
Abstract
In this article, we examine the bodily experiences of Mexican women, to investigate their acceptance of the thin ideal and resulting body dissatisfaction. We conducted semi-structured individual interviews with 30 adult participants in Mexico City. Interviewees accepted the thin body ideal, but experiencing their bodies as signifiers of motherhood protected them from body dissatisfaction. Instead of a personal body project, they engaged in a project of caring for their children’s bodies. We suggest that health campaigns directed to adult women should consider the relational aspects of their lives.
Introduction
Public health efforts are increasingly aimed at the prevention of chronic diseases (World Health Organization, 2008), and health campaigns stress the importance of keeping weight within a “healthy” range. At the same time, weight control is promoted by a culture that equates thinness to beauty and beauty to success and happiness (Bordo, 1993).
In this way, two mainstream discourses reinforce each other in the production of a cultural emphasis on thinness (Burns and Gavey, 2004). This, in turn, can promote a “normative discontent” (Rodin et al., 1984), with potentially serious psychological and physical consequences. Weight-related body dissatisfaction (BD) can lead to dangerous practices, including chronic dieting, cycles of food restriction followed by bingeing, compulsive exercising, or the use of weight-loss pills and laxatives (Neumark-Sztainer et al., 2006; Rich et al., 2010). BD can also be a precursor of eating disorders (Polivy and Herman, 2002).
BD, disordered eating, and the appreciation of the thin body ideal are present worldwide and among diverse social and cultural groups (Becker et al., 2004; Holmqvist and Frisen, 2010; McCabe et al., 2012; Swami et al., 2010). However, differences along sociocultural lines can still be observed. A recent review concluded that BD is more frequent among people with “a more Western life-style” (Holmqvist and Frisen, 2010: 135), and others have shown its relationship to social transition, cultural change, and globalization (Becker et al., 2004; Nasser et al., 2001). In the richer Western countries, BD varies according to culture or ethnicity, although in different ways that could depend on context. Thus, Kronenfeld et al. (2010) found African American women to be less dissatisfied with their shapes than Whites in the United States, while others have shown women from racial minorities to be equally or more likely than Whites to present disordered eating (Marques et al., 2011; Striegel-Moore et al., 2011). In nonrich countries, BD and disordered eating appear mainly (although not exclusively) among groups of higher economic and educational level, in cities rather than in rural areas, and among young women in professions, such as tourism, that require contact with an international audience (Alwan et al., 2010; Anderson-Fye, 2004; Becker, 2004; Katzman et al., 2004; Olsen et al., 2011; Palma-Coca et al., 2011; Swami et al., 2010).
The social and cultural origins of BD can be theorized in different ways. One of them is to suggest that women in cultures where the thin ideal is sustained are more likely to experience BD because they internalize the ideal. The thin ideal internalization is mediated by characteristics such as self-esteem, body weight, and the filtering of media messages through cognitive strategies (Ahern et al., 2011; Mask and Blanchard, 2011; Unikel et al., 2013).
Another approach, which constitutes the focus of this article, is the understanding of the relationship between body and self as a reflection of social values (Reischer and Koo, 2004; Turner, 1984). In this sense, Shilling’s (2003) concept of the body project can explain the presence of BD in modern societies. According to this author, the body in late modernity becomes a mean for the production of identity, through the enactment of reflexive body practices (Crossley, 2006) in which appearance is worked upon and transformed. The body project is an individualistic pursuit, in which anatomy is experienced as an “… entity in the process of becoming …” (Shilling, 2003: 4), that must be endlessly perfected in order to signify individual responsibility and social success. This description of a Sisyphean task fits the body-related anxieties of the “normative discontent” well. The concept of body project has been used in regard to the body-related practices of women, including body image preoccupation (Brumberg, 1997). But this is not the only way that body and self can be related. Thus, for example, Becker (1990) found that Fijians in a traditional society based a valued self-identity on the care bestowed on members of the community. As care was displayed through food-sharing, fuller bodies indexed success in the cultivation of relationships and were valued because of this. Importantly, fuller bodies were not individualistically produced to comply with a body ideal. Another interesting fact is the association of cultural change to the increase in BD in subsequent studies of the same population (Becker, 2004; Becker et al., 2007).
Research about the variation in BD between different societies can shed light on the ways culture either promotes or protects against this problem. In this article, we explore these issues by examining the body-related experiences of Mexican women. Our research questions were whether women in this setting endorsed the thin body ideal and its consequences in terms of BD and weight control practices.
Methods
Setting
A qualitative study was conducted from April to December 2011 in Mexico City. As other Latin American countries, Mexico has undergone rapid social change in past decades, which includes an increase in women’s participation in the paid workforce, higher female education, and smaller families. These changes have occurred faster than transformations in social gender norms (Garcia and De Oliveira, 2011). Social norms vary between socioeconomic segments, and those in the lower levels tend to endorse more traditional norms (De Oliveira and Ariza, 2002). Mexico’s Ministry of Health has included weight control as a main component of the national health strategy, and the acceptance of the thin ideal has been documented in urban and rural areas (Bojorquez-Chapela and Unikel, 2004; Perez-Gil et al., 2007). Therefore, Mexico is still a diverse country in terms of the sociocultural aspects related to BD and a good place to explore its variations.
Participants in this study came from three colonias (neighborhoods) in which, according to a 2005 survey (Bojorquez-Chapela et al., 2010), 68 percent of households were in the lower-middle and lower socioeconomic level, corresponding to monthly household incomes of roughly US$208–US$892 (López-Romo, 2005). The neighborhoods’ streets are lined by trees, and in every other block, there are small shops or stalls placed in doorways from which candies, food, or secondhand clothes are offered. No supermarkets, malls, or cinemas exist within the limits of the colonias. A big public park is nearby. Buildings are old, one- or two-storey. Seen from the outside, they could be ample one-family houses. Inside, they are divided into smaller apartments. Participants in this study lived in one of the two types of housing: a small house or room within a plot shared with extended family or a rented apartment. The nuclear family of two to six people usually occupied one or two rooms, some without an independent kitchen or bathroom.
Participants’ selection and characteristics
Adult (over 17 years) female respondents to a survey conducted in 2005 were invited in 2011 to participate in the interviews, through consecutive phone calls. No upper age limit was defined for this study. We made calls to 195 potential participants, reaching 62 (32%). The main reasons why the rest could not be located included the following: phone numbers registered in the previous study were no longer in service or the participant had moved out and left no contact data. Of 62 reached, 31 (50%) agreed to participate. One of them did not show up for the appointment, leaving a final group of 30 participants. The reason more frequently given for refusals was lack of time. Before the interview, participants read and signed an informed consent form. All procedures in the study were reviewed and approved by the Committee of Research Ethics of El Colegio de la Frontera Norte.
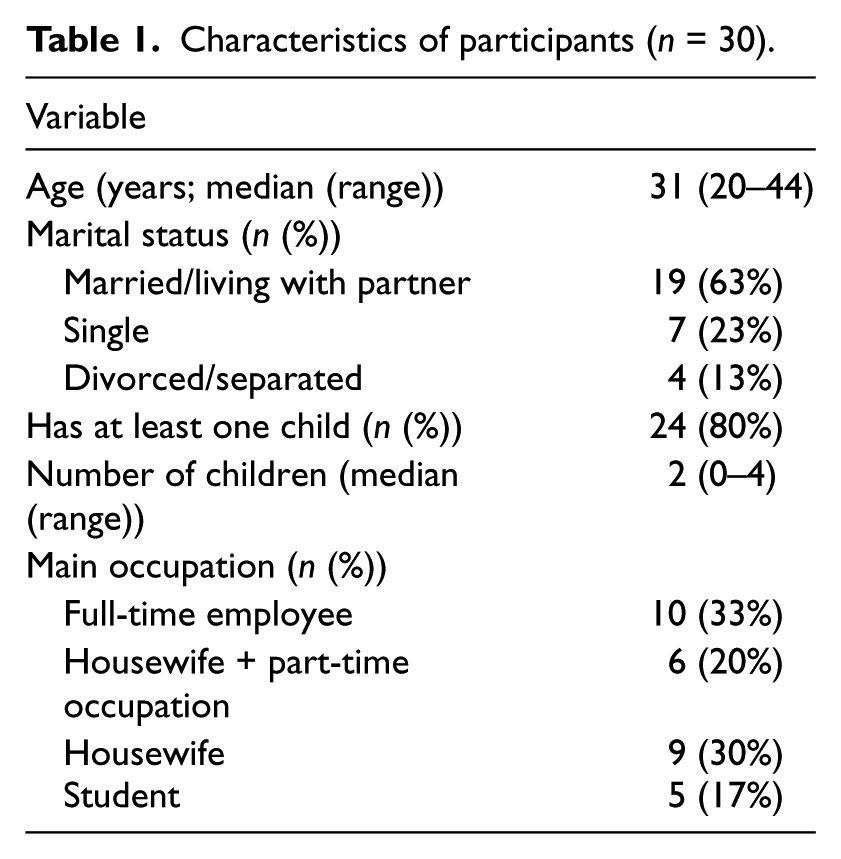
Table 1 shows some characteristics of the participants. Most of them were married or living with a partner and had children. Living arrangements included nuclear and extended families, but many of those in the former had other family close by and visited daily. Full-time employees had occupations such as cook, secretary, or sales. Part-time occupations included helping in family-owned shops or eateries, repairing clothes, or preparing food for selling at home. Two of the students also had paid jobs (one assistant cook and one cleaning/maintenance employee). During analysis, a group of eight participants was identified, whose responses consistently differed from those of the rest. While 7 of them lived with their parents (5 single and 2 who had separated from their partners), only 3 out of 27 of the other participants lived as single or separated women living with their parents. Also, five of the eight had no children, and five of the eight were students. We labeled them “younger women,” to convey our sense of them as more carefree and modern in their practices. Their median age was 27 years, and six of them were below 30 years.
Characteristics of participants (n = 30).
Data collection
We conducted semi-structured, individual interviews on the subjects of food and eating, body-related experiences, and weight control practices. Interviewers introduced subjects with probing questions (“How would you describe yourself?”; “How do you feel about your body?”), letting the conversation flow from there. Interviews lasted from 30 minutes to 1.5 hours. Three of the authors separately conducted the interviews. All of them are women, Mexican, and have a postgraduate degree. Interviews were audio-recorded and transcribed verbatim, and interviewers took notes afterward to register impressions about the person, context, and the results of the interview. Interviews were conducted, transcribed, and analyzed in Spanish. For this article, participant’s quotes were translated to English by one of the authors, and the translation was reviewed by a native English speaker fluent in both Spanish and English.
Of the interviews, 23 were conducted at the participant’s home and 7 in an office at a health research institution. In some cases, a third person (child or other relative) was present for at least part of the conversation. In no case was the third party perceived as intrusive by the interviewers.
Data analysis
We followed a modified version of grounded theory, appropriate for exploratory research where the aim is to allow meanings and themes to emerge from the participants’ accounts (Strauss and Corbin, 1994). From an early phase of the analysis, it came to our attention the scarcity of descriptions of self-oriented body-related practices, which we had expected would come up naturally, given our questions. Following this, we employed the concept of body project as a heuristic tool for contrast during analysis. In this, we followed the recommendations of interplaying data and theory during analysis and of complementing grounded theory methods with explicit theoretical frameworks (Henwood and Pidgeon, 1992; Kushner and Morrow, 2003).
Two of the authors separately coded all transcripts, and their preliminary conclusions were reviewed and discussed by all the authors. The first author conducted axial and selective coding, presenting results to the other authors and incorporating their comments in an iterative process, until conclusions were reached. Atlas.ti 6.2 (1993–2012, GmbH, Berlin) was used at all stages of analysis.
Findings and discussion
The first theme that emerged from the interviews was participants’ acceptance of the thin ideal. The second one, however, qualified this acceptance by situating bodily experience in the context of motherhood. In the last one, participants described how attending to the needs of their families took precedence over a personal body project.
The thin ideal: The beauty–health complex
Most respondents equated thinness with beauty and were dissatisfied with their bodies. To the question “How do you feel about your body?” 24 out of 30 interviewees responded with a version of “Not so well, I’ve been putting on weight.” The concern about weight gain was situated by participants in the context of changes in body shape from their younger age to present:
… How would you like to look like?
Actually I would like to have no belly, thinner … because I’m even going to do some sit ups to not have so much of a belly. But I just say it and don’t do it.
But you are quite determined.
Yes, I want to look as I used to, because, I say, I’m not that old as to start giving up on myself. (31-year-old, three children) 1
When asked to clarify why losing weight was important, all interviewees who were dissatisfied with their bodies responded that they wanted “to look good,” showing acceptance of the thin aesthetic ideal. A slim body was also considered important for “good presentation” at work and to keep a romantic partner interested. At the same time, 20 of them emphasized health as their main motivation for weight control (Dixon, 2009; Kwan, 2009):
[Describing why she is not satisfied with her body] … Right now for example being overweight. I mean, I don’t feel like, I mean, and a lot of people tell me “you’re tall, it doesn’t show, there’s no problem,” and I mean, but, it’s not that I’m not tall, but for example my feet swell up, that’s what I feel. And for example my father already is a diabetic, my grandfather passed away from diabetes, my mother has hypertension, so yes, I think I’m gaining weight and yes, I’m concerned about that. (31-year-old, one child)
Also related to the desire to lose weight was the wish for an agile, functional body. Participants mentioned that obesity was a problem because it made daily life activities more difficult:
How do you feel about your body?
… Bad.
Why?
Because I feel heavy, I get tired when I walk … I mean, yes, I feel it heavy, yes … (38-year-old, two children)
The agile body was also mentioned by many of the interviewees as a source of enjoyment, one which did not depend on fulfilling an aesthetic ideal, the gaze of others, or the fitting of clothes.
However, even though accepting the importance of thinness, almost none of our participants described weight control as central in their lives, and looking in a certain way was not “a priority” for them:
… I’m really not that concerned about what people think, if I were I would have gotten surgery … boobs on, tummy out, getting, what’s its name?… liposuction, right? But it’s not like that really, it’s not, my priority, my priority is to feel good, healthy. (44-year old, two children)
The eight “younger women” provided a contrast, as they described exercise as an important part of their lives and said that they constantly watched over what they eat. While the other participants rarely cooked or purchased special food for themselves, “younger women” described eating practices that were different from those of their families:
What do you [usually] have for lunch?
Well, I try to eat … I eat a lot of vegetables and fruit, so I take salads over [to work], as I’m a vegetarian, well … I don’t eat meat.
And, how do you manage at home? I mean, your mother is a vegetarian too?
No, nobody [is]
And, how do you manage?
Well, when they’re like, going to prepare meals, they cook for themselves and not for me, because I always tell them: “Cook for yourselves, I’ll cook for me afterwards.” (20-year-old, no children)
While most interviewees experienced some BD and engaged in weight control practices, their acceptance of the thin body ideal was qualified through a set of body-related meanings that were different from those of the health and beauty discourses. We develop this idea in the following sections.
A mother’s body: Anatomy as a signifier of motherhood
Out of 30 participants, 24 were mothers, and interviewees displayed pride in fulfilling this role. In their accounts, motherhood had a transforming effect on the body, causing weight gain via physiological changes and the antojos (cravings) of pregnant women. Cravings were described as natural, and scenes in which someone provided the desired food were pictured as happy moments. Keeping the weight after the child was born was described as one of the changes that came with maternity:
When I was single I weighted between 60 and 65 kilos. When I married I weighted between 70 and 72 kilos. After having my kids I gained weight, as is normal. (31-year-old, two children)
During that year when you had your second child, did you try to go on a diet or something?
No, no, no, no. Also I, eh, felt so ill that I was spoiled, almost like in the [television] add where I have a craving for strawberries and cream at three in the morning, and my husband hurries to get me it [laughter]. Yes, I was terribly spoiled, and of course I gained a lot of weight, because I was in bed almost all the time … I mean, whatever I craved, I ate. (36-year-old, two children)
Motherhood and the body were also related through the image of the self-sacrificing mother. Interviewees narrated how they had no time or money to spend on themselves because all resources were invested on children (Gillies, 2007; Martin Criado, 2007). This was a frequent explanation given for not being able to exercise, diet, or seek the advice of a nutritionist’s (practices that participant’s considered would help them losing weight). In the living context of these women, this self-presentation was of course realistic: one of the participants quit a zumba class because the price was increased from 10 to 30 pesos per session (approximately US$0.79–US$2.36). Child care, which could allow the woman to set aside some time for exercise, was also out of question unless another woman in the family could keep an eye on children for no cost. Structural factors limiting access to weight control practices were accompanied by the acceptance of a woman’s second place when it came to the use of resources, a common finding in studies of mothers’ leisure time activities (Dixon, 2009; Lewis and Ridge, 2005; Martin Criado, 2007; Miller and Brown, 2005).
In this way, participants depicted their bodies as products and signifiers of motherhood. Not having a body approaching the explicitly accepted aesthetic ideal was implicitly presented as expression of a female identity based less on individual presentation than in the woman’s position in a network of relations. This could even take the form of resistance to the thin ideal, on the grounds that it was unrealistic for a woman who had mothered children:
And now, you could say you enjoy your body, you like your body?
Well, I think you have to love it, right? I mean, all in all if I want my body … if I have sagging breasts but I already had … two pregnancies, my youngest son I breastfed less, the other one a whole year, and I mean what can I ask of my breasts, I had two pregnancies with huge babies. And yes, I have a lot of stretch marks, two cesarean sections. I better learn to live with that or I will never be comfortable in my body. All in all I do care for myself, I like to dress up, I like to look not that fat, lose weight, but in the end it’s the house of my soul, I have to learn to love it. (36-year-old, two children)
Similar to Becker’s (1990: 64) description of interpersonal care as “… indexed in changes in body morphology,” striations and weight gain were interpreted as the proud marks of pregnancy, the results of a corporeal sacrifice through which a valuable status was obtained. The bodies of interviewees were the result of caring for children and family and were presented discursively as markers of good motherhood. Being acceptant of their motherhood-infused bodies, participants were presumably less subject to BD.
It is not, however, that interviewees had never engaged in practices of body cultivation. In their stories, the transition from the role of single woman to the role of mother/wife defined the passage from investing efforts in one’s own body to cultivating the bodies of others:
[talking about the time when she was an aerobics instructor] And yes, I was fit, I lost weight too, I looked very nice and fit. I had many hours of classes. Then I started taking swimming lessons, because I didn’t know how to swim. I felt I was, how to say, a complete athlete at that time, sort of high performance, because I could resist a lot. Now I can’t. And suddenly I left it all because of the house, because the truth is you neglect … I was less depressed but I was neglecting the house, the children, and I was told [her husband told her] “Hey, you’re OK, you go out to take classes and everything [but], what happens to your home?” Then I got back to reality and you say “oops, it’s true.” (44-year-old, two children)
Of the 24 mothers, 16 in the sample described how, at a younger age, they used to “take care of themselves” (cuidarse) through food restriction and exercise, but then discontinued those practices in order to take care of their families. The dichotomy between “taking care of oneself” (cuidarse) versus “letting oneself go” or “giving up on oneself” (dejarse), representing two ways of self-relation, showed a certain questioning of the ideal of the mother who lives for others. Dejarse was not only presented as a sorrowful state and used as synonym of gaining weight through careless eating and lack of exercise but also used to describe times when the woman was unable to stand her own ground. Turning away from the relational narrative of motherhood, the cuidarse/dejarse dichotomy issued from a more individualistic plane:
… I like to take care of my family, but sometimes that also implies to leave the person [herself] a little bit aside [dejarla]. (36-year-old, two children)
In one of its aspects, dejarse implied that one’s (bad) physical state was a result of individual lack of responsibility, will power, or self-respect and was described as a character flaw. In a more positive note, descriptions of pleasurable bodily states came up in the context of cuidarse. Apart from dieting and exercising to lose weight, cuidarse activities included setting some time apart for oneself, exercising for relaxation or to take a break from daily concerns, and for participants who were economically better off, manicure and facials. Trying on clothes and dressing up could also be part of this pleasurable ensemble of body-related activities, although they were mostly mentioned by younger women.
In contrast to the preeminence of the mother role in other participants’ accounts, younger women described “the superwoman ideal” (Steiner-Adair, 1986), according to which a woman should excel in all fields. Therefore, for them, motherhood was important, but it had to be combined with success in career and beauty:
[…] also I used to look at my mom, I looked at her when she was leaving [for work], I was still very little, and I looked at her, how before getting in the shower she would do sit-ups, squats or something, I remember that clearly. You look at your mother, when you’re a kid, and you say “wow!” Right? Or, well, it depends on what kind of mom you have, but I used to look at mine and say “my mother takes care of us just right, she fixes breakfast for us, she goes to work, she comes back, she exercises, she does something to keep looking pretty and everything,” right? And that’s something that remains with me. (27-year-old, no children)
Another body project: The cultivation of other persons’ bodies
Participants in our study, while spending relatively little effort in transforming their own bodies, were highly dedicated to the cultivation of the bodies of children, spouses, and other members of the family. Even in sections of the interview that were intended to elicit descriptions of reflexive body techniques and perceptions of their own body, participants kept guiding the conversation in the direction of children and how to promote their growth. Decisions regarding what to eat were almost never made in reference to the woman’s needs or tastes, but following those of other members of the family:
[the interviewer asked about the woman’s likes and dislikes in food] … No sweet, and nor salted stuff … Because of my father [he has hypertension] I can’t cook salted stuff … and no sugar, because he is diabetic … So putting salt or sugar is forbidden to us, so I say “Ay, I’m not going to cook double, I better …” We all have to eat the same thing, and no, we don’t eat like that [with sugar or salt] anymore. (38-year old, two children)
According to the answers, a woman’s worth seemed to be, not in having a beautiful body herself, but in the sustenance of the bodies of others. The growing child’s body was proof of the mother’s success, and the mother was described as the only one capable of giving children a nourishing enough meal (Martin Criado, 2007). Food prepared by the mother and eaten at home was considered the basis for good upbringing and promotion of family values. Children who were short, weak, or falling behind in school were presented as the result of a mother’s selfishness:
What do you think is the consequence of eating well?
Health, mainly. And then performance, growth. I see a lot of the mothers of my children’s friends, they work, and about growth, they tell me “Oh, your son is so tall, he’s so strong.” Well, yes, their kids eat a snack at 11:00, and they get home at 5:00 and their mothers are just getting home from work, and they can’t prepare a meal. So, if I have … We have decided to sacrifice some things in exchange for others. I could find a job somewhere, and we could have more money, but, in what conditions would my family be? I mean, my children eat at home every day … They eat food that I prepare myself. (36-year-old, two children)
Some mothers closely watched over their children’s, and especially their daughters’, weight. One idea mentioned was that girls naturally need less food than boys, and they would get fat if let alone, and therefore, mothers needed to restrict their intake. Preventing girls from getting fat was for some an attempt to spare them weight-related bullying. Mothers in this sense can be seen as agents of normalization (Foucault, 1990), infusing in their children’s bodies the appropriate techniques:
How old is your daughter?
Ten. When she was nine she was a little overweight, because she wanted to eat as much as the boy. Boys eat more than girls. And she used to get mad and say “why you put more food in his plate, and less in mine?” “Because you’re younger” And I tried to explain, but she still was mad, because I served the boy a little bit more, she always noticed when I was giving him more soup, and a bit more of the main course. And, well, since they are only one year apart in age, the girl used to get mad, and … [the mother used to say] “Well, no, it’s because I don’t want you to get fat,” and so … (37-year-old, three children)
Conclusion
In this article, we explored the body-related experiences of Mexican women. According to our findings, participants were relatively protected against BD by a “motherhood project,” in which caring for the bodies of others took precedence over reflexive self-cultivation.
BD can be understood within the context of social values. The notion of body project suggests that in modern societies, self-reflective body practices are crucial for the production of a valued self-identity. However, as Shilling (2003) points out, power is at play in the construction of body ideals. Given the parallel discourses of health and the beauty ideal, it is not gratuitous that the pursuit of thinness has become one of the main body projects for modern individuals and especially for women (Brumberg, 1997). However, social values can influence bodily experience in different ways, and we argue that for the participants in this study, this experience is better explained in terms of relational identities and a different hierarchy of body-related values (Miller and Brown, 2005; Rubin et al., 2003).
Motherhood has profound effects on the embodied experience of self (Bailey, 1999). On the one hand, it changes the position of the woman vis-à-vis the thin ideal, as the body transitions from an object to be seen to an integral part of the mother–child relationship. On the other hand, it can reinforce gender stereotypes of women as caregivers, and in this sense be as much a disciplinary force as the thin aesthetic ideal (Bailey, 2001; Lewis and Ridge, 2005; Miller and Brown, 2005). This duality is reflected in our study in the way that the motherhood project, although limiting BD, also inhibited self-care. “Younger women” provided an interesting counterexample, as they described exercise and eating practices as part of ongoing projects of health and beauty. It is possible that these women are part of a different generation, one in which higher education and transformations in women’s roles are defining different social positions and constructions of motherhood (Becker et al., 2004; Nicolson et al., 2010). It could also be the case that they are in a different stage in the life course, and as time goes on, they might come to resemble the older participants. These are aspects worth of additional study.
A low response rate was one of the limitations of our study; however, the general characteristics of participants were similar to those of women in a previous survey of the same population. Also, interviewees identified the research team as part of a previous survey on nutrition and health, which despite our intentions to allow them to express freely could have made their responses more health oriented. Replication of our findings in a different group might help to clarify these issues.
Public health efforts to prevent chronic diseases have led to the implementation of campaigns centered on weight control, which could have as side effect an increase in BD (Neumark-Sztainer et al., 2006). They also tend to put the emphasis on individual behavior (Pond et al., 2010; Rich et al., 2010). A more comprehensive approach for public health campaigns directed to adult women should emphasize care and well-being, along with the relational aspects of their lives (Dixon, 2009; Lewis and Ridge, 2005).
Footnotes
Acknowledgements
The authors want to acknowledge participants’ willingness and generosity in sharing their time and stories with us. We also thank two anonymous reviewers for commentaries that greatly improved this article.
Funding
Support for this research was provided by the National Council for Science and Technology (CONACYT), Mexico (grant number SALUD-2010-01-141021). The funding source had no influence on the design, conduction, analysis, or decision to publish this research.