
Abstract
The aim of the study was to test whether a screening navigation program leads to more favorable health beliefs and decreases social inequalities in them. The selected 261 noncompliant participants in a screening navigation versus a usual screening program arm had to respond to health belief measures inspired by the Protection Motivation Theory. Regression analyses showed that social inequalities in perceived efficacy of screening, favorable attitude, and perceived facility were reduced in the screening navigation compared to the usual screening program. These results highlight the importance of health beliefs to understand the mechanism of screening navigation programs in reducing social inequalities.
Keywords
Introduction
Colorectal cancer is the third most common cancer and the second cause of mortality by cancer in France (Institut National du Cancer (INCa)). 1 Because treatment efficacy is better if colorectal cancer is detected at an early stage, screening is considered a major means of improving the prognosis of this cancer. In France, screening takes place via a national organized screening program, which invites people to consult their general practitioner (GP). GPs are in charge of evaluating individual risks and encouraging the use of fecal occult blood testing (FOBT) for people aged between 50 and 74 years with an average risk of cancer. However, despite this national program in France, as in similar western countries, screening participation is still low and unequal, and depends on socioeconomic status (Champion et al., 2016; Frederiksen et al., 2010; Javanparast et al., 2010). For instance, screening participation is higher for people living in a privileged geographical area than in a deprived geographical area (Pornet et al., 2010).
In response to the need to reduce social inequalities, there are various levels of intervention for health policy-making according to the main sources of influences on health being considered. These range from general socioeconomic, cultural, and environmental conditions to individual factors (Dahlgren and Whitehead, 1991). Regarding screening, the major factors associated with low adhesion can be organizational (e.g. national recommendations for testing, insurance coverage system, provider-related variables) and individual (e.g. demographic variables, health-related behaviors, social support, stress, life difficulties, temporal orientation, language, medical mistrust, defense strategies, religiosity; Berkowitz et al., 2008; Cokkinides et al., 2003; McQueen et al., 2014; Power et al., 2008; Vernon, 1997; Wee et al., 2005). Based on an individual approach, a growing literature has pointed to the effectiveness of screening navigation programs (SNPs) in decreasing social inequalities (Lasser et al., 2011; Paskett et al., 2011; Percac-Lima et al., 2009; Wells et al., 2008). In a pro-active way, SNPs have aimed to identify and remove the remaining individual barriers to screening (Dejardin et al., 2011; Freund et al., 2008). These barriers can be logistical (e.g. transportation or financial issues, lack of discussion of screening with GPs) or linked to individual knowledge, emotions, and beliefs (e.g. need for information, explanation of the screening efficacy, and need for reassurance). SNPs have mostly been developed in the United States, while, to our knowledge, no program has been carried out in France.
In this work, the mechanisms of action of a French screening navigation were investigated. The study focused especially on perceptions about screening and colorectal cancer, that is to say health beliefs, which have previously been shown to be linked to screening participation (Gorin, 2005; Janz et al., 2003; Kiviniemi, 2011; Stanley et al., 2013) and socioeconomic status (Wardle et al., 2004; Whitaker et al., 2011). Given that SNPs act against barriers such as knowledge, emotions, and beliefs, they should lead to greater adhesion to health beliefs encouraging screening participation (e.g. perceiving oneself more vulnerable, perceiving screening as more effective). The theoretical framework of the Protection Motivation Theory—originally developed to explain fear appeal processes leading to the motivation to adopt protective behavior (Floyd et al., 2000; Rogers, 1983)—assumes that two processes lead to the motivation to protection: threat-appraisal and coping-appraisal. More specifically, the threat-appraisal component refers to the perceived severity of cancer and the perceived vulnerability of having cancer. Severity and vulnerability could increase the likelihood of adopting the recommended behavior. The coping-appraisal component refers to the ability to cope by adopting the recommended response, here the screening. It comprises beliefs in the response efficacy, in self-efficacy, which increases the likelihood of adopting the recommended behavior, and in the costs that decrease this likelihood. All of these components, which are known to motivate people to protection, were assumed to be influenced by screening navigation (SN).
To our knowledge, no previous study has tested the impact of an SNP on health beliefs. Assessing health beliefs is a promising way to (1) evaluate a secondary outcome of the effectiveness of an SNP that may influence further screening adherence and reduce social inequalities and (2) provide a better understanding of the mechanisms of SNP action, thus consolidating them. The research aimed to test whether SNPs (1) lead noncompliant people to adopt more health beliefs encouraging them to screen and (2) decrease social inequalities in health beliefs.
Method
Participants
Data were obtained from a larger study in France, a cluster randomized trial, stratified by the characteristics of the geographical unit where participants live, and comparing SN and usual screening program (USP) arms (http://clinicaltrials.gov website ID: NCT01555450). The whole study was conducted in accordance with French law (Council for the Protection of Individuals, Advisory Council for Health Research Information, and Data Protection Authority) and with the ethical principles of the Declaration of Helsinki of 1964 revised in Seoul in 2008.
Participants were those who (1) were eligible for the whole study, (2) were eligible to receive a questionnaire, and (3) returned a filled out questionnaire. First, participants selected for the whole study were those (1) eligible for the FOBT (e.g. aged between 50 and 74 years, not suffering from cancer) and (2) with a known address in the geographical units selected. Second, questionnaires were sent to participants (1) included in the study during a defined period of 6 months within the study, (2) with an available phone number, (3) with no regular screening adherence, and (4) from them, only the 2216 participants were retained who had no previous screening adherence and who had been targeted by a previous campaign encouraging them to participate (excluding primo-participants), in order to study noncompliant participants. Third, as self-report measures were of interest, responses to the questionnaire were considered.
Of the 2216 questionnaires received by participants, 267 were returned. Among these, data from six participants were deleted because dissimilarities (e.g. gender, age) were detected between the self-report data and those collected by the screening management structures. Thus, the sample was constituted of 261 participants who filled at least in part the total questionnaire. There are various possible reasons for the nonparticipation, for instance, the questionnaire length may have discouraged some participants from responding. Moreover, because the questionnaire was sent to a large variety of people selected at random, perhaps some were not willing to respond to a questionnaire, or had no time or other external conditions. It is also possible that people who did not respond did not feel concerned by the screening, and thus by the questionnaire, especially given the large proportion of nonparticipation in screening among the nonselected sample.
Differences between the sample of the 261 responders and the remaining 1955 nonresponders were analyzed and are presented in section “Results.”
Material
Postal address was used to determine a geographical unit for each participant: the IRIS (Ilots Regroupés pour des Indicateurs Statistiques; in French, the smallest geographical area with available statistical information). The IRIS were then stratified into their rurality, determined on the basis of the population size of IRIS reference towns, and socioeconomic status. Socioeconomic status was measured by the Townsend Index (Townsend, 1987) assessing deprivation at a geographical level, with a higher positive score meaning a more deprived IRIS. This measure enabled people to be targeted based on information about their socioeconomic status, which was available for all the population selected for the screening program, even in the absence of available individual information.
Inspired by the general theoretical framework and models based on the Protection Motivation Theory, components measured by one to several items, relevant in assessing health beliefs (Boer and Seydel, 1996; Milne et al., 2002; Rogers, 1983; Weinstein, 1993), were extracted from a larger questionnaire. Thus, threat-appraisal: perceived severity and perceived vulnerability; problem-solving/screening appraisal: perceived costs, perceived facility (i.e. evaluation that screening was perceived as feasible by the respondent, similarly to self-efficacy), and three measures of perceived efficacy were measured. Moreover, more general measures were added about the value accorded to colorectal cancer screening: overall favorable attitude and the fact that screening is not a priority among other preoccupations. Details are given in Appendix 1.
For each item, the response was given on a 5-point scale from 1 to 5. Beliefs were considered favorable, that is to say as having an effect of encouraging screening, when scores were high for severity, vulnerability, perceived facility, perceived efficacy, and favorable attitude and low for perceived costs and not a priority.
Procedure
The SN arm, receiving the action of the screening navigator, was distinguished from the USP arm, benefiting only from the national organized screening program. Screening management structures sent an invitation letter, followed by a reminder letter in the case of no adherence, and finally the test was sent 1 year after the first invitation letter in the case of no adherence. The main actions of the three screening navigators were to identify individual barriers to screening and to inform participants about screening and discuss it with them in order to suppress these barriers. The intervention began with a letter (for six participants the intervention was only this letter) and then screening navigators contacted each person by telephone. The questionnaires were sent at least 9 months after the invitation letter by screening management structures for each arm.
Statistical analyses
First, the characteristics of participants were analyzed and compared to those of the nonselected participants in order to evaluate the specificity of the respondents. Because of the hierarchical structure of the data with 67 IRIS including the 261 participants, multilevel analyses were conducted. First, using empty models (intercept-only model), the difference between considering intercepts at random and fixed was tested. No significant differences (p > 0.30) were found when the difference of the −2 log-likelihood value between the two models was tested with a restricted iterative generalized least squares estimation method. Because of these nonsignificant effects and for more simplicity, data were treated with multiple regression analyses. For each regression (one for each belief measure as the outcome variable to be predicted), the following predictors were introduced: SNP (−1 = USP vs 1 = SN), standardized Deprivation Index, 2 and the interaction between both these variables. Moreover, analyses were carried out to test the simple effect of Deprivation for USP (0 = USP vs 1 = SN) and for SN (−1 = USP vs 0 = SN). Finally, complementary analyses were conducted that were adjusted regressions for age, gender, the geographical unit rurality, living alone or not, and whether the GP had given information about colorectal cancer screening.
Using the Stevens (1984) criterion, Studentized deleted residual outliers higher than the 3.73 absolute value were examined and deleted for each analysis. Statistical Package for the Social Sciences (SPSS) version 21 statistical software was used to analyze data.
Results
Participant characteristics
The participant characteristics of the selected and nonselected samples are reported in Table 1.
Participant characteristics.
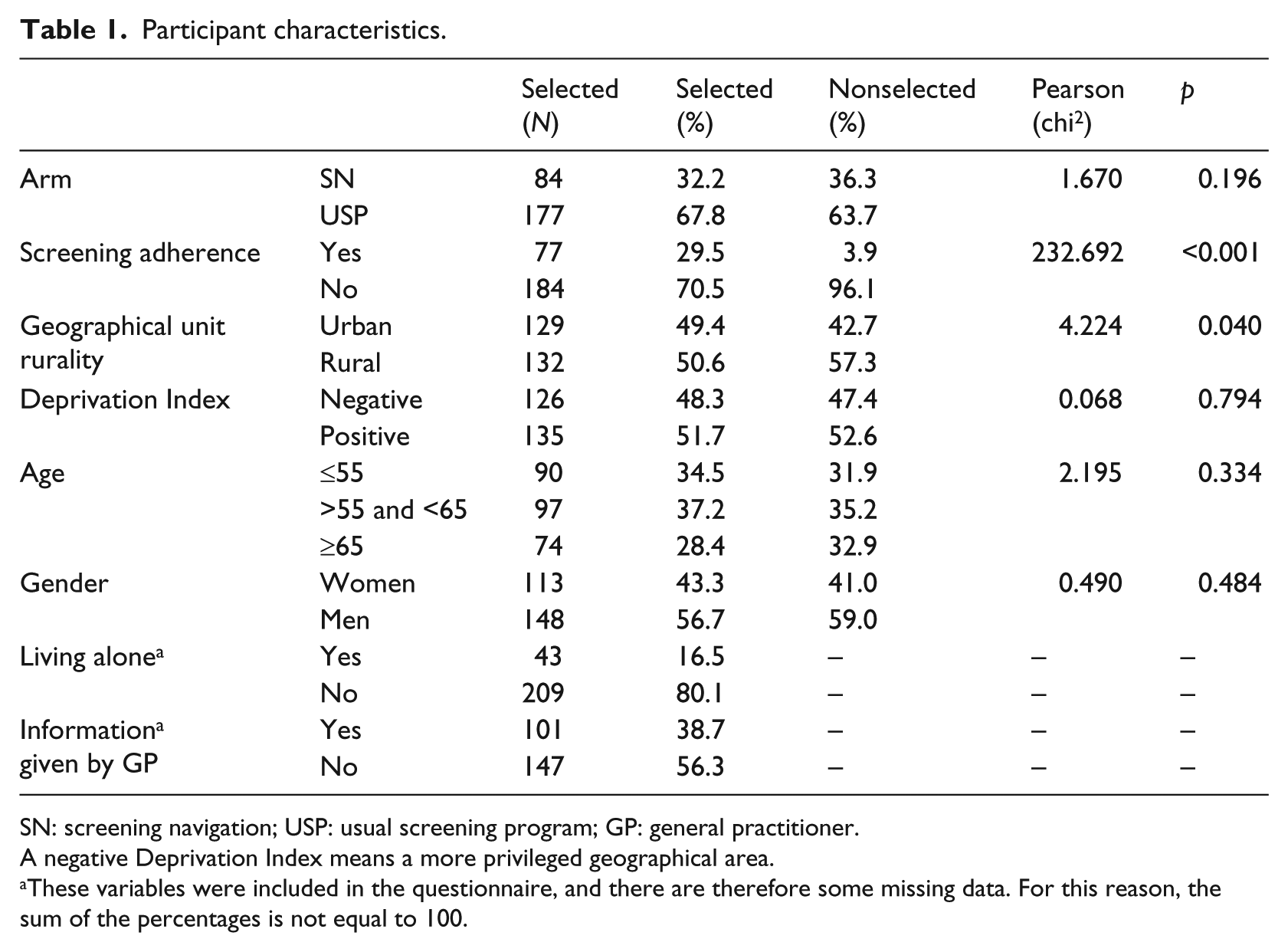
SN: screening navigation; USP: usual screening program; GP: general practitioner.
A negative Deprivation Index means a more privileged geographical area.
These variables were included in the questionnaire, and there are therefore some missing data. For this reason, the sum of the percentages is not equal to 100.
The selected sample was not exactly the same as the nonselected one, in particular because the former were mostly those who adhered to screening and those who lived in urban places.
Effect of SN and Deprivation Index on health beliefs
The results are presented in detail in Table 2. They showed no significant main effect of SN on any beliefs. However, they did show significant interactions between SN and the Deprivation Index (see Figure 1) on the efficacy of the screening test to detect colorectal cancer, the efficacy of the screening to reduce colorectal cancer consequences, overall favorable attitude, and tendentially on perceived facility. These interaction effects were characterized by simple effects of the Deprivation Index in the USP arm but nonsignificant simple effects of the Deprivation Index in the SN arm, except for attitude where no simple effect was significant. These effects mean that people living in a more privileged place (i.e. with a lower Deprivation Index) had more favorable beliefs than those living in a more deprived IRIS and that this social inequality was reduced by the SN intervention.
Results from regression analyses testing the effects of screening navigation program, deprivation, and their interaction on health beliefs.
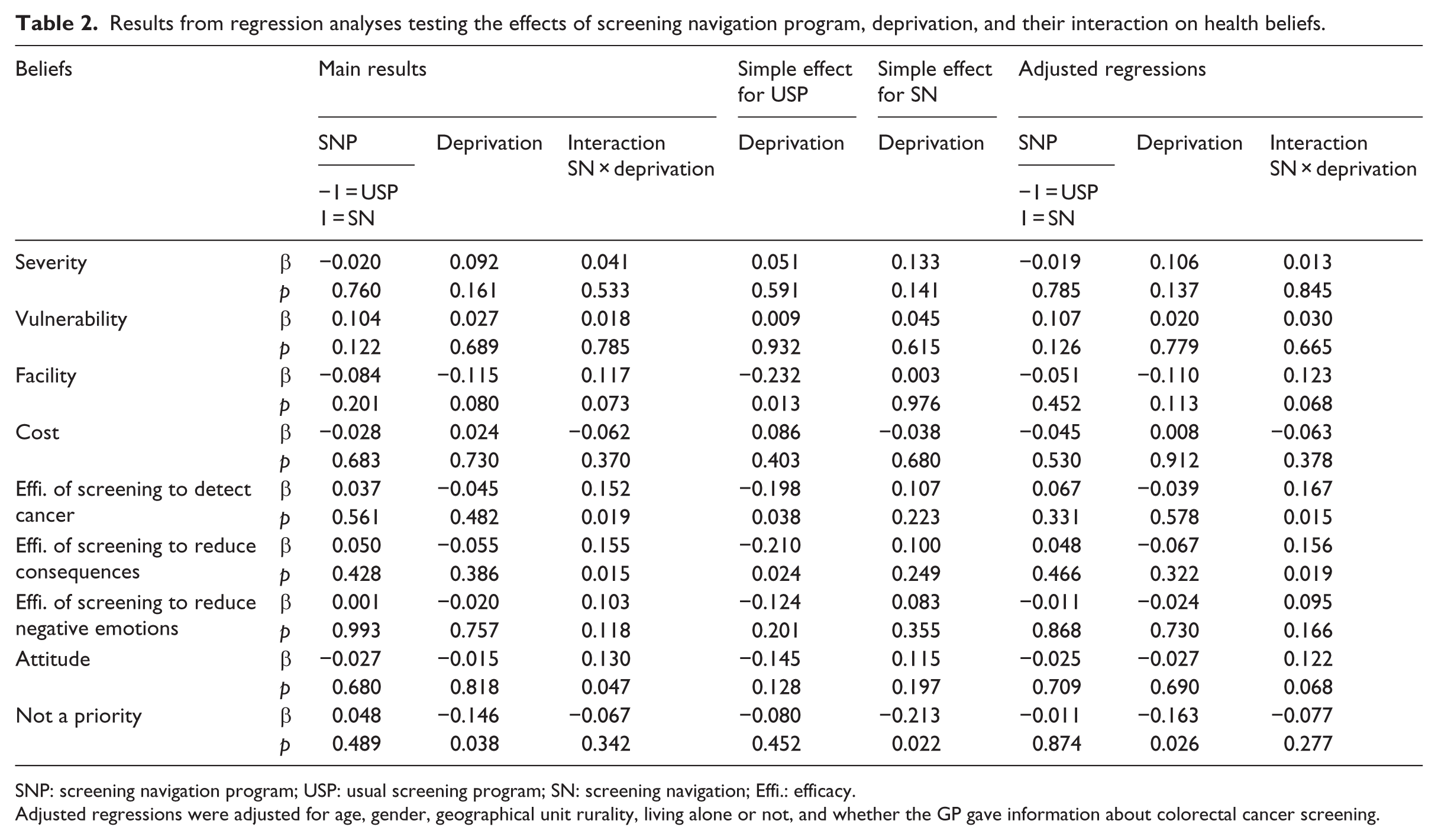
SNP: screening navigation program; USP: usual screening program; SN: screening navigation; Effi.: efficacy.
Adjusted regressions were adjusted for age, gender, geographical unit rurality, living alone or not, and whether the GP gave information about colorectal cancer screening.
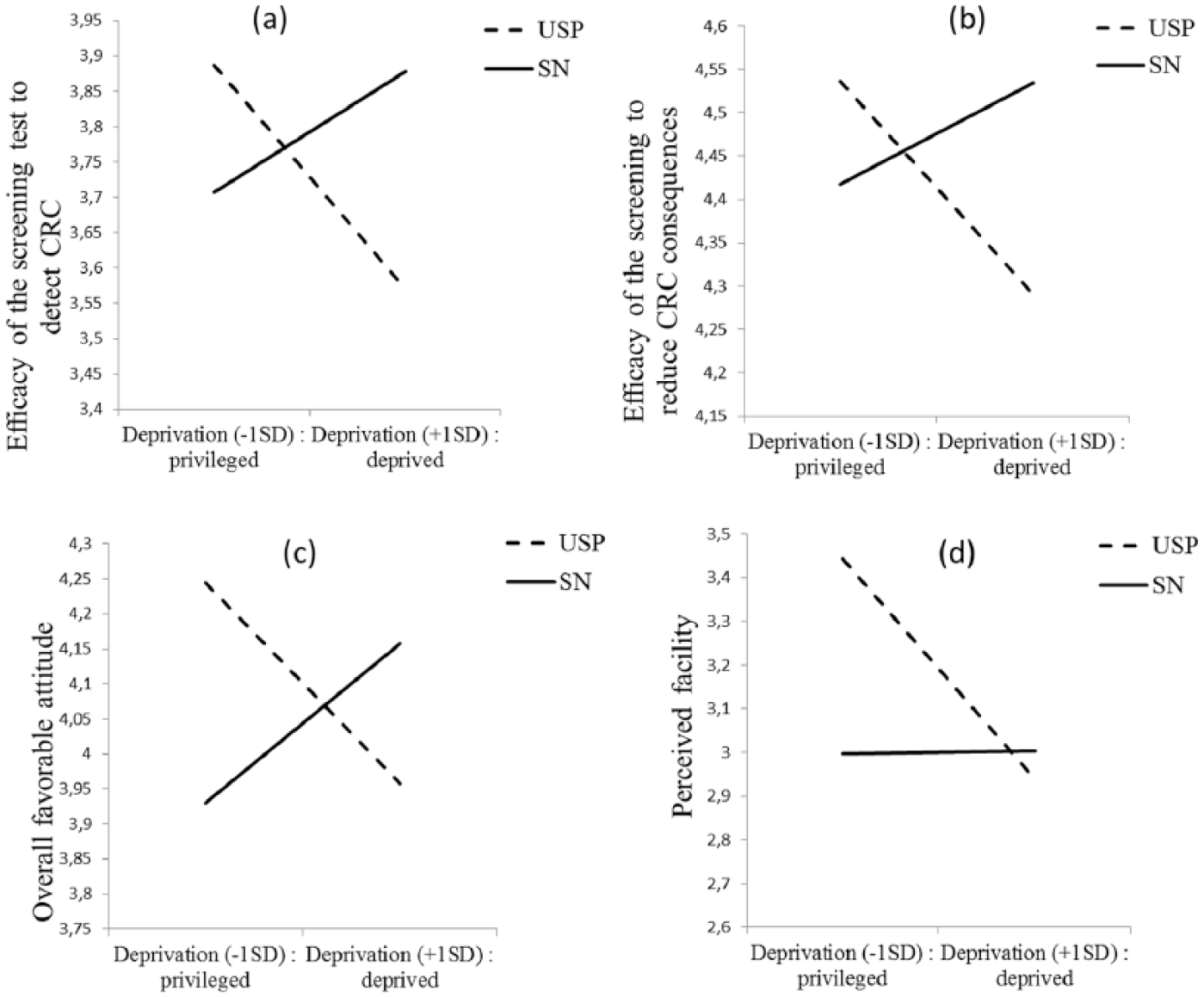
Results regarding the effect of screening navigation and Deprivation Index on (a) efficacy of the screening test to detect colorectal cancer, (b) efficacy of the screening to reduce colorectal cancer consequences, and (c) overall favorable attitude, and (d) perceived facility.
Note that no main effect of the Deprivation Index was found, as expected, for considering screening not a priority, and tendentially on perceived efficacy in the sense that people living in a more privileged IRIS believed more that colorectal cancer was not a priority and that screening was easier. Moreover, the adjusted regressions showed the same significant or tendential effects, except for overall attitude for which there was a tendential interaction effect between SN and the Deprivation Index. These interactions agreed with those obtained with the regressions without the controls, meaning that the effect of social deprivation on beliefs differed according to the arm (USP vs SN).
Discussion
This study aimed to test how an SNP intervention could lead to more favorable health beliefs and reduce social inequalities in them. The results showed no main effect of an SNP but SNP effects in interaction with socioeconomic status, measured by the Deprivation Index of the IRIS, on some beliefs. It is interesting to note that the threat-appraisal components of the Protection Motivation Theory (severity and vulnerability) were less affected by screening navigator actions to reduce social inequalities than were problem-solving components (e.g. perceived efficacy) or general perception of screening (attitude). This suggests that the SNP focused mostly on the screening procedure rather than on the perception people had about the possibility of having colorectal cancer or about its severity. The perceived costs, perceived efficacy in reducing negative emotions, as well as considering screening a priority, were not affected by the SNP in interaction with socioeconomic status. It is possible that these beliefs were not perceived as important barriers among the people contacted, were not expressed by people, or were not detected or removed by the screening navigators. Future research needs to investigate this point specifically, perhaps with a qualitative method in which people are asked to explain how they perceive the screening procedure of colorectal cancer and the benefits or costs of the SNP. Thus, the perception of SN should be evaluated by noncompliant participants in order to investigate whether (1) each belief is perceived as a barrier to screening, (2) participants might be disposed to express each of the possible barriers to a screening navigator and (3) each possible barrier might be addressed by a screening navigator according to the participants.
This research supports the role of SNPs to work on individual barriers encountered by a less privileged population, by showing that screening navigators, beyond logistical barriers, acted on the perception people have about screening. To our knowledge, this is the first study that has showed that SNP action is effective on health beliefs. Moreover, as this study targeted noncompliant people, the action of an SNP was effective in convincing people who had never been screened about the value of screening. The findings revealed that SN affected psychological processes (i.e. health beliefs) about screening. The reduction in social inequalities by the SNP could mean that health beliefs were different, or were of different importance, or that the information and interventions needed were different according to the social deprivation level of the groups (for differences between various social groups, see Austin et al., 2009; Davis et al., 2013; Holmes-Rovner et al., 2002; Molina-Barceló et al., 2011; Nayaradou et al., 2010). Moreover, in this study, the reduction in social inequalities could be increasing in deprived populations as well as decreasing in privileged populations. Further studies should explore more precisely which components of screening navigator actions could account for these changes in health beliefs in specific populations.
The study had some limitations. First, it was retrospective and therefore presented some limitations regarding cognitive reconstruction bias. Second, the questionnaire was sent 9 months after the intervention, which could mean that some more short-term effects were not observed. A follow-up study would identify the health beliefs of people involved in colorectal cancer screening before and after the SNP action, and thus provide a better understanding of its causal mechanisms in the short-term, and limit cognitive reconstruction. Third, the sample selected was not representative of the whole population (i.e. the population studied had a home and a telephone number). In order to reach people who were not contacted by this study, actions from the community (e.g. associations working on the ground) or GPs are needed to increase the representativeness of respondents (e.g. Sabatino et al., 2012).
To conclude, this study found a positive impact of the SNP on reducing social inequalities in health beliefs. This is an argument in favor of the development of SNP interventions, especially those targeting the more deprived population in France. Moreover, health beliefs were a mechanism of action of these SNPs and a promising way to understand the complex action of the SNP according to the person’s socioeconomic status. In order to understand the action of SNP intervention better, further research should investigate the precise information and help that are responsible for changes in health beliefs about colorectal cancer screening. Moreover, it seems important to examine how SN complements the information given by the GP (see Fenton et al., 2011, for results regarding the effects of GP messages). SN may encourage people to consult their GP more, who in turn will give them some information. Finally, an interesting point of this study was to focus on reducing social inequalities about health beliefs, which is rarely addressed by current interventions (e.g. Javanparast et al., 2010). Therefore, actions that reduce social inequalities about screening and consider the role of health beliefs in screening need to be further developed.
Footnotes
Appendix 1
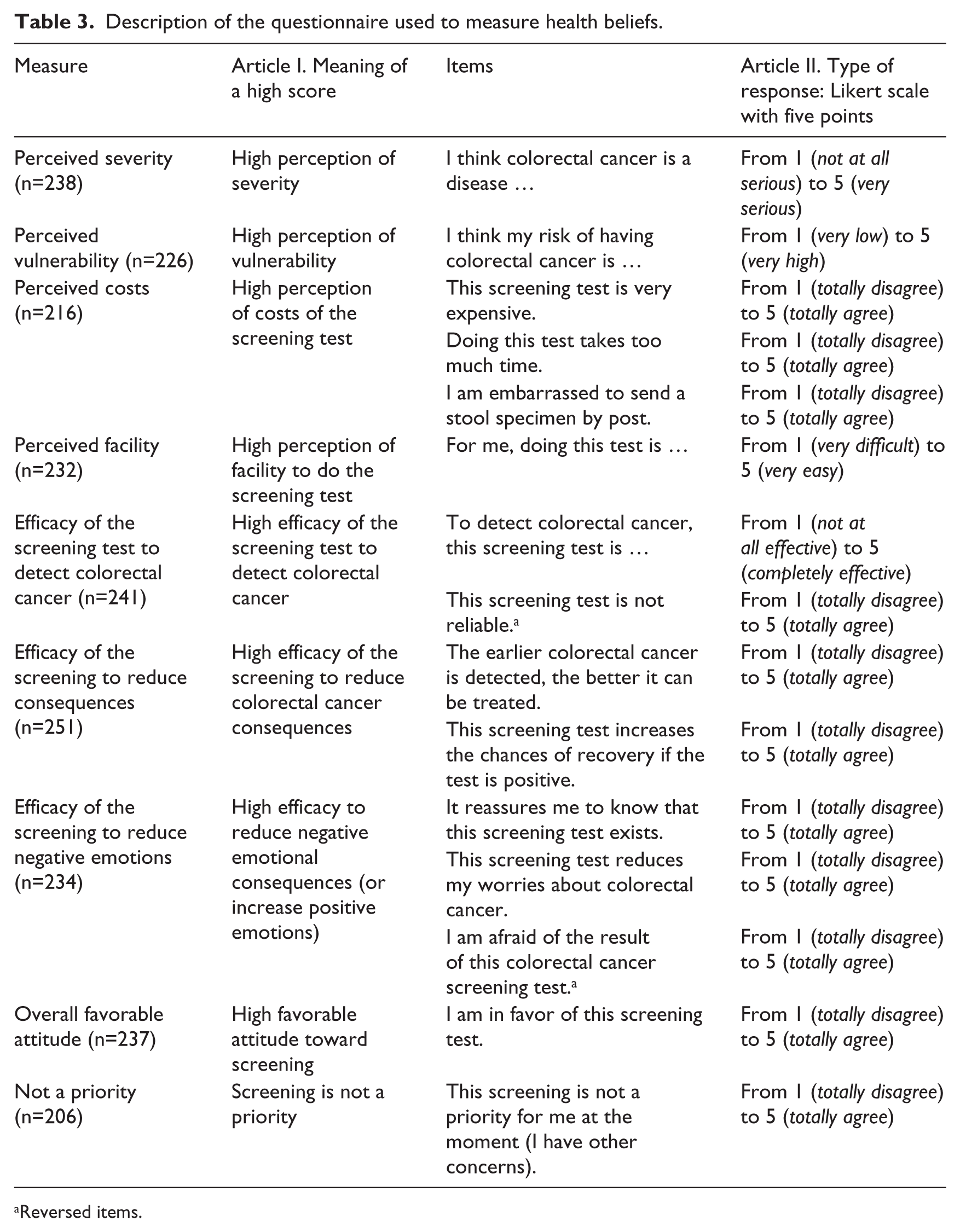
Description of the questionnaire used to measure health beliefs.
| Measure | Article I. Meaning of a high score | Items | Article II. Type of response: Likert scale with five points |
|---|---|---|---|
| Perceived severity (n=238) | High perception of severity | I think colorectal cancer is a disease … | From 1 (not at all serious) to 5 (very serious) |
| Perceived vulnerability (n=226) | High perception of vulnerability | I think my risk of having colorectal cancer is … | From 1 (very low) to 5 (very high) |
| Perceived costs (n=216) | High perception of costs of the screening test | This screening test is very expensive. | From 1 (totally disagree) to 5 (totally agree) |
| Doing this test takes too much time. | From 1 (totally disagree) to 5 (totally agree) | ||
| I am embarrassed to send a stool specimen by post. | From 1 (totally disagree) to 5 (totally agree) | ||
| Perceived facility (n=232) | High perception of facility to do the screening test | For me, doing this test is … | From 1 (very difficult) to 5 (very easy) |
| Efficacy of the screening test to detect colorectal cancer (n=241) | High efficacy of the screening test to detect colorectal cancer | To detect colorectal cancer, this screening test is … | From 1 (not at all effective) to 5 (completely effective) |
| This screening test is not reliable. a | From 1 (totally disagree) to 5 (totally agree) | ||
| Efficacy of the screening to reduce consequences (n=251) | High efficacy of the screening to reduce colorectal cancer consequences | The earlier colorectal cancer is detected, the better it can be treated. | From 1 (totally disagree) to 5 (totally agree) |
| This screening test increases the chances of recovery if the test is positive. | From 1 (totally disagree) to 5 (totally agree) | ||
| Efficacy of the screening to reduce negative emotions (n=234) | High efficacy to reduce negative emotional consequences (or increase positive emotions) | It reassures me to know that this screening test exists. | From 1 (totally disagree) to 5 (totally agree) |
| This screening test reduces my worries about colorectal cancer. | From 1 (totally disagree) to 5 (totally agree) | ||
| I am afraid of the result of this colorectal cancer screening test. a | From 1 (totally disagree) to 5 (totally agree) | ||
| Overall favorable attitude (n=237) | High favorable attitude toward screening | I am in favor of this screening test. | From 1 (totally disagree) to 5 (totally agree) |
| Not a priority (n=206) | Screening is not a priority | This screening is not a priority for me at the moment (I have other concerns). | From 1 (totally disagree) to 5 (totally agree) |
Reversed items.
Acknowledgements
This study received support from the Institut National du Cancer (INCa) and from the Cancéropôle Nord-Ouest. We would like to thank everyone who agreed to participate in this study. We are also grateful to the screening navigators whose work enabled the study to run smoothly and the screening management structures.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.