
Abstract
There is a high unmet need for contraceptives in developing countries such as Uganda, with high population growth, where efforts are needed to promote family planning and contraceptive use. Despite this high need, little research has investigated applications of health-behaviour-change theories to contraceptive use among this population. This study tested the Theory of Planned Behaviour’s ability to predict contraceptive-use-related behaviours among post-partum women in rural Uganda. Results gave modest support to the theory’s application and suggest an urgent need for improved theory-based interventions to promote contraceptive use in the populations of developing countries.
Introduction
The use of contraception, the intentional prevention of pregnancy by artificial or natural means, is a pressing issue worldwide. More than 120 million women aged 15 to 49 years who are married or in a union have an unmet need for family planning, meaning they want to avoid or delay pregnancy but are not using contraceptives (United Nations, 2011). The issue is especially in need of attention in developing nations, such as Uganda. At a population level, an increase in family planning programmes to regulate the number and spacing of children through contraceptive use could be a key factor in efforts to reduce poverty and Uganda’s high annual population growth rate, which in 2010 was 3.2 per cent, ranking Uganda the fifth highest globally according to The United Nations Children’s Fund (UNICEF) (2012) figures. At an individual level, contraception can play a key role in the control and spacing of pregnancy.
The 2011 Demographic and Health Survey (DHS) reports a 34 per cent unmet need for contraceptives among married women in Uganda (Uganda Bureau of Statistics and IFC International, 2012). According to the DHS data, 64 per cent of currently married women want to avoid pregnancy, 44 per cent of pregnancies are unplanned, and abortion and maternal mortality rates are high. Women who have recently given birth are likely to have an especially high demand for family planning services due to a desire to limit their number of children or delay their next childbirth. Only 14 per cent of currently married women were found to want a child in the next 2 years; the majority either wanted no more children or to wait at least 2 years (Uganda Bureau of Statistics and IFC International, 2012), but only 26 per cent of married women reported currently using an effective contraceptive method. The proportion wanting another child decreases with the increasing number of living children. Despite this need for, and desire to use, contraception, nearly 80 per cent of married women report using a traditional contraceptive method (2.9%) or no method (76.4%): the most common method among currently married women are injectables (14%) (Uganda Bureau of Statistics and IFC International, 2012).
A number of theories have been applied to explain the use of contraception and the interaction of individual and interpersonal-level factors that lead to decisions regarding their use. Research has shown that the most effective behavioural interventions are often grounded in conceptual models derived from theories of behaviour change (e.g. Fisher and Fisher, 1992). Despite this, many interventions do not incorporate theoretical models. Glanz and Bishop (2010) suggest that the preponderance of theories of health behaviour makes it difficult to discern which factors or theories are likely to be the most effective targets effective targets for a given intervention. The manner in which a theory is specified and the extent of its predictive value reflect, in part, the context in which it has been operationalized and tested.
There have been significant attempts to test theories predicting condom use; however, these applications have been largely focused on Western, mainly North American, populations (e.g. Myklestad and Rise, 2007; Sutton et al., 1999), or specifically on condom use with reference to disease prevention and decreasing HIV risk, rather than the behaviour of contraceptive use which is primarily concerned with preventing pregnancy (e.g. Lugoe and Rise, 1999; Molla et al., 2007; Schaalma et al., 2009; Wilson et al., 1992). One such model that has been regularly used to explain condom use and HIV risk behaviours in Africa is the Theory of Planned Behaviour (TPB; Ajzen, 1985). The TPB focuses on the relation of attitudes, subjective norms and perceived behavioural control as predictors of behavioural intentions which in turn predict behaviour. These three predictors are alleged to influence subsequent behaviour indirectly through intentions.
While individual-level factors identified by the TPB and other social cognitive theoretical models are recognized as possible contributors to behaviour, structural factors not addressed by these models may also be major contributors to contraceptive use. Inadequate availability of family planning services and health systems issues are common in resource-limited settings such as Uganda, and prior research found an association with such factors and low rates of contraceptive use and high rates of abortions (Creanga et al., 2011). The appropriateness of using social cognitive theories like the TPB in non-Western settings has been called into question (Campbell, 2003), and such frameworks have been criticized for masking important social, economic and political influences in their narrow focus on individual behaviours (Marks, 2008; Murray and Campbell, 2003).
Despite these limitations, behaviour-change theories have provided significant insight into the individual-level factors motivating risk behaviours and condom use for HIV prevention in resource-limited settings. A critical review of 11 studies in sub-Saharan Africa using TPB to predict sexual risk behaviour among youth found predictive ability of the model in all studies, supporting its use in urban, rural and traditional African settings (Protogerou et al., 2012). One study in this review among Xhosa-speaking South African youth found some support of TPB factors in predicting condom-use intentions, with significant associations found between attitude and perceived behavioural control, but no other variables (Jemmott et al., 2007). Schaalma et al. (2009) found TPB constructs with the addition of other factors to explain 77 per cent of the variance in condom-use intentions among youth in South Africa and Tanzania (Schaalma et al., 2009). Other work has validated TPB constructs in predicting intentions to use contraceptives in the Ethiopian cultural setting (Fekadu and Kraft, 2001). These studies lend support for the predictive value of TPB in resource-limited settings, warranting exploration of the appropriateness of using the TPB in the cultural context of Uganda.
However, previous studies have mainly focused on condom use for HIV prevention, with few exceptions (Fekadu and Kraft, 2001), rather than contraceptive use for pregnancy prevention. The extent to which such results can be generalized to general contraceptive use for pregnancy prevention purposes is uncertain. Altering the behavioural outcome (contraceptive use instead of condom use) and the expected outcome of such behaviour (preventing pregnancy instead of preventing HIV/AIDS) may alter the conditions and constructs which influence the behaviour and the associations between such constructs. Factors which lead to selecting a contraceptive method for purposes of preventing pregnancy have been found to be not always the same factors that influence choice of methods for purposes of preventing sexually transmitted diseases (STDs). For example, one study using two hypothetical vignettes assessed intentions to use condoms with a new sex partner (Hoefnagels et al., 2006). One vignette did not mention risk of pregnancy, and the other specifically stated there was no risk of pregnancy. When there was no risk of pregnancy, respondents’ intention not to use a condom was three times that of the condition in which pregnancy risk was not mentioned, indicating differential factors influencing condom-use intentions depending on concerns related to pregnancy versus STD prevention. Participants in this study responded to both vignettes, and researchers compared those who changed their response from condom use to no condom use when there was no pregnancy risk to participants who did not change their response. Perceived seriousness of STDs, perceived peers’ perceptions of seriousness of STDs, and perceived susceptibility to STDs after unsafe sex significantly predicted condom-use intentions among those consistent reporters, but was not a significant predictor among those who changed their intention to no condom use when there was no risk of pregnancy. Similarly, in a study among African American college students comparing correlates of condom use for those reporting use for pregnancy prevention only, disease prevention only and dual prevention, participants in the pregnancy prevention only group had fewer sexual partners, lower HIV risk perception and perceived less barriers to condom use compared to the other groups (Whaley and Winfield, 2003). Although other contextual factors not controlled for may also have an influence, it is possible that the differences between groups relate to differences in focus on disease versus pregnancy prevention. The two behaviours also differ due to the different methods involved in each and the implications that this has on factors contributing to intentions to use and actual use. In terms of preventing HIV/AIDS, the condom has historically been the only prophylactic which is effective in achieving such an end (although new effective methods such as antiretroviral therapy, circumcision and microbicides have been recently identified; Abdool Karim et al., 2010; Grant et al., 2010; Gray et al., 2007). In contrast, however, pregnancy prevention can be achieved through a variety of different types of contraceptives.
There are, however, many similarities in condom use versus contraceptive use behaviours, thereby raising the possibility that the general constructs and models used may still prove useful in explaining contraceptive use more generally. The TPB may therefore be useful in understanding the use of contraceptives for pregnancy prevention purposes. A woman may be more likely to intend to use contraceptives if she has favourable attitudes towards using contraceptives, perceives that her partner is supportive of using contraceptives and feels that she is able to use contraception and to discuss it with and persuade her partner. Many of the barriers identified by Ugandan women regarding contraception use reflect a lack of behavioural control and sexual relationship power on their part (Mugisha and Reynolds, 2008), reflecting the actual behavioural control construct which the TPB depicts as influencing both perceived behavioural control and the transformation of intentions into actions. There is, therefore, a need to empirically assess the extent to which the TPB can predict use of contraceptives for pregnancy prevention among rural Ugandan women.
The TPB has several constructs which are common to many other social–behavioural theories (e.g. Fishbein and Ajzen, 1975; Fisher and Fisher, 1992). It proposes that intentions are a predictor of behaviour and that these intentions are derived from personal attitudes and norms. However, it differs from other theories such as the Information–Motivation–Behaviour (IMB) model in its lack of an explicit construct of knowledge. The IMB model argues that information (knowledge) and motivation (including social norms, attitudes and intentions) predict behaviour both directly and as mediators through behavioural skills (similar to perceived behavioural control). One would expect knowledge regarding types of contraception to be a necessary prerequisite for contraceptive use; however, the evidence regarding the importance of knowledge in predicting behaviour is mixed. Several studies in sub-Saharan Africa have found contraceptive knowledge not to be a strong predictor of use (Grabbe et al., 2009; Moyo et al., 2012; Seutlwadi et al., 2012). This trend is mirrored in findings that levels of general knowledge regarding contraception are high in Uganda, while the use of contraceptives is low: 98 per cent of all women aged 15–49 years have heard of at least one effective method (Uganda Bureau of Statistics and IFC International, 2012). Although evidence exists regarding the potential generalizability of social cognitive theories of behaviour change to developing nations, the focus is largely on sexual behaviour in the frame of HIV/AIDS prevention. Further empirical investigation is needed as to whether such theoretical models are also relevant to contraceptive use for the purpose of pregnancy prevention in Africa. The TPB appears to be a promising model for factors predicting contraceptive use among a Ugandan population and warrants assessment of its predictive value. Other than structural factors, one possible limitation of the theory is its lack of an explicit knowledge component, a factor which may be especially variable and therefore critical in a resource-poor context. It would therefore also be useful to investigate the extent to which adding a knowledge construct to the TPB influences the ability of the theory to accurately model contraceptive use among Ugandan women.
The aims of this study were to test the extent to which the TPB predicts rural Ugandan women’s contraception-related behaviours for the purposes of pregnancy prevention and to determine whether adding the construct of knowledge improves the model.
Methods
Study population and procedure
The study was conducted at Gombe Hospital, a rural 100-bed public hospital in the Butambala district of central Uganda located approximately 2 hours by public transportation from the capital city of Kampala. The data were collected from pregnant women attending the antenatal clinic (ANC) at Gombe Hospital. This study was part of a larger study examining partner attendance at ANC and the uptake of partner HIV testing and use of contraceptives. Women typically attend ANC for the first time at the fourth month of their pregnancy and then approximately every month until the eighth month, at which point they return every 1–2 weeks. After delivery, the women return at 6 weeks for postnatal care and then at 10 and 15 weeks for infant immunizations. Family planning and contraception is discussed during ANC and contraceptives are available free of charge.
Women attending the ANC for approximately their seventh-month (M = 7.11 months, range = 5–8 months) visit were informed by hospital staff about the study and then referred to the research assistant, who explained the study and obtained written informed consent to participate in the study. Criteria for inclusion were as follows: being at least 18 years of age, the father of the current pregnancy being around and known (necessary for measures regarding partner interaction), living within approximately 20 km from the hospital and being willing to return for a follow-up interview. Overall, 49 women declined to participate. Participants (N = 301) completed a baseline questionnaire interview and a follow-up questionnaire interview approximately 10 weeks post-partum, although this time varied based upon when mothers brought their infants to the hospital for immunizations. Only data from the follow-up interviews were used for the present analyses since we were interested in potential contraceptive use at follow-up (post-partum), and participants were excluded if they did not complete the follow-up interview (n = 43) or if they reported wanting to become pregnant again within the next year (n = 6), as we assumed that the latter would have no reason to use contraception. Written informed consent was obtained from all participants and the study was approved by the Rhode Island Hospital Institutional Review Board (IRB) in the United States (the first author’s (S.M.K.) affiliation at the time of the study), Makerere University School of Public Health’s IRB in Uganda and the Ugandan National Council for Science and Technology.
Measures
We assessed the TPB constructs of attitudes, subjective norms, perceived behavioural control and intentions relevant to using contraception including the following three behaviours: discussing family planning with her partner, receiving couples counselling about family planning and using contraceptives. We assessed each construct with 3 items mapping onto those three contraceptive-use-related behaviours. We calculated the mean scores for the 3 items to obtain an overall score for each TPB construct. Attitudes items had the following stem: ‘how would you feel about …’, and responses were formatted on a 5-point scale ranging from ‘very bad’ to ‘very good’ (α = 0.80). Subjective norms focused on partner norms, through questions assessing how the participant perceived that her partner would feel about the three contraceptive-related behaviours listed above. Responses on the subjective norms items followed the format of the attitudes items (α = 0.98). We assessed perceived behaviour control using the following stem: ‘How hard or easy would it be for you to …’, and the responses were formatted on a 5-point scale ranging from ‘very hard’ to ‘very easy’ (α = 0.94). Intentions items had the following stem: ‘In the future do you plan to …’, and the responses ranged from ‘definitely no’ to ‘definitely yes’, on a 5-point scale (α = 0.73).
We also assessed participants’ knowledge of effective contraceptive methods using a series of nine questions in which participants were asked to rate the effectiveness of various types of contraception (e.g. pills, injections, tubal ligation, rhythm method/counting days, withdraw, etc.). Question responses were scored as either 1 (correct) or 0 (incorrect). Scores were then summed across all 9 items and a score indicating percentage correct was calculated.
The outcome measure was created from a series of questions about the participant’s current contraceptive-use-related behaviour with higher scores representing greater commitment to use contraception. The contraceptive-use-related behaviours were as follows: talking to her partner about contraception, receiving couples counselling about contraception, seeking contraceptive/family planning services and use of effective contraception since delivery. The following were considered to be effective contraceptives: pills, injections, condoms (currently using during at least 90% of sex acts), tubal ligation, vasectomy, interuterine device, implant and emergency contraception. Scores on the outcome variable ranged from 0 to 3 according to a ranking of the behaviours reflecting progressive behaviour towards contraceptive use: a score of 0 reflected having done none of the behaviours; a score of 1 was given to women who had discussed contraception with her partner but had carried out none of the other behaviours; a score of 2 was given if she sought contraceptive services or received couples counselling about contraception but did not report actually using any methods of contraception; a score of 3 was given if the participant reported using an effective contraceptive method since delivery.
Statistical analysis
Structural equation modelling, using Amos™ 18.0 (Amos Development Corporation, Craw-fordville, FL, USA) with maximum likelihood estimation, was used to test the fit of the data to the structure of the TPB model and causal paths among the latent constructs of attitudes, subjective norms, perceived behavioural control and intentions and the outcome of contraceptive-use-related behaviour. The analyses assessed the closeness of fit between the TPB model and the data. Root mean square error of approximation (RMSEA) and the comparative fit index (CFI) model fit indices are reported. SPSS was used to obtain the descriptive statistics. We modelled the TPB structure and then ran a second model adding the knowledge construct as a predictor of intentions.
Results
Participant characteristics
The sample size was 252 women aged 18–44 years (M = 25.69 years, standard deviation (SD) = 6.127 years). The majority (91.4%) of the women were married and living with their partner most of the time. In all, 97 per cent of the sample had received some schooling, with 54 per cent having attended primary only, 36 per cent attended secondary (3% completed secondary) and 7 per cent had a level of education which exceeded secondary. At baseline, the number of children the women already had ranged from 0 (28.8%) to 10 (0.7%, M = 2.27). The participants lived an average of 72 minutes away from the clinic and most commonly used a public minibus taxi (46.7%) or motorbike (33.8%) to get to the ANC. The average length of time since delivery at follow-up was 97 days (SD = 32.1 days, range = 17–203 days).
TPB constructs
Intentions towards contraceptive use were high: 57 per cent of the women scored the maximum possible, answering definitely yes to all 3 questions (M = 4.47, SD = 0.80). Attitudes towards contraceptive use were mostly positive, with a large proportion of the women (63.5%) scoring 5 (M = 4.67, SD = 0.57). Similarly, perceived behavioural control was high: 41.3 per cent reported maximum perceived control (M = 4.10, SD = 1.04). Subjective norms were also fairly supportive towards contraceptive use: over 60 per cent of the women answered very good to at least 2 of the 3 questions (M = 3.87, SD = 0.57) (Table 1). Knowledge regarding different methods of contraception was moderate, the mean percentage correct being 40.2 per cent (SD = 20.5). Despite this, actual contraceptive use was lower, with only 26.2 per cent reporting using effective contraception currently or since they had delivered (score of 3 on outcome variable). The most common type of contraception was injections (48.5% of contraceptive users), followed by condoms (consistent use: 18.2%) and pills (13.6%). Other methods were less common: tubal ligation and implant (6.1% each), multiple effective methods (3.0%) and withdraw and ‘counting days’ (1.5% each) (Table 2).
Descriptive statistics for the Theory of Planned Behaviour constructs.

Descriptive statistics for reported contraceptive use at post-partum.
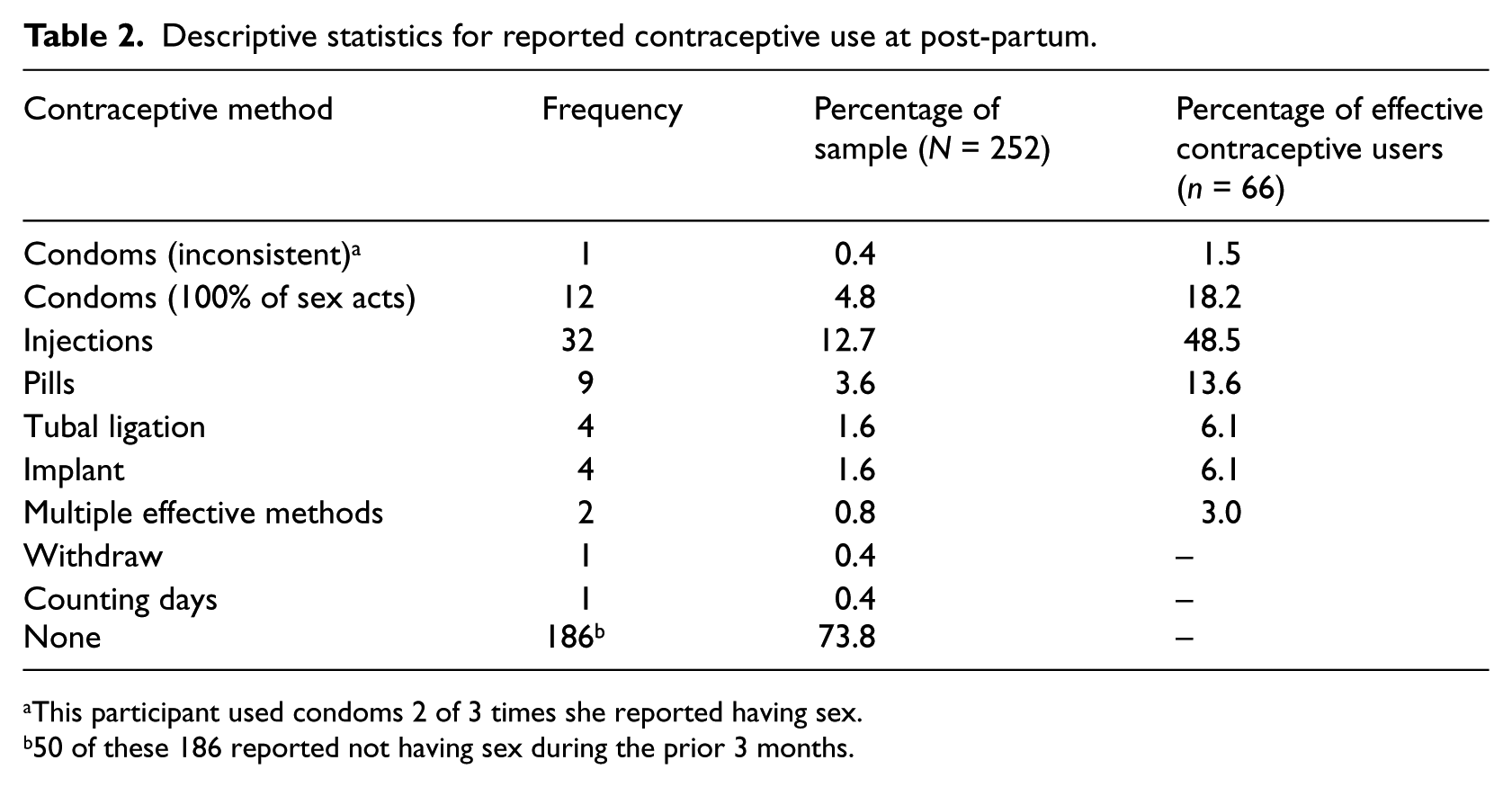
This participant used condoms 2 of 3 times she reported having sex.
50 of these 186 reported not having sex during the prior 3 months.
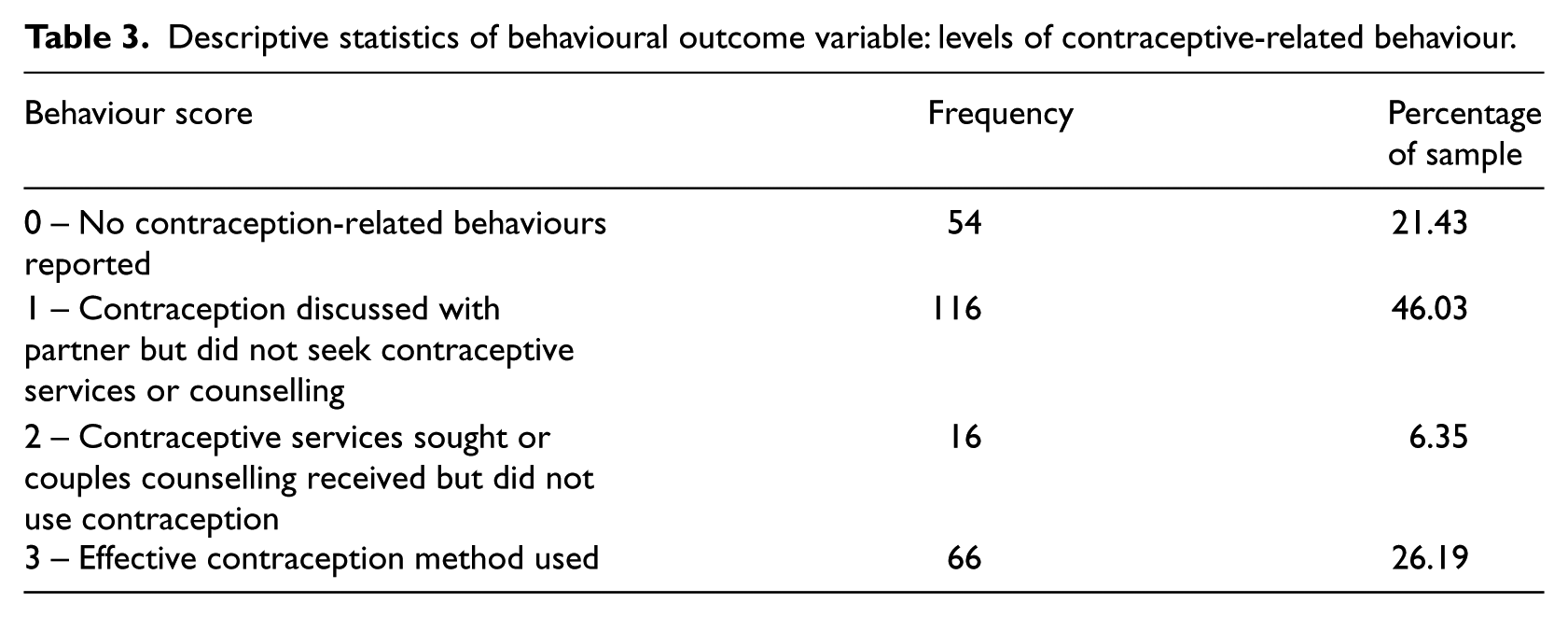
Over three-quarters (79.76%) reported having engaged in some contraception-related behaviour: 46.03 per cent report having just discussed contraception with their partner (score of 1 on outcome), and 6.35 per cent report having sought family planning services (either with or without their partner, score of 2 on outcome), but did not use contraceptives; 21.43 per cent of the sample therefore scored 0 on the outcome variable scale, indicating no contraception-related behaviours (Table 3).
Descriptive statistics of behavioural outcome variable: levels of contraceptive-related behaviour.
Model 1: TPB model
As shown in Figure 1, all specified relationships between constructs in the TPB were statistically significant, and the model explained 26.0 per cent of the variance in the outcome of contraceptive-use-related behaviour. A direct path from perceived behavioural control to behaviour was not found to be statistically significant and did not improve the overall fit of the model, and therefore, it was not included in the final model. The model was a good fit to the data: χ2 = 9.89, df = 4, p = .042, CFI = 0.985 RMSEA = 0.077, 90% confidence interval (CI): (0.014–0.13), which indicates a reasonable to good fit of the model (Bollen and Long, 1993).

Model 1: The Theory of Planned Behaviour model for contraception-related behaviour among post-partum women in rural Uganda.
Model 2: TPB adding knowledge
We also modelled the TPB adding contraceptive knowledge as a predictor of behavioural intentions. Figure 2 shows the coefficient path estimates for the new model. Overall, this model was also a good fit to the data: χ2 = 10.56, df = 5, p = .061, CFI = 0.987, RMSEA = 0.067, 90% CI: (0.00–0.12), but was not significantly better than model 1, which did not include knowledge: χ2diff = 0.67, df = 1, p > .05.

Model 2: The Theory of Planned Behaviour model adding a knowledge construct for contraception-related behaviour among post-partum women in rural Uganda.
Discussion
Contraceptive-use-related behaviour among post-partum rural Ugandan women was modelled using the TPB. The model was a good fit to the data and significantly predicted contraceptive-use-related behaviour, as measured with an outcome measure indicating increasing degrees of behavioural commitment. Attitudes, norms and perceived behavioural control were all found to significantly predict intentions to use contraception with perceived behavioural control being the strongest predictor. This suggests that the TPB may be a suitable theory upon which to understand the use of contraception for pregnancy prevention in this population. Adding the construct of knowledge was not found to significantly improve the fit of the model, however, suggesting that any impact of knowledge is likely to be indirect. This is supported by findings of often high levels of knowledge about contraception among the Ugandan population, yet low use of contraception (Uganda Bureau of Statistics and IFC International, 2012). Although knowledge is necessary for the use of contraception, it is not sufficient and is likely to be only a distal cause of intentions and behaviour primarily working through attitudes and perceived behavioural control (as evidenced by the observed decrease in association between these two constructs and intentions in the second model).
While attitudes, social norms and perceived behavioural control were significant predictors of contraceptive use among the study population, the TPB model explained 26 per cent of the variance in the outcome of contraceptive-use-related behaviour, leaving 74 per cent of the variance in the model unexplained by TPB variables. However, this percentage of variance explained is consistent with most other studies utilizing the TPB to predict sexual behaviour–related outcomes (e.g. Albarrcin et al., 2001; Armitage and Conner, 2001; Protogerou et al., 2012) as well as other behavioural theories (e.g. IMB; Fisher et al., 2009). Nonetheless, prior research has demonstrated the importance of structural factors in influencing contraceptive use in developing countries, including distal factors such as poverty, cultural norms, health-care access and gender inequity (Cleland and Watkins, 2006; Parker et al., 2000). For this reason, the utility of individual-level health-behaviour-change theories in resource-limited settings has been doubted (Campbell, 2003; Marks, 2008; Murray and Campbell, 2003). Such structural and community-level factors not included in the model may account for the large portion of unexplained variance observed, suggesting the need to further explore structural and community-level influences of contraceptive use among this population in order to develop future interventions aimed at increasing contraceptive use within this context. Such interventions may benefit from using an integrated, multilevel model that is both grounded in the principles of the TPB, particularly considering the interplay between attitudes, social norms and perceived behavioural control, and also considers structural variables such as poverty, health-care infrastructure and accessibility and other social, economic and political factors.
The use of contraceptives was generally low, with less than 30 per cent reporting using contraceptives. This low level of contraceptive use therefore does not wholly reflect the level of attitudes, norms and intentions which were moderate to high. Such psychological constructs were found to be better predictors of intentions rather than behaviour. The moderate to high levels of intentions to use contraceptives, but low levels of actual contraceptive use, may be indicative of higher level factors at play that were not captured by the TPB; as discussed above, even with high intentions to use contraceptives, social, economic and political factors beyond individual control may be impeding women’s access to and ability to use contraceptives. The low rates of actual contraceptive use may also partially reflect the sample: many of the women may have felt that they did not need to use contraception yet, since they had recently given birth. Lactation provides some level of pregnancy prevention due to delaying the re-onset of menstruation. Many of the women’s self-reported attitudes, intentions, norms and perceived behavioural control therefore may have reflected general ones related to a standard context and time, while their behaviour was more reflective of the specific circumstances in which they currently found themselves, having recently given birth.
A large proportion of the sample (46%) reported discussing family planning with their partner but did not report using contraception, even though they did not want to become pregnant again within the next year. Examining potential reasons for why these discussions did not result in contraceptive use, we found that compared to women who reported using contraception, women who reported only discussing family planning with their partner perceived that their partner wanted them to have a slightly greater number of additional children (M = 3.07 vs 3.25, non-significant difference), despite the fact that there was no difference between these two groups based on the number of additional children the women themselves wanted to have (M = 2.18). There was no difference between perceived partner attitudes about using contraception between these two groups.
Limitations
We acknowledge a number of limitations which may limit the generalisability of these findings. First, all data were self-reports and therefore rely on the accurate recall and honesty of participants. Furthermore, all participants were women who had recently given birth: contraception use in these situations is likely to be lower than at other times (Ross and Winfrey, 2001), partially due to natural contraceptive properties of having recently given birth until menses returns. Timing of the follow-up interview after delivery varied between 17 and 203 days post-partum. This occurred because, to reduce participant burden, the women were asked to complete the interview when they brought their infant for immunizations. While the immunization schedule recommends a 10-week immunization visit, mothers did not adhere to this schedule. This may have introduced additional heterogeneity in the data. All participants were also women attending ANC, and therefore, the findings may not generalize to women who do not attend ANC. A large proportion (95%) of women in Uganda, however, do receive antenatal care from a skilled provider (Uganda Bureau of Statistics and IFC International, 2012), so this is not likely to be overly problematic. In addition, the TPB accounts for primarily individual-level influences on behaviour and does not account for structural or community-level factors such as health systems issues, which may also influence women’s ability to use contraceptives. Additional research that incorporates factors at multiple levels (e.g. individual, community, structural and policy) is needed to fully understand contraceptive use among rural Ugandan women. Additional research is also needed to confirm and elaborate these findings, especially about how to translate couples’ discussions about family planning into actual contraceptive use when the couple does not want to become pregnant in the near future.
Conclusion
This research demonstrates the utility of applying a well-articulated theoretical model, the TPB, in efforts to understand contraceptive use behaviour in a population of post-partum women in Uganda. Given Uganda’s high population growth rate, high poverty, high unmet need for contraception and high maternal mortality rate (Uganda Bureau of Statistics and IFC International, 2012), these findings are especially germane to current efforts by international organizations including United States Agency for International Development (USAID), Family Health International, Marie Stoppes and United Nations Population Fund (UNFPA) to promote family planning in Uganda. The results suggest important factors to consider when developing interventions promoting contraceptive use in developing countries similar to Uganda.
Footnotes
Acknowledgements
The authors thank Katelyn Sileo for her research and editorial assistance. We also thank Harriet Nantaba, Hajara Kagulire and Farouk Kimbowa for their assistance with data collection, and the midwives at Gombe Hospital.
Funding
This study was supported by an Innovations in Women’s Health Research Seed Grant from Brown University/Women & Infants Hospital National Center of Excellence in Women’s Health. S. Kiene was supported by a K01 Mentored Research Scientist Development Award from National Institute of Mental Health (NIMH) (K01MH083536). S. Hopwood was supported by the Craig Studentship for graduate study at Brown University.