorder). Ninety participants responded (81 men, 7 women, 2 not known). Mean age was 50.4 years (standard deviation (SD) = 11.6 years, range = 21–83 years); 48 participants were married, 28 were single, 7 were divorced, 4 were cohabiting and 1 was widowed (2 not known); 46 participants were employed, 25 were retired, 17 were unemployed and 1 was a student (2 not known). Following a previous written invitation from the HPA, 47 (55%) participants had chosen to find out whether they had been exposed to blood products infected with vCJD, while 38 (45%) had chosen not to find out.
Measures
The TPB questionnaire was constructed based on published guidelines (Francis et al., 2004). Attitudes were assessed by 5 bidirectional items on a 7-point Likert scale using the stem ‘Being tested for vCJD would be …’. Items were anchored at either end by the pairs of evaluative adjectives harmful–beneficial, good–bad, helpful–unhelpful, reassuring–distressing and foolish–wise. Items were re-coded so that high scores indicated a more positive attitude, and items were averaged to give an overall mean.
Subjective Norms were assessed using the same items as for attitudes described above, also rated on a 7-point Likert scale, but scored separately for the perceived attitudes of family/friends and doctors. The stems were ‘My friends and family would think that being tested for vCJD is …’ and ‘My doctor would think that being tested for vCJD is …’. These items were not counterbalanced, and the definition of ‘doctor’ was not specified since people with bleeding disorders refer to a specialist consultant rather than, for example, a GP, for all issues to do with their condition (although the consultant could refer to doctor or nurse). Items were re-coded so that high scores indicated a more positive attitude of the named others, and items were then averaged to give an overall mean.
Self-efficacy was assessed with the items ‘If there were a test available, I am confident that I could ask to be tested’ and ‘If there were a test available it would be easy for me to ask my consultant to refer me for a test’. Items were rated on a 7-point Likert scale anchored at either end with strongly disagree–strongly agree. Scores for each item were averaged so that higher scores indicated greater self-efficacy.
PCB was assessed with the items ‘If there were a test available the decision whether to be tested or not would be within my control’ and ‘If there were a test available, whether I am tested for vCJD or not is entirely up to me’. Items were rated on a 7-point Likert scale anchored at either end with strongly disagree–strongly agree. However, combining these two items gave a low internal reliability (α = .28), and so they were retained as separate items (Control 1 and Control 2, respectively).
Anticipated Affect was assessed with two items: ‘It would be a relief to know my vCJD status, one way or the other’ and ‘If I chose not to be tested I might regret the decision in the future’. Items were rated on a 7-point Likert scale anchored at either end with strongly disagree–strongly agree and were averaged so that higher scores indicated greater Anticipated Regret.
Intention was assessed using the single item ‘If a test for vCJD were available I would intend to go for a test’. This item was rated on a 7-point Likert scale anchored at either end with strongly disagree–strongly agree, and higher scores indicated greater Intention.
Internal reliabilities were high for all scales (see Table 1) although, as described above, the two PCB items did not form a reliable scale and so were retained but as separate scores rather than combined.
Mean scores for TPB items.
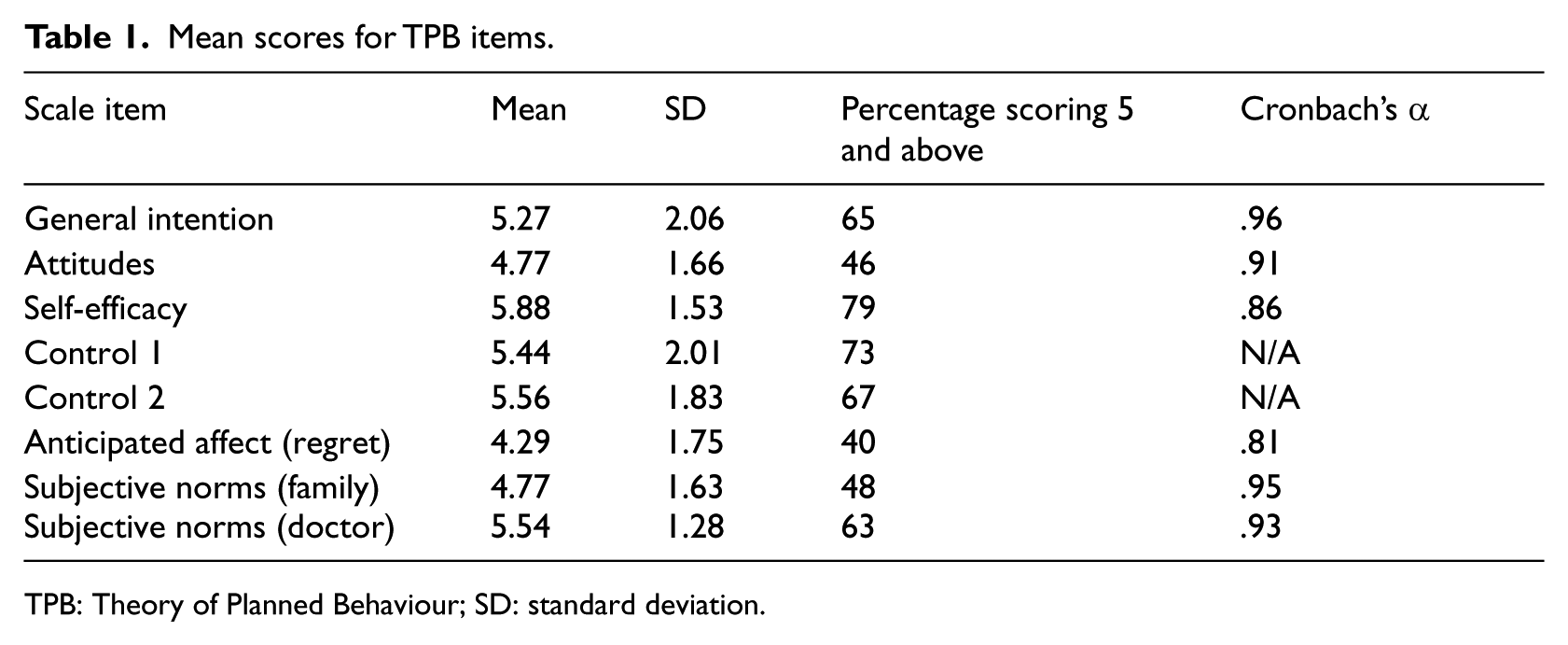
TPB: Theory of Planned Behaviour; SD: standard deviation.
Procedure
Ethical approval was obtained from the relevant university authorities. All questionnaires (along with cover information sheets, sources of further help and information and pre-paid envelopes for the return of questionnaires) were sent from, and returned to, the Haemophilia Society headquarters in London. Once returned, Haemophilia Society staff separated consent forms from completed questionnaires in order to preserve participant anonymity.
Although participants were asked whether they had chosen to find out whether they had been exposed to an implicated batch, on the advice of the Haemophilia Society, it was decided not to ask whether they had actually been exposed since this may provoke unwarranted stress and anxiety. Similarly, precise diagnoses were also not asked.
Statistical methods
Data were analysed using SPSS 19.0. Associations between TPB variables were examined using Pearson’s correlation. Predictors of intention according to the TPB and extended TPB were evaluated using hierarchical linear regression using only variables that were identified to correlate with intention in univariate analysis. In an initial regression model Intention was regressed onto standard TPB variables. A second model was then run including Anticipated Affect. Model improvement was evaluated by examining the change in F-statistic and subsequent change in explained variance.
Results
Table 1 shows the descriptive statistics for the TPB items. Intention to be screened for vCJD was high, as indicated by the proportion scoring 5 or above on the 7-point intention scale (65%), as were perceptions of Self-efficacy and Control.Participants rated Subjective Norm in relation to friends and family as less positive than Subjective Norm in relation to doctors.
Intercorrelations between TPB variables are shown in Table 2. Intention significantly correlated with Attitudes, Subjective Norms, Self-efficacy and Anticipated Affect (effect sizes between .22 and .65), yet failed to correlate with Control variables. Furthermore, Control variables failed to correlate with Attitudes, Subjective Norms, Self-efficacy and Anticipated Affect. None of the socio-demographic factors measured were significantly related with Intention or other TPB variables.
Intercorrelations between TPB variables.
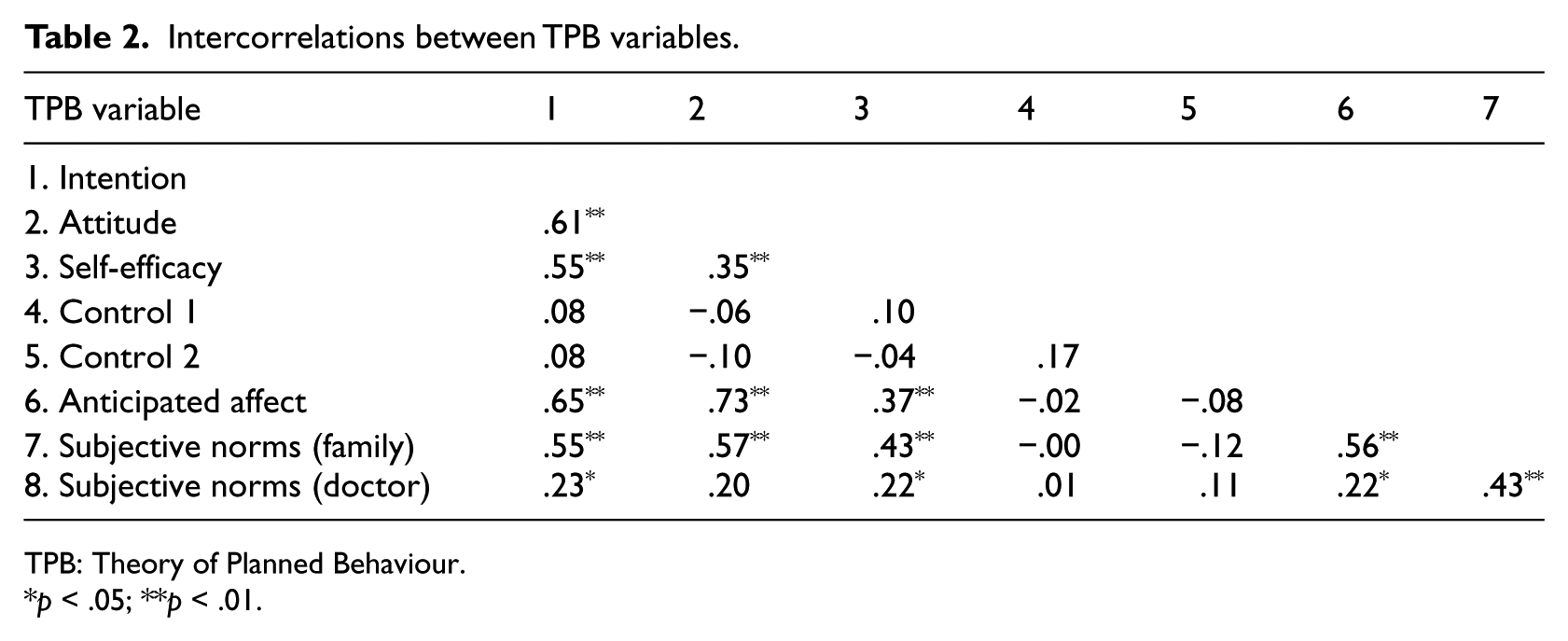
TPB: Theory of Planned Behaviour.
p < .05; **p < .01.
Regression analysis
Factors that were significantly associated with Intention in univariate analysis were examined further in a hierarchical regression. However, given the high intercorrelations between variables, multi-collinearity is a potential problem. Therefore, prior to regression analysis, all relevant variables were centred resulting in satisfactory collinearity diagnostics (variance inflation factors (VIF) < 2.32, tolerances > .43, condition indices < 3.15).
In the first model, Intention was regressed onto Attitude, Self-efficacy and Subjective Norms. This model accounted for 52 per cent of the variance in intention, with Attitudes and Self-efficacy significantly predicting Intention (see Table 3, model 1). Subjective Norms failed to predict Intention.
Hierarchical regression analysis testing an extended TPB model.
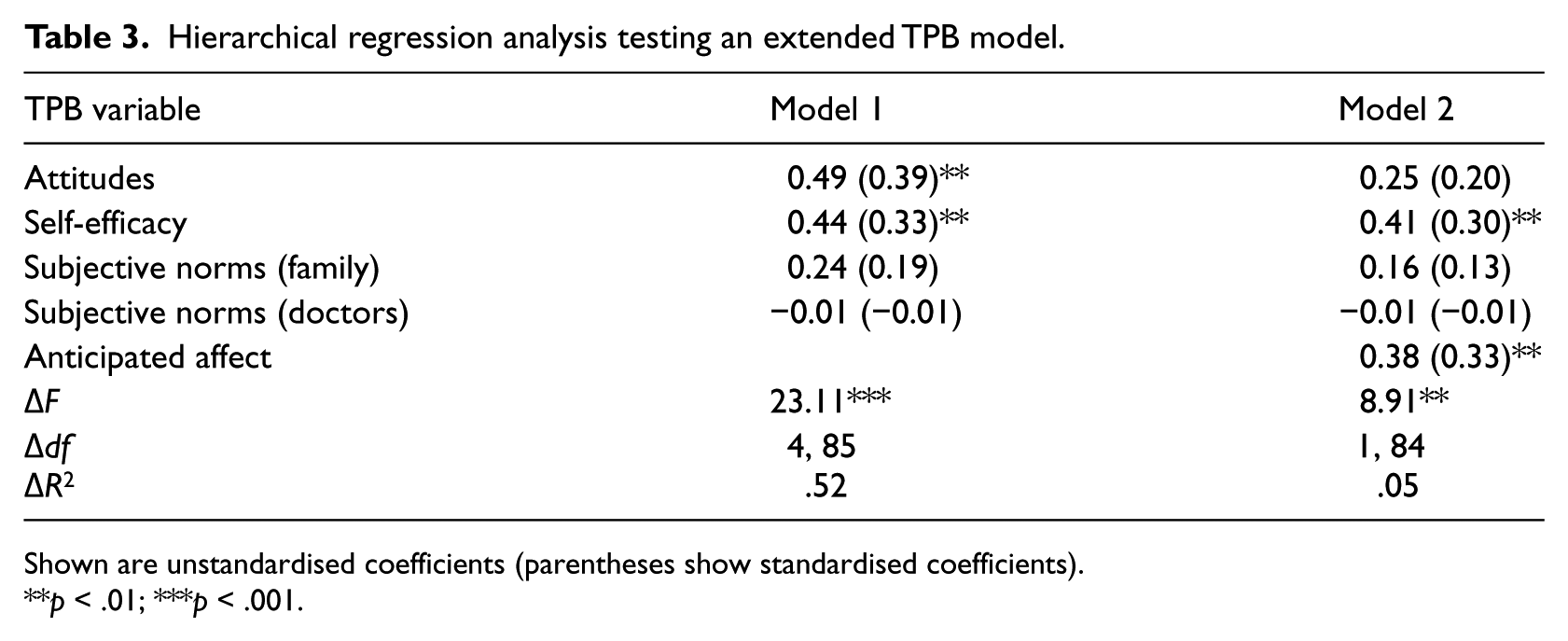
Shown are unstandardised coefficients (parentheses show standardised coefficients).
p < .01; ***p < .001.
Anticipated Affect was entered into a second model that included Attitude, Self-efficacy and Subjective Norms (see Table 3, model 2). Model 2 was a significant improvement over the initial model (ΔF = 8.91, df = 1, 84, p = .004) explaining a total of 57 per cent of the variance in Intention. Self-efficacy and Anticipated Affect significantly predicted intention (Table 3). A 1-point increase in Self-efficacy (i.e. increasing efficacy) was associated with a .41-point increase in Intention, while a 1-point increase in Anticipated Affect (i.e. increasing regret) was associated with a .38-point increase in Intention. Attitudes no longer predicted Intention (β = .25, p = .07, model 2) suggesting that Anticipated Affect mediates the association between Attitude and Intention observed in model 1.
Discussion
The current study explored social cognitive factors using an extended TPB that predicted intention to attend screening for a hypothetical test for vCJD in individuals with haemophilia and other bleeding disorders. Given that the prevalence of vCJD is unknown, yet is potentially greater in these groups than in the general population, it is important to understand the psychological factors that might predict the uptake of vCJD testing.
Findings
Overall, the sample had high levels of intention to screen for vCJD if a test were available and reported high levels of self-efficacy. Attitudes and normative beliefs were less positive and only one-third of participants felt they would regret not taking the test.
In predicting intention to screen for vCJD, the standard TPB accounted for 52 per cent of the variance with attitudes and self-efficacy being independently predictive. However, the inclusion of anticipated affect in the model accounted for a significant amount of additional variance (5%) over and above the standard TPB. Furthermore, while self-efficacy was still predictive in this extended model, attitude was no longer uniquely predictive of intention, and its effect was mediated by anticipated affect. This extended TPB accounted for a total of 57 per cent of the variance in intention to screen for vCJD.
Strengths and limitations
Despite the novelty of this study, there are some limitations to consider. Ethical considerations meant that HIV and Hepatitis status were not asked about and exposure to prior blood contamination may have had an effect on cognitions concerning testing for vCJD. Similarly, the exact nature of participants’ conditions may have influenced results, for example, those with severe haemophilia may have differing views from those with less severe forms. In comparison to the World Federation of Hemophilia’s (2011) report on the Annual Global Survey 2010, the sample in the present study was slightly over-represented with men (90% vs 80% worldwide). The sample was also older than would normally be expected, with 73 per cent above the age of 45 years, compared to the United Kingdom as a whole with 46 per cent above the age of 45 years. However, this may be due to the issue under consideration since the increased risk of vCJD is more strongly linked to older treatments that were derived from blood products.
The study was also cross-sectional and was unable to measure actual behaviour. However, while a full test of the TPB requires the prediction of actual behaviour, no reliable test for vCJD is currently available, and so it was not possible to test the prediction of attending for testing. Nevertheless, at the time of writing, the validation of such a test is imminent and so such a study could be carried out in the future to examine intentions and uptake of screening as well as evaluate various TPB-based interventions. It should also be noted that the high explained variance in intention is likely to be attenuated when an actual test is available.
Nevertheless, and in spite of the relatively small sample size, the study recruited participants from a wide range of ages, employment statuses and relationship statuses, suggesting that results are based on a wide population sample and so may be generalisable to the wider community of people with bleeding disorders. However, we make no claim for the generalisability of these results to the general population without bleeding disorders.
Implications
Notwithstanding the limitations, the results have a number of theoretical and practical implications. The results broadly support the TPB (Ajzen, 1991) with attitudes and self-efficacy (but not subjective norm or perceptions of control over behaviour) predicting intention. However, the inclusion of anticipated affect rendered the effect of attitudes non-significant (though only marginally so), suggesting the effect of attitude on intention is mediated through the anticipation of regret.
Other variables have been considered as improving the ability of the TPB to predict intention including differentiating between cognitive and affective attitudes (Payne et al., 2004), delineating other normative influences such as moral norms (Rivis et al., 2009), descriptive norms (what important others do, not just what they say) and media norms (Conner et al., 1996) as well as other social influences such as self-identity (Armitage and Conner, 1999). Although the final model in the present study accounts for 57 per cent of the variance in intention, the inclusion of these other variables might add significant additional variance.
Although participants were asked whether they had chosen to find out about their risk status, it was felt that it would be inappropriate in a postal questionnaire study actually to ask what that status was. It is possible that this knowledge may influence people’s intention to seek testing (Rosenstock, 1966). Indeed, when perceptions of threat are added to TPB variables, they can account for a significant additional amount of variance (e.g. Norman et al., 1999).
There are also practical implications for clinicians helping people decide whether to go for screening or not. On the basis of significant associations with intention, information can be provided to address salient attitudes, subjective norms and perceptions of control (Sutton, 2010). In addition (again, on the basis of a significant correlation between intention and subjective norm), family or friends should be included at all stages of decision-making and consultation. Outcome simulation (imagining the consequences of a behaviour) influences anticipated regret (Richard et al., 1996), while process simulation (imagining the act of going for testing including planning and overcoming obstacles) increases self-efficacy (Armitage and Reidy, 2008). Given the importance of anticipated affect and self-efficacy in particular in the regression analysis, these interventions could help people with bleeding disorders to firm up their intention to attend screening.
However, other research has identified that even when intentions to perform a behaviour have been formed, the translation of these into actual behaviour is more likely if people form what are called, ‘implementation intentions’ (Gollwitzer, 1999), situational cues that would trigger the behaviour. Individuals asked to write down when, where and how a particular behaviour would be performed are significantly more likely to translate their goal intentions into actual behaviour (Gollwitzer and Sheeran, 2006), including attending for screening (Sheeran and Orbell, 2000). The most effective intervention, therefore, may be one where the intention to screen for vCJD is formed by addressing beliefs and anticipated outcomes followed by asking people to determine precisely when, where and how they would act on that intention.
However, one further practical consideration is the role of pretest counselling. This is compulsory prior to testing for HIV or Huntington’s disease (Marteau and Croyle, 1998). Pretest counselling not only ensures that individuals are fully informed and mentally prepared for a negative outcome but also helps detect those who are at high risk of adverse outcomes (Marteau and Croyle, 1998).
Conclusion
This study identified social cognitive variables (anticipated regret and self-efficacy) that predicted intention to screen for vCJD. While highly predictive, it is important to remember that a reliable test is not yet available. Even when it is, however, it may be some time before infected individuals can benefit from treatment. It would be beneficial to replicate this study once a test has actually been introduced and to determine what effect knowing the result of such a test would have on adjustment and quality of life.
Footnotes
Acknowledgements
We wish to thank all the people with haemophilia and other clotting disorders who took part in this study and the Haemophilia Society for their support.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.