
Abstract
The Perceptions of Parental Illness Questionnaire was developed based on interviews with 15 adolescents with a parent with multiple sclerosis and refined using cognitive interviews. In total, 104 adolescents with a parent with multiple sclerosis then completed the Perceptions of Parental Illness Questionnaire and adjustment measures at two time points 6 months apart. Principal component analysis resulted in 11 Perceptions of Parental Illness Questionnaire sub-scales. Mixed-effect models showed that adolescents’ perceptions of parental multiple sclerosis at baseline rather than disease severity were associated with their psychosocial well-being 6 months later. The results indicate that Perceptions of Parental Illness Questionnaire may be a reliable and valid measure of adolescents’ representations of parents’ multiple sclerosis. Further studies are needed to replicate these findings with other illness groups.
Introduction
There is increasing evidence that having a parent with a physical health problem can place children at an increased risk of developing emotional and behavioural difficulties (Romer et al., 2002). For example, children who have a parent with chronic illness (compared with children with healthy parents) have been found to experience higher levels of anxiety and depression (Harris and Zakowski, 2003), somatic complaints, social difficulties (Mikail and von Baeyer, 1990) and lower levels of self-esteem (Harris and Zakowski, 2003).
A number of factors have been associated with children’s adjustment to having a parent with a chronic illness (Bogosian et al., 2010a). One important factor relates to how children and adolescents view their parent’s illness. For instance, some research has shown that children’s appraisal of the severity of parental cancer plays a role in the development of their anxiety and depression (Compas et al., 1996) and is associated more clearly with their own adjustment than the characteristics of the parent’s disease (Grant and Compas, 1995). Furthermore, children with a parent with cancer report very little opportunity for control over their parent’s cancer, which has been argued to constrain them from seeking active, problem-oriented types of coping (Compas et al., 1996).
Despite these important findings, there is a paucity of research that explores how children perceive parental illnesses and its potential impact on development. In contrast, a large body of literature has shown links between adults’ perceptions of their own health problems and adjustment (e.g. Hagger and Orbell, 2003; Kaptein et al., 2010; Llewellyn et al., 2007). Most of this literature has made use of the Illness Perception Questionnaire (IPQ) and its derivatives (Broadbent et al., 2006; Moss-Morris et al., 2002; Weinman et al., 1996). The IPQ was based on the Common Sense Model (CSM) of illness representations, which proposes that individuals construct schematic representations of illness falling into five dimensions: identity, causal attributions, timeline, consequences and cure/control (Leventhal et al., 1980). In addition to holding these cognitive representations of their illness, people also hold emotional representations of their condition (Moss-Morris et al., 2002).
Previous research suggests that parental illness is more likely to have a negative impact on psychological well-being of older children and adolescents compared with young children (Bogosian et al., 2010; Welch et al., 1996). Given that illness perceptions have been found to moderate adjustment, this study developed the Perceptions of Parental Illness Questionnaire (PPIQ) to measure these perceptions in adolescence. To develop this questionnaire, we focused on adolescents with a parent with multiple sclerosis (MS).
MS is an unpredictable, demyelinating disease of the central nervous system (CNS) and causes either remitting or progressive physical and cognitive dysfunction (Murray, 1995). In addition to physical symptoms, people with MS are at increased risk of developing depression (Feinstein, 2004) and anxiety (Janssens et al., 2003). Causes of the illness remain unknown and there are no known cures. All these factors make MS a particularly challenging illness for families. Also, the lack of certainty surrounding MS, the unknown causes of the illness and the symptom variability make it particularly challenging with regard to understanding illness perceptions, held by people with MS and their children.
The first objective of this study was to develop items for an age-appropriate questionnaire to measure adolescents’ perceptions of their parent’s MS and establish the face validity and accessibility of the questionnaire using qualitative methods (study 1). The second objective was to examine the structural validity, internal reliability and predictive validity of the newly developed questionnaire using quantitative methods (study 2).
Study 1: Development of the questionnaire
Methods
Design
Semi-structured, face-to-face interviews with adolescents with a parent with MS were used to elicit age-appropriate items for the questionnaire. Subsequent cognitive interviews with these adolescents were used to refine questionnaire items. Ethical approval was obtained through the Ethics Committee at the University of Southampton and Research Governance (ref: 625/6196). Parents gave written informed consent for their children’s participation in the study. Adolescents were asked to sign informed assent forms.
Participants
Adolescents were recruited through adverts on MS-related websites. Additionally, local young carers’ support workers handed out information about the study to potential participants. We used purposive sampling techniques to identify adolescents with different characteristics and in a variety of circumstances. Fifteen participants 13–18 years old were recruited (eight adolescents were between 13 and 15 years old and seven adolescents were between 16 and 18 years old). Five adolescents were male and 10 female. In four cases, both siblings of the same family were interviewed. In the 11 families that took part in the study, 9 mothers and 2 fathers had MS. Four boys had a mother with MS and one boy had a father with MS. Eight girls had a mother with MS and two girls had a father with MS. We asked the parent with MS a series of questions about walking ability and use of aids as indications of illness severity. These questions were the questionnaire items 2, 4 and 6, extracted from the ‘walking distance’ sub-scale of the Expanded Disability Status Scale (EDSS; Bowen et al., 2001). Five parents had minimal ambulation difficulties and were able to walk at least 300 m without aid or rest, two parents had significant difficulties but were able to walk at least 100 m and four parents could walk a few steps or less and used wheelchairs. Parents had MS for a period between 1½ years and 27 years (two parents had MS for a period between 1 and 5 years, three parents between 6 and 10 years, four parents between 11 and 16 years and two parents for over 20 years). One parent had primary progressive type of MS, four parents had secondary progressive MS, five parents had relapsing remitting MS and one did not know his or her type of MS.
Face-to-face interviews
The interviews lastedbetween 10 and 90 minutes (median: 31 minutes). Questions were open-ended and broad. Participants were asked to talk about the impact of parental MS, their feelings towards parental MS, descriptions of MS, what makes MS symptoms better or worse, the treatments available, how their parents got MS and for how long they think MS will last. The answers to the first two questions were separately analysed and presented elsewhere(Bogosian et al., 2011).
Analysis
Verbatim transcripts of the interviews were analysed using deductive thematic analysis within the theoretical framework provided by the CSM (Leventhal et al., 1980). A coding manual was developed based on CSM dimensions and the two added dimensions from the Illness Perception Questionnaire–Revised (IPQ-R; emotional representation and illness coherence). The coding manual was used flexibly to ensure that the categories were ‘grounded’ in the data. The fit of the data was carefully checked, and the categories were redefined or discarded when they looked inapplicable or empirically ill-fitting. Earlier transcripts were re-categorized as categories were developed and refined.
Study 1: Results
Main themes
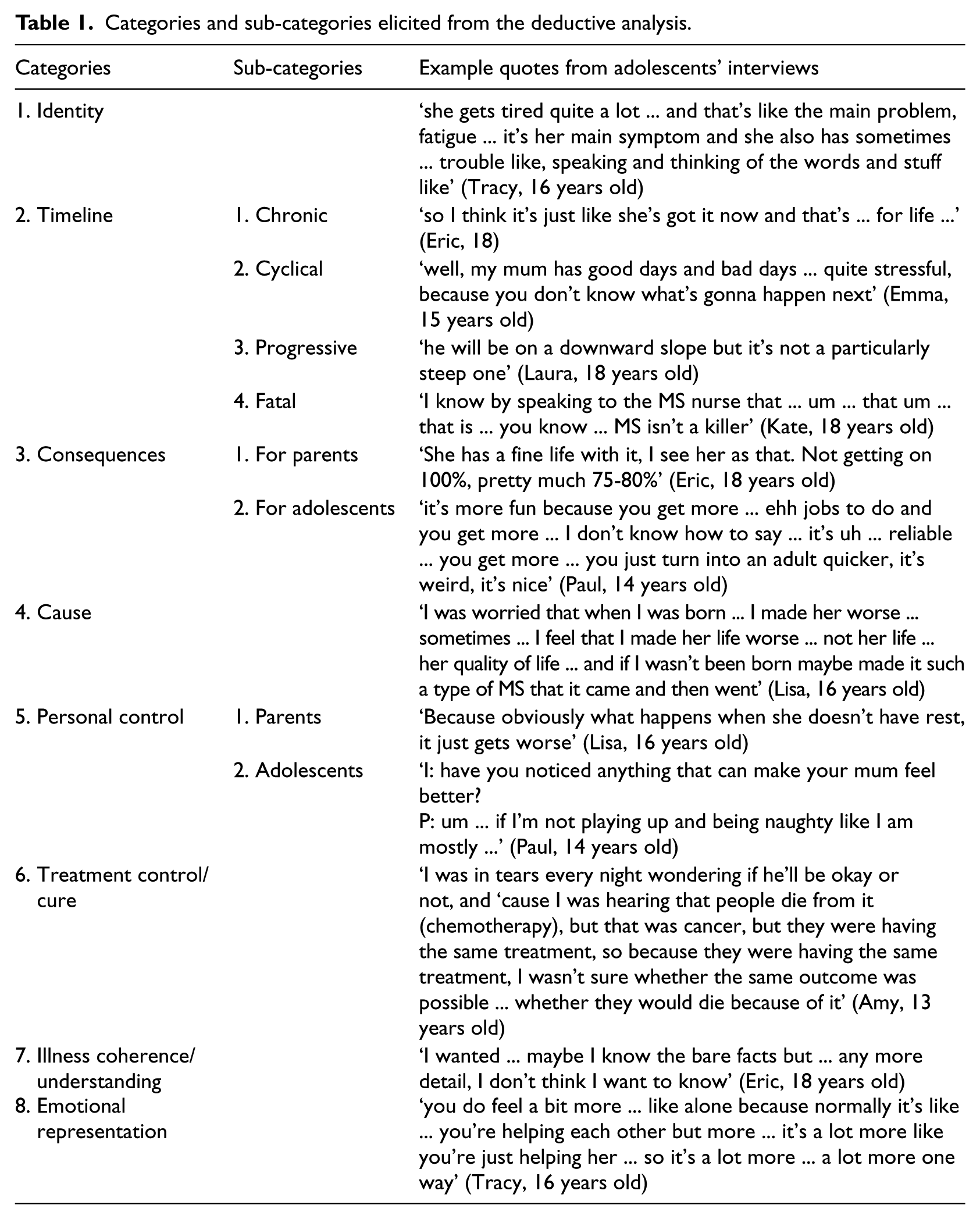
The dimensions of the CSM fitted well with the interview data. In the timeline category, two new sub-categories were identified: progressive and fatal. Furthermore, the personal control category was divided into the parent’s control over their MS and adolescents’ control over parental MS. The consequence category was divided into consequences for the parent with MS and consequences for the adolescent. Table 1 summarises the final categories and sub-categories used to construct the first version of the questionnaire along with quotes from adolescents’ interviews. Participants’ names have been replaced.
Categories and sub-categories elicited from the deductive analysis.
Generating questionnaire items
Items for the PPIQ were generated directly from quotes, which mapped onto all the categories. Special care was taken for the items to be phrased in a balanced and neutral way. Complex and lengthy questions were avoided. Two identical versions of the questionnaire were developed: one for mothers with MS and one for fathers with MS (see Appendix 1).
Refining items using cognitive interviews
Participants who took part in the qualitative interviews were invited to a second interview to help refine the questionnaire items. Due to time and budget constraints, only the first six adolescents who replied were interviewed. These included four girls and two boys between 13 and 18 years old (median = 17 years). Four adolescents had a mother with MS and two had a father with MS.
In the cognitive interviews, we used ‘think aloud techniques’ and verbal probing (DeMaio et al., 1998), where the participants were encouraged to read each item aloud and tell the researcher all the thoughts that came to their minds when hearing the item. Following this, specific probes for each questionnaire item were used. For example, when participants answered after a long time of thinking or felt unsure about the answer and changed the answer before giving the final answer, participants were probed to explore their confusion (Willis, 2004). The cognitive interviews lasted between 30 and 49 minutes (median: 37 minutes).
Cognitive interviews revealed problems with the wording of some items. These problems were addressed by changing the wording of the original items or by replacing the broad items with more specific items. The sections on parental symptoms (identity) and available treatments (treatment control/cure) were omitted as adolescents were not familiar with available treatments for MS and were confused about which symptoms can be attributed to MS and which to medical treatments.
The first draft of the questionnaire included eight proposed sub-scales (see Appendix 2): emotional representations (4 items), parents with MS control (4 items), adolescents’ control (6 items), timeline chronic (4 items), timeline cyclical (3 items), consequences for the parents (2 items), consequences for adolescents (15 items) and illness coherence/understanding (3 items).
Study 2: Questionnaire validation
Methods
Design
The PPIQ was completed by 104 adolescents of parents with MS, and a detailed psychometric analysis was followed. The associations between PPIQ variables and adjustment variables were assessed longitudinally. A longitudinal design allows for a more accurate picture of how changes in adolescents’ illness beliefs can effect changes in their adjustment. Ethical approval was obtained through the National Research Ethics Service, Southampton and South West Hampshire Research Ethics Committee (ref: 09/HO502/30) and the School of Psychology, University of Southampton and Research Governance (ref: 917/AB5). Parents gave written informed consent for their own participation in the study and their adolescent children’s participation. Adolescents after reading and considering the information sheets of the study were asked to sign an assent form for their participation in the study.
Participants
Participants were recruited through MS nurses and neurologists from two UK hospitals (Southampton (n = 39) and Liverpool (n = 10)) and adverts on MS-related websites (n = 55). Seventy-five adolescents completed hard copies of the questionnaires and 29 completed online questionnaires. The parents (n = 58) of the 75 adolescents who completed hard copies of the questionnaire were also asked to complete questionnaires about their MS. Sixty-two of these adolescents also completed the same measurements after 6 months in order to measure changes between illness perceptions and their adjustment and whether illness perceptions at baseline were associated with adolescents’ adjustment at follow-up.
Measures
Both parents and adolescents were asked to complete demographic questionnaires that included question about their age and gender, and parents were also asked about MS duration, type and whether they were currently on relapse or not.
To assess criterion validity, adolescents completed the PPIQ along with the following two questionnaires:
The Work and Social Adjustment Scale (WSAS; Mundt et al., 2002): a 5-item scale measuring the impact of illness on social and work/school activities that has been used with adolescent samples (e.g. Chalder et al., 2010). The mean score for this scale can range from 0 to 8. A high score means high impact of parental MS. For this sample, the Cronbach’s α was .78.
The Strength and Difficulties Questionnaire (SDQ; Goodman, 1997): a 25-item scale measuring emotional and behavioural difficulties that has good reliability and validity (Goodman, 2001). The mean score can range from 0 to 40. A high score means more emotional and behavioural difficulties. For this sample, the Cronbach’s α was .72.
Fifty-six parents with MS completed the EDSS–Self-Report (Bowen et al., 2001) in order to explore the associations between illness severity and adolescents’ illness perceptions and adjustment. This self-report version has very good correlation between patient and physician scores (Bowen et al., 2001). The total score can range from 0 (normal neurological exam) to 10 (death due to MS).
Statistical analyses
The data were analysed using SPSS (v17). Principal component analysis (PCA) with Varimax rotation was conducted to assess the factor structure of the questionnaire. Cronbach’s α was computed to assess internal reliability of the sub-scales. We hypothesised that adolescents’ adjustment will change over time and that adolescents’ illness perceptions at baseline will be related to adolescents’ adjustment at 6 months. Pearson’s correlations and linear mixed-effect models were computed to assess the relations between adolescents’ illness perceptions and adolescent adjustment and how changes in illness beliefs affected changes in adjustment, in order to assess criterion validity.
Study 2: Results
Participants included 104 adolescents between 12 and 19 years old (mean = 15.4 (1.97)). Of the 104 adolescents, 62 (59.6%) were female. The majority of participants were from United Kingdom (n = 97), three were from New Zealand, two from United States, one from Australia and one from Canada.
Structural validity and internal reliability
To validate the factor structure of the PPIQ and to determine which of the items best represented each of the dimensions, a series of PCAs were conducted. Varimax rotation was used, and the selection criterion was an eigenvalue greater than 1. Items measuring the ‘causes’ component were entered into a separate analysis as they were rated on a different scale.
In the first analysis, 41 items were entered into the PCA. This produced 13 factors, which together accounted for 70 per cent of the variance. Five items loaded onto factors that were not related conceptually (IP9, IP24, IP27) and one item did not load onto any factor (IP18); therefore, these were removed. The remaining 37 items were entered into a second PCA, which produced 10 factors accounting for 69 per cent of the variance. Six more items were removed that loaded on two factors (IP1, IP36) or loaded onto factors not related conceptually (IP8, IP14, IP25, IP30). Twenty-five items were entered in a final PCA, which produced seven factors with eigenvalues greater than 1 accounting for 65 per cent of the variance. Table 2 shows the labels of each factor, and that in the majority of cases, the items loaded exclusively onto one factor. One exception was the emotional representation item ‘My mum’s MS makes me feel angry’, which loaded .50 onto the emotional representation as well as .57 on the consequences for the family factor. All the sub-scales except the timeline chronic (α = .64) demonstrated good internal consistency with scores ranging from .71 to .79 (see Table 2).
Final principal components analysis, internal of the Perceptions of Parental Illness Questionnaire items.
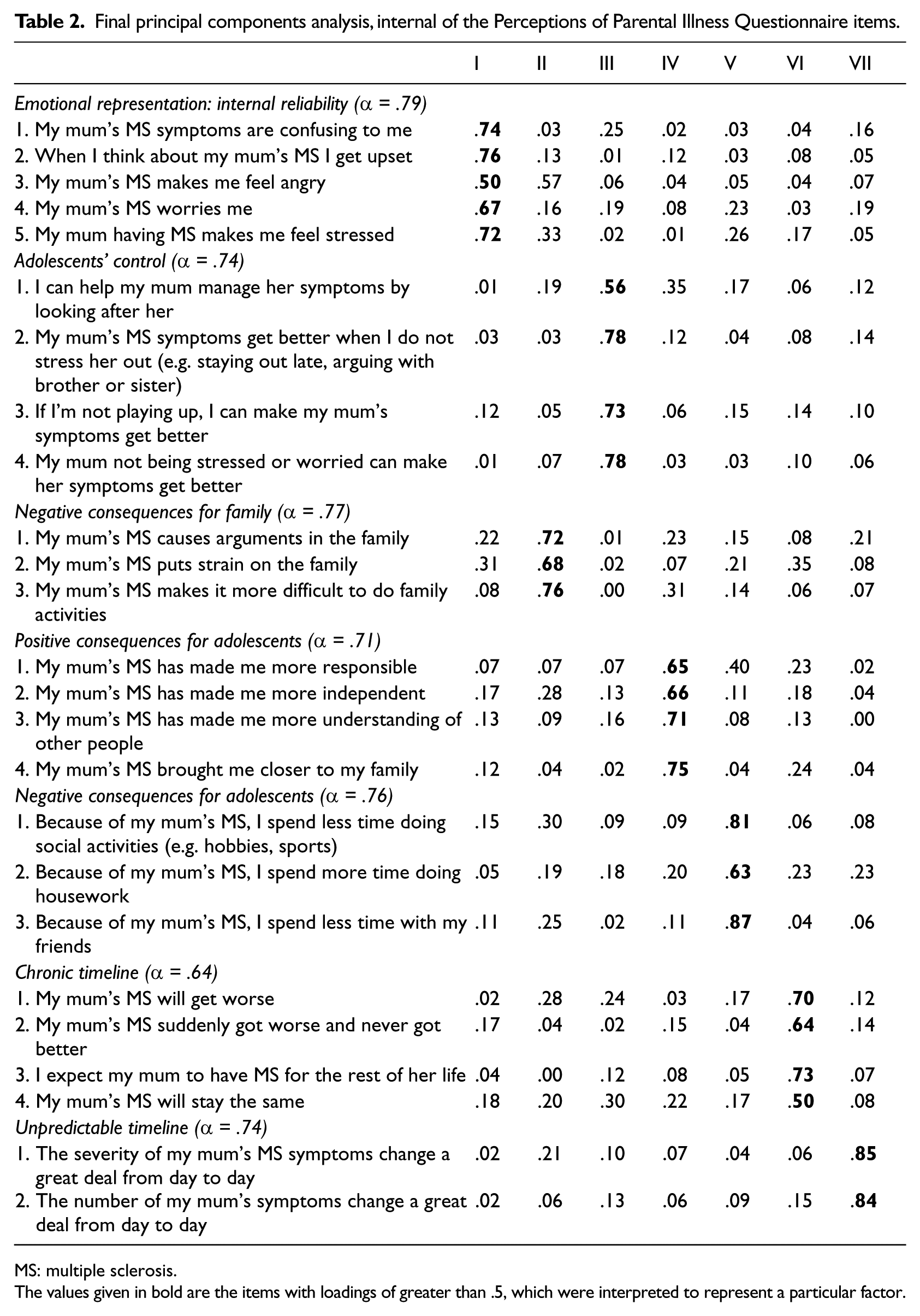
MS: multiple sclerosis.
The values given in bold are the items with loadings of greater than .5, which were interpreted to represent a particular factor.
Structural validity of the causal sub-scale
Five causal items were deleted because they lacked variability and were endorsed by very few of the people in the sample including ‘My dad’s/mum’s DNA’, ‘it’s passed by other people’, ‘something that he/she did’, ‘something to do with me’ and ‘God’s will’. The remaining items were entered in a PCA with Varimax rotation, which produced four factors accounting for 68 per cent of the total variance. The factor loadings for the individual items and their factors are presented in Table 3. The correlations between the items of each sub-scale were small and ranged from .24 to .48.
Principal component analysis of the Perceptions of Parental Illness Questionnaire causal items.

The values given in bold are the items with loadings of greater than .5, which were interpreted to represent a particular factor.
Criterion validity
Exploratory correlations werecomputed between the PPIQ sub-scales and the outcome variables to determine whether illness perceptions are associated with psychological adjustment as suggested by the CSM. The 75 adolescents who completed the hard copies of the questionnaire and then the 6-month follow-up were nested within 58 families; therefore, linear mixed-effect models were used to account for the family grouping of the data. Two separate linear mixed-effect models were computed with each of the outcome measures. The PPIQ sub-scales that were correlated with the WSAS and the total SDQ score at baseline were entered into each model as predictor variables. However, the PPIQ negative consequences for adolescents sub-scale was not included in the model for the WSAS, and the PPIQ emotional representation sub-scale was not included in the model for the SDQ due to item overlap between the scales. The total scores of WSAS were severely positive-skewed indicating low scores in this scale. The scores were then transformed using reciprocal transformation. Because of the transformation, the scores of WSAS were reversed. Therefore, high scores mean less impact of parental MS on adolescents’ life roles.
The results of these analyses are presented in Table 4. Mixed-effect models showed that adolescents’ beliefs about the impact of MS on the family environment (γfam.env. = 1.55, p = .01) and their beliefs about the unpredictable course of MS (γunpr. = 0.92, p = 0.05) were the strongest correlates to emotional and behavioural difficulties. On the contrary, adolescents’ beliefs about parental MS having an impact on the family (γfam.con. = −0.08, p = .001) and their beliefs about positive consequences of MS on their lives (γanx. = −0.12, p = .001) were the stronger correlates to adolescents’ emotional and behavioural difficulties.
Relationships between illness beliefs (PPIQ) at baseline and adolescents’ adjustment (SDQ, WSAS) at 6-month follow-up.
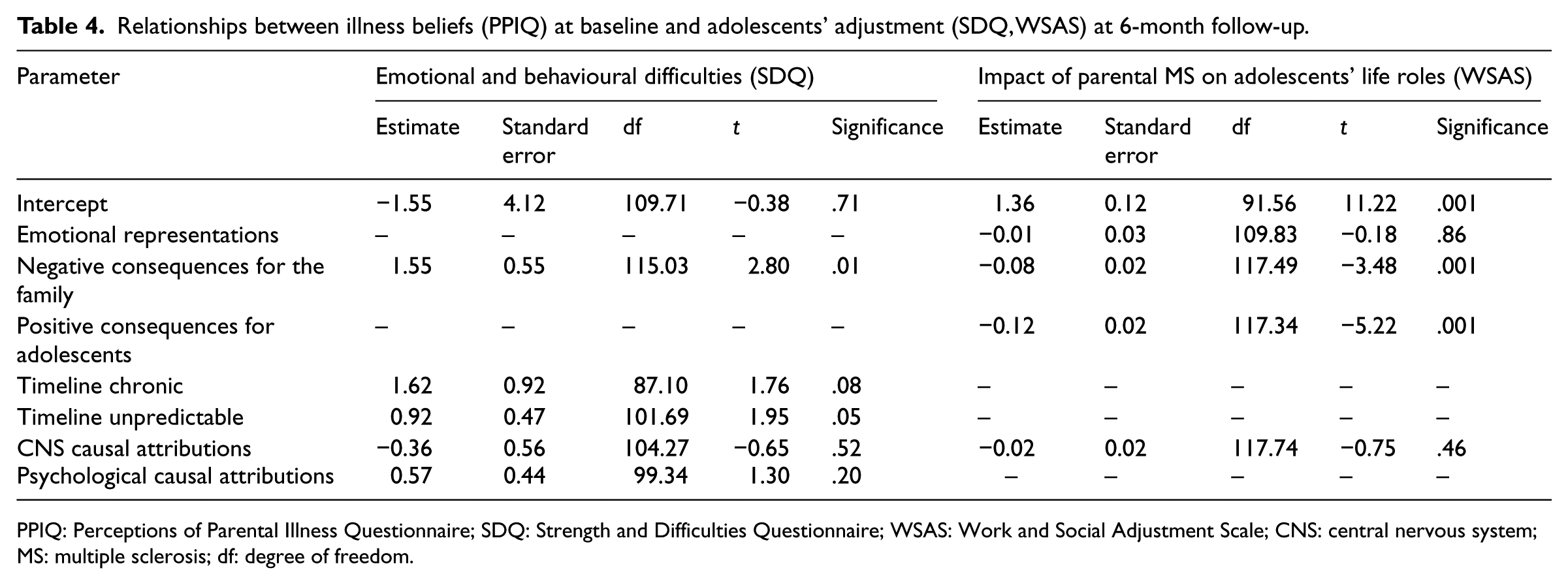
PPIQ: Perceptions of Parental Illness Questionnaire; SDQ: Strength and Difficulties Questionnaire; WSAS: Work and Social Adjustment Scale; CNS: central nervous system; MS: multiple sclerosis; df: degree of freedom.
Correlations between demographic characteristics and illness representations and adjustment
Relationships between adolescents’ and parents’ demographic characteristics and adolescents’ illness perceptions and adjustment measures were also investigated. Pearson’s correlations showed that the age of the adolescents was not related to either their adjustment or any of their illness perceptions. Two-way analysis of variance (ANOVA) also showed that the gender of the parent, the gender of adolescent and the interaction between the gender of the parent and gender of the adolescent were not associated with either adolescents’ adjustment measures or their illness perceptions.
One-way ANOVA showed no statistical significant effects of the type of MS on adolescents’ adjustment or any of their illness perceptions, with the exception of adolescent’s perceptions of MS unpredictability (F(2, 65) = 4.04, p = .02). Adolescents with a parent with relapsing remitting MS had significantly stronger beliefs that their parents’ MS was unpredictable compared to adolescents with a parent with primary progressive MS. Independent samples t-tests showed that adolescents with a parent currently reporting a relapse and adolescents whose parent were not in relapse during the time of the study did not differ significantly in their adjustment scores or their perceptions of parental illness. The only illness perception sub-scale that differed significantly was adolescents’ control (t = −2.67(66), p = .009). Adolescents with a parent who currently had a relapse had stronger beliefs about their control over their parents’ MS symptoms. Furthermore, Pearson’s correlations showed that the duration of parental MS was not associated with WSAS or SDQ or any of the parental illness perceptions. Pearson’s correlations also showed that only two PPIQ sub-scales were significantly correlated with illness severity. Higher EDSS scores were correlated with stronger beliefs about positive consequences for adolescents (r = .47, p = .001) and weaker beliefs about causal attributions to chance or hereditary (r = −.35, p = .003). Using partial correlations and multiple regressions controlling for illness severity, we explored the relationships between PPIQ sub-scales and adjustment variables. Controlling for illness severity did not affect the relationships between PPIQ and the adjustment variables.
Discussion
This article aimed to develop an age-appropriate questionnaire to measure adolescents’ perceptions of their parent’s MS, based on the CSM dimensions. Qualitative and cognitive interviews with adolescents in the piloting stage of the questionnaire helped to augment the face validity of the questionnaire by increasing the relevance and applicability of its items and decreasing problems with items in terms of their meaning and their wording. The results of the second study indicate that the PPIQ appears to be a valid and reliable measure for assessing adolescents’ illness perceptions of parental health.
The final sub-scales of the PPIQ differ somewhat from the original dimensions of the CSM. The consequences dimension was factored into three sub-categories, including negative consequences for the family and positive and negative consequences for adolescents. The timeline dimension was divided into chronic and unpredictable timelines. The unpredictable sub-scale showed some overlap with cyclical timeline. The dimensions identity, illness coherence and treatment control were not included as items for the sub-scales failed to load coherently onto factors during the PC analysis.
The scale also showed acceptable criterion validity. Consistent with the CSM and following studies on adults’ perceptions about their illness (Heijmans and De Ridder, 1998; Jopson and Moss-Morris, 2003; Murphy et al., 1999), adolescents’ perceptions about their parent’s illness were associated with psychosocial outcomes. In accordance with studies with adults with chronic illnesses (Scharloo et al., 1998), this study showed that stronger beliefs that the illness has negative consequences and is chronic and unpredictable were associated with worse psychosocial adjustment. However, contrary to studies on adults that have found that perceptions of control over the illness are positively related to psychological well-being and social functioning (Hagger and Orbell, 2003), perceptions that adolescents can help control parental MS symptoms were not significantly associated with either their emotional and behavioural difficulties or the impact of parental MS on their life roles. This finding suggests that adolescents’ beliefs about whether they can help their parents manage their symptoms did not impact on adjustment, based on the measures we used.
The effect of parental illness perceptions on psychological well-being and behavioural adjustment may also differ between long- and short-term adjustments. As shown in research on parentification in children of parents with HIV/AIDS, there is a negative impact on a premature assumption of parental roles on psychological adjustment of children in the short term (6 months), but there is a positive impact on their adjustment in the long term (6 years). Furthermore, even though the 6-month follow-up period for this study did not show any differentiations in adolescents’ perceptions of their parents’ MS, a longer investigation may have shown changes in illness perceptions as well as adjustment. In an ever-changing condition such as MS, illness perceptions may change over time as the illness progresses and the changes in adolescents’ perceptions may reflect on changes on how adolescents’ adjust. Longitudinal studies with longer periods of follow-ups are needed to investigate the potential changes and effects of illness perceptions and adjustment.
Some limitations of this study should be acknowledged. The adolescents who were asked for feedback in the cognitive interviews were the same whose interviews were used to develop the questionnaire items. Therefore, the questionnaire items might be very relevant only to this group of people. Also, the validation of the questionnaire was based on a relatively small sample. This sample was adequate for factor analysis based on the Kaiser–Meyer–Olkin measure of sampling adequacy (.61). However, future studies with larger sample need to replicate the results of this study and confirm the structure of the scale with the use of confirmatory factor analysis procedures.
In this study, the focus was on adolescents with a parent with MS. We suggest that PPIQ items can be applied to adolescents with a parent with other chronic illnesses with appropriate changes to the wording. Future validation research would be needed if the PPIQ was to be applied in the context of other chronic illnesses.
The development of the PPIQ is an important first step in measuring beliefs that adolescents hold about their parents’ health problems. Beliefs about emotional representation, negative consequences for the family, positive and negative consequences for the adolescent and timeline chronic and unpredictable were all associated with adjustment outcomes. If beliefs are shown to have a predictive role in determining psychosocial adjustment, then future interventions to improve adjustment in adolescents with a parent with chronic illness may benefit from exploring perceptions of the illness and helping to challenge these if necessary.
Footnotes
Acknowledgements
The authors would like to thank the UK MS Society for funding the project, the families who took part in the study, the neurologists (Dr Halfpenny and Dr Turner) and MS nurses (Carry Day, Jane Ware and Kerry Mutch) who helped us with the recruitment.
Funding
This study received financial support from UK MS Society.