
Abstract
The objective of this study was to develop the Pro-Change Functional Well-Being Scale, a measure that provides an informative evaluation of general functioning loss due to well-being-related barriers. Exploratory and confirmatory analyses on data from 642 individuals supported a one-factor solution with good model fit. A strong positive correlation existed between the Pro-Change Functional Well-Being Scale and Well-Being Assessment for Productivity. Initial construct validity was demonstrated by predictable relationships between functioning loss and other measures of health and well-being. This initial psychometric evidence suggests that the Pro-Change Functional Well-Being Scale is a reliable and valid assessment of functioning loss due to common well-being-related barriers.
Well-being, functioning, and productivity are a central focus of both the health and job performance literature. The study of well-being in the context of health is growing rapidly. Recent years saw a 227 percent increase in the number health psychology articles focusing on constructs such as well-being, quality of life, and other aspects of optimal human functioning (Schmidt et al., 2011). This last decade also saw increasing attention to health-related factors that influence well-being such as mental illness, disability, infectious disease, and problematic lifestyle behaviors (Camfield and Skevington, 2008).
Research has now conclusively linked positive well-being with decreased morbidity and mortality among healthy and medical populations (Chida and Steptoe, 2008). This relationship is likely due to multitude of factors. Regular exercise is linked to positive mood states and better overall physical health (Gaitan-Sierra and Hyland, 2013; Penedo and Dahn, 2005). Weight loss can increase well-being and decrease depression (Gaitan-Sierra and Hyland, 2013; Wright et al., 2013), and those with higher well-being typically have better social support and access to financial, health, and environmental resources (Camfield and Skevington, 2008). Well-being, however, is not a static construct. It can be increased through intervention. Among patients with cancer, psychological distress can be decreased by physician-initiated assessment and discussion of well-being (Adamsen et al., 2006; Velikova et al., 2004), and interventions to increase physical activity can increase well-being (Adamsen et al., 2006). Cross-cultural research also emphasizes the importance of well-being and health optimism for health functioning across demographic groups (Ruthig and Allery, 2008). In short, assessing and studying well-being can help researchers understand and promote health across diverse populations and issues.
Well-being is also the focus of job performance research because of its strong link to worker satisfaction and productivity. Decreased productivity is related to physical and emotional health problems (Collins et al., 2005; Goetzel et al., 2002), psychosocial stress, suboptimal working conditions (Spector and Jex, 1998), and personal problems (Allen et al., 2000). The Well-Being Assessment for Productivity (WBA-P) is a measure that was designed to assess well-being-related barriers that reduce productivity, thus providing organizations with detailed information about the sources and consequences of differential levels of well-being among employees (Prochaska et al., 2011). The validity of the WBA-P was supported by correlations with two other commonly used measures of workplace productivity, the Work Productivity and Activity Impairment Questionnaire–General Health (WPAI-GH) and the Health and Work Performance Questionnaire (HPQ) (Kessler et al., 2003; Reilly et al., 1993). The findings indicated that the WBA-P captured unique and common variance in key constructs relative to these established measures. The WBA-P also showed that productivity loss increased significantly as the number of chronic conditions and risk behaviors increased, and as overall, physical and emotional health decreased. This study aimed to expand the application of the WBA-P (which specifically addresses productivity in the workplace) to a broader population of both employed and unemployed individuals in order to assess the impact of well-being on daily functioning outside of the workplace.
The Pro-Change Functional Well-Being Scale (WBA-F)© is, to our knowledge, the first measure developed that examines the relationship between general domains of well-being (e.g. physical and emotional health, psychosocial stressors, and basic access; Evers et al., 2012; Gallup, Inc., 2009) with functioning and in daily life among nonmedical populations. Contemporary models of health recognize that well-being, functioning, and health are intimately connected. This measure is consistent with this well-being approach to health promotion in that it aims to improve the functioning of the whole individual at home, at work, and in the community (World Health Organization (WHO), 2006).
“Functioning” is a generic term used in the health and disability literature to describe the complex relationship between an individual, the environment, and a disease (WHO, 2012). The focus on functioning as opposed to disability is a paradigm shift intended to place ability and disability along a continuum and to characterize illness according to how it impacts a person’s everyday life. Functioning, in a health context may be defined generally in terms of abilities to participate in various activities, or more specifically in terms of distinct activities of daily living such as self-care and housework (Salvador-Carulla and Gasca, 2010). This study defines functioning more broadly as “the ability to concentrate or do one’s best in day-to-day life.” Rather than a prospective belief in one’s ability, which would be more aligned with self-efficacy (Bandura, 1977), this subjective view of ability is retrospective.
This study describes the development and validation of the WBA-F, a measure of functioning loss due to well-being-related barriers. The WBA-F was designed to act as an independent, subjective measure of functioning loss and to extend the WBA-P (Prochaska et al., 2011) to nonworking populations. It is appropriate for all individuals regardless of health or employment status.
Method
Instrument development
Items for the WBA-F were adapted from the WBA-P (Prochaska et al., 2011) which asks participants to rate how often specific situations caused them to have difficulty concentrating at work. The stem for all of the items in the WBA-F was revised to eliminate the specific reference to the workplace. Eight of the original 11 WBA-P items required no further refinement. The remaining 3 items in the WBA-P referred specifically to work-related concerns such as “lack of training” and “technology issues” and were therefore not included. In order to expand WBA-F measure to look at the effect of all relationships in the individual’s life (not just coworkers), three additional items were added (family, friends, and others). Finally, two additional items were added to the WBA-F initial item set to deal with issues of boredom and being tired. This resulted in an initial item set of 13 items. Participants were asked to rate on a Likert scale (1 = a lot, 2 = some, 3 = not at all) their ability to concentrate or do their best when dealing with these issues over the prior 4 weeks.
Participants
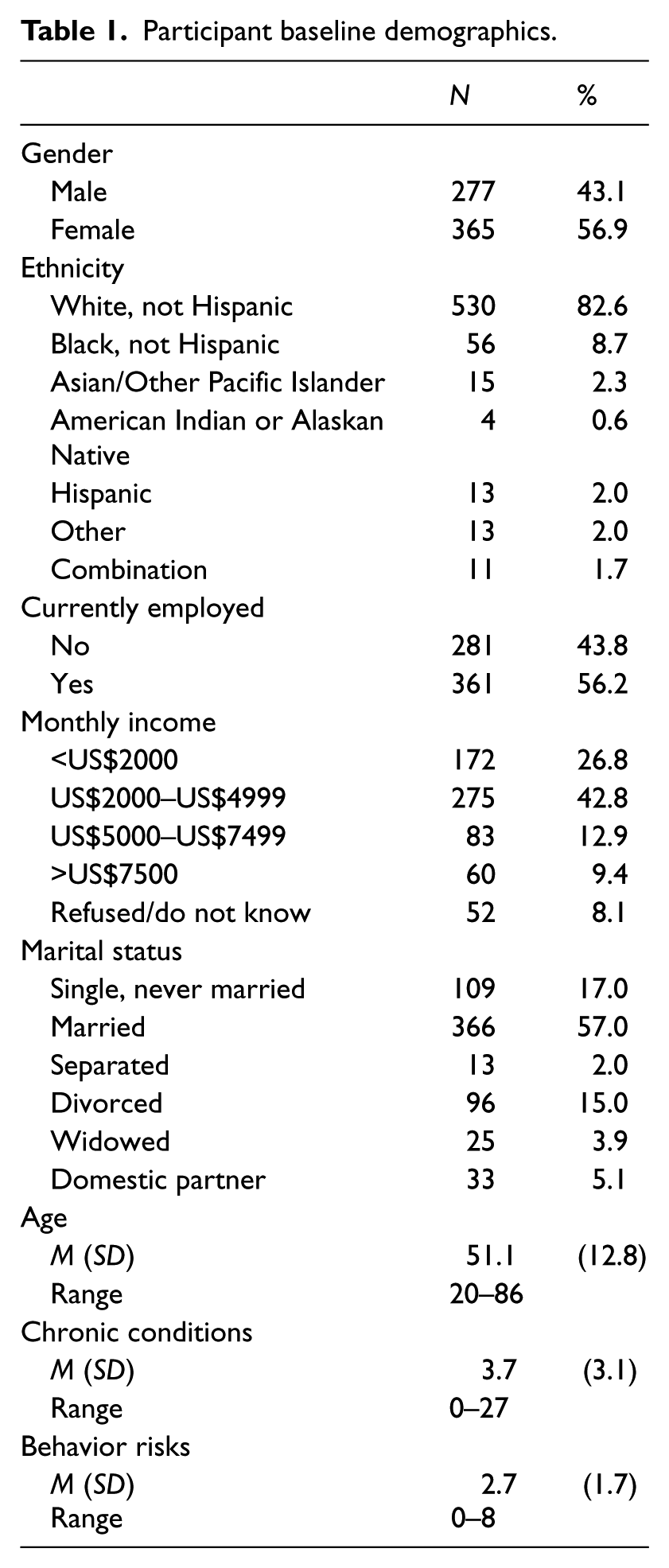
Data from 642 participants were collected via the Internet and recruited through a survey sampling company with a national panel of roughly 1,500,000 potential participants. Invitations to participate in the research were emailed to potential participants who then were able to complete a screener to ensure that they were over the age of 18 years, English speaking, and consented to participate as part of a larger randomized clinical trial to enhance multiple domains of well-being by decreasing multiple health risk behaviors. All of the questions included in this study were administered via a single assessment to the whole sample. Participant baseline demographics are reported in Table 1. The sample was 56.9% male and 82.6% white. The mean age was 51.1 years (standard deviation (SD) = 12.8 years), and the majority of the sample was employed (56.2%). Roughly 43% reported having an average monthly household income in the US$2000 to US$4999 range.
Participant baseline demographics.
Measures
A variety of measures were included in the study. In addition to demographics (i.e. gender, age, employment status, income, etc.), the following assessments were included:
WBA-P
This is an 11-item, two-factor measure of presenteeism and job productivity loss due to personal problems and work-related well-being barriers (Prochaska et al., 2011).
Life evaluation
This is a 2-item measure from the Cantril Self-Anchoring Striving Scale (Cantril, 1965). Participants were asked to evaluate their lives and imagine a “ladder” with steps numbered from 0 to 10, where “0” represents the worst possible life and “10” represents the best possible life. Gallup classified people as either “thriving” (presently standing on step 7 or higher and expecting to stand on step 8 or higher 5 years from now), “suffering” (presently standing on steps 0–4 and expect to stand on steps 0–4, 5 years from now), and “struggling” (those who are neither “thriving” nor “suffering” (Gallup, Inc., 2009).
Health Risk Intervention Assessment
The Health Risk Intervention (HRI) Assessment is an expansion of a general health risk assessment that includes measures of chronic conditions, overall health, physical and emotional health, and behavior risk factors (Prochaska et al., 2008). Participants were assessed on 11 specific chronic conditions and 9 behavior risk factors. Chronic conditions and behavior risks were summed separately and categorized into categories of 0–2, 3–4, and 5 or more. An individual item assessed perceptions of overall health ranging from poor to excellent. Separate individual items also assessed perceptions of physical and emotional health on a 0–10 scale with 0 being the worst health and 10 being the best.
Statistical procedures
The WBA-F was developed using sequential measurement development (Jackson, 1970) where the sample was randomly split in half for exploratory and confirmatory analyses. Exploratory analyses were conducted using principal component analysis (PCA) with varimax rotation. The minimum average partial (MAP) procedure (Velicer, 1976; Velicer et al., 2000) and parallel analysis (Horn, 1965) were used to determine factor structure decisions. Item loadings and breadth of content determined the final number of components to retain. Confirmatory factor analysis (CFA) was conducted on the second half of the sample using structural equation modeling to validate the model found by the PCA.
Correlations between WBA-F and two factors of the WBA-P were examined to determine convergent validity. Analysis of variance (ANOVA) was used to determine the relationships between the WBA-F and self-reported indices of chronic health conditions, health behavior risks, quality of overall health and physical health, and levels of emotional health and life evaluation. This type of analysis provided evidence of construct validity and has been identified as the most fundamental of best practices for developing measures of productivity (Schwartz and Riedel, 2010).
Findings
Exploratory factor analysis in the first half of the sample (n = 325) indicated a single-factor solution. Three items were removed due to low loadings and breadth of content in a series of iterations on the measurement model. Optimal results in the exploratory sample were achieved with a one-factor solution, accounting for 46% of the variance. Item loadings ranged from 0.53 to 0.82 (average loading = 0.67). CFA on the second half of the sample confirmed the one-factor exploratory model, χ2(35) = 243.16, comparative fit index (CFI) = 0.85, average absolute standardized residual (AASR) = 0.05, and root mean square error of approximation (RMSEA) = 0.13. Item loadings ranged from 0.48 to 0.85 (average loading = 0.64), with high internal consistency (α = 0.88) (see Figure 1). Convergent validity was evidenced by significant correlations with the two factors of the WBA-P (r = 0.53 for the work factor, and r = 0.76 for the personal problems factor).
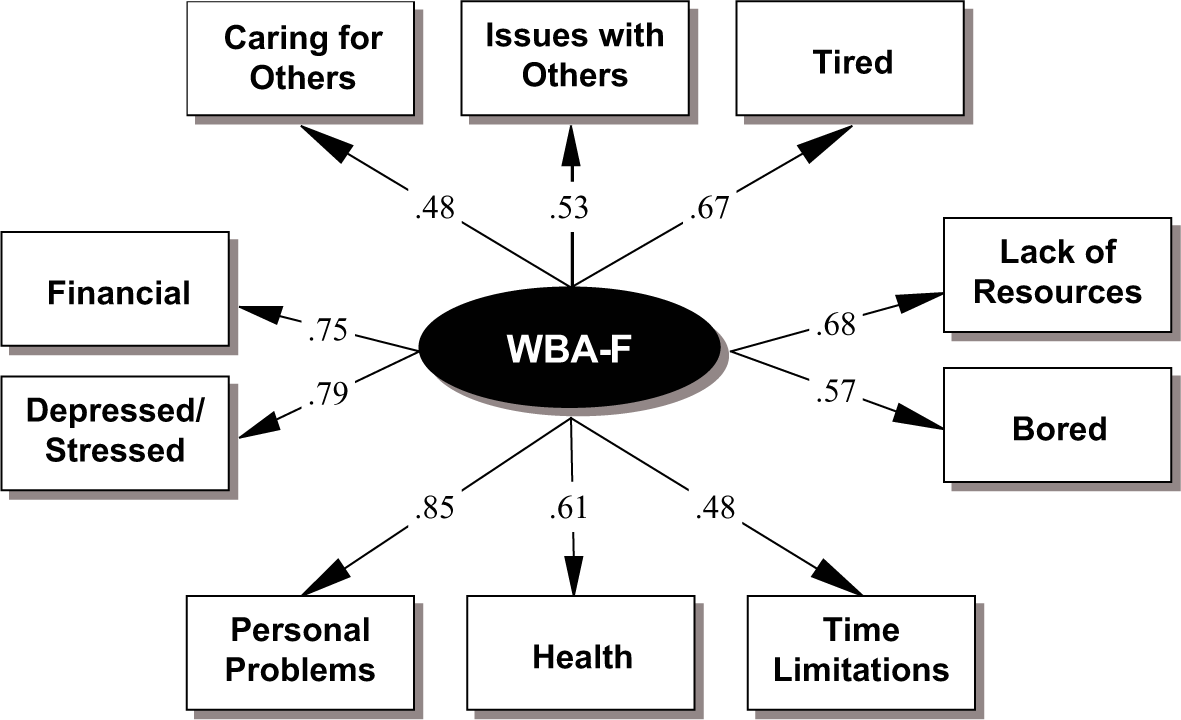
Well-being assessment of functioning structural model.
A series of ANOVAs detected significant relationships between the WBA-F and several demographic factors including gender (F(1, 648) = 30.20, p < .001, η2 = .05), age (F(3, 646) = 8.07, η2 = .04), income (F(3, 592) = 5.19, p < .01, η2 = .03), and employment status (F(1, 648) = 21.69, η2 = .03). Women (M = 29.43, SD = 23.43) reported more functioning loss than men (M = 19.92, SD = 19.69). Those in the 18–34 years age range (M = 33.97, SD = 2.9) reported higher functioning loss compared to all other age groups. Those between the ages of 35 and 49 years (M = 25.66, SD = 1.53) and 50 and 64 years (M = 25.25, SD = 1.32) reported more functioning loss compared to those in the 65–86 years age range (M = 17.28, SD = 2.32) age bracket. Participants with a monthly household income of less than US$2000 (M = 30.17, SD = 25.26) reported more functioning loss compared to those making between US$2000 and US$4999 (M = 24.0, SD = 21.58), US$5000 and US$7499 (M = 22.14, SD = 19.93), and US$7500 or more (M = 19.08, SD = 19.10). Participants who were unemployed (M = 29.81, SD = 23.90) reported more functioning loss than those who were employed (M = 21.73, SD = 20.30).
Table 2 summarizes ANOVA results and relationships between the WBA-F and measures of health and well-being (see Table 2). Generally, as reports of health and well-being worsened, the amount of functioning loss due to well-being-related barriers increased. Effect sizes ranged from medium to large in magnitude (Cohen, 1988).
WBA-F relationships with health and well-being.
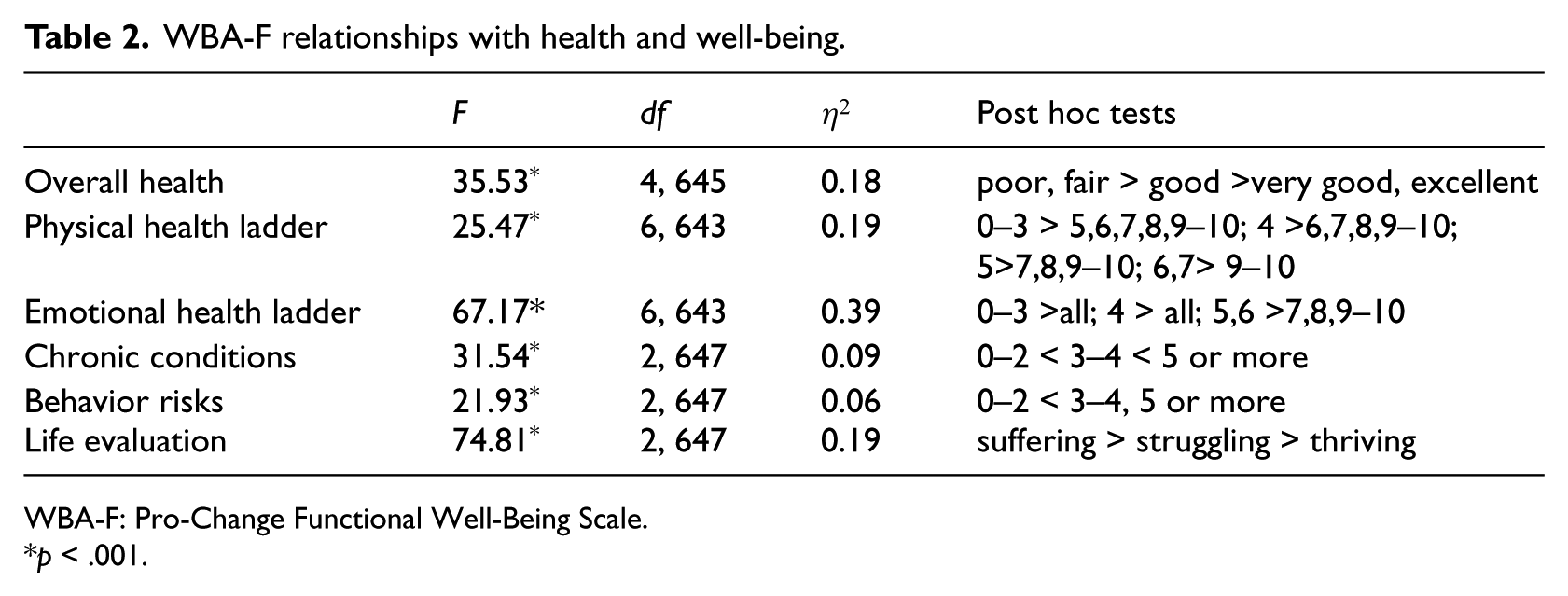
WBA-F: Pro-Change Functional Well-Being Scale.
p < .001.
Discussion
Results suggest that the WBA-F is a reliable and valid measure of overall functioning due to well-being-related barriers in a sample of employed and unemployed individuals. Exploratory and confirmatory analyses indicated a single-factor solution for this measure. Strong positive correlations with the two factors of the WBA-P measure indicate convergent validity. Additional construct validity was evidenced by higher reported functioning loss among participants with more physical and emotional health problems, chronic health conditions, and lower life satisfaction.
Significant differences in well-being-related barriers were found for gender, age, income, and employment status. These findings are consistent with demographic differences in health-related functioning in the literature that generally indicate women, the unemployed, and those with lower socioeconomic status (SES) suffer from more health-related decreases in functioning (Hemingway et al., 1997; Hopman et al., 2000; McKee-Ryan et al., 2005; Obidoa et al., 2010). In our study, older age groups generally reported less functioning loss due to well-being-related barriers. The relationship among age, functioning, and well-being is complex and findings in the literature are generally mixed; however, aging is often associated with increased life satisfaction but decreased health-related quality of life (Hopman et al., 2000; Shmotkin, 1990).
Effect sizes indicated the strong magnitude of the relationship between the WBA-F and measures of health and well-being. Large effect sizes were observed for emotional health, physical health, overall health, and life evaluation constructs. Medium effect sizes were observed for measures of chronic conditions and health risks. These findings suggest that to minimize functioning loss, interventions need to enhance multiple domains of well-being, not just target health risk behaviors and chronic conditions.
This measure adds an extra dimension to the well-being literature by linking well-being domains with functioning loss in a general, nonmedical population of adults. It also offers an assessment strategy that can complement work-related productivity measures among unemployed or retired individuals. In addition, it could be used with employed individuals to compare how they are functioning at home versus how productive they are at work. It would be suitable as an intervention outcome measure for a study that aims to improve well-being and/or functioning in a variety of populations. This brief, 10-item, measure could help researchers, policy makers, or other groups to identify which domains of well-being are negatively impacting functioning at the individual, citizen, or group level.
Strengths of this study include the recruitment of a large national sample that was relatively diverse (in terms of age, gender, employment status, and SES). Limitations of this research include the use of a single cross-sectional study sample. Longitudinal research with various populations (e.g. retired, medical, and racially diverse) could build upon the findings of this study. In addition, future research could examine the effectiveness of health behavior and well-being interventions on functional well-being by including the WBA-F as an outcome measure.
Footnotes
Funding
This research received partial funding from Healthways, Inc.