
Abstract
The current study aimed to explore the phenomenon of disease-related ‘query escalation’ in high/low health anxious Internet users (N = 40). During a 15-minute health-related Internet search, participants rated their anxiety and the perceived seriousness of information on each page. Post-search interviews determined the reasons for, and effects of, escalating queries to consider serious diseases. Both groups were found to be significantly more anxious after escalating queries. The high group was significantly more likely to escalate queries. Evaluating personal relevance of material was the main reason for escalations and moderated anxiety post-escalation. We conclude that searching for online disease information can increase anxiety, particularly for people worried about their health.
Introduction
Health anxiety is worry about having or acquiring a serious disease/illness (Warwick and Salkovskis, 1990). It is considered to be a dimensional construct ranging from minor and sporadic worry to clinically significant concern about one’s health (Ferguson, 2009; Longley et al., 2010), where a formal diagnosis may be warranted (American Psychological Association, 2013). The cognitive behavioural therapy (CBT) model of health anxiety (Warwick and Salkovskis, 1990) suggests that an instance of health anxiety occurs when dormant dysfunctional beliefs (e.g. ‘all symptoms are serious’) are triggered by a critical event (e.g. physical symptom). A maladaptive appraisal process then begins where threat confirmatory evidence is collected. Once activated, various cognitive, behavioural, affective and physiological maintenance factors sustain health anxiety (Warwick and Salkovskis, 1990).
Some commentators suggest that one such maintenance factor is excessive health-related Internet usage (e.g. Starcevic and Berle, 2013; Wells, 1997), which may constitute a form of reassurance seeking, checking or safety behaviour that negatively reinforces illness preoccupation. Such usage may also expose users to potentially alarming, inaccurate and/or contradictory information, thereby increasing anxiety/preoccupation. Furthermore, the sheer volume of health information online makes evaluating relevance to one’s own health issue a difficult task (Singh et al., 2015), increasing the likelihood of misinterpretation and catastrophic thinking. Several studies support the idea that health-related Internet use is more common in high health anxious individuals. Such individuals search more frequently, for longer and for more medical/illness-related information than low-anxious controls; they also report feeling tenser, more distressed and anxious post-search and indicate possible health-related Internet addiction (Baumgartner and Hartmann, 2011; Muse et al., 2012; Singh and Brown, 2014).
‘Query escalations’ (e.g. searching for information about serious diseases that are a possible, but unlikely, cause of symptoms that were the original focus of the enquiry) may be a particular source of anxiety during online searches. Such escalations are often a feature of health-related Internet searching (White and Horvitz, 2009) and may expose users to information that could trigger health anxiety. Health anxious individuals may be particularly at risk of experiencing the negative effects of query escalating, as they are inclined to overestimate the relevance of serious material (Marcus et al., 2008), and focus on threat confirmatory illness information (Warwick and Salkovskis, 1990). Such alarming material could lead to increased worry, checking behaviour (e.g. for new symptoms that have been identified as relevant to that disorder) and healthcare utilization (Singh et al., 2015).
As Microsoft Corporation employees, White and Horvitz (2009) determined the extent of query escalations during online health searches by logging the health-related Internet searches/activity of several hundred thousand Internet users. Medical queries within these logs were matched with ‘a consumer health vocabulary’, drug names from the US Food and Drug Administration and a list of medical symptoms with both innocuous and serious causes for each. They defined escalations as queries where the content pertained to serious causes of symptoms that had previously been searched for within that session and/or if queries were accompanied by modifiers that suggested serious concern (e.g. ‘fatal’; White and Horvitz, 2009). They found that 2 per cent of all Internet queries were health-related, of which 5.3 per cent constituted escalations. However, this low prevalence of escalations may be attributable to the limited number of symptoms in their list.
As White and Horvitz used anonymous logs of web searches, why such health searches were being conducted and their effects on users are unclear. It is also unknown whether high health anxious individuals are more likely to escalate queries than low health anxious individuals or experience more adverse consequences as a result. Theory suggests that health anxious individuals may be prone to escalating online queries, perhaps due to their selective abstraction of illness information (Lucock et al., 1997), illness-related catastrophizing (Tang et al., 2007) and confirmatory bias for illness information (Hadjistavropoulos et al., 1998).
We aimed to explore the relationship between health anxiety and query escalation using groups scoring as high or low health anxious on the Short Health Anxiety Inventory (SHAI; Salkovskis et al., 2002). Low health anxious participants were included to aid in determining whether or not query escalations and changes in anxiety were exclusive to the health-related searches of high health anxious individuals. Including a low health anxious control group also helped examine any inter-group differences in health-related online searching (e.g. type and number of pages utilized). We observed participants’ health searches in vivo to identify instances of query escalation, understand the rationale behind searches and determine the effect of escalations on users’ anxiety. Unlike White and Horvitz, who used objective medical criteria to determine the seriousness of escalated-to causes, we defined query escalations as searches about conditions that the participant perceived to be a serious cause of a symptom, which we regarded as more relevant to health anxiety.
We predicted that query escalation would be more common in health anxious individuals than those with low health anxiety and would be associated with a greater increase in anxiety. Furthermore, we predicted that health anxious individuals would (prior to escalating) perceive their escalated-to causes as more serious and would be quicker to escalate than low health anxious individuals. We also obtained qualitative information to understand why participants were escalating queries and its effect on their anxiety.
Method
Design
A between-subject design was adopted, using a novel task designed to capture Internet search behaviour in relation to personally relevant physical symptoms. Participants were later asked to view a recording of their behaviour while searching and were interviewed about this search behaviour and experiences. We used this information to identify instances of query escalation, which we defined as any search (by clicking on a link, entering a term into a search engine, etc.) about a potentially serious cause for a symptom previously enquired about during the session. Anxiety changes associated with search behaviour were determined by examining the participants’ anxiety immediately before accessing new pages/sites and at the beginning, middle and end of their time on each page/site. Questions about the reasons for, and effects of, searching were also asked, and responses were analysed qualitatively using content analysis.
Content analysis
The content analysis was based on the approach recommended by Mayring (2004). The in-experiment searches and associated qualitative questioning were carried out primarily by the first author (K.S.) who also later transcribed, coded, quantified and analysed findings. The second author (R.J.B.) reviewed the work of the first author during all stages of this process in order to ensure proper analysis and reduce any potential bias.
Screening and study participants
A total of 300 undergraduate students from the University of Manchester were screened using the SHAI (Salkovskis et al., 2002) as a part of a study conducted 2 weeks prior to the current investigation. The SHAI is an 18-item measure with established validity and reliability as a measure of health anxiety (Abramowitz et al., 2007; Salkovskis et al., 2002). Each item is scored from 0 to 3, with total scores ranging from 0 to 54. Although disagreement remains as to what constitutes clinically significant health anxiety on the SHAI (Alberts et al., 2013), a score of ⩾18 is often used as a clinical cut-off (Improving Access to Psychological Therapies – National Health Service (IAPT-NHS), 2011; Muse et al., 2012). Participants scoring in the top (i.e. high health anxious; scores ⩾18) and bottom quartiles (i.e. low health anxious; scores ⩽10) on the scale were invited to take part in this study. The first 20 high (SHAI = 24.50; SD ± 4.27; mean age = 20.50 years; SD ± 2.74; 80 percent female) and 20 low health anxious (SHAI = 8.15; SD ± 2.15; mean age = 19.60 years; SD ± 1.31; 75 percent female) volunteers were recruited for the main study using a credit for voluntary participation scheme. There were no significant between-group differences in gender (χ2(1) = .143; p > .705) or age t(38) = −1.184; p > .244). A student sample was utilized for convenience purposes. A student sample also provides a sample more likely to have searched online for health information due to the Internet’s prominence in their lives and would display relative expertise in using the medium for such purposes. Recruiting a student sample also demonstrates proof of principle, which could highlight areas of health-related Internet searching that are particularly important to health anxious users; these findings could target suggestions/research for use in clinically diagnosed health anxious individuals.
Internet search paradigm
Symptom selection phase
We sought to simulate participants’ normal behaviour when searching online for personally relevant symptomatic information. For this, idiosyncratic search targets were determined using a selection procedure designed to identify symptoms that were regarded as most threatening by that participant. In total, 15 symptoms were derived from the Patient Health Questionnaire (PHQ-15; Kroenke et al., 2002) representing 90 per cent of the symptoms encountered in primary care settings (Kroenke et al., 2002). Participants were first asked to indicate which of the 15 symptoms they had experienced previously (to determine relevant symptoms most likely to instigate a health-related Internet search under normal circumstances). For any previously experienced symptom, they rated how worried they would be should that symptom recur, on a 6-point Likert scale ranging from 0 (‘not worried at all’) to 5 (‘extremely worried’). Finally, they rated the likelihood of symptom recurrence for any previously experienced symptom, on a 6-point Likert scale ranging from 0 (‘not likely at all’) to 5 (‘extremely likely’). Scores from the second and third questions were summed for each symptom with the highest scoring (i.e. most threatening) symptom selected for use in the Internet search task. When a tie occurred, the symptom with the highest worry rating was used.
Symptom search phase
Participants were sat in front of a computer and asked to spend 15 minutes searching online for information pertaining to the most threatening symptom identified in the selection phase, imagining that they were experiencing, or had recently experienced, the symptom. The duration of the search matched the average online health information search time identified by Singh and Brown (2014). Participants were encouraged to search as they normally would at home but were given no further direction on how or what to search. Data concerning their search behaviour were obtained by using Apple QuickTime (v.10.6.3) to record the screen.
Interview phase
Immediately after the search, participants completed a task validity check question (‘how similar was searching for this symptom here to what you would normally do at home?’) on a 6-point Likert scale ranging from 1 (‘not similar at all’) to 6 (‘it is exactly how I would do it at home’) to determine any differences between normal and in-experiment search behaviour. The screen recording was then played back double speed (for optimal interview efficiency), and participants were interviewed about their experiences during the task. For each page/website accessed, participants were asked the following: why that particular website/page had been selected (over any alternatives) and/or why a new search (if applicable) had been initiated; their anxiety level at the beginning, middle and end of the site/page (rated verbally from 0 (‘not anxious at all’) to 10 (‘extremely anxious’)); thoughts as to why anxiety had/had not changed while on the site/page; the perceived seriousness of any conditions being searched for (prior to escalating, rated from 0 (‘not serious at all’) to 10 (‘extremely serious’)); and thoughts concerning the relevance of the site/page to their own symptoms. At the end of the interview, participants were asked to explain their answer to the above mentioned task validity check question.This was used as an indicator of the ecological validity of our task.
Procedure
Participants previously identified as high and low health anxious read an electronic information sheet and then completed a consent form and the symptom selection phase online. They then arranged to attend an experimental session where they completed the symptom search task and interview. Finally, participants were debriefed, questions were answered and university counselling centre details were reiterated.
Data analysis
Quantitative
Searches were deemed to be escalations if (a) the participant rated the perceived seriousness of the escalated-to cause/condition as five or above (on a scale from 0 (not serious at all) to 10 (extremely serious)) before accessing the page and/or (b) the participant verbally stated that they regarded the cause/condition as serious. We determined the proportion of participants in each group who engaged in at least one query escalation, number of escalations per group, perceived seriousness of the escalated-to causes, the number of different sites/pages visited and anxiety changes associated with all page/website changes (three measures: anxiety rating at the beginning of the changed-to page minus the last anxiety rating on the site/page prior to changing page, anxiety rating at the middle of the changed-to page minus the last anxiety rating on the prior site/page and anxiety rating at the end of the changed-to page minus the last anxiety rating on the prior site/page), per group. Overall sessional anxiety (calculated as the mean of all anxiety ratings taken) was also measured to determine between-group differences in anxiety while searching. These measures were compared using chi-square and t/F-tests (or Mann–Whitney tests for non-normal variables) as appropriate. Given that this is a relatively unexplored phenomenon, as well as Perneger’s (1998) critique of Bonferroni adjustments, a relatively liberal alpha of p < .05 (two-tailed) was used to determine statistical significance.
Qualitative
Content analysis was used to explore participants’ thoughts regarding any anxiety changes while searching, focusing specifically on what caused these changes (if any). This was repeated for perceived seriousness, explanation of the task validity measure rating, thoughts occurring on each site/page and reasons cited for escalating queries. During content analysis, interview data were transcribed and divided into separate sites/pages for each participant; content (i.e. escalations, anxiety changes, etc.) were then quantified and compared between groups. Common themes regarding why escalations and/or anxiety changes were occurring were also analysed in order to contextualize quantitative findings.
Results
Task validity check
Over 75 per cent of the total sample rated their Internet search as at least ‘quite similar’ to how they would search at home (‘it is exactly how I would do it at home’, 25 % ‘very similar’, 27.5 % ‘quite similar’, 25 percent). The remainder of the participants rated their in-experiment search as ‘moderately similar’, 15 percent (6); ‘a little similar’, 5 percent (2); and ‘not similar at all’ 2.5 percent (1). The between-group differences, however, were not significant (high group mean: 4.80; SD ±1.28; low group mean: 4.10; SD ±1.25; t(38) = −1.747, p = .089; partial η2 = .074). Though the differences in the group means suggested that the high health anxious group’s in-experiment searches were slightly more comparable to their usual searches.
Search characteristics
Table 1 provides the quantitative data concerning participants’ search behaviour.
Between-group descriptive statistics for pages with and without query escalations.
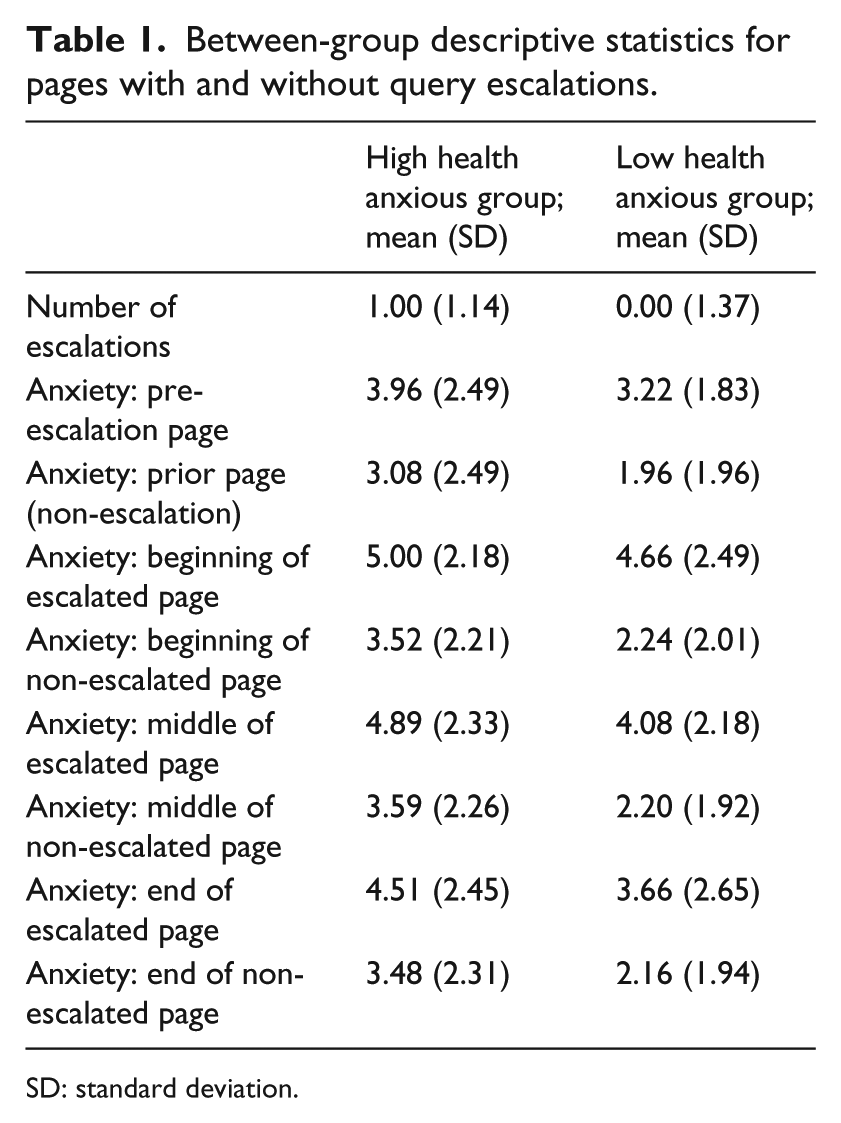
SD: standard deviation.
Number of sites/pages visited
A two-way analysis of variance (ANOVA) was conducted using the number of pages/sites visited as the target variable, with group (high vs low health anxiety) and escalation tendency (participants who escalated at least once vs participants who never escalated) as between-subject factors. There was no significant difference between groups in the number of pages searched overall (F(1) = .458, p > .503; partial η2 = .013), and no significant group × escalation tendency interaction (F(1) = .458, p > .503; partial η2 = .013). However, those participants who escalated at least once visited significantly more pages than those participants who did not escalate at all (F(1) = 9.27, p < .004; partial η2 = .205).
Overall anxiety
A two-way ANOVA was conducted using overall within-session anxiety as the target variable and health anxiety group and escalation tendency as between-subject factors. Neither of the main effects (group: F(1) = 2.35, p > .133; partial η2 = .061; search-type F(1) = 2.49, p > .123; partial η2 = .065) nor the interaction (F(1) = .007, p > .936; partial η2 = .000) was significant.
Tests of hypotheses
The entire sample made 347 searches (i.e. new sites/pages), of which 47 (13.54 percent) constituted query escalations. The majority of the non-escalation searches were typically for conditions not perceived as serious or for indirect material about disease (e.g. media articles, personal experiences). In total, 60 per cent (n = 24) of participants escalated their queries at least once during the search session, of whom 8 were low health anxious and 16 were high health anxious. This difference was statistically significant (χ2(1) = 6.66; p < .01). However, the difference in the average number of query escalations per group was close to, but not, significant (U(38) = 132.50, p = .056; r = .30). Although high health anxious participants were quicker (mean: 4 minutes, 30 seconds; SD ±3:52 minutes) to their first (or only) query escalation than the low health anxious participants (mean: 7 minutes, 22 seconds; SD ±4:36 minutes), this difference was not statistically significant (t(22) = 1.73, p = .097; d = .73). Prior to escalating queries, high health anxious participants perceived the escalated-to causes as more serious on average (mean 8.16; SD ±1.50) than the low health anxious participants (mean = 7.13; SD ±1.76); however, this difference was close to, but not, significant (t(31) = −1.815, p = .079; d = .65).
Of the 47 escalations, anxiety reduced immediately after accessing the escalated-to page in 8 (17.02 percent), remained the same in 13 (27.65 percent) and increased in 26 (55.31 percent) cases. In comparison, of the 300 non-escalation page/site changes, anxiety immediately reduced in 88 (29.33 percent), remained the same in 129 (43 percent) and increased in 83 (27.6 percent) cases. These proportions were comparable for the high and low health anxious groups (χ2(2) = .491; p > .782). A mixed-model ANOVA on anxiety change scores taking group (high vs low health anxious) and search type (escalation vs non-escalation) as between-subject factors and time (start vs middle vs end of changed-to page) as a within-subject factor was conducted. Only a significant interaction between search type and time was found (F(2) = 3.96, p < .05; η2 = .022); the source of this interaction was a significant main effect for search type on anxiety change at the start of reading the changed-to page (F(1) = 7.66, p < .006; partial η2 = 0.22), indicating a significantly greater increase in anxiety immediately after query escalations than after non-escalation page changes. Within groups, analyses indicated that both groups were significantly more anxious when first accessing the escalated-to page compared to their pre-escalation anxiety (low health anxiety: t(17) = −3.14, p < .01, d = −1.52; high health anxiety: t(28) = −2.79, p < .01, d = 1.05).
Content analysis
Content analysis revealed that the most popular strategy was to use the topmost sites on a search engine’s search result and continue down the list in a sequential order. All 40 participants indicated that they preferred to utilize sources they perceived as credible/reliable and familiar for finding online health information (e.g. government websites; WebMD).
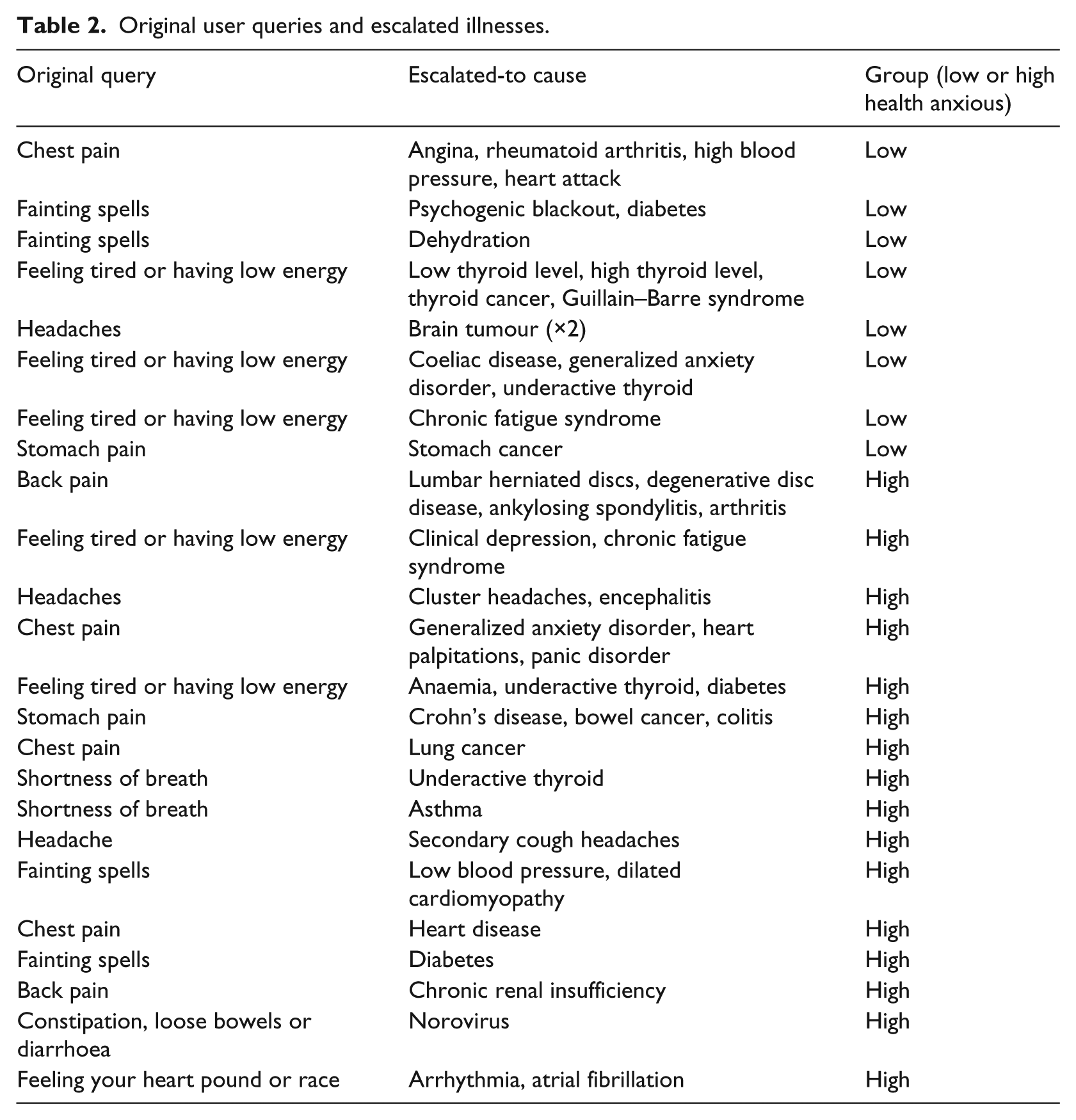
Table 2 summarizes the query escalations across the two groups. Participants often cited more than one reason for escalating a query. The most common reason for escalating was to evaluate the relevance of the escalated-to material (to oneself or others; e.g. family). Participants often said that their choice of websites/pages related specifically to their desire to evaluate the likelihood of a serious cause as the reason for their symptoms/concerns. In general, serious causes that were perceived as likely explanations increased anxiety:
… I’ve heard of it before but I think it’s really serious [the escalated cause] … it obviously said that it could be one of the symptoms again, so then I think that’s very scary … – Participant 32
Original user queries and escalated illnesses.
Conversely, anxiety typically reduced if the page suggested little relation between symptoms and the serious escalated-to cause:
… I thought it was quite serious, when I opened the page … I was worried about it from having something similar previously, but then as I read on … and saw some of the things, I thought, it doesn’t really apply to me … – Participant 25
In total, 23 instances of query escalation were explicitly attributed to examining the possibility/likelihood of a serious illness being relevant to one’s own/others’ symptoms; 13 instances were attributable to the high and 10 to the low health anxious group. This difference was not significant (χ2(1) = .921; p > .337). In total, 10 participants (2 low health anxious, 8 high; χ2(1) = 4.80; p < .02) cited previous symptom experience or genetic predisposition as the reason for escalating a query to serious causes.
Three participants (two low health anxious and one high) escalated queries to determine whether a specific condition referred to in the title of a link/page might be relevant to them or significant others:
… It sounded quite serious, I didn’t think I had it but because it sounded [serious], that’s what I think drew me in … – Participant 36
All three participants experienced minor anxiety increases due to the perceived relevance of the serious cause to their symptoms; all three ended the page with lower anxiety because information became irrelevant as they read on.
Other instances of escalation (each n = 1) were related to evaluating the prevalence of a serious issue, to confirm earlier search findings and to find out more about a disease that had received recent media coverage. In each case, the motive behind searching also appeared to be determining the personal relevance of the escalated-to causes. One high health anxious participant stated that she habitually escalated queries and gravitated towards serious causes to determine symptom relevance. In this case, the escalated-to cause was perceived as relevant and concerning (partly related to the complicated/invasive nature of diagnostic tests) and therefore increased her anxiety. This increase remained throughout the session and prompted the participant to consider post-search doctor utilization.
In some cases (five low health anxious, seven high), participants cited curiosity/interest or a desire for general knowledge as a reason for escalating:
… I’m not sure, it was just something … about that one where I was just like, I think I just wanted to know more about it … what it is, how it’s caused and stuff … – Participant 23
These searches typically reduced anxiety when serious causes were deemed irrelevant, although two participants (one high health anxious, one low) experienced increased anxiety. Although participants explicitly cited curiosity as their primary motive, the nature of their responses suggested an underlying motivation to evaluate the personal relevance of escalated-to causes:
… I was just interested, I thought, that’s quite a serious one, um bowel cancer, so I thought maybe I should look at it … – Participant 32
Some participants experienced reduced anxiety while reading information on escalated-to pages, but their anxiety remained above zero. Participants attributed this to the following: remaining uncertain regarding their symptom’s cause (three high health anxious, six low), confusion surrounding information encountered (seven high health anxious, three low), failing to resolve the issue (e.g. due to having not complied with treatment; one high health anxious, three low) and uncertainty regarding symptom worsening. The high health anxious group was unique in reporting unresolved anxiety because their symptoms had not dissipated (four cases); responses suggested that their anxiety would dissipate entirely with symptom cessation.
Discussion
We examined the occurrence of query escalation in health-related web searches conducted by high and low health anxious participants. We extended previous research by determining whether escalating from symptom to serious disease searches was more common and more anxiety provoking in high than low health anxious individuals, and exploring possible between-group differences in reasons for, and the effects of, escalating. Overall, we found that 13.5 per cent of all health-related site/page visits were query escalations; this is slightly higher than the previous estimate of 5 per cent (White and Horvitz, 2009), although both studies suggest that escalation is relatively uncommon. However, more escalations might have been uncovered with longer or multiple search sessions, this is something for future research to consider. Future research should also examine our findings using a continuum of health anxious individuals (high, medium and low), perhaps by using a regression analysis to determine how health anxiety, as a dimensional construct, predicts the number of escalations, associated anxiety, the number and type of pages visited and so on.
Interestingly, those who escalated their queries at least once utilized more websites/pages during their search session. Although the overall nature and extent of searching was broadly comparable between the high and low health anxious groups, a significantly greater proportion of the high health anxious group engaged in query escalation than the control group, consistent with expectation. Although just non-significant, effect size estimates for the average number of searches and time to first search suggest that high health anxious participants engage in more query escalation and escalate quicker than their low health anxious counterparts. This is particularly noteworthy given that some high health anxious participants were already familiar with uncovered causes/information and therefore might have ignored or avoided previously searched/found information. Modifying the method to require participants to search for novel, yet feared, symptoms may address this particular shortcoming.
Query escalations resulted in significantly greater anxiety increases than non-escalation page changes, but only immediately after accessing the new page. This was comparable for high and low health anxious groups, suggesting that escalation is anxiety provoking regardless of any characteristic level of health anxiety. We note that it is likely that increases in anxiety were due to the perceived seriousness of the escalated-to cause, which was our main criterion in defining an instance of query escalation. Therefore, it was expected that searches that were deemed serious were also more likely to cause anxiety. Similarly, increases in anxiety, although significantly higher in both groups post-escalation, largely placed participants in both groups in the range of moderate to high anxiety. Nonetheless, the results still suggest that query escalations associated with health-related Internet use do contribute to a detrimental increase in anxiety. Given the popularity of the medium to obtain health-related information (for both health anxious and non-health anxious individuals), our results warrant further investigation from future studies. Qualitative data suggested that subsequent anxiety dissipations, as the search(s) continued, were typically because escalated-to causes were evaluated as less applicable/relevant to participants personally (e.g. irrelevant symptoms listed), less serious than previously feared and/or because alternative, less serious, explanations were also identified. However, when escalated-to causes continued to be perceived as serious and/or directly relevant, anxiety remained elevated throughout the time spent on the escalated-to page. Future research should determine the accuracy of such relevance/seriousness appraisals and determine how online health resources might be modified to help users draw more accurate conclusions about information relevance.
Notably, the anxiety associated with query escalation in our study was relatively short-lived (cf. Singh and Brown, 2014; White and Horvitz, 2009), although some participants did experience enduring health anxiety post query escalation. Uncertainty and confusion were the two most prominent reasons cited for this. We did not explicitly determine the extent and duration of participants’ anxiety after the experiment, but it is possible that any between-group differences in anxiety resulting from the search only manifested later, after the opportunity for extended rumination about the search results (Marcus et al., 2008).
There were no between-group differences (regardless of escalation) in overall anxiety during the search session, which was unexpected given participants’ SHAI scores. As above, this may be because the high health anxious group were more likely to have searched the Internet previously about the symptom in question and may (as several participants suggested) have been familiar with the material from prior searches. This could be seen as a limitation of this method.
Qualitative analysis revealed that the participants’ main rationale for escalating was to determine whether the escalated-to causes were a possible explanation of their own/others’ symptoms. Various factors seemed to influence whether escalated-to causes were regarded as potentially relevant, including symptom overlap, prior illness experiences, perceived predisposition and the prevalence and seriousness of the cause. In total, 10 participants (25 percent) evaluated the information’s relevance to someone else’s symptoms, consistent with previous research (Singh et al., 2015). Future studies should also attempt to better control for individual variables from our current findings such as genetic predisposition, which could improve explanations for anxiety increases over time (e.g. repeated experience with unknown symptoms over time causing increases in anxiety). Controlling these individual variables could magnify between-group differences in the likelihood of search escalations, therefore providing a better explanation for query escalations.
Some participants reported that searches for curiosity, interest and general knowledge accounted for some of their query escalations, which could reflect that the duration of the search was longer than some participants would normally spend searching at home. Although a proportion of these searches seemed to be driven by relevance evaluation, our earlier study (Singh et al., 2015) suggested that searches for curiosity, interest and general knowledge are largely separate from anxiety-based searches. This may explain why most escalations in this category did not increase anxiety. Nevertheless, searches driven by curiosity increased two participants’ anxiety as escalated-to causes were (presumably unexpectedly) considered relevant to them. It should also be noted that the methodology currently utilized assumes that participants have an accurate insight into the reasons for their query escalations. However, we cannot be certain of this. It could be that participants are inaccurately attributing escalations to curiosity, general knowledge and so on, rather than to their own anxieties. This may be seen as a limitation of our study.
The finding that our health anxious group was more likely to escalate queries is consistent with the cognitive-behavioural notion that selectively attending to threatening illness information, perhaps as a result of a confirmatory bias, is a feature of health anxiety (Hadjistavropoulos et al., 1998; Owens et al., 2004; Salkovskis and Warwick, 2001; Tang et al., 2007). In the case of query escalation, this bias is likely to be more strategic than automatic as it involves a deliberate choice motivated by specific goals. Focusing online searches on serious causes in this way may increase the likelihood of catastrophic thinking and disease conviction in susceptible individuals (Warwick et al., 1996), thereby exacerbating prior health concerns, preoccupation and anxiety.
Consistent with previous research (Singh et al., 2015), we found that both high and low health anxious participants attempt to utilize sources that are perceived as familiar, credible, reliable and renowned. This further suggests that in-experiment searches were comparable to those conducted at home. The most prominent search strategy was to utilize websites at the top of the search results page. We also found that both groups evaluated websites in relation to whether they are likely to provide relevant information for themselves or others (including escalated sources).
The paradigm utilized in our study is a novel approach that allows detailed scrutiny of Internet search behaviour under controlled conditions. Our task validity check suggested that the majority of participants regarded their during-experiment Internet searches as broadly comparable to their normal at-home search behaviour, with the only major difference being the amount of time spent per search. Contrary to previous research (Singh and Brown, 2014), the majority of participants in this study stated that they would spend less time searching for online health information (5–10 minutes) per search session, although more time might be allocated depending on issue familiarity and perceived seriousness (consistent with Singh et al., 2015). Although most participants rated their within-experiment search as similar to their normal routine, the laboratory environment may have caused participants to modify their search behaviour and reasoning to meet experimenter expectations (i.e. Hawthorne effect) or to suppress potentially embarrassing queries/behaviours. Future research could utilize more naturalistic methods to study online search behaviour and escalations by using a method to examine the participants’ unprompted health-related Internet use at home, perhaps with an automated procedure that does not require participants to interact with a researcher at all; this would be less labour intensive and could limit social desirability and experimenter effects, although it would be less controlled than the method used here.
One of the potential limitations of our study is that the interviewer followed a pre-defined set of questions and elected not to probe answers in order to limit the amount of information collected. Including additional questions to clarify, online search behaviour (e.g. ‘what were you trying to find here?’, ‘did you find what you expected?’) could have benefitted the study and better contextualized participants’ motivations to escalate queries. Probe questions would also have been useful for extracting relevant details, particularly for participants who cite curiosity as their main motivator but imply that relevance evaluation is also a contributing factor.
Our participants were asked to imagine that they had recently, or were currently, experiencing the symptom they were meant to search for during the experiment. It would have been beneficial to determine the number of participants who were currently experiencing the searched-for symptom, particularly as escalations may be more likely for symptoms/illnesses that are actually present, rather than imagined. Future research might benefit from using samples (perhaps recruited from hospital or general practice settings) that are all experiencing the symptoms they are searching for.
Furthermore, although participants were asked to provide anxiety and seriousness ratings while watching a video recording of their search, there is a possibility that recall bias may have affected our results. Nonetheless, participants viewed their recording immediately after their original search in order to reduce the likelihood of such recall bias. Also, asking participants to rate their anxiety and perceived seriousness of illnesses during search would have added a level of distraction that could have reduced the likelihood of observing naturalistic search behaviours.
This study is limited by its use of a non-clinical sample. Even so, our high health anxious group’s average SHAI score of 24.50 is well beyond the cut-off for clinical health anxiety used by several other studies (Muse et al., 2012; Rode et al., 2006). It is also above the score (18) that is used to identify cases of clinically significant health anxiety in the UK National Health Service (NHS; IAPT-NHS, 2011). We would therefore argue that the results from our high health anxious group are of clinical relevance. Nonetheless, future studies may benefit for replicating these findings with a pre-defined clinical sample. In any case, the current investigation provides positive clinical implications such as aiding case formulation and areas to focus on during therapy. For example, similar to our methodology, a clinician may record their patient’s online search behaviour in order to later review and determine problematic areas of health-related Internet usage. These areas may then be used as a basis of in-session experiments, psychoeducation within therapy or as a basis of homework assignments. Here, we found that determining relevancy was the main motivation in deciding to escalate queries. A metacognitive therapist may decide to determine the specific underlying motivations behind needing to seek relevancy of online health information, and then target changing these underlying motivations within therapy. When changed, this may lead to reductions in query escalation and associated increases in anxiety. Future researchers should attempt to further our current methodology/findings as a basis of uncovering additional clinical benefits within this area of research.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.