
Abstract
We adopted an intersectionality framework and examined whether the relationship between internalized HIV stigma and depressive symptoms is moderated by internalized substance use stigma. A total of 85 people living with HIV with a history of substance use in the Bronx, New York, completed a survey. Results revealed evidence of moderation: Participants who internalized HIV stigma experienced greater depressive symptoms only if they also internalized substance use stigma. Researchers should examine stigma associated with multiple socially devalued characteristics to best understand how stigma impacts mental health among people living with HIV. Healthcare providers should address stigma associated with the full range of socially devalued characteristics with which people living with HIV live.
Introduction
A substantial body of evidence demonstrates that people living with HIV (PLWH) who have internalized HIV stigma are more likely to be depressed and experience depressive symptoms (Lee et al., 2002; Mak et al., 2007; Riggs et al., 2007; Simbayi et al., 2007). Internalized stigma involves endorsing negative feelings and beliefs associated with a socially devalued characteristic such as HIV and applying them to the self (Link, 1987). For example, PLWH who have internalized HIV stigma may feel “less than” others, and/or dirty or unclean because of their HIV status. In addition to internalizing stigma associated with HIV, PLWH may internalize stigma associated with other socially devalued characteristics such as a history of substance use; lesbian, gay, or bisexual orientation; minority race and/or ethnicity; sex work; and/or incarceration. In this study, we examine whether the relationship between internalized HIV stigma and depressive symptoms is moderated, or changed, by internalized substance use stigma. Findings may provide a stronger understanding of how internalized stigma relates to depressive symptoms among PLWH living with multiple socially devalued characteristics.
Recent theoretical work emphasizes the importance of adopting an intersectionality framework to best conceptualize how living with multiple socially devalued characteristics impacts the health of PLWH (Earnshaw et al., 2013a; Logie et al., 2011). An intersectionality framework suggests that socially devalued characteristics are often interdependent and may interact with each other to influence outcomes (Berger, 2004; Cole, 2009). Empirical work increasingly supports this perspective. Within a qualitative study, women living with HIV stressed the importance of attending to the effects of stigma associated with HIV, sex work, race, sexual orientation, and gender identity simultaneously (Logie et al., 2011). Results of quantitative studies demonstrate that analyses that examine enacted stigma (i.e. experiences of discrimination from others) associated with multiple socially devalued characteristics are better able to explain the impact of stigma on outcomes such as depression (Logie et al., 2013) and antiretroviral adherence (Bogart et al., 2010) than analyses that examine enacted stigma associated with just one characteristic. No known studies, however, have examined whether internalized HIV stigma interacts or intersects with internalized stigma associated with other socially devalued characteristics to impact depressive symptoms among PLWH.
We focus on internalized substance use stigma in the current investigation partly because many PLWH in the United States have a history of substance use. Approximately 7% of new HIV diagnoses and 12% of AIDS diagnoses in 2011 were among people who had engaged in injection drug use (Centers for Disease Control and Prevention, 2013). Many other PLWH have used noninjection substances such as crack cocaine (Edlin et al., 1994), methamphetamine (Patterson et al., 2005), and alcohol (Galvan et al., 2002). Additionally, people with a history of substance use report high levels of internalized substance use stigma (Luoma et al., 2007). Similar to internalized HIV stigma, internalized substance use stigma is associated with poor outcomes including worse mental health and less engagement in substance abuse treatment services (Luoma et al., 2007).
In this study, we aimed to explore intersectionality between internalized HIV stigma and internalized substance use stigma by examining whether the effect of internalized HIV stigma on depressive symptoms is moderated by internalized substance use stigma. We hypothesized that internalized substance use stigma worsens the impact of internalized HIV stigma on depressive symptoms among PLWH with a history of substance use.
Methods
Procedure and participants
Data were drawn from a study examining psychosocial determinants of retention in HIV medical care at a community clinic located in the Bronx, New York, conducted between August 2011 and March 2012. Members of the clinic staff introduced the study to patients, and those who were interested met with a trained interviewer to determine study eligibility. To be eligible, patients had to be HIV-positive, English- or Spanish-speaking, 18 years or older, and diagnosed with HIV more than 2 years prior to their participation date. The interviewer conducted in-person interviews with participants in a private space for approximately 60 minutes, and participants were remunerated US$15. All procedures had Institutional Review Board approval. A total of 101 patients participated in the study.
For the current investigation, analyses are limited to participants with a history of self-reported substance use. The World Health Organization’s Alcohol, Smoking and Substance Involvement Screening Test (ASSIST) was used to determine which participants had a history of substance use (Ali et al., 2002; Humeniuk et al., 2008). Participants who indicated that they had used illicit substances, misused prescription drugs, and/or used alcohol in the past 3 months are included. Past work suggests that substance use stigma lingers even after people have initiated recovery (Earnshaw et al., 2013b). Therefore, participants who indicated that they ever had a friend or relative who expressed concern regarding their use of substances and/or participants who indicated that they had ever tried and failed to control, cut down, or stop using substances are also included.
A total of 85 participants are included in this study, 63.5% of whom had received substance use treatment in the past. Participant characteristics reflected those of the clinic population. The average age was 48.96 (standard deviation (SD) = 9.39) years, and 55.3% were identified as male. Participants primarily identified as Latino(a) (55.3%) and/or Black (50.6%). One-third (32.9%) were born outside of the United States, and 21.2% identified as gay, lesbian, or bisexual. Most reported having a high school degree or more education (56.5%) and an annual income of less than US$10,000 (56.5%). Participants had been living with HIV for an average of 15.44 years (SD = 6.69 years).
Measures
Participants reported information regarding sociodemographics and completed measures of internalized stigma and depressive symptoms.
Internalized HIV and substance use stigma
Internalized HIV stigma and internalized substance use stigma were measured with the internalized stigma subscale of the HIV Stigma Mechanism Measure (Earnshaw et al., 2013c). The six items of the subscale were tailored to having HIV or having used substances. Example items include “Having HIV (used drugs/alcohol) makes me feel like I’m a bad person” and “I feel I’m not as good as others because I have HIV (used drugs/alcohol).” Responses were indicated on a scale ranging from strongly disagree (1) to strongly agree (5). Items were averaged to create composite scores (internalized HIV stigma: mean (SD) = 2.12 (0.88), α = 0.89; internalized substance use stigma: mean (SD) = 2.21 (0.90), α = 0.89).
There was a positive correlation between internalized HIV stigma and internalized substance use stigma (r = 0.27, p < .001) indicating that participants who reported greater internalized HIV stigma also reported greater internalized substance use stigma. The correlation was medium in effect size, however, supporting divergent validity between constructs.
Depressive symptoms
Depressive symptoms were measured with the 10-item Center for Epidemiological Studies Depression Scale (Irwin et al., 1999). Participants were asked whether they experienced 10 symptoms of depression such as feeling sad and having restless sleep in the past week. Responses included yes (1) or no (0), and items were summed (mean (SD) = 3.81 (2.26)).
Data analyses
We examined whether internalized substance use stigma moderated the relationship between internalized HIV stigma and depressive symptoms using multivariate linear regression analysis. Included in the analysis were the main effects of internalized HIV stigma and internalized substance use stigma and the interaction effect between internalized HIV stigma and internalized substance use stigma. Sociodemographic characteristics were excluded from the model because none were associated with depressive symptoms in preliminary bivariate analyses (ps > .10 for all correlations). Internalized HIV stigma and internalized substance use stigma were centered prior to analysis to prevent multicollinearity (Aiken and West, 1991). We used the PROCESS macro to probe the interaction with the pick-a-point approach described by Hayes and Matthes (2009).
Results
The regression analysis demonstrated a statistically significant interaction between internalized HIV stigma and internalized substance use stigma on depressive symptoms (B (standard error; SE) = 0.63 (0.22)), t = 2.86, p < .01). As shown in Figure 1, at low to moderate percentiles (i.e. 10th–75th) of substance use stigma, the association between internalized HIV stigma and depressive symptoms is not statistically significant. At the highest percentile (i.e. 90th) of substance use stigma, in contrast, the association between internalized HIV stigma and depressive symptoms is statistically significant (B (SE) = 0.73 (0.32), t = 2.25, p = .03). Namely, there is a positive association between internalized HIV stigma and depressive symptoms only among participants at the highest percentile of internalized substance use stigma.
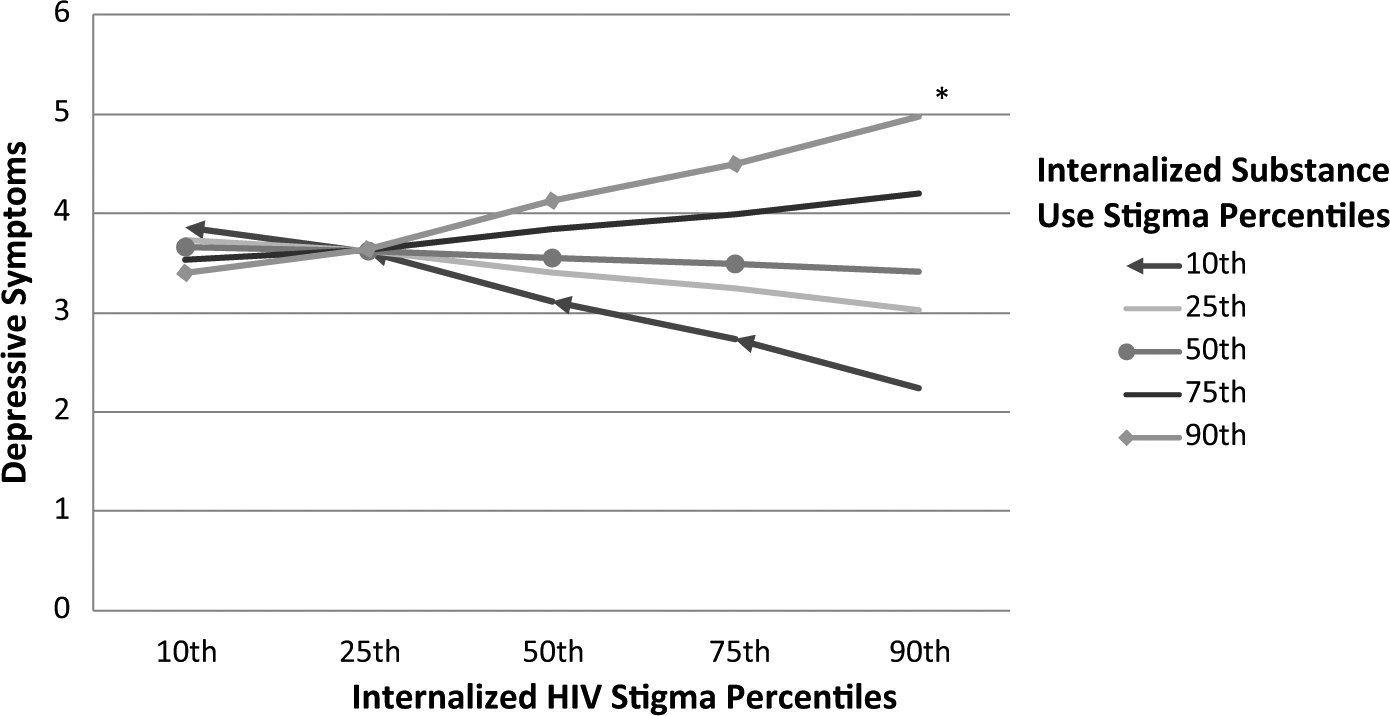
Line graph representing interaction between internalized HIV stigma and internalized substance use stigma on depressive symptoms.
Discussion
Results of this study contribute to a stronger understanding of the association between internalized stigma and depressive symptoms among PLWH with a history of substance use. Internalized substance use stigma moderated the association between internalized HIV stigma and depressive symptoms: Participants who internalized HIV stigma experienced greater depressive symptoms only if they had also internalized substance use stigma. Results suggest that the combination of internalized HIV stigma and internalized substance use stigma may be particularly damaging to the mental health of PLWH.
There are several limitations of this study that future work may expand on. The study was cross-sectional, limiting our ability to form conclusions about whether internalized stigma predicts subsequent depressive symptoms. Future work might employ longitudinal methodology to examine whether internalized stigma predicts depressive symptoms over time. Furthermore, our sample size was small and limited to PLWH with a history of substance use attending a community clinic in the Bronx, New York. Future work should examine whether these results replicate among larger, more diverse samples to test the generalizability of these effects. Relatedly, our sample comprised participants reporting a wide range of substance use, extending from illicit drug use to alcohol use. This allowed us to capture a wide range of internalized substance use stigma. Future work, however, may choose to focus more exclusively on samples with histories of illicit drug use among whom internalized substance use stigma may be stronger. Many of the participants of this study lived with multiple socially devalued characteristics such as minority sexual orientation and/or race/ethnicity. However, we only examined the effects of internalized stigma associated with HIV and substance use. Future work might also examine the effects of internalized stigma associated with lesbian, gay, or bisexual orientation; race/ethnicity; sex work; incarceration; gender; socioeconomic status; and other socially devalued characteristics prevalent in HIV-positive populations.
This work further highlights several other avenues of future research. Results suggest that people who internalize stigma associated with both HIV and substance use are particularly at risk of experiencing depressive symptoms. Future research may focus on this group of people to examine whether they differ from people who do not internalize stigma or people who only internalize stigma associated with one characteristic. People who internalize stigma associated with both characteristics may, for example, also experience high levels of shame in general. Additionally, results suggest that studying stigma associated with multiple characteristics may provide a fuller understanding of the extent to which stigma impacts health outcomes among PLWH. Future research should seek to adopt an intersectionality framework by examining stigma associated with multiple socially devalued characteristics to best understand how stigma impacts health outcomes among PLWH. It is important that researchers continue developing measures of stigma associated with multiple socially devalued characteristics as well as stigma intersectionality to achieve this goal within quantitative work. Finally, although this study focused on intersectionality associated with internalized stigma given evidence of its strong associations with depressive symptoms (Lee et al., 2002; Mak et al., 2007; Simbayi et al., 2007), future research may also examine other stigma mechanisms such as enacted stigma (i.e. experiences of discrimination in the past) and anticipated stigma (i.e. expectations of discrimination in the future). Different stigma mechanisms are associated with different health outcomes among PLWH (Earnshaw et al., 2013c), and therefore, such research may provide a greater breadth of understanding of the impact of stigma on the health of PLWH.
This study has significant implications for clinical practice with PLWH. Healthcare providers might address internalized stigma associated with both HIV and other characteristics among patients living with HIV when intervening to reduce depressive symptoms. Acceptance and Commitment Therapy represents a promising intervention to reduce internalized stigma among people with a history of substance use that may be adapted for PLWH (Luoma et al., 2008). This therapy incorporates aspects of psychological acceptance, cognitive diffusion, mindfulness, value exploration, and human connection. Participants of a pilot study who completed at least 4 hours of Acceptance and Commitment Therapy demonstrated decreased internalized stigma and internalized shame (Luoma et al., 2008). Interventions that incorporate spiritual striving, disengagement coping, acceptance coping, and social sharing of emotion may also be successful in reducing internalized stigma (Cantisano et al., 2012; Gonzalez et al., 2009; Hansen et al., 2013; Perez et al., 2009). Beyond intervening among PLWH to reduce internalized stigma, it is critical to develop strategies to eliminate stigma at the societal level (Campbell et al., 2007). Only by eradicating societal stigma will we prevent individuals from internalizing stigma and ensure that stigma ceases to pose a threat to the health of PLWH.
Footnotes
Acknowledgements
The authors thank the participants as well as HIV care providers and clinic staff for their support of and contributions to this project.
Declaration of conflicting interests
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or the Center for Health Intervention and Prevention.
Funding
A seed grant from the University of Connecticut Center for Health Intervention and Prevention partly funded this work. Grants from the National Institutes of Health funded Earnshaw’s (T32MH020031), Smith’s (F31MH093264), Cunningham’s (R25DA023021), and Copenhaver’s (K02DA033139) efforts.