
Abstract
This experiment explored consequences of two common lay theories about the diet–disease link: nutrient-centrism, the belief that nutrients (e.g. potassium) are crucial to staving off disease, and whole-food centrism, the belief that whole foods (e.g. bananas), containing these nutrients in their natural context, are most beneficial. Depicting an individual’s diet in terms of nutrients rather than whole foods containing these nutrients reduced the perceived likelihood that the individual would experience leading diet-related diseases (e.g. heart disease, diabetes). Although nutrition experts increasingly emphasize the health benefits of natural whole foods, people nevertheless appear to privilege nutrients when estimating disease risks.
Diseases that are strongly linked to dietary patterns are among the most formidable of public health challenges. In an era in which one-third of the US population qualifies as clinically obese, heart disease and diabetes have emerged as leading causes of mortality (World Health Organization (WHO), 2014), with treatment costs for heart disease alone estimated at over US$150 billion annually—a figure expected to double in the coming decades (Heidenreich et al., 2011). Meanwhile, the public is confronted with often conflicting advice from nutrition experts and the food industry regarding the connection between dietary intake and disease, as well as the food consumption habits that are most likely to promote long-term health. Food companies routinely advertise the vitamin and mineral content of their products on the basis of purported scientific evidence that these micronutrients are associated with positive health outcomes. Relevant examples abound, such as a recent label appearing on boxes of Kellogg’s Cocoa Krispies highlighting “25% Daily Value of Antioxidants & Nutrients” alongside a controversial claim to “support your child’s immunity” (Horovitz, 2009). In contrast, government dietary guidelines, such as the recent MyPlate initiative of the US Department of Agriculture, are increasingly taking a dietary pattern approach to healthy eating—one that bases recommendations on the natural whole foods that people should incorporate into their diets and in what amounts (for an overview, see Levine et al., 2012).
Although both types of dietary advice—that focusing on healthy nutrients and that focusing on healthy whole foods—are prevalent, some scholars have argued that the former has emerged as the dominate lens through which the public thinks about the link between dietary consumption and disease outcomes, which may carry negative implications for individual and public health (e.g. Scrinis, 2008). This study examined whether a focus on nutrients—a mindset we refer to as nutrient-centrism—carries implications for an important but under-researched aspect of this contemporary health crisis, namely, perceptions about the risk of diet-related disease.
The diet–disease link: nutrients versus whole foods
Although their relationship has been acknowledged as far back as Hippocrates’s famed advice to “let food be thy medicine …” (Lucock, 2004), scientific advances of the 20th century paved the way for a more nuanced understanding of the role of diet in disease outcomes. While often perceived as uniform, homogeneous substances, most foods are in fact biochemically complex, containing various micronutrients (such as vitamins and minerals) and macronutrients (such as carbohydrates, fats, and proteins); thus, they can be described and understood at both lower levels (“rich in vitamin C”) and higher levels of analysis (“apple,” “fruit”). Whereas research in nutrition science has long focused on beneficial effects of individual nutrients (e.g. vitamin C, omega-3 fatty acids) for human health and disease prevention (e.g. cancer, heart disease; Block, 1991; Kris-Etherton et al., 2002), epidemiological studies increasingly emphasize the importance of diets based on whole foods, which contain nutrients embedded in their natural context and confer a variety of health benefits, many of which remain poorly understood (e.g. Jacobs and Tapsell, 2007; van’t Veer et al., 2000). Yet, scholars contend that a nutrient focus serves as the dominant lens through which the public understands how dietary consumption impacts disease—a so-called “ideology of nutritionism” (Scrinis, 2002, 2008)—that distills the healthy aspects of food down to a selected set of disease-fighting nutrients and encourages consumers to overlook “more specific advice about what foods to eat more or less of, such as fewer processed foods and more plant-based foods” (Scrinis, 2008: 39; see also Pollan, 2008). This nutrient focus is readily apparent in the United States, where a majority of Americans now report taking some form of dietary supplement despite mounting evidence that many of these products are ineffective and potentially harmful for the general public (e.g. Guallar et al., 2013; Mursu et al., 2011). It is also apparent in the widespread marketing of “healthy” nutrients contained within packaged food products (e.g. sugary cereal) that most experts deem nutritionally poor on average (Nestle, 2002; Roberto et al., 2012).
If a nutrient focus is as widespread as many experts suggest, consumers may not see the proverbial forest for the trees when thinking about connections between diet and disease. That is, apples may seem healthy because they contain disease-fighting fiber, bananas because of their heart-healthy potassium, and so on—a heuristic or lay theory that overweights the presence of “good” nutrients relative to the myriad other healthy qualities that whole foods confer (Eastwood and Kritchevsky, 2005) and that may influence perceptions of diet-related disease risk. We examined this possibility in this research.
Lay theories of food and health
Recent psychological research suggests that perceptions of a food’s healthfulness are guided by lay theories that simplify judgments but are prone to bias. For example, consumers tend to think dichotomously about food as either “good” or “bad” for health, a heuristic that explains why spinach is unwisely selected over chocolate in survival scenarios (Rozin et al., 1996), why meals are judged to contain fewer calories when a “virtuous” food (e.g. salad) accompanies a “vice” one (e.g. burger; Chernev, 2011), and why promoting individual nutrients on food packaging makes nutritionally poor products appear healthy (Chandon, 2013). Importantly, these positive impressions are theorized to depend on perceivers’ health-related motivations and ability to process nutrition-related information (Moorman, 1990; see also Chernev, 2011).
Lay theories may similarly guide the public’s understanding of the health consequences of food choice and dietary patterns. A nutrient-centric theory—one that privileges lower-level properties (e.g. vitamin and mineral content) over its higher-level ones (i.e. the whole foods themselves)—may affect how people reason about the link between dietary patterns and disease and influence perceptions of disease risk. If so, “healthy” nutrients may paradoxically be deemed more disease-preventive than the “healthy” whole foods that contain them, despite the fact that people must eat food (not isolated nutrients) to survive and thrive. Moreover, because this tendency is presumably rooted in nutritional knowledge and understanding (e.g. awareness of vitamin C’s cancer-preventive properties; Block, 1991), this nutrient-centrism may be positively correlated with individual difference variables shown to moderate nutritional judgments in past research, such as diet-consciousness and information processing ability (Chernev, 2011; Moorman, 1990).
In this experiment, we explored the potential impact of a nutrient-centric versus whole-food centric mindset on judgments of disease risk and explored individual difference variables that potentially moderate such an effect. Specifically, we hypothesized the following:
H1. All else equal, describing a target person’s diet primarily in terms of nutrients as opposed to whole foods will lead observers to perceive the target as being at less risk for leading diet-related diseases (e.g. heart disease, diabetes).
Moreover, on the basis of recent nutritional judgment research suggesting that effects of health-relevant stimuli vary across individual perceivers, we explored the following research question.
RQ1. Might the hypothesized effect of highlighting a diet’s nutrients over its whole foods depend on individual difference variables previously shown to shape health-related perceptions (e.g. diet-consciousness)?
Method
Participants
A total of 114 participants from the Introductory Psychology participant pool at a large Midwestern university completed the experiment as part of a longer (30 minutes) food-themed laboratory session in exchange for partial course credit (for previously published data from this session, see Schuldt and Schwarz, 2010). In line with the general demographic profile of the university’s psychology students, participants were approximately 19 years old (M = 18.75, standard deviation (SD) = 2.30), predominately female (70%), and most described their upbringing as “middle class” or above in terms of socio-economic status (88%). This research was approved by the university’s institutional review board.
Materials and procedure
Upon arriving to the lab, participants were seated at semi-private computer stations, provided informed consent, and completed a web-based questionnaire that included standard demographic information (e.g. gender) along with individual difference variables that were explored as potential moderators of the predicted effect on the basis of previous research. These included height and weight (for calculating body mass index (BMI)); standardized test scores (i.e. self-reported Scholastic Aptitude Test (SAT)/American College Testing (ACT) score), as a proxy for general cognitive ability, or g (see Frey and Detterman, 2004); and diet-consciousness, which was worded as follows: “To what extent would you describe yourself as ‘diet-conscious,’ or focused on the nutritional quality of the foods you eat?” (1 = not at all to 5 = very much). Next came a series of short tasks, each lasting approximately 3 to 5 minutes and topically related to food and/or health, which were randomly ordered for each participant to avoid any systematic order bias.
Experimental manipulation
For the present task, participants were asked to read a brief (approximately 120-word) description and form an impression of a target person, “Steve Thompson,” adapted from prior work (Schuldt et al., 2012). The first two paragraphs were held constant across conditions and depicted Steve as young, generally healthy, and leading a typical middle-class American lifestyle. The key manipulation was applied to the third and final paragraph. In a between-subjects design, participants were randomly assigned to a description that either emphasized “healthy” nutrients (n = 58) in the target’s diet or a matched set of whole foods known to contain them (n = 56), which were selected based on pilot testing. For the pilot test, we selected five foods with a “healthy” reputation that also represented a wide range of food groups (i.e. animal protein, dairy, and fruits and vegetables), namely, bananas, fish, oranges, milk, and spinach. A separate sample of undergraduate participants (N = 237) from the same institution was then asked to “name the first three nutrients you can think of” contained within each food. Nutrients named by a majority of pilot participants were then selected to comprise the final set of matched nutrient-food pairings, specifically, potassium (bananas), omega-3 fatty acids (fish), vitamin C (oranges), calcium (milk), and iron (spinach). All other aspects of the person description were identical across conditions (see Appendix 1 for the complete text).
Measures
Immediately after reading the person description, participants reported their health-related impressions of the target. They first rated Steve’s overall health on the following item: “Overall, how healthy would you judge Steve to be, compared to the average American?” (1 = less healthy to 7 = more healthy), which was included to assess whether a person described as seeking a nutrient-rich diet would simply be perceived as a healthier person in general, as opposed to being at less risk for diet-related diseases specifically. Participants then completed the main dependent measures, rating Steve’s likelihood of ever experiencing five leading diet-related diseases: “During his lifetime, how likely is Steve to suffer from each of the following diseases or ailments?” (1 = very unlikely to 7 = very likely), the assessed diseases being heart disease, diabetes, stroke, cancer, and obesity, randomly ordered for each participant. A composite risk score, serving as an overall measure of disease-risk perception, was also computed by averaging across the five disease judgments for each participant (α = .87).
Results
For each disease examined, a multivariate analysis of variance (MANOVA) revealed lower risk estimates in the nutrients condition than whole foods condition (see Figure 1). This difference was statistically significant for four of the five diseases, Fs > 4.61, ps < .05, ds = .40 to .61; only the obesity measure did not show a significant difference, F(1,112) = 1.92, p = .17, d = .26. To examine the overall effect of condition on disease-risk perception, a follow-up analysis of participants’ composite risk scores revealed significantly lower risk ratings in the nutrients condition (M = 2.79, SD = .94) than in the whole foods condition (M = 3.34, SD = .96), F(1,112) = 9.43, p < .01, d = .58. These effects remained significant when controlling for BMI, gender, diet-consciousness, and SAT/ACT score. Furthermore, no effect of condition was found on perceptions of the target’s overall health (Mnut = 5.55 vs Mwf = 5.59; |t| < 1), suggesting that the experimental manipulation influenced perceptions of disease risk in particular.
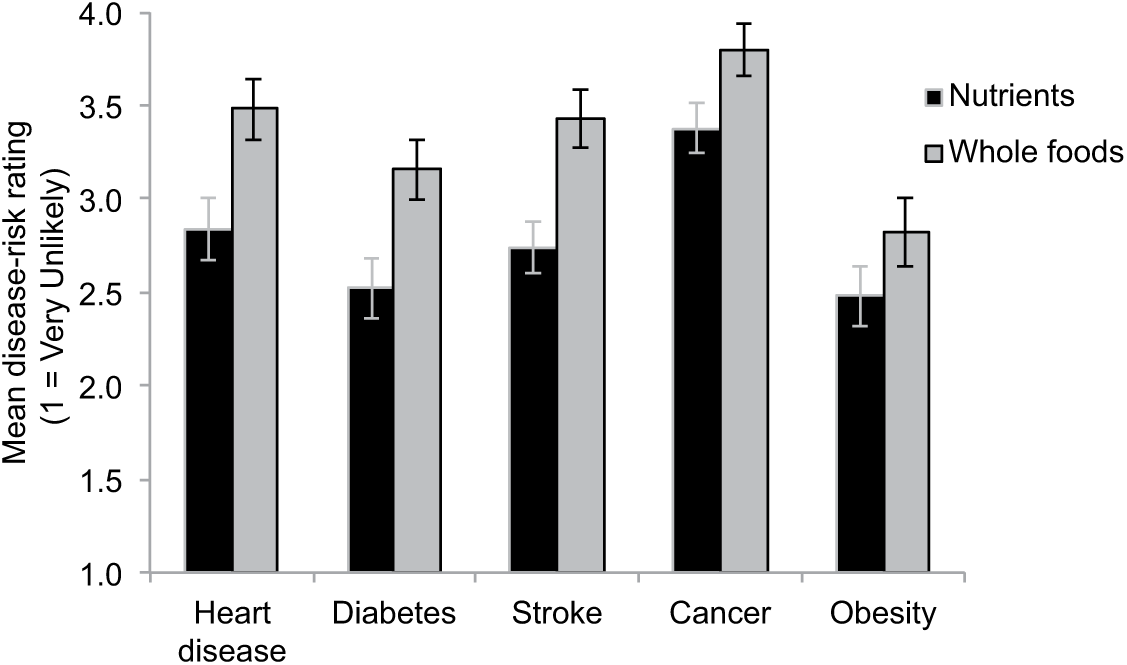
Mean risk judgments for five leading diet-related diseases by condition (nutrients vs whole foods). Error bars represent mean standard errors. All comparisons except obesity are significant at p < .05.
Next, regression models and spotlight analyses (Aiken and West, 1991) tested whether the reported significant effects were moderated by the individual difference variables described above (condition was coded 0 = nutrient-centric, 1 = whole-food centric; continuous moderators were mean-centered prior to constructing interaction terms). Of the four moderators examined, significant effects were observed for two: SAT/ACT score and diet-consciousness. Specifically, the SAT/ACT interaction term was significant, |t|(102) = 2.66, p < .01, and spotlight analyses (at M ± 1SD) revealed a stronger effect of condition among participants with higher SAT/ACT scores (Mnut = 2.52 vs Mwf = 3.53; |t|(102) = 3.91, p < .001) but no difference among those with lower test scores (Mnut = 3.15 vs Mwf = 3.18; |t| < 1). Turning to diet-consciousness, although its interaction term was not significant, a more pronounced (and significant) effect was again observed at higher levels of this variable (Mnut = 2.77 vs Mwf = 3.46; |t|(102) = 2.58, p = .01) but not lower levels of this variable (Mnut = 2.86 vs Mwf = 3.21; |t|(102) = 1.31, p = .19).
Discussion and conclusion
Is a diet deemed more disease-preventive when it is described in terms of nutrients rather than whole foods that contain them? While scholars from various disciplines have expressed concern about society’s tendency to privilege nutrients over whole foods in health judgments and decision-making (e.g. Jacobs and Tapsell, 2007; Scrinis, 2008), scant research has examined its implications for perceived risk of diet-related illnesses, such as cardiovascular diseases, which claimed over 17 million lives (31% of global deaths) in 2012 alone (WHO, 2014). When judging a person’s risk for experiencing diseases including heart disease, stroke, and diabetes, these results suggest that people may rely on a nutrient-centric lay theory that privileges a diet’s nutrient content and overlooks the health and disease-preventive properties of the whole foods that contain them (e.g. van’t Veer et al., 2000). Moreover, consistent with past work on the role of individual differences in nutrition-related judgment, this research suggests that the effect of nutrient-centrism may be larger among those with greater dietary concern as well as greater processing ability, presumably because they may be more likely to attend to nutritional information and understand its potential relation to disease.
Although these findings provide initial evidence that nutrients hold more sway than whole foods when it comes to disease-risk perception, a few limitations are worth noting. Our participants (students at an elite public university) were not representative of the broader public; thus, we caution against generalizing from this sample and this laboratory context (a food-themed study). It is possible, for instance, that although the associations between the nutrients examined here and positive health outcomes may be more pronounced among more educated individuals from higher socio-economic backgrounds, effects for nutritional experts, clinicians, and consumers with more extensive health knowledge may differ from those reported here—an important avenue for future research. Also, although the reported effects were significant and moderate in magnitude (Cohen, 1992), mean risk ratings were below the scale midpoint (4.0), suggesting the target was perceived as being at relatively low risk for experiencing these diseases overall. This observation is consistent with the biographical description that appeared in both conditions, which portrayed the target (“Steve”) as young, active, and “conscious about his diet.” Similarly, this generally healthy description might help explain the lack of significant effect on perceived risk for obesity, which received the lowest risk estimates of the five diseases examined and which—although recently recognized as a disease by the American Medical Association (AMA, 2013)—may not yet be widely regarded as such by the general public (Lombrozo, 2014). And while these analyses suggested some important moderating factors, variables not assessed in this study may well have contributed to this effect. For example, participants may have perceived certain whole foods (e.g. bananas, milk) as less healthy because they include some “disreputable” nutrients (e.g. sugars, fat; see Oakes, 2004).
Nevertheless, these findings suggest that society’s widespread nutrient focus may influence how people reason about the link between dietary patterns and disease, and specifically, that a food’s low-level properties (nutrients) may be perceived as playing a particularly crucial role in the development and prevention of leading diet-related diseases.
Future research should examine factors that contribute to and attenuate these effects. In particular, as others have noted (Scrinis, 2002, 2008), these perceptions may reflect the current preponderance of information in both nutritional literature and in industry advertising that links disease outcomes to specific nutrients, as compared to whole foods (see also Guallar et al., 2013; Jacobs and Tapsell, 2007). Future research should also examine the role of conscious and non-conscious processes in these judgments. In this study, we employed a between-subjects design to explore more subtle associations between nutrients and disease-risk perceptions rather than testing explicit comparative judgments (e.g. opinions about the relative health value of nutrients vs whole foods). Nevertheless, future studies might explore the role of conscious awareness more systematically, for example, by examining whether these effects are more pronounced under conditions in which cognitive resources are limited (e.g. Gilbert et al., 1998).
These findings also suggest a tendency toward reductionist thinking when assessing health consequences that may be enhanced under conditions that promote lower-level over higher-level (abstract) construal, such as decision scenarios that are temporally proximal (e.g. food choices intended for immediate vs delayed consumption; Trope and Liberman, 2010). Finally, these results may also have important implications for public health. To the extent that people privilege nutrients in isolation over the whole foods that contain them, even well-intentioned efforts to incorporate heathier dietary choices into one’s diet may backfire in a contemporary food environment where “healthy” nutrient claims adorn boxes of Frosted Flakes but not fennel.
Footnotes
Appendix 1
Text of the person description with alternative wording in brackets.
Steve grew up in Bangor, Maine, and he graduated from the University of Arizona with a Bachelors degree in 2004. While he was still an undergraduate, Steve was recruited by a small Internet company in Chicago, where he has lived and worked ever since.
In his free time, Steve enjoys watching Alfred Hitchcock movies, reading, cooking, playing poker, and exploring local pubs with coworkers and friends. During the winter season, Steve spends his vacation time skiing in the western states of Colorado and Wyoming.
Steve is also conscious about his diet. For instance, during the week, he makes sure that the foods he eats include bananas [potassium], fish [omega-3 fatty acids], oranges [vitamin C], milk [calcium], spinach [iron], and a variety of other healthy foods [nutrients]. On the weekends, however, he is more relaxed about his diet and often eats out at restaurants with friends.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.