
Abstract
Predictors of breast cancer worry in healthy women remain unclear. Healthy women less than 50 years (N = 857) completed measures of family history, anxiety, absolute and comparative risk perceptions, illness perceptions, and breast cancer worry. Regression analyses revealed that having a family history of breast cancer, greater anxiety, higher absolute risk perceptions and negative illness perceptions predicted 45 per cent of the variance in breast cancer worry. Risk perceptions also partially mediated the relationship between illness perceptions and worry. This study provides novel evidence that both illness and risk perceptions are predictors of breast cancer worry in younger women from the community.
Breast cancer is the most common form of invasive cancer diagnosed in women worldwide (Jemal et al., 2010). Although only a quarter of women diagnosed with breast cancer are below 50 years of age, tumours in younger women tend to be more advanced (Kroman et al., 2000). Breast cancer can cause distress in women with a diagnosis and may cause worry in healthy women considering their risk of developing the disease. Breast cancer worry is a specific concern, fear, anxiety or worry about developing breast cancer in the future (Consedine et al., 2004). It is associated with adherence to breast cancer screening, breast self-examination (Brain et al., 1999; Hay et al., 2006) and BCRA1/2 testing for breast cancer (Lerman et al., 1995), so understanding the predictors of breast cancer worry is an important focus of concern.
Breast cancer screening is not advisable for women under the age of 50 years, as its efficacy and reliability are unclear for this group. It is, however, recommended that all women become breast aware (Austoker, 2003), and identifying factors that influence breast cancer worry in this group may help to improve women’s breast awareness, while also avoiding premature breast screening.
General distress, which can accompany breast cancer diagnosis, may influence cancer worry. While the majority of women adjust well within a year of diagnosis (Ganz et al., 2011), some continue to experience significant adjustment problems. For example, anxiety and depression improved over 1 year post-treatment for breast cancer but at 18-month follow-up some women still reported severe anxiety and depression (Vahdaninia et al., 2010). Women with breast cancer who report general distress also experience greater cancer-related distress, anxiety or fear of the future. The influence of general distress on cancer-related worry in healthy women has not been examined. It may be that general worry precipitates cancer-specific worry, which may lead to inappropriate screening behaviours in this group.
Previous studies have documented a positive relationship between family history and cancer worry and related outcomes such as cancer-related distress (Bennett et al., 2010; Patenaude et al., 2013). Having a family history of breast cancer may also lead to greater perceived risk of developing the disease. Risk perceptions are subjective, reasoned estimates of the likelihood of a threatening event taking place (Weinstein, 1999). Absolute risk is the subjective evaluation of risk of developing breast cancer, and comparative risk is the subjective evaluation of risk compared to others of similar age and characteristics (Lipkus et al., 2005). Only comparative risk perceptions predicted higher levels of worry in healthy women in a study by Lipkus et al. (2005). While it seems plausible to suggest that the heightened awareness of risk in women with a family history could determine this worry, risk perceptions are associated with worry in healthy women with no family history (Gurmankin Levy et al., 2006) and in women with affected relatives (Hopwood et al., 2001). Risk perceptions may be important in predicting breast cancer worry in all women in the general population, but the research is limited by measurement issues (Bottorff et al., 2004). There is no gold standard to assess risk perceptions (French and Marteau, 2008), so they are measured in a variety of ways, such as numerical (e.g. 0–100), and verbal scales (e.g. very high risk to very low risk). This makes comparisons across studies difficult and leads to varying levels of reported risk. For example, in a meta-analytic review of breast cancer (Katapodi et al., 2004), numerical risk measures produced overestimations, whereas verbal measures produced optimistic bias. The impact of this measurement issue needs to be addressed, and importantly, this study was the first to include a comparison of measures within the same sample.
The Self-Regulatory Model of Illness Behaviour (SRM; Leventhal et al., 1980) may provide a framework to understand breast cancer worry in healthy women. The SRM explains how coping, behaviour and distress are influenced by illness perceptions which are cognitions about an illness or illness threat that direct a person’s behaviour in goal-directed ways. Illness perceptions are characterised by five dimensions: identity, consequences, cure/control, timeline and causes. Identity is related to both the label and the associated symptoms of the illness. Consequence beliefs refer to the perceived impact or severity of an illness. The cure/control dimension measures how curable or controllable an illness is. Timeline beliefs indicate the perceived timeframe of an illness. Causal beliefs vary considerably, but are often ordered into biological, emotional, psychological and environmental causes for an illness. Two further dimensions were later added to the model: emotional representations and illness coherence, which measures understanding of an illness.
Illness perceptions guide the response to an illness or illness threat and are associated with psychological functioning and distress across a wide variety of illnesses (Hagger and Orbell, 2003), including breast cancer (McCorry et al., 2013). The beliefs that healthy women hold as to the consequences and curability of breast cancer can impact upon cancer-specific worry (Buick and Petrie, 2002). For example, lower perceived control and more severe consequences were linked to more breast cancer–related distress in healthy women (Rees et al., 2004).
Researchers agree that although distinct constructs, risk perceptions may be influenced by illness perceptions (Marteau and Weinman, 2006). For example, risk judgements are constructed from likelihood and severity estimates, and personal risk beliefs of illness can be constructed by patients from their health status, health habits and family history of illness (Cameron, 2008). The content of illness perceptions can be linked to risk perceptions, for example, causal beliefs include the evaluation of factors that may increase one’s risk. Timeline beliefs relate to the perceived timing of when an illness will occur and the nature of the illness progression. In contrast, severity estimates relate more to perceived consequences and control. Despite this, little is known of the relationship between illness and risk perceptions as studies rarely measure these variables together.
One of the few studies to do so was conducted by Rees et al. (2004) who assessed 117 women at increased risk of developing breast cancer (based on family history of the disease) and 100 healthy women with average risk of developing the disease. Healthy women with an average risk of developing breast cancer reported less cancer-specific distress, different causal beliefs, more illness coherence, higher identity and less severe consequences than women with increased risk. Within the context of the SRM, illness and risk perceptions are considered more than simply independent predictors of worry, but as no research to date has examined both risk and illness perceptions as predictors of cancer-related worry, this relationship has not been assessed. One previous study examined risk and illness perceptions in individuals with a genetic predisposition to venous thrombosis (Kaptein et al., 2007). Higher risk perceptions were correlated with more negative illness perceptions and greater worry. Although illness perceptions predicted risk perception and thrombosis worry, they did not mediate the relationship between risk and worry. A possible alternative is that risk perceptions may mediate the relationship between illness perceptions and worry.
The aim of the investigators in carrying out this study, therefore, was to assess factors that predict breast cancer worry in healthy women below the age of 50 years. Variables such as family history, anxiety and risk and illness perceptions have all been assessed separately, but this study examined their combined influence on breast cancer worry. Specifically, it was hypothesised that having a family history of breast cancer, higher levels of state anxiety, higher risk perceptions and more negative illness perceptions predict greater breast cancer worry. Due to the lack of research on the relationship between risk and illness perceptions, and the implication of the SRM that variables such as risk perceptions may mediate the influence of illness perceptions on breast cancer worry (Cameron, 1997, 2003), this study also examined the potential mediating role of risk perceptions on the relationship between illness perceptions and breast cancer worry.
Method
Participants
The sample comprised 857 women (M = 27.15 years, standard deviation (SD) = 8.35 years) from the Republic of Ireland. Women included were between 18 and 50 years of age, without a previous diagnosis of breast cancer and able to read and write English. The majority of respondents were Anglo-Saxon in their cultural background (n = 846; 98.70%). Women were single (n = 508; 59.30%), married (n = 175; 20.40%), living with a partner (n = 158; 18.30%), divorced (n = 13; 1.60%) or widowed (n = 3; 0.40%). Women were employed (n = 473; 55.20%), in third level education (n = 343; 40.00%), working in the home (n = 21; 2.50%) or unemployed (n = 20; 2.30%). Many women reported no family history of breast cancer (n = 478; 55.80%), were unaware of their family history (n = 38; 4.50%) or had one relative (n = 273; 31.80%) or more than one relative diagnosed (n = 68; 7.90%).
Measures
Family history of breast cancer was measured by asking participants to indicate whether any female relatives had ever been diagnosed with breast cancer. Participants were also asked to indicate how often they perform breast self-examination, ranging from 0 (never) to 5 (more than once a month). Mammography screening was assessed by asking participants to indicate whether they have ever had a mammogram.
The Spielberger State-Trait Anxiety Scale (STAI; Spielberger et al., 1970) was used to measure state and trait anxiety. Participants indicated their agreement to 20 statements from 1 to 4. Items were summed to give a total trait and total state anxiety score, ranging from 20 to 80. The STAI has demonstrated reliability across a number of studies (Barnes et al., 2002). In this study, internal consistency for trait anxiety was α = .90 and .92 for state anxiety.
Absolute risk perceptions were assessed using four questions adapted from Gurmankin Levy et al. (2006). Numerical risk perceptions were assessed by asking participants to rate the likelihood of developing breast cancer in one’s lifetime, and also in the next 5 years, from 0 (you definitely will not be diagnosed with breast cancer) to 100 (you definitely will be diagnosed with breast cancer). Verbal risk estimates were also measured (how would you rate the chance of developing breast cancer; from very low to very high). Participants were also asked to rate how vulnerable they felt to getting breast cancer at some point in their lifetime from 1 (not at all) to 7 (extremely).
Comparative risk perceptions were measured using one item asking women to rate their perceived chance of developing breast cancer in comparison to that of the average woman from 1 (much lower) to 5 (much higher).
The Revised Illness Perception Questionnaire (IPQ-R; Moss-Morris et al., 2002), modified for a healthy population assessed illness perceptions. Respondents rated their agreement with statements about breast cancer. Items are rated from 1 to 5 except for those in the identity dimension; respondents indicate from a list of symptoms, whether they believe they are symptoms of breast cancer (yes/no). The questionnaire yields a total of nine subscales: timeline (acute/chronic), cyclical timeline, consequences, identity, personal control, treatment control, emotional representations, illness coherence and causes. The causal subscale was divided into psychological causes (e.g. stress or worry), behavioural and environmental causes (e.g. smoking), external causes (e.g. germ or virus) and medical causes (e.g. ageing, hormones), as suggested by Moss-Morris et al. (2002). Acceptable internal reliabilities for the subscales have been reported (Hagger and Orbell, 2003). Internal consistency ranged from .48 to .90 in this study.
Breast cancer worry was assessed by four questions adapted from previous research (Cameron and Diefenbach, 2001; Consedine et al., 2004; Lipkus et al., 2005). Participants were asked to rate how fearful, worried, concerned and anxious they were of getting breast cancer in their lifetime, from 1 to 5, and a mean worry score was calculated. Higher scores indicate greater breast cancer worry. Internal consistency for this study was α = .92.
Procedure
The study received approval from the Institutional Research Ethics Committee. Information about the study, along with contact details of the researcher, was sent to various organisations via email and websites. Participants completed the questionnaires anonymously. Participants who were interested were invited to complete the survey using a password protected survey link online. Participants who did not want to participate online could contact the researcher for a paper copy of the survey and consent form. A modified online consent form was used for those who completed the study online.
Statistical analyses
Data were analysed using SPSS for Windows (Version 21). Correlational analyses were conducted to examine variables that relate to breast cancer worry. A hierarchical multiple regression was conducted to test the hypothesis that having a family history of breast cancer, higher levels of state anxiety, higher risk perceptions and more negative illness perceptions predict greater breast cancer worry. To test the mediator hypothesis that the relationship between illness perceptions and breast cancer worry exists because women perceived themselves to be more at risk of developing the disease, a series of multiple regressions were conducted using Baron and Kenny’s method for testing mediation (Baron and Kenny, 1986).
Results
Participant characteristics and descriptive statistics
In total, 788 women completed the study online and 69 completed paper versions of the study. Due to the anonymous nature of the study, participation rate could not be calculated. Details of the study were sent to various organisations and websites, so it is not possible to calculate how many people saw details of the study, compared to those who took part. All variables were normally distributed. Means and SDs are reported in Table 1.
Descriptive statistics of the variables under study.
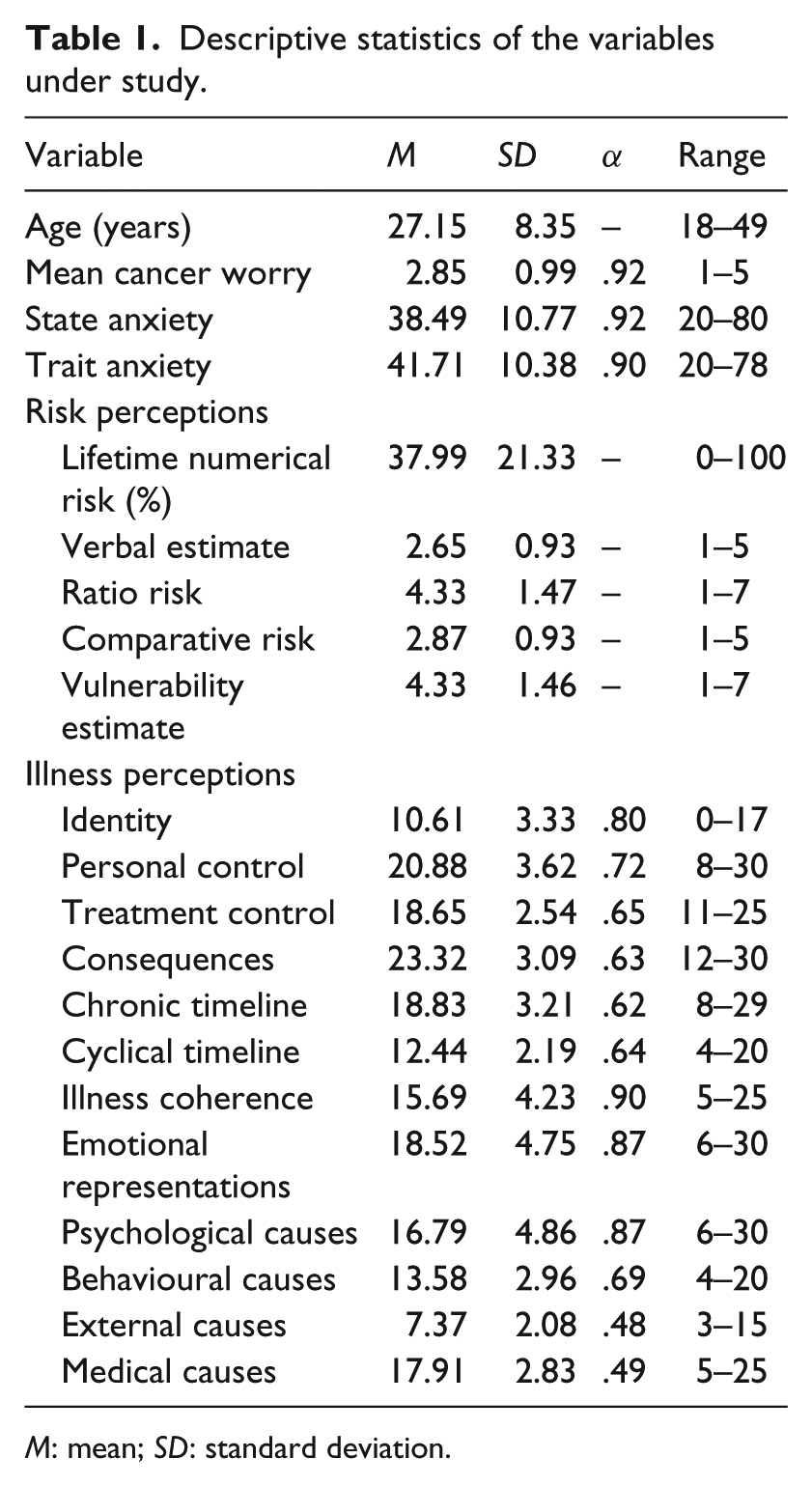
M: mean; SD: standard deviation.
Moderate to high levels of breast cancer worry were reported by 16.20 per cent of women, with a mean score of 2.85 (SD = 0.99). Approximately, 32 per cent of women reported never performing breast self-examination and only 6.20 per cent of women reported having a mammogram.
Predictors of breast cancer worry
A hierarchical multiple regression was conducted to test the hypothesis that family history, anxiety, risk perceptions and illness perceptions predict breast cancer worry. The variables were entered in blocks, so that each block of variables could be examined for their additional contribution to the variance, and were chosen based on an examination of results from the correlation analyses. Age was entered in the first step, along with family history, which has been shown in previous research to influence breast cancer worry. State and trait anxiety were entered into the second step to examine the role of general anxiety. Risk perceptions are considered important in the development of perceptions of illness (Cameron, 1997), so were entered in the third step. Illness perceptions were included in the final step. Correlations between predictor variables ranged from r = .08 to r = .58, while the variance inflation factor (VIF) scores ranged from 1.00 to 1.25 (tolerance scores ranged from 0.80 to 0.99), indicating that multicollinearity was not present in this study.
The overall model was significant, accounting for 45 per cent of the variance in breast cancer worry (F(21, 679) = 28.42, p < .001, R2 = .47, Adj R2 = .45). Age and family history explained 2 per cent of the variance in breast cancer worry (Fchange (2, 698) = 8.72, p < .001, Adj R2 = .02), although the beta weights were not significant. Anxiety accounted for 8 per cent of the variance (Fchange (2, 696) = 32.99, p < .001, Adj R2 = .08), with higher levels of state anxiety (β = .12, p = .005) predicting greater worry. Risk perceptions accounted for 19 per cent of the variance (Fchange (5, 691) = 38.59, p < .001, Adj R2 = .19). Women holding higher numerical risk perceptions (β = .21, p < .001) and higher verbal risk estimates (β = .10, p = .028) reported greater worry. Illness perceptions explained a further 16 per cent of the variance (Fchange (12, 679) = 17.47, p < .001, Adj R2 = .16). Holding more chronic timeline beliefs (β = .07, p = .039), a strong sense or understanding of breast cancer (β = .11, p < .001) and more negative emotional representations (β = .44, p < .001) predicted greater worry.
Mediation analyses
To test the hypothesis that the relationship between illness perceptions and breast cancer worry exists because women perceive themselves to be more at risk of developing the disease, four multiple regressions were conducted (see Table 2). In this study, a mediation effect is demonstrated when (1) illness perceptions are related to risk perceptions, (2) risk perceptions are related to breast cancer worry, (3) risk perceptions are related to breast cancer worry and (4) the contribution of illness perceptions to breast cancer worry is reduced when controlling for risk perceptions. In each analysis, age and family history were controlled in the first step. Correlational analyses (see online supplementary material) identified the illness perception dimensions and measures of risk perceptions that correlated with each other and breast cancer worry. Numerical risk perceptions were correlated with chronic timeline, cyclical timeline, illness coherence and emotional representations, as well as breast cancer worry. These variables were therefore included in the regressions.
Series of hierarchical multiple regressions assessing the mediating role of lifetime numerical risk perceptions to the relationship between illness perceptions and breast cancer worry.
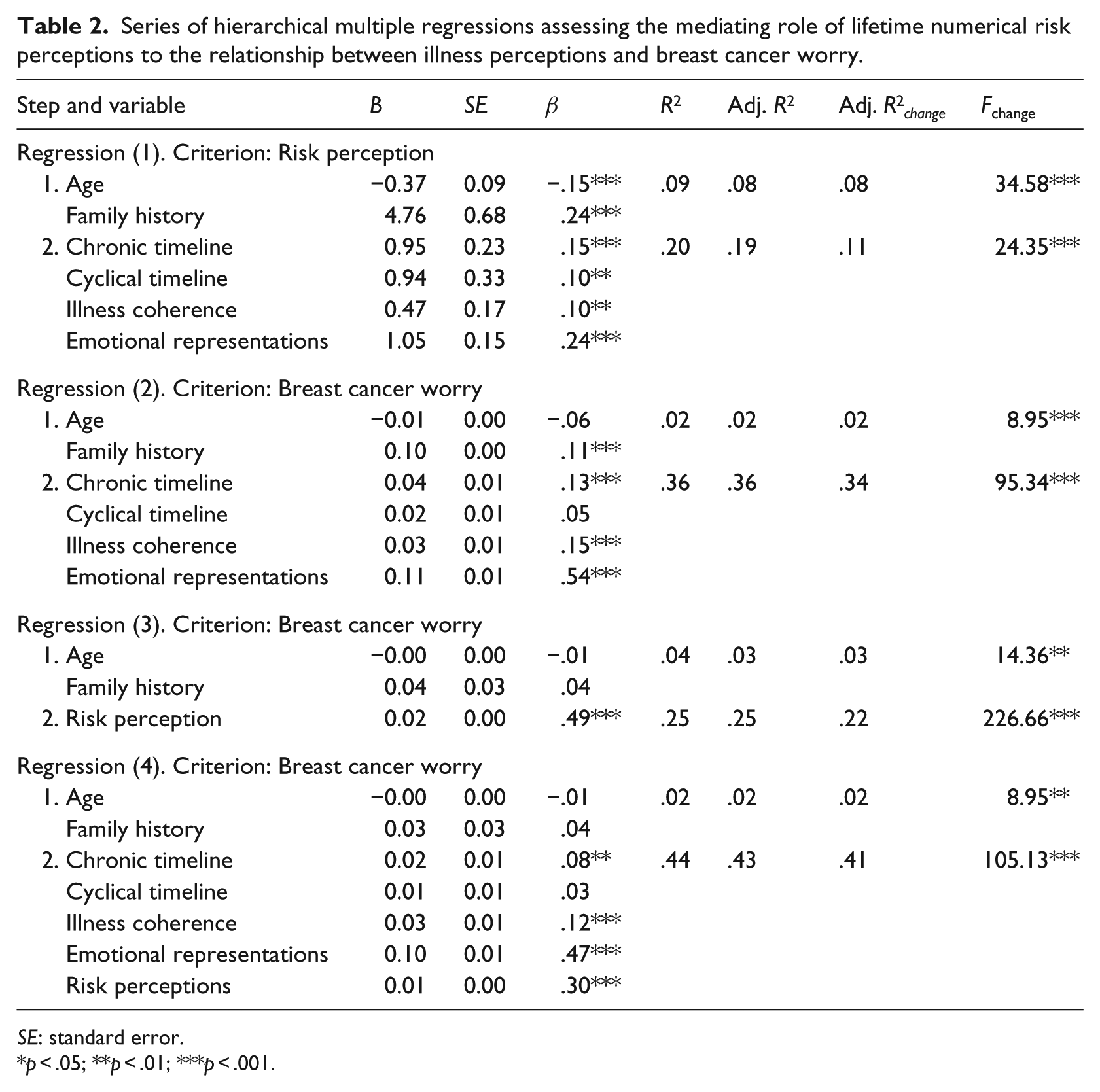
SE: standard error.
p < .05; **p < .01; ***p < .001.
In the first regression, illness perceptions were regressed onto risk perceptions, explaining 11 per cent of the variance. Only cyclical timeline, chronic timeline, illness coherence and emotional representations predicted risk perceptions. In the second regression, illness perceptions were regressed onto the dependent variable, breast cancer worry, and explained 34 per cent of the variance. In the third regression, risk perceptions were regressed onto breast cancer worry and explained 22 per cent of the variance. Illness perceptions and risk perceptions were regressed onto breast cancer worry. The total variance explained by risk and illness perceptions was 41 per cent. The beta weights for chronic timeline, illness coherence and emotional representations were reduced, although still significant, indicating that risk perceptions partially mediate the influence of these variables on breast cancer worry. In applying the Sobel (1982) test to assess the significance of intervening intervention effects, the differences between the coefficients before and after adjustment for risk perceptions were significant (ps < .01), indicating partial mediation.
Discussion
This study examined factors that influence breast cancer worry in a community sample of women under 50 years of age. Analyses were conducted to examine the influence of family history, state and trait anxiety, risk perceptions and illness perceptions on breast cancer worry. The overall regression model was significant, explaining 45 per cent of the variance. Specifically, it was found that younger women reported more worry. While the variance explained was small, this finding confirms previous research (Brain et al., 1999). Having a family history of breast cancer was also related to greater worry. This finding has been found previously (Van Oostrom et al., 2007), indicating that women feel more worried about developing breast cancer in the future if they have affected family members. Family history should, therefore, continue to be accounted for in future research in this area.
Women who reported more state anxiety also reported higher breast cancer worry, but it only accounted for a small percentage of the variance, suggesting that worry is not simply due to a predisposition to general anxiety or negative mood. This was the first study to examine this relationship in a healthy sample, highlighting the importance of examining anxiety in studies that also measure worry and distress. This finding needs to be confirmed, so further work examining the relationship between general worry and cancer-specific worry would be useful.
Risk perceptions influenced breast cancer worry. Women with higher absolute risk estimates measured numerically and verbally, reported greater worry, akin to Hopwood et al. (2001). It is interesting to note that only absolute risk perceptions were predictive of worry in the regression. Previous research has argued that comparative risk (compared to average woman), rather than absolute risk, predicts cancer worry (Lipkus et al., 2005). It may be that these estimates utilise different information; such that absolute risk is associated with negative affect and perceptions of control, while comparative risk is related to positive mood (Helweg-Larsen and Shepperd, 2001). Further research is needed to reveal the predictive influence of these different types of risk estimates. This study included women from the community. In previous studies, women who were ‘at-risk’ were sampled (Katapodi et al., 2004), wherein women who are attending genetic testing or have a known higher risk of developing cancer were included. Weinstein (1988, 1999) has suggested that there is a temporal component to risk estimates; women who are recruited at hospital settings are more aware of their risk, which is reflected in their estimates, whereas the perceived risk in women from the community who have a family history may be minimised. Although family history can influence breast cancer worry, perceived risk of developing the disease was more predictive of worry. The greater the perceived risk, the more worry reported. It is, therefore, important to not limit the focus of research to high-risk groups that have been identified based on their family history, without also measuring perceived risk of developing the disease in healthy, younger women. Also of note is that the reported risk perceptions were high. Younger women have a lower risk of developing cancer but this group reported high levels of perceived risk. Younger women reported more worry, so, for example, those in their 20s worried the most about cancer but had the lowest risk. Educational programmes may be necessary to help healthy women become more aware of their own personal risk, which in turn could reduce worry and unnecessary screening behaviours.
Risk perceptions measured numerically and verbally predicted breast cancer worry, but risk perceptions measured in ratio and comparative terms did not. Previous research has shown that type of measure of risk perceptions can influence how optimistic, accurate or pessimistic women seem to be in their perceptions of risk (Katapodi et al., 2004). Although there is no standard measurement of risk perceptions, this was the first study to include such a variety of risk measures. It provides a unique insight into how different risk perception measures relate to an outcome and highlights an important limitation in the methodology used in existing risk research.
Only one previous study has examined illness and risk perceptions simultaneously in healthy women (Rees et al., 2004). Specifically, it showed that women with average risk of developing cancer and with a strong illness identity reported more cancer-related distress. In this study, illness coherence, chronic timeline and emotional representations predicted greater worry. That is, women were more worried if they believed they had a greater understanding of breast cancer, believed it to be a chronic disease and held more negative emotional representations. The findings are supportive of the importance of illness perceptions in determining psychological outcomes (Hagger and Orbell, 2003). The different dimensions found to be predictive in this study in comparison to Rees et al. (2004) are of note. Their sample was older, and they were receiving counselling for genetic testing for BCRA1/2 mutations. In addition, in the Rees study, analyses were conducted on the two groups separately; risk and illness perceptions were assessed in women with increased or average risk. This study included healthy women in the community less than 50 years, with varying levels of perceived risk.
The SRM was constructed initially to explain a person’s response to a health threat, but was utilised in this study to examine how illness perceptions relate to perceptions of risk and subsequent worry. Risk perceptions partially mediated the relationship between chronic timeline, illness coherence, emotional representations and breast cancer worry. Women who found breast cancer to be more negative emotionally considered it to be a chronic condition and believed they had a greater understanding of breast cancer reported greater worry only when they also perceived greater risk. So, although women may hold negative perceptions of breast cancer, it will not lead to increased worry, unless they also hold high perceptions of risk of developing the disease. While this mediation warrants confirmation and further exploration, the findings provide tentative support that risk and illness perceptions are associated with one another in relation to cancer worry. The SRM could perhaps be expanded to include measures of risk, which may help to increase the predictive value of the model in healthy populations.
Clinical implications and future research
This study focused on the role of the SRM and risk perceptions in predicting breast cancer worry, but these variables may have implications for future health promotion campaigns aimed at enhancing breast awareness. Increasing breast awareness in women who previously reported high levels of worry may reduce their worry, which may influence subsequent screening behaviour. Illness perceptions have been implicated as predictors of mammography screening attendance in women in the community (Lostao et al., 2001), but very little research has explicitly measured the influence of risk perceptions on screening. Future research could usefully extend current findings by measuring the influence of worry, risk and illness perceptions, on adherence rates to screening and observable behaviours such as breast self-examination in healthy women of all ages. The SRM is a useful model, and its applicability to healthy populations is becoming more pertinent with the advent of screening programmes and genetic susceptibility testing for illnesses. Also of relevance is that illness perceptions are developed from a variety of sources, so they may be fully developed before individuals are diagnosed with an illness. Measurement of illness perceptions in at-risk as well as healthy populations may explain both an individuals’ response to a diagnosis and to the perceived risk of developing a disease.
There are limitations to this study that need to be noted. It was a cross-sectional study and thus causal relationships cannot be inferred. Conducting prospective research will help clarify the factors that influence cancer worry and the directional relationship between risk and illness perceptions. The sample overall was below 50 years of age so the results are not generalisable to older women. One further limitation is that although general anxiety was included, a broader range of mood was not assessed in this study. An alternative explanation for greater breast cancer worry and risk perceptions in younger women is that they may report more distress in general. Mood may influence participants’ judgements and perceptions of risk in the future, and breast cancer worry may reflect general mood, so this should be incorporated in future risk research.
Despite these limitations, the findings add to the literature given that the study was one of few to measure both risk perceptions and illness perceptions in a healthy group. It is the only study to date that has examined risk perceptions as a potential mediator between illness perceptions and worry in breast cancer and to have included a range of different measures of perceived risk. The interaction of risk and illness perceptions is a novel finding and may provide a better understanding of how these constructs can be conceptualised. Moreover, as the study comprised a large number of community-based women, the findings can be generalised to the wider population of women less than 50 years.
The study highlights that breast cancer worry is not influenced by any one single factor, but a range of variables that can be considered in future studies that aim to reduce breast cancer worry.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a Lady Gregory Doctoral Research Fellowship from the College of Arts, Social Sciences & Celtic Studies, National University of Ireland, Galway, and by a Doctoral Scholarship from the Irish Research Council.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.