
Abstract
This study examined the association between propensity for emotional rehearsal, body image self-perception and weight status in Chinese Hong Kong pre-adolescents. Children 8–12 years of age (n = 278) completed measurement of body mass index, body image and emotional rehearsal. Multinomial regression analyses revealed that body mass index was positively associated with body image dissatisfaction and a significant predictor of body size estimation. However, only body size underestimation was associated with lower rehearsal tendencies. The prevalence of body image dissatisfaction and body size estimation was also reported for this population. Future research is suggested for greater understanding of emotional coping in body image dissatisfaction in young children.
Introduction
Body image dissatisfaction is characterized by negative self-appraisal of one’s body and is often accompanied by body size misperception (in terms of underestimation or overestimation of one’s actual body size); both are common in overweight and normal weight children (Evans et al., 2013; Skrzypek et al., 2001). While the majority of research has focused on body image dissatisfaction in eating disorders, increasing evidence points to the importance of considering body size misperception separately as the latter appeared to have different neuronal orientations to eating disorders and that it may mediate the relationship between body image dissatisfaction and eating disorders (Mohr et al., 2008, 2011; Mussap et al., 2008) Specifically, body image dissatisfaction elicited from body size overestimation (i.e. the perception of being bigger than actual body size) is linked to anorexia nervosa, bulimia nervosa and binge-eating disorder (Castellini et al., 2012; Mond et al., 2007; Mussap et al., 2008), whereas body size underestimation (i.e. the perception of being smaller than actual body size) is associated with overweight/obesity (Edwards et al., 2010). The above evidence suggests that body image dissatisfaction and body size misperception are likely to manifest in disordered eating behaviours which could potentially be carried into adulthood (Stice et al., 2012).
Recently, researchers have proposed the possible role of rumination (i.e. the propensity to recurrently focus on symptoms of distress and their possible causes and consequences) as a psychological mechanism for body image dissatisfaction, body size misperception and related eating pathologies, as well as their prolongation. For instance, rumination was among other emotion regulation strategies that appeared to moderate the relationship between body image concerns and bulimic symptoms in adolescent girls (Hughes and Gullone, 2011). Longitudinally, rumination was found to be a predictor of increased eating pathology in 7 months, and a reciprocal relationship between rumination and bulimic and depressive symptoms was evident in a 4-year period (McLaughlin et al., 2011; Nolen-Hoeksema et al., 2007). Additionally, Holm-Denoma and Hankin (2010) showed that high ruminative adolescent girls with low physical appearance competence were more likely to develop bulimic symptoms in 10 weeks than those with high physical appearance competence. The above research has provided partial support for rumination being a potential psychological mechanism for feeding one’s negative body image perception, which may have contributed to the exacerbation of eating pathologies. Essentially, the greater propensity to focus on adverse experiences and thoughts may reinforce the psychological stress and negative emotions generated from the unattained ideal body image (Clark, 1996; Klinger, 1996; Martin and Tesser, 1996; Wegner, 1994). In an attempt to distract or to relieve from the intensity of the psychological disturbances, maladaptive behaviours such as disordered eating may result (Heatherton and Baumeister, 1991; Rawal et al., 2010; Selby et al., 2008). While most body image research in the role of rumination has been conducted with adolescents, little is known about the psychological mechanisms contributing to a disturbed body image in pre-adolescents despite growing evidence on body image dissatisfaction and body size misperception in this age group (Gardner et al., 1999). Nonetheless, research on emotional rehearsal, a form of generic rumination, may shed some light on the how rumination may also be a mechanism behind body image dissatisfaction in young children.
Emotional rehearsal refers to the tendency to have repetitive emotional thoughts about upsetting experiences from the past, present or possibly in the future (Roger and Nesshoever, 1987). Emotional rehearsal has been linked to psychological stress in adults where abnormal physiological response, that is, notable cortisol increase or slower heart rate recovery, was noted in high rehearsers compared to low rehearsers (Roger and Jamieson, 1988; Roger and Najarian, 1998). Based on the above evidence, Ling et al. (2011) argued that their findings on the association between rehearsal tendencies and excess adiposity in Chinese children could potentially be explained by physiological, psychosocial and/or behavioural factors that are stress-related. It is possible that bigger children, who seemed more likely to possess a higher rehearsal tendencies, might be more prone to misperception of their body size and/or that they might be more dissatisfied with their current perceived body size which could be a regular source of stress as reinforced by their constant focus on it. It is also possible that the recurrent negative emotions associated with their unattained ideal body image may cause adiposity through the psychoendocrinological or the behavioural pathway. Both explanations denote the possible link between high rehearsal tendencies in childhood and body size dissatisfaction and misperceived body size estimation, which are evident to be a source of anxiety for children across different cultures (Hillman et al., 2010; Tang et al., 2010), yet their relationships have not been investigated.
In view of the above, we examined the association between rehearsal, body size satisfaction, body size estimation and weight status in Chinese pre-adolescents. With thinner body image ideals common in this age group (Kelly et al., 2011), we hypothesized that children with higher body mass index (BMI) and greater rehearsal tendencies were more likely (a) to be dissatisfied with their body image and (b) to overestimate their body size. The body image of Hong Kong Chinese children has been under-studied despite some evidence of body image disturbance in Chinese (see Soh et al., 2006). Therefore, another aim of this study was to examine the prevalence of body image dissatisfaction and body size misperception in Hong Kong children. The findings have potential to be clinically valuable as Asian youth are showing a secular increase in adiposity, which is leading to increasing cardiovascular disease risks (Lam et al., 2010; Xanthopoulos et al., 2011). Furthermore, with previous body image interventions demonstrating limited success (McCabe et al., 2006), our results can potentially inform the design of future interventions that may achieve greater sustainable effectiveness in alleviating body image disturbance in young children.
Methods
Participants
Parental consent was obtained from 278 children in Grade 4–6, representing approximately 77.2% of the three year groups, from a local government aided school in the southern district of Hong Kong. Assented participants were 8–12 years of age (mean age = 10.79 ± .81 years; 50% boys), and all completed the measures detailed below.
Procedure
Parental consent and detailed information about the study were sent to all parents of students in Grade 4–6 through the participating school. The researchers’ contact details were provided on the information sheet and parents were encouraged to contact the researchers for any questions regarding the study. Completed parental consent and student assent were returned to the school in a sealed envelope which was then passed onto the research team. Under the arrangement of the school, all assented participants completed the two questionnaires, the Rehearsal Scale for Children–Chinese (RSC-C) first, followed by the Children’s Body Image Scale (CBIS), before having their anthropometric measurements taken in one morning of a normal school day. All the measures and protocols were approved by the Institutional Review Board for Human Ethics.
Measurements
Anthropometry
Stature and body mass were measured barefoot to the nearest 0.1 cm and 0.1 kg, respectively. For stature, a fixed stadiometer (Invicta 2007246, UK) was used and an electronic scale (Tanita TBF-410, Japan) was used for measuring body mass.
CBIS
The CBIS was designed to assess the self-perceived current and ideal body image in 7- to 12-year-old children (Truby and Paxton, 2002). The gender-specific scale consists of seven child figures, each representing a BMI range within the 3rd to 97th percentile (Hamill et al., 1979). The scale is presented in ascending order, with the corresponding BMI range for boys for each percentile range on the scale (with a category number assigned to each child figure) as (1) 14.0–14.6 (3rd percentile), (2) 14.7–15.5 (10th percentile), (3) 15.6–16.5 (25th percentile), (4) 16.6–18.5 (50th percentile), (5) 18.6–24.9 (75th percentile), (6) 25.0–28.4 (90th percentile) and (7) 28.5–29.0 (97th percentile), whereas for girls it was (1) 13.0–13.5 (3rd percentile), (2) 13.6–14.9 (10th percentile), (3) 15.0–16.6 (25th percentile), (4) 16.7–17.7 (50th percentile), (5) 17.8–19.4 (75th percentile), (6) 19.5–24.6 (90th percentile) and (7) 24.7–28.5 (97th percentile). Prior to their anthropometric measurements, participants were asked to indicate the child figure that best represented their current body size (i.e. their perceived body size) and their ideal body size. The questions were translated/back-translated from English to Chinese. The CBIS has shown good construct validity and test–retest reliability (r = .76 and .85 for boys and girls, respectively) (Truby and Paxton, 2008).
Based on the category number assigned to each CBIS child figure, body size satisfaction was assessed by computing the difference between participants’ perceived body size and their ratings of their ideal body size (i.e. ‘perceived minus ideal’). Directional interpretation was completed on the basis of whether the difference was negative or positive. For example, a child wanting a ‘thinner’ body size would score positively, whereas a child wanting to be ‘bigger’ would score negatively.
For body size estimation, the actual BMI of each participant was categorized into one of the seven CBIS child figures. Participants’ body size estimation was categorized by grouping the data into ‘accurate estimation’ (when the category number for the perceived size was the same as that for the actual size), ‘underestimation’ (when the category number for the perceived size was lower than that for the actual size) and ‘overestimation’ (when the category number for the perceived size was higher than that for the actual size).
RSC-C
The RSC-C measures the propensity to rehearse and has been validated in 6- to 12-year-old Chinese children (Ling et al., 2010). The 13-item scale possesses high internal validity (α = .83) and satisfactory test–retest reliability within 1 year (r = .43). Each item is rated on a 4-point Likert scale from ‘never’ to ‘all the time’. Example items are ‘If I lose out, I get over it quickly’ and ‘I find myself thinking over and over about things that have made me angry.’ All participants completed the RSC-C before having their anthropometric measurements taken.
Statistical analyses
Descriptive data are presented as means and standard deviations (SDs) (mean ± SD). Two forced entry multinomial logistic regression models were computed with body size satisfaction (classified as ‘bigger’, ‘thinner’ or ‘same’, with ‘same’ as the reference category) (model 1) and body size estimation (classified as ‘overestimation’, ‘underestimation’ or ‘accurate estimation’, with ‘accurate estimation’ as the reference category) (model 2) as the respective dependent variables. Gender and body size estimation (for model 1) or body size satisfaction (for model 2) were entered as the predicting variables, whereas the continuous variables, BMI and rehearsal, were entered as covariates. A p value of <.05 was set a priori for all analyses.
Results
Perceived and ideal body size ratings, alongside actual body size, are provided in Table 1. Mean BMI was 18.52 ± 3.44 (ranging between 12.98 and 33.88). Most boys’ actual body size fell under the 75th percentile for BMI (category 5) and most of their perceived and ideal body size fell under the 25th percentile (category 3). Most girls’ actual body size, perceived and ideal body size fell under the 25th percentile for BMI (category 3).
Percentage of boys and girls in the actual, perceived and ideal CBIS category.
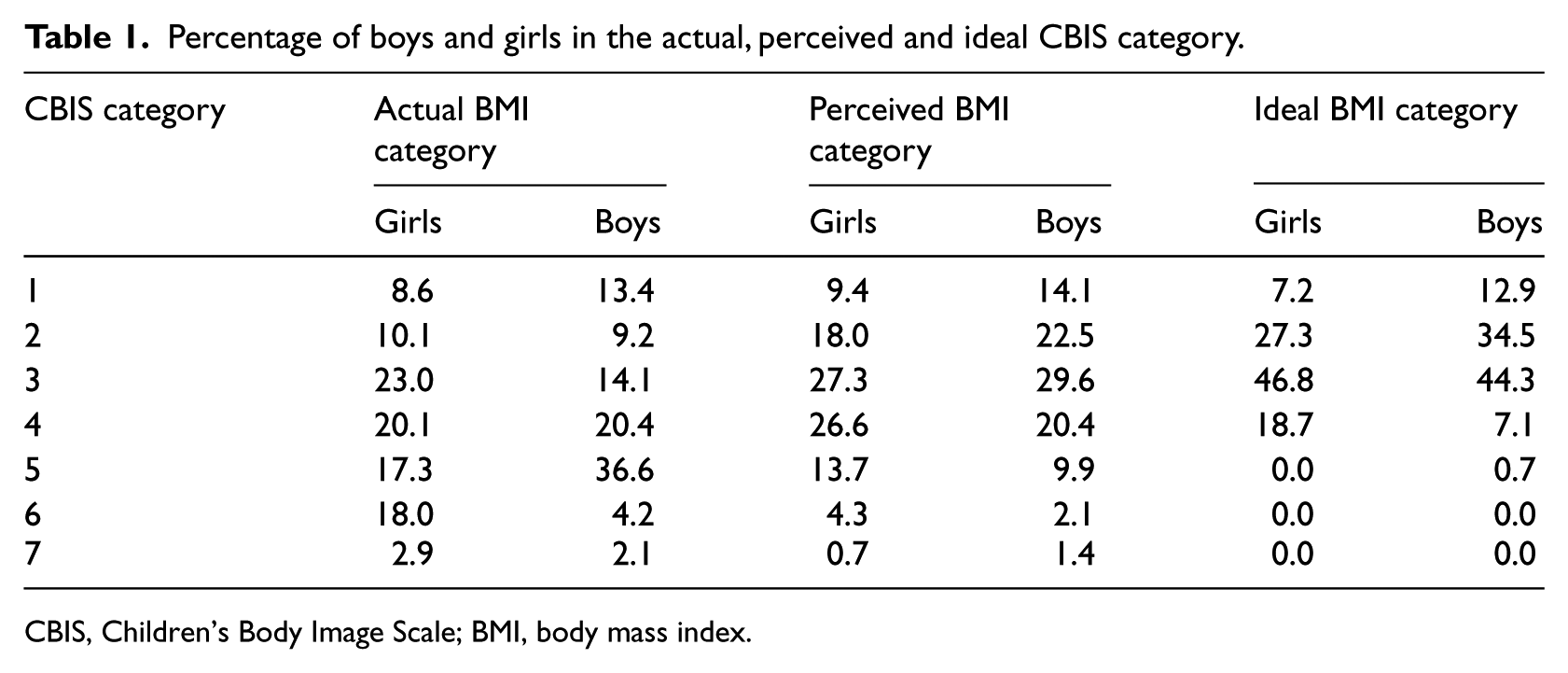
CBIS, Children’s Body Image Scale; BMI, body mass index.
As for the perceived and ideal body size ratings by gender, only 27% of boys and 26% of girls wanted to maintain their current body size, suggesting that the majority were dissatisfied with their body image. Forty-eight per cent of the boys and 55% of the girls preferred to be thinner, while 25% of the boys and 19% of the girls preferred to be bigger. Fifty-eight per cent of the boys and 53% of the girls underestimated their size, whereas 17% of the boys and 19% of the girls overestimated their actual body size.
Results of the regression analysis for body image satisfaction (model 1) and body size estimation (model 2) are presented in Table 2. For body image satisfaction (model 1), desire for a ‘bigger’ body size was predicted by lower BMI (β = −.26, p < .05; adjusted odds ratio (OR): .77; 95% confidence interval (CI): .61, .98). Preferring a ‘thinner’ body size was predicted by higher BMI (β = .65, p < .01; adjusted OR: 1.91; 95% CI: 1.56, 2.34), an underestimation (β = 1.57, p < .01; adjusted OR: 4.80; 95% CI: 1.91, 12.03) and an overestimation of body size (β = 2.40, p < .01; adjusted OR: 11.06; 95% CI: 2.69, 45.50). However, neither propensity for rehearsal nor gender was a significant predictor of body size satisfaction. Approximately 38% of the variance was explained by the model.
Multinomial regression analysis results for predictors of body image satisfaction (model 1) and body size estimation (model 2).

RSC-C: Rehearsal Scale for Children–Chinese; BMI: body mass index; OR: odds ratio; CI: confidence interval.
p < .05, **p < .01.
For model 2, body size overestimation was predicted by lower BMI (β = −.48, p < .01; adjusted OR: .62; 95% CI: .46, .83) and body size underestimation was predicted by higher BMI (β = .32, p < .01; adjusted OR: 1.37; 95% CI: 1.20, 1.57). Moreover, children who underestimated their body size were likely to prefer either a bigger body size (β = 1.15, p < .01; adjusted OR: 3.15; 95% CI: 1.32, 7.54) or a smaller body size (β = .99, p < .05; adjusted OR: 2.70; 95% CI: 1.25, 5.85). Underestimation of body size was also associated with lower rehearsal tendencies (β = −.06, p < .05; adjusted OR: .94; 95% CI: .90, .99). Again, no gender differences were found. Approximately 23% of the variance was explained by the model.
Discussion
To the best of our knowledge, this study is the first to explore body size satisfaction, body size estimation and the propensity for rehearsal in Hong Kong Chinese children. Our results are generally consistent with previous research with the non-clinical children population in that weight status is inversely related to the desired body size and children with a lower BMI were more likely to overestimate their body size and the reverse applies to those with a higher BMI (Kostanski et al., 2004; Kurth and Ellert, 2010). However, contrary to our expectations, propensity for rehearsal was not related to body size satisfaction. Our results show that underestimation of body size was associated with a lower propensity for rehearsal and a higher BMI. This suggests that bigger children may tend to incorrectly perceive themselves as thinner than they are, which may somewhat prevent them from rehearsing about their body size. Alternatively, children with a low propensity for rehearsal may perceive themselves as thinner than they are, and consequently, they might be at greater risk for neglecting their actual body size. The latter could become a health issue if a developmental trend of cardiovascular disease risks is already observed in a child. It is possible that psychological self-regulatory mechanisms other than rehearsal, such as avoidance, are involved in the relationship between weight status and body size overestimation (Schmidt and Treasure, 2006; Wendell et al., 2012) and possibly in body image dissatisfaction too (Hughes and Gullone, 2011; McLaughlin et al., 2011). In other words, even for a child who may possess a higher tendency to rehearse about his or her body size, the tendency for him or her to avoid addressing these recurrent negative thoughts may moderate the level of dissatisfaction or overestimation towards it. It is also possible that rehearsal does not play as an important role in Chinese children as in their Western counterparts as empirical evidence suggests that Chinese children’s ideal body image is less extreme relative to their actual body size and obesity seemed to be more acceptable due to the Chinese cultural values (Marsh et al., 2007), thus making a bigger body size, and/or the perception of it, less undesirable and hence less likely to fuel the negative thoughts of it. Nonetheless, and crucially, our findings may suggest that Chinese children’s underestimation of their body size could potentially contribute to the upward trend of childhood obesity in Hong Kong. If children are simply unaware that they are becoming overweight, and continue to perceive themselves as smaller than they actually are, excessive weight gain may occur unabated.
As for the prevalence of body image dissatisfaction and body size estimation, all results appear to be comparable between boys and girls suggesting that gender differences might not be as prominent for the Chinese children as for children from other cultures (Xanthopoulos et al., 2011). Nevertheless, future studies using similar measurements of body size satisfaction and estimation are called for to ascertain this observation.
Several limitations of this study need addressing. Our relatively small sample size limits insight into potential age effects, but age should be considered in future studies given previous research has suggested that there are changes in body image disturbances across childhood (Gardner et al., 1999). In addition, the CBIS was not developed in Chinese children; however, each photo used in the CBIS corresponds to a known BMI percentile range, originally based on the National Center for Health Statistics (NCHS) 1979 reference data (ranging from the 3rd to the 97th percentile) (Hamill et al., 1979), but recently mapped onto the International Obesity Task Force (IOTF) standards, which includes data for Hong Kong Chinese children (Cole et al., 2000). The use of the CBIS could be further improved if the figures are presented randomly to avoid potential response bias (see Gardner and Brown, 2010).
To conclude, body image dissatisfaction and misperception can have serious clinical implications for the development of eating pathologies and maladaptive health behaviours, and it is possible that there are weight gain consequences for bigger children who incorrectly perceive themselves as thinner than they are. More research is warranted into the possible psychological mechanisms that create body image disturbances in childhood, particularly in young boys as they seem to be less studied than girls despite that the prevalence of body image dissatisfaction is comparable between the sexes. Educational and health professionals are also strongly encouraged to promote a better understanding of body image perception in young children both at schools and within the community.
Footnotes
Acknowledgements
The authors are grateful to the University of Hong Kong Research Council Strategic Research Theme Public Health for supporting this project and Tsang Fan Pong for his technical support.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.