
Abstract
The link between burnout and depression remains unclear. In this study, we compared depressive symptoms in 46 burned-out workers, 46 outpatients experiencing a major depressive episode, and 453 burnout-free workers to test the distinctiveness of burnout as a clinical entity. Participants with burnout and major depressive episode reported similar, severe levels of overall depressive symptoms. The between-syndrome overlap was further verified for eight of the nine major depressive episode diagnostic criteria of the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.). Our findings do not support the view hypothesizing that burnout and depression are separate entities and question the nosological added value of the burnout construct.
Burnout is usually defined as the combination of three clusters of symptoms, namely, emotional exhaustion, depersonalization, and reduced personal accomplishment (Maslach et al., 2001). Etiologically, burnout is seen as the end product of a work-related chronic stress process (Schaufeli and Enzmann, 1998), signaling the failure of a time of active coping and sustained resource expenditure, and marking the beginning of an era of passive coping and withdrawal associated with resource depletion. The severity of the collapse afflicting workers with burnout has frequently been emphasized, for instance, when it has been noted that “first and foremost, burnt-out individuals feel helpless, hopeless, and powerless” (Schaufeli and Buunk, 2002, p. 399). Initially observed in helping professions and human services (Freudenberger, 1974; Maslach, 1976), burnout has been described in various occupational areas (e.g. Carson et al., 2010; Chiron et al., 2010), and thousands of publications have been dedicated to it since the introduction of the construct in the 1970s (Schaufeli et al., 2009). Despite considerable empirical research, burnout’s nosological status is still controversial (Weber and Jaekel-Reinhard, 2000), and burnout is not recognized as a distinct condition in diagnostic classification systems such as the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR) (American Psychiatric Association, 2000). One key question in this matter deals with the overlap of burnout and depression.
Although it is accepted that burnout shares features with depression, there is a growing consensus that burnout is irreducible to a mere depression subtype and presents a specific clinical picture (Glass and McKnight, 1996; Iacovides et al., 2003; see also Thomas, 2004). However, most studies supporting this view suffered from inadequate sampling, confusing burnout with mild or moderate job stress (for discussions of this issue: Cox et al., 2005; Schaufeli and Enzmann, 1998). Thus, in a recent study (Ahola et al., 2005) reporting that about 53 percent of the individuals with severe burnout presented a depressive disorder the cutoff delineating severe burnout (3.5/6.0 on the Maslach Burnout Inventory (MBI)–General Survey) was lower than generally recommended (Maslach et al., 1996; Schaufeli and Enzmann, 1998), implying a high risk of false-positive inclusion. To date, such limitations preclude any definite conclusion regarding the degree of overlap between burnout and depression, with depression-related characteristics remaining insufficiently investigated in the subgroups of individuals experiencing severe or clinical (i.e. actual) burnout.
The aim of our study was to examine whether burnout was distinguishable from depression at a symptom level, a level of analysis that is of prime importance for medical practice (e.g. for diagnosis and treatment purposes). We used strict cutoffs for identifying individuals with burnout so that selection biases could be limited. The choice of a categorical approach to burnout and depression was made for its clinical relevance (Cox et al., 2005).
Method
Depressive symptoms were compared in a group of burned-out workers (BOG), a group of depressed outpatients (DEP), and a control group of burnout-free workers (CTR). Between-group comparisons were carried out in reference to the major depressive episode (MDE) diagnostic criteria of the DSM-IV-TR (American Psychiatric Association, 2000). Two different recruitment procedures were followed.
To form the BOG and the CTR, we emailed the MBI (Dion and Tessier, 1994; Maslach and Jackson, 1986) to several hundred middle and high schools in France by using academic databases—past research has shown that Internet questionnaires are as valid and reliable as traditional, paper-and-pencil questionnaires (Gosling et al., 2004; Ritter et al., 2004). The questionnaire was returned by 1658 teachers (see Table 1 for sociodemographic and health characteristics of the full worker sample). To be assigned to the BOG, a participant had to exhibit mean scores of at least 4 on the MBI (Brenninkmeijer and van Yperen, 2003; Maslach et al., 1996) and 4.5 on the MBI emotional exhaustion subscale—special emphasis was placed on the emotional exhaustion dimension given its centrality in the burnout syndrome (Maslach et al., 2001; Schaufeli and Enzmann, 1998). A total of 46 teachers (3%) met these inclusion criteria. Their mean age was 43.20 years (standard deviation (SD) = 9.79 years, range = 25–59 years), and 63% were female. The CTR consisted of participants displaying at most 2 on the MBI and 1.5 on the MBI emotional exhaustion subscale (n = 453). Mean age in the CTR was 41.23 years (SD = 9.70 years, range = 21–64 years), with 60 percent of the sample consisting of female participants.
Means, SDs, and correlations of sociodemographic and health characteristics for the full worker sample (n = 1658). Values of Cronbach’s alpha (α) are indicated for each multiple-item questionnaire used in this study.

SD: standard deviation; BDI-II: Beck Depression Inventory-II; MBI: Maslach Burnout Inventory; EE: emotional exhaustion; D: depersonalization; RPA: reduced personal accomplishment; HD: history of depressive disorders; HA: history of anxiety disorders.
Gender was coded 0 for “female” and 1 for “male.”
HD and HA were coded 0 for “absence” and 1 for “presence.”
p < .05; **p < .01; ***p < .001.
The DEP was composed of 46 outpatients consecutively diagnosed for a DSM-IV-TR MDE (American Psychiatric Association, 2000) in a medical and psychological care unit over a period of about 2 years. MDE diagnoses were based on psychiatric interviews. Given that most patients were either on sick leave or unemployed because of their depression, they did not complete the MBI. To avoid a possible initial overlap of burnout and depression diagnoses, patients with work-related depression (i.e. patients mentioning work-related factors as primary depressogenic agents) were excluded. In the DEP, mean age was 39.02 years (SD = 11.27 years, range = 19–60 years), with 87 percent of participants being female.
The Beck Depression Inventory-II (BDI-II; Beck et al., 1998) was used for assessing depressive symptoms. The BDI-II has demonstrated strong psychometric properties and is one of the most widely used instruments for the measurement of depressive symptoms in both patient and nonpatient populations (e.g. Chilcot et al., 2011; Sing and Wong, 2011; Tully et al., 2011; for an overview, see Nezu et al., 2009). Patients completed the BDI-II during a regular psychotherapy session in the first 2 weeks following their diagnosis, whereas workers received and filled in the BDI-II together with the MBI. To obtain a score for each of the nine MDE diagnostic criteria of the DSM-IV-TR in addition to the total depression score normally provided by the BDI-II, 16 of the BDI-II items were extracted and either considered individually or combined when appropriate (combination modalities are presented in Table 2).
Self-reported depressive symptoms as a function of the group, control (n = 453) versus burnout (n = 46) versus depression (n = 46).
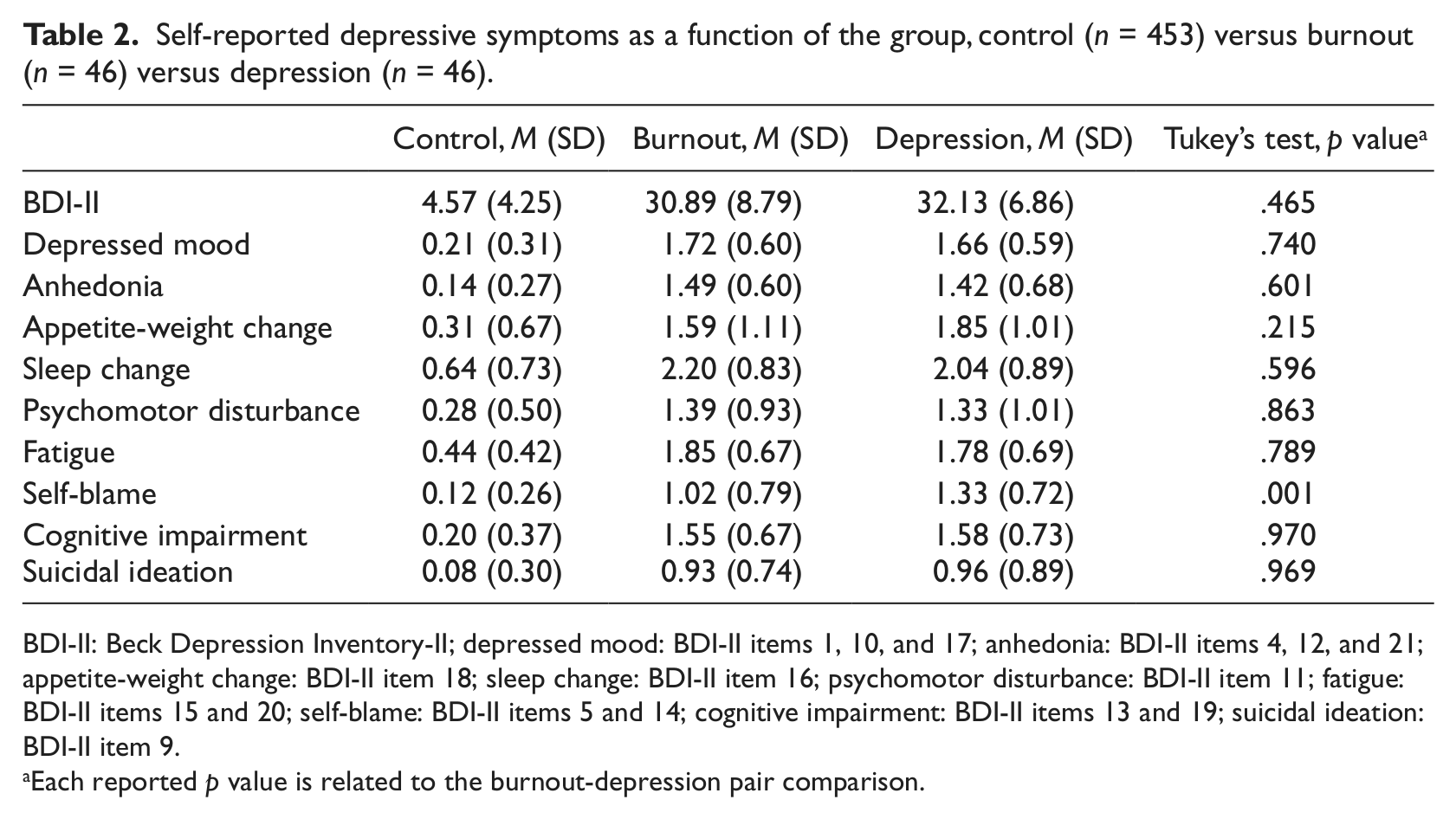
BDI-II: Beck Depression Inventory-II; depressed mood: BDI-II items 1, 10, and 17; anhedonia: BDI-II items 4, 12, and 21; appetite-weight change: BDI-II item 18; sleep change: BDI-II item 16; psychomotor disturbance: BDI-II item 11; fatigue: BDI-II items 15 and 20; self-blame: BDI-II items 5 and 14; cognitive impairment: BDI-II items 13 and 19; suicidal ideation: BDI-II item 9.
Each reported p value is related to the burnout-depression pair comparison.
Statistical analyses were carried out by using Statistica software (Statsoft, Inc.; Tulsa, OK). Overall depression ratings were compared using univariate analysis of variance (ANOVA), while ratings related to MDE diagnostic criteria were examined using multivariate analysis of variance (MANOVA). Tukey’s test was run for pairwise comparisons. The significance threshold was defined by a p value of .05.
Results
In the full worker sample (n = 1658), BDI-II scores were positively correlated both to MBI scores, r = .68, p < .001, and to emotional exhaustion scores, r = .74, p < .001 (Table 1). When corrected for attenuation (Cohen et al., 2003), correlation values reached .87 for the association between BDI-II and MBI scores and .82 for the association between BDI-II and emotional exhaustion scores, ps < .001.
The three groups did not differ in age, all ps > .10, but differed in gender with the DEP containing a higher number of females than the CTR, p < .01. MBI mean scores were 4.53 (SD = 0.38) in the BOG and 1.03 (SD = 0.46) in the CTR. The BOG displayed an emotional exhaustion mean score of 5.31 (SD = 0.48) and the CTR of 0.90 (SD = 0.41).
The ANOVA revealed an effect of the group on BDI-II total score, F(2, 542) = 1095.05, p < .0001, partial η2 = 0.80. Tukey’s test showed that BDI-II total score was higher in the BOG and the DEP than in the CTR, whereas the BOG and the DEP could not be distinguished from one another (Table 2). According to BDI-II French cutoffs (Beck et al., 1998), depressive symptoms were severe in both the BOG and the DEP—with mean scores of 30.89 (SD = 8.79) and 32.13 (SD = 6.86), respectively—and no burned-out worker was free of depressive symptoms (i.e. displayed less than 12 on the BDI-II).
The MANOVA, including the nine MDE diagnostic criteria as dependent variables, revealed an effect of the group, Wilks’ λ = 0.20, F(18, 1068) = 72.89, p < .0001, and partial η2 = 0.55. For each criterion, post hoc analyses indicated that participants with burnout and depression exhibited higher BDI-II scores than controls, all ps < .0001. BDI-II scores were similar in the BOG and the DEP except for the “self-blame” criterion (results are detailed in Table 2).
Discussion
The objective of this study was to examine whether burnout could be distinguished from depression in terms of reported symptoms, a key source of information in medical practice. It turned out that burnout and MDE were associated with a similar amount of depressive symptoms both when considering overall depression ratings and when scrutinizing ratings related to eight of the nine MDE diagnostic criteria. To our knowledge, this study was the first to propose a detailed, DSM-referenced symptom comparison between burned-out workers and depressed patients.
Our findings do not support the view hypothesizing that burnout and depression are separate entities (Glass and McKnight, 1996; Iacovides et al., 2003). Rather, they suggest that burnout and depression might actually match the same pathological realm (Hallsten, 1993; Schonfeld, 1991). Indeed, by sharing eight of the nine MDE defining features, burnout reveals a prominent depressive core, remembering that a MDE diagnosis can be produced in the presence of only five of the nine MDE diagnostic criteria (American Psychiatric Association, 2000). Furthermore, the only symptom appearing as less reported in burnout than in depression—namely, “self-blame”—is not cardinal to MDE diagnosis, contrary to depressed mood and anhedonia (American Psychiatric Association, 2000). This being specified, our results regarding the “self-blame” criterion are consistent with early descriptions of burnout presenting guilt as less conspicuous in burnout than in depression (Freudenberger and Richelson, 1980). Finally, our results do not corroborate the often cited idea that burnout is a situation-specific and relatively work-confined condition (Maslach et al., 2001; Schaufeli and Enzmann, 1998). In this study, burnout was associated with symptoms denoting pervasive alterations (e.g. changes in sleeping patterns).
Two main limitations to our study should be mentioned. First, medication intake was not controlled and possibly affected symptom self-reports in an asymmetric manner. Second, gender distribution varied according to the group, and male representation was too low to allow meaningful group × gender interaction analyses.
The massive overlap of the symptoms reported by burned-out workers and depressed patients questions the added value of burnout as a potential nosological category. Relatedly, our results warn against the pitfall of generalizing findings associated with mild and moderate job stress to severe or clinical burnout, and tend to confirm that more rigorous sampling procedures are needed in burnout research (Cox et al., 2005; Schaufeli and Enzmann, 1998). Indeed, by using strict cutoffs for the assessment of burnout, we were led to conclusions differing substantially from those dominating previous research, which pointed to between-syndrome distinctions rather than similarities (e.g. Iacovides et al., 2003). Notions such as “job stress-induced depression” (Rydmark et al., 2006) emphasize work-related depressogenic factors while benefiting from the DSM framework dedicated to depressive disorders. Whether the construct of burnout complements them in any medically useful way is not self-evident (Shirom, 2005; Taris, 2006) and should be clarified.
Footnotes
Acknowledgements
The authors thank Romain Brisson and Philippe Millot for their helpful comments and suggestions.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.